
Abstract
The unification of the American Association for Health Education (AAHE) and the Society for Public Health Education (SOPHE) generates a long-desired synergy, a ramping up of our leadership influence in promoting health. It also serves as an ongoing opportunity to reflect on how we synergize the distinct philosophic, scientific, and practical approaches that our AAHE colleagues bring in constructing a larger tent for public health education. Running parallel to our union with AAHE is the undertaking by several schools of health, physical education, and recreation (HPER) to become schools of public health. The unification between AAHE and SOPHE can be of enormous benefit to such a process. Just as the harmonious integration of two organizations with similar but distinct perspectives depends on compromise and transcendence, the schools that they embody—both public health and HPER—might consider ways to engage in continued dialogue to assure a more expansive paradigm for public health. SOPHE has an important role to play in this process, and with the additional insight and influence that our AAHE colleagues bring, we can become more instrumental as a boundary spanner. Mechanisms for such integration are discussed.
Keywords
On July 17, 2012, the American Association for Health Education (AAHE) and the Society for Public Health Education (SOPHE) issued a joint statement of historic importance to the profession: As of May 1, 2013, AAHE will formally retire as one of the five organizations under the American Association for Health, Physical Education, Recreation and Dance (AAHPERD) and AAHE members are being encouraged to join SOPHE. Quoting Dr. Caile Spear, the AAHE President, For more than 40 years, health promotion leaders have advocated for AAHE and SOPHE to combine their efforts, and this historic milestone brings us one step closer to that vision. . . . Our combined membership will focus on advocating for quality health education and promotion programs in all areas of society including schools, health care, government, community and international arenas. (SOPHE, 2012)
This joining of forces generates a long-desired synergy, a ramping up of our leadership influence in promoting health. It also serves as an ongoing opportunity to reflect on how we synergize the distinct philosophic, scientific, and practical approaches that our AAHE colleagues bring in constructing a larger tent for public health education. Although memberships of the two organizations overlapped and the following is a generalization, historically AAHE has been associated with schools of health, physical education, and recreation (HPER)—hence the alignment with AAHPERD—whereas SOPHE reflected a greater representation from public health schools and programs, the latter sometimes in schools of HPER. We should not assume that the perspective(s) that AAHE members offer is entirely congruent with that of SOPHE members, because many AAHE and AAHPERD members are informed by and have allegiance to different professional histories. Perhaps this is an obvious point, but it exists within a subtler context in which our newly merged Society should be active: Running parallel to our union with AAHE is the undertaking by several schools of HPER to become schools of public health. Dr. Robert Gold, SOPHE Immediate Past President, was dean of a school that underwent such a transformation at the University of Maryland. The new school of public health at the University of Colorado and the reconfigured City University of New York school at Hunter College also integrate HPER-type programs within the larger constellation. At Indiana University–Bloomington, I began a process as dean of the School of HPER that culminated in the summer of 2012 in acceptance by the Council on Education For Public Health (CEPH), the national accrediting body for schools of public health, of our application to embark on the prerequisite self-study and reorganization with the goal of becoming an accredited school within the next 2 years. Accordingly, we have just changed our name to the Indiana University School of Public Health–Bloomington. Other HPER schools are actively considering such a transition, many already having CEPH-accredited programs for the MPH degree in health education and health promotion.
The SOPHE–AAHE unification provides strategic opportunities for our expanded membership to support allied professional schools that embark on a transition to public health. My experience leads me to suggest at least two arenas for our involvement. The first concerns how we may be supportive of HPER and other allied health schools wishing to transition to public health in being adequately represented by the professions that are traditionally required for accreditation: biostatistics, environmental health, epidemiology, health administration, and the social and behavioral sciences. The second concerns how we work with CEPH and other policymaking bodies in embracing the professional specialties uniquely represented in schools of HPER and other allied health schools as legitimate arenas for public health research, training, and practice. As for the first, at Indiana University–Bloomington, this meant adding units for environmental health, epidemiology, and biostatistics, along with hiring new faculty with the requisite specialties. What type of encouragement and assistance can and should we provide as a professional society in supporting institutional reorganization necessary to meet current accreditation standards for public health schools? From my experience, the transition from HPER to public health causes great anxiety among faculty members and students who experience the change as disconcerting. As AAHPERD represents many of the professions affected by schools that desire to transition, how can the new alignment with AAHE reinforce collaborations with professional organizations that represent the affected disciplines?
