
Abstract
Objective. Motivation is not sufficient to actually use condoms, as self-regulatory processes are needed to translate motivation into action. Buying condoms and carrying them constitute preparatory behaviors that may serve as proximal predictors of action. Whether or not such preparatory behaviors operate as mediators between intention and action within a broader behavior change framework has been examined. Method. A sample of 150 heterosexual men between ages 18 and 25 years responded at three points in time to a computer-based survey that assessed behavior as well as social-cognitive antecedents. A structural equation model was specified that included preparatory behaviors and self-efficacy as mediators at Time 2. Results. Preparatory behaviors were the most proximal predictors of condom use, and they were, themselves, predicted by self-efficacy and intention. The latter was partly determined by positive emotional outcome expectancies. Conclusion. To bridge the intention-behavior gap, preparatory behaviors play a mediating role, and they represent a side of planning that constitutes the most proximal predictor of condom use.
To prevent infectious sexual diseases (ISDs), condom use has been identified as an appropriate strategy. Motivation for using condoms is a prerequisite of such behavior. However, a good intention is not always translated into action, and therefore, a mediating role of preparatory behaviors has been suggested in previous studies. Buying condoms and carrying them have proven to be essential steps to be taken before actual use (Bryan, Fisher, & Fisher, 2002; van Empelen, & Kok, 2006, 2008). A meta-analysis has concluded that preparatory behaviors (e.g., carrying a condom or having a condom available) were associated with medium to large effect sizes in the prediction of condom use (Sheeran, Abraham, & Orbell, 1999). In these studies, intentions to use condoms by themselves did not appear to affect condom use, unless the intentions were associated with preparatory behaviors, such as buying or carrying condoms. Thus, studies that focus entirely on intentions for condom-use prediction may be missing important aspects of the process of moving from intentions to actual behavioral change (Lewis, Kaysen, Rees, & Woods, 2010). The present study further examines the mediating role of such behaviors within the context of a larger framework of health behavior change.
Sexual Risk Behavior and Condom Use
Condoms are one mechanism by which to prevent the transmission of HIV (Malcolm et al., 2013), and recent advances in knowledge involve harnessing the behavioral and social sciences to promote improved frequency of condom use. Young men are often motivated to use condoms; however, in practice, they fail to act in accordance with their intentions, because in the heat of the moment, the motivation to prevent sexually transmitted infections becomes secondary (Albarracín et al., 2005). There is a need to ensure that accurate messages are delivered about safer sex and condom use to this vulnerable group (East, Jackson, O’Brien, & Peters, 2007).
Changing health behaviors may be based on models that make assumptions about the interplay of psychological constructs. One of these assumptions is related to the prominent role of intention in health behavior change. The main determinants of health behaviors focus primarily on motivational factors, such as beliefs, attitudes, and personal vulnerability, and these determinants affect behavior through the mediation of a behavioral intention. Hence, several health behavior models converge on the idea that intention is the most proximal cause of behavior (Armitage & Conner, 2000). However, change involves more than an intention, and this is empirically revealed by what is acknowledged in the literature as the intention-behavior gap; that is, successful changes in intention engender only small to medium change in behavior (Webb & Sheeran, 2006). Therefore, motivational models provide only a partial account of how motivation is translated into action.
A model that attempts to explain the mechanisms that operate after individuals have formed an intention to change their behavior is the health action process approach (HAPA; Schwarzer, 2008) that explicitly includes post-intentional factors.
The HAPA
In the HAPA, the social-cognitive factors in changing health-related behaviors are organized as two distinct phases, one conducive to a behavioral intention, a pre-intentional phase, and the other leading to actual behavior, a post-intentional phase (see Figure 1). People first need to become motivated. Perceived risk, outcome expectancies, and perceived self-efficacy are responsible for the development of an intention to refrain from a risk behavior or to adopt a health behavior. Second, in order to change, the individual needs self-regulatory effort before taking action and maintaining such changes. Planning, action control, and perceived self-efficacy to overcome barriers and to recover from setbacks are the main variables proposed to explain the translation of intention into action. Risk perception is seen as a distal antecedent of the motivation to change but is insufficient to enable a person to form an intention if not accompanied by outcome expectancies and self-efficacy (Schwarzer, 2008).