As for the second arena, what considerations can professional organizations such as SOPHE take into account in promoting the accreditation process for new schools of public health emerging from traditions that are historically outside of CEPH’s purview? The Indiana University School of HPER began planning its transformation to a school of public health at the same time that the Department of Public Health within the Indiana University Medical School was doing so in Indianapolis. In proposing two schools within a state university system (and a state) that previously had none, a distinct and purposeful rationale was required for each to obtain the necessary approvals by the university president, board of trustees, and state oversight commission on higher education. In Indianapolis, as with most schools of public health that emanate from a medical tradition, a strong focus was placed on disease prevention with leading interventions being informed largely by the epidemiological, medical, and psychological sciences. The history of schools of public health in the 20th century largely reflects the medical profession’s influence on federally funded research with eradication of disease as the main focus (Gebbie, Rosenstock, & Hernandez, 2003). In contrast, the Indiana University HPER school’s programs derive from specialties in physical health and fitness, promotion of wellness, recreation, exercise and sports sciences, and school and community health education with leading interventions informed largely by the social, behavioral, and kinesthetic sciences. Degree programs and concentrations include those not often found in schools of public health such as kinesiology, exercise and sports sciences; parks, recreation, and tourism; and school health, physical education, and dance. These programs represent a valid and innovative niche in public health. Consider, for instance, their relevance for the most pressing epidemic of our time—obesity. But for accreditation purposes, schools that arise from the HPER tradition must articulate an epistemology and related scientific processes that parallel those of the established public health disciplines (N. Clark, personal communication, August 23, 2012). By so doing, public health schools emerging from HPER—while maintaining their distinct precepts—can become more synergistic with schools influenced by the medical tradition, and at the same time modernize focal niches in the training of public health professionals. In constructing a path to building a new kind of school, I found two established and complementary frameworks to be helpful, one based on public health functions and a second for structuring them organizationally into a model for public health education that reflects expected future trends and developments.
A Framework of Public Health Functions
The first framework, shown in Figure 1, is a continuum of functions that are foundational in the training of the public health disciplines. Disease prevention cuts across three of the dimensions: repair (3° prevention), recovery (2° prevention), and avoidance of disease (1° prevention). Repair consists of stabilization of a permanent disability to an optimum state of recovery. Recovery is a return to an original state of health. Avoidance consists of steps taken to evade ill-health. As noted above, the disease prevention side of the continuum has been the main focus of traditional public health, informed by epidemiologic, medical, toxicological, behavioral, and psychological approaches. From an epistemic perspective, their scientific processes are informed primarily by statistical applications to randomized controlled and quasi-experimental research designs. Of the HPER professions, kinesiology, exercise science, and sports science best integrate with the disease prevention dimensions of the continuum in that the scientific methods are most consonant with experimentalism and many of the applications are for recovery and repair of physical disabilities, for example, techniques to return to full functioning after a sports injury among active children and adults (2° prevention), or recovery from fractures due to falls among the frail elderly (3° prevention).

Functional dimensions of public health
In the latter half of the 20th century, a movement to expand public health beyond a disease orientation emphasized the relevance of health promotion, holistic wellness, and increased quality of life. These added dimensions reflect the World Health Organization’s (1948) definition of health as a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity. The framework in Figure 1, therefore, also includes dimensions of health promotion: individual wellness (1° health promotion), community wellness (2° health promotion), and community well-being (3° health promotion). Individual wellness consists of attaining an optimum state of personal health through health promoting activities (Green & Raeburn, 1990). Community wellness involves grassroots and organizational efforts to improve the health of the local community and its citizenry (Minkler, 2005). In contrast, community well-being is not health risk—or condition—focused per se but directed at producing the highest quality of community life through indigenous social and/or cultural movements (Beauchamp, 1976; Buchanan, 2000). Research and planning approaches to health promotion now incorporate methods with established epistemologies such as social cognitive theory and the application of collective efficacy in informing community health interventions (Bandura, 1986), community-based participatory research involving lay constituents in all aspects of research (Minkler & Wallerstein, 2003), and the PEN-3 Model situating aspects of culture as central in developing program interventions (Airhihenbuwa, 1995). The exercise, recreation, and physical education disciplines in HPER schools are integral to assuring a healthy citizenry and therefore consistent with primary promotion. Moreover, sports, dance, recreation, and other forms of social activity are linked to tertiary promotion because they are directed at community quality of life, incline interventions toward social protective factors rather than—as in secondary health promotion—targeting specific health risks, intervene in naturally occurring and positive community functions, use intervention strategies that affirm functional social and cultural norms, and are not prescriptive in intervening (e.g., lose weight, exercise, just say “no”), but encouraging by building on the innate enthusiasm of ongoing social and cultural activities. When disciplines found in schools of HPER become the basis for organized community action, they also can function in the secondary promotion domain. The following story perhaps best illustrates the point.
What Does Captain Kidd’s Pirate Ship Have To Do With Public Health?
As a public health traditionalist who became dean of the oldest School of HPER, I experienced a new lens through which I could envision approaches to community health promotion. An example early in my tenure occurred when I was asked by faculty holding a joint appointment in the Department of Recreation, Parks and Tourism Studies and Department of Kinesiology to fund a project for final verification of the authenticity of the Captain Kidd’s last pirate ship that lay in shallow waters off the coast of the Dominican Republic. Our academic diving program had been involved in the Dominican Republic since the 1990s and it was well received locally because it was instrumental in recovering underwater heritage sites such as the Captain Kidd wreck. Although the funding request seemed unusual considering that the school was increasingly tilting toward a public health focus, the faculty nevertheless made a convincing case. I was willing to provide support from the school’s discretionary fund only under the condition that the program linked with local health development efforts. Without the discretionary funding, it was unlikely that the project would have proceeded as rapidly, if at all.
The subsequent goodwill that we received from government officials, hotel operators, and local community members for assisting in a culturally resonant initiative—along with the long-established relationship that solidified a basis of trust—paved the way for meetings with the Dominican Republic’s Ministers of Public Health, the Environment, and Tourism; the dean of the health school at the national university; key influential members of the hotel tourism industry; the director of the national cultural museum and other local officials. In these meetings, we introduced the concept of linking public health works to the discovery of the pirate ship. For instance, the local hotels were interested in the natural underwater preserve that was being established for the ship to attract tourists. Yet, the natural water supply was not potable and tropical vector-borne diseases, including malaria and dengue fever, were common. In addition, other vectors such as rodents were prevalent in local beach communities, and the beaches themselves had glass shards and other dangerous objects that would require careful maintenance. Because the Captain Kidd ship was seen as both a source of national pride and an economic development opportunity, all these groups were interested in improving health conditions within the country. On a return visit to the Dominican Republic, the director of the museum who had contacts with local, nonprofit, civic development organizations suggested that we meet with one particular grassroots organization that worked in communities in the interior of the Dominican Republic that lacked basic health needs. As a result, we collaborated with a U.S.-based nonprofit health foundation and provided faculty expertise, student interns, and needed medical supplies to the community. This experience convinced me that sometimes the most direct route to a public health concern is not by focusing on the issue itself but by focusing on positive cultural and social opportunities that build a sense of community pride and that may enhance opportunities to nurture well-being.
Similar examples of such synergies between 3° health promotion approaches like the Captain Kidd initiative and 2° health promotion approaches like the resulting community-based health initiatives occur with other programs emanating from the HPER tradition. Dance, music, and mural painting are currently being used both in the barrios of South America and New York City for peace, reconciliation, and intellectual and social development. Local club sports are enormous cultural and social influences on adolescents and young adults in contemporary society. They not only motivate problem-awareness and solutions to common sports injuries such as concussions or fractures but also stimulate social development, competition, conflict resolution, and cooperation. Similarly, recreation, games, and play reinforce social emotional connections. The Captain Kidd story illustrates the salutary influence that recreation and tourism can have when arched in the direction of social and cultural well-being. A main challenge for the disciplines in schools of HPER transitioning to a school of public health is their willingness to embrace a health promotion orientation like that in Figure 1 as central to their mission.