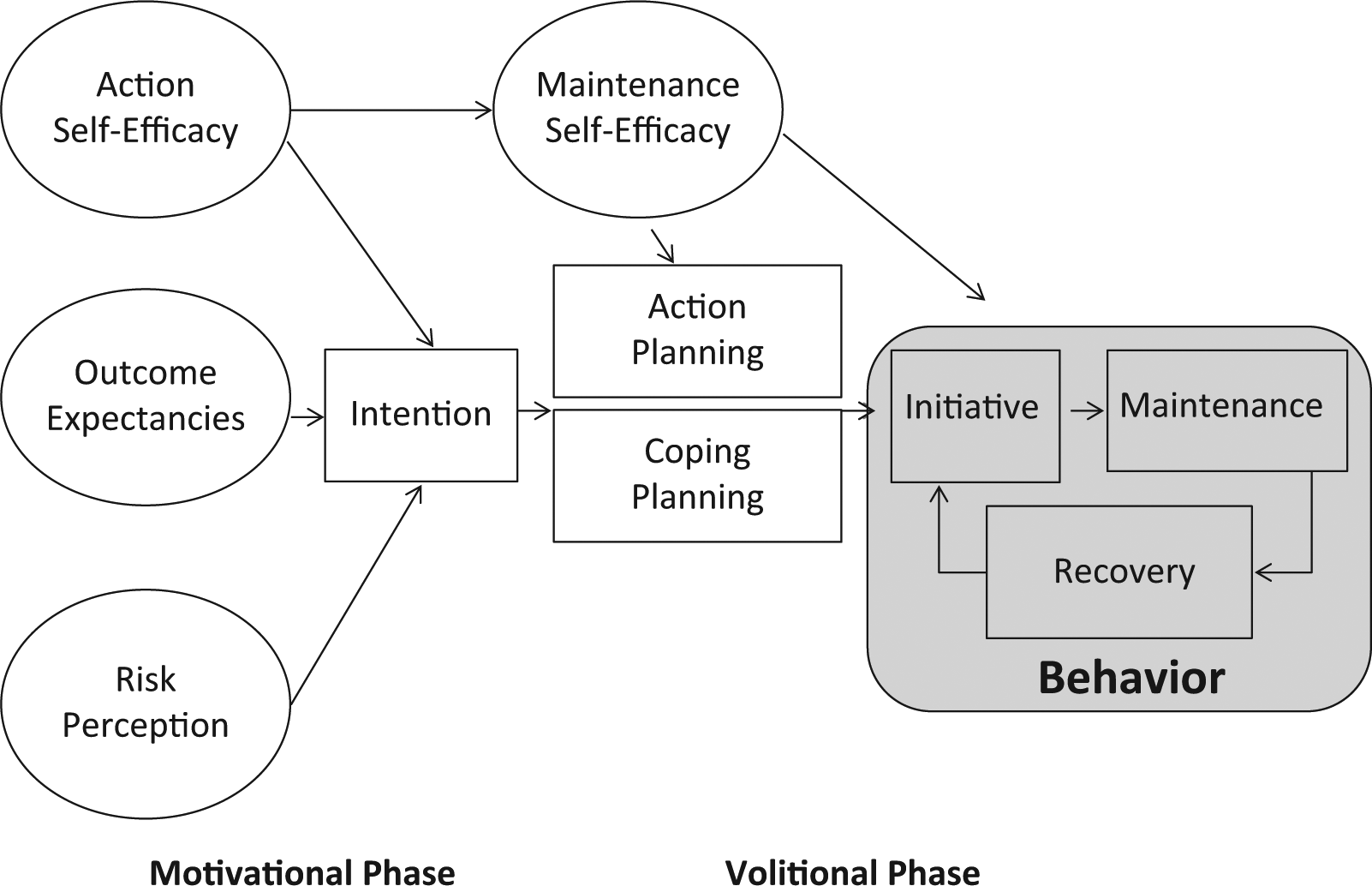
Health action process approach (HAPA) model.
Outcome expectancies