Reenvisioning an Organizational Framework for Public Health Education
Whereas Figure 1 helped in conceptualizing the functional niches occupied by the health specialties in HPER, Figure 2 aided in developing an organizational framework that both embraced and integrated the HPER disciplines with those required for accreditation. CEPH expects schools of public health to maintain five core disciplines—biostatistics, epidemiology, environmental health, health administration, and the social and behavioral sciences—and most schools of public health are organized by departments for each. In making the transition from HPER to public health, schools have an opportunity to innovate new structural arrangements. If our process at Indiana University–Bloomington provides a lesson, it is that the resistance to new organizational arrangements can be a major stumbling block in undergoing a successful transformation.
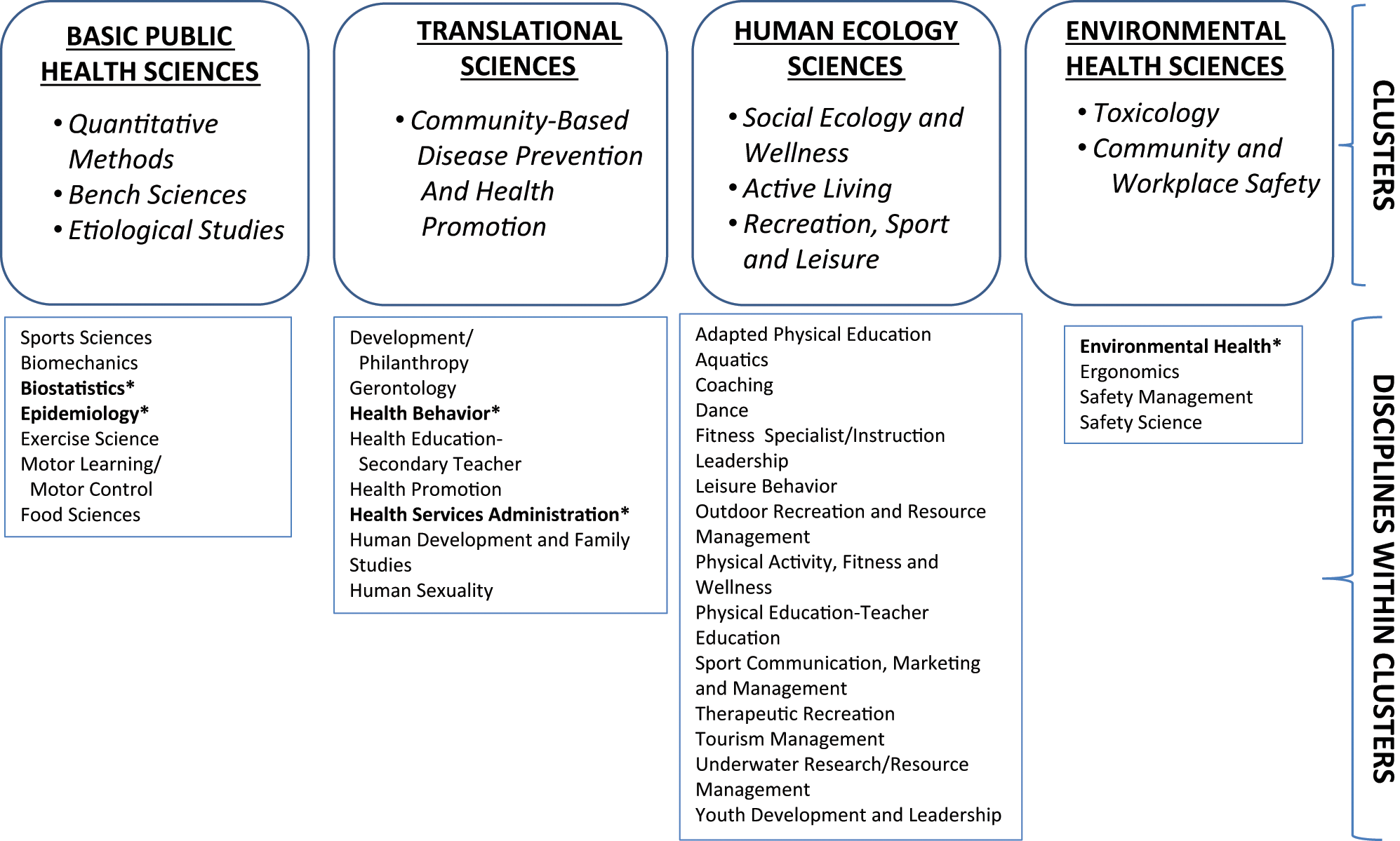
Organizational cluster model for IU-B school of public health
In 2010, rather than appending departments traditional in schools of public health to those already in HPER, our school’s faculty council approved the organizational model that appears in Figure 2. The model is composed of four integrated clusters: Basic Public Health Sciences, Translational Sciences, Human Ecology Sciences, and Environmental Health Sciences. It illustrates one possible approach to structural rearrangements that can meet current public health accreditation standards and integrate the HPER disciplines. Additionally, it creates innovative opportunities for research collaborations. The model is informed by two leading public health authorities: The National Institutes for Health (NIH), the foremost research arm of the federal government (Greenwald & Cullen, 1985); and the Institute of Medicine (IOM), the foremost health policy institute chartered by the federal government (Gebbie et al., 2003). From a science standpoint, the structure in Figure 2 reflects the five phases of research developed at NIH that has been widely adopted by other federal agencies such as the Centers for Disease Control and Prevention: (a) research, or the investigation of new knowledge about diseases and approaches to their prevention; (b) methods development, or the specification of program development, measurement, and analysis designs for pilot testing interventions informed by Phase 1; (c) efficacy trials, typically randomized, controlled trials to test the intervention under ideal conditions; (d) effectiveness trials, or tests of the intervention in real-world settings; and (e) dissemination trials, or monitoring and evaluating the conditions that hinder or facilitate widespread use of the intervention (Centers for Disease Control and Prevention Office of Public Health Research, 2007; Greenwald & Cullen, 1985). This approach is most aligned with the disease prevention side in Figure 1 and the Basic Public Health Sciences in Figure 2.
In recognizing the inherent limitations in the NIH framework, the IOM produced a report on public health education for the 21st century that characterized federal research funding in the 20th century as fostering single-discipline approaches in schools of public health (Gebbie et al., 2003). The IOM report recommended restructuring to transdisciplinary research consisting of questions that transcend the singular departments or specialized knowledge bases. In so doing, the IOM called on schools of public health to reevaluate their research portfolios and reformulate curricula and faculty. Accordingly, the model in Figure 2 not only incorporates the traditional research elements from the NIH model but also reconstitutes departments that are traditional to schools of public health into transdisciplinary clusters with the HPER disciplines integrated throughout. In this model, a cluster for Basic Public Health Sciences includes the traditional disciplines such as biostatistics and epidemiology, but adds kinesiology because it employs similar methodological designs. With sufficient encouragement, such a department could develop innovative arrangements for research that parallel the first three phases of the NIH model (i.e., research, methods development, and efficacy trials). The cluster for Translational Sciences combines two traditional areas—administration and public health education—that specialize in program development, management, evaluation, and community health. These specialties typically maintain the community networks and organizational linkages that can assist with the latter two phases of research (i.e., effectiveness and dissemination). Indiana University–Bloomington HPER already had a Department of Applied Health Sciences (with several faculty members affiliated with both AAHE and SOPHE), and it formed the basis for this cluster. The Human Ecology Sciences cluster is devoted to the social and cultural aspects of well-being represented on the health promotion side of the continuum in Figure 1. Because of its complex nature consisting of both the clinical and ecological sciences, the traditional environmental functions form a cluster that span the entire continuum in Figure 1 adding safety and ergonomics that were already specialties in HPER.
Collaborations not only within but across clusters enrich approaches to research by importing new epistemological approaches. A return to the parable of Captain Kidd illustrates how just such arrangements can work. By taking a transdisciplinary approach to our activities in the Dominican Republic, several disciplines from the Human Ecology Cluster became involved—tourism management, underwater resource management, aquatics, therapeutic recreation, and leisure behavior. Working with disciplines in the Translational Sciences Cluster, community health promotion expertise joined the mix in assessing community health needs that could be addressed simultaneously with the work around the pirate ship. Similarly, scientists that would fit into the Environmental Health Sciences Cluster team assisted in the water- and vector-borne threats. The entire operation could serve as the basis for transdisciplinary research conducted in collaboration with the Basic Public Health Sciences Cluster. The main challenge for integrating the disciplines in such fashion is the ability to overcome professional turf issues that result in departments remaining as silos rather than embracing a more holistic vision.
Reconciling the Schisms of “isms”
About 20 years ago, Green and Raeburn (1990) lamented the sharp theoretical and ideological divide between the social and behavioral sciences. Such professional conflict is commonplace in public health: experimental versus nonexperimental research, qualitative versus quantitative methods, disease prevention versus health promotion, individual versus social-systems approaches. These conflicts also extend to the challenge in incorporating HPER disciplines into public health models. No consensus exists on whether and how to develop schools of public health from complementary institutions like HPER, and conflict will inevitably arise in reformulating public health education for our present world. But sectarian bickering diverts the profession-at-large from a more “universal” and compelling objective in bringing a holistic and comprehensive approach to vexing contemporary public health challenges. Some of the leading minds in the basic sciences give reason to believe that anything but a holistic approach is inappropriate and misleading: There seems to be no single mathematical model or theory that can describe every aspect of the universe. Instead . . . there seems to be the network of theories called m-theory. Each theory in the m-theory network is good at describing phenomena within a certain range. Wherever their ranges overlap, the various theories and the network agreed, so they can all be said to be parts of the same. (Hawking & Mlodinow, p. 58)
Physicists term this interplay across and among theories model dependent realism. In reference to Figure 1, it suggests that the most powerful theories are linked across the continuum. As Figure 2 suggests, the more we combine approaches intelligently to become transdisciplinary, the more synergy we create in producing desired outcomes. The unification between the AAHE and SOPHE can be of enormous benefit to such a process. Harmonizing the interests of these two organizations parallels that which is required for integrating the disciplines from Schools of HPER and Public Health. One core measure of successful integration is that it results in positive transformations that advance the profession. Pondering how the HPER and traditional public health disciplines may unify is most salient. Just as the harmonious integration of two organizations with similar but distinct perspectives depends on compromise and transcendence, the schools that they embody—both public health and HPER—might consider ways to engage in continued dialog to assure a more expansive paradigm for public health. SOPHE has a role in this process, and with the additional insight and influence that our AAHE colleagues bring, we can become more instrumental as a boundary spanner. Certainly, not all schools of HPER have an interest in transforming to a public health school, a boundary to be respected. But in either case, our colleagues in the HPER disciplines are important to our collective work. How we continue under our newly merged membership to embrace the perspectives of our allied professions is a central question in a world becoming increasingly interconnected and complex. Physicists came up with the elusive unified field theory for the universe. Hopefully we can do the same for public health education.
Footnotes
Editor’s Note
SOPHE has been working for several years with leaders of the American Association for Health Education (AAHE) to strengthen the health education profession by uniting our resources under one roof within SOPHE. This has been no small task, in part since AAHE has been a part of the American Alliance for Health, Physical Education, Recreation and Dance (AAHPERD) for some 70+ years. It is expected that AAHPERD’s National Associations (including AAHE) and Research Consortium will unify as of May 2013 (upon approval of revised bylaws by the AAHPERD Alliance Assembly). At that time, AAHPERD will primarily focus on physical education, physical activity, and health. AAHE will be sunset. SOPHE has been negotiating with AAHPERD leaders about particular AAHE products or services that could be integrated into SOPHE as the principal independent organization representing the health education profession.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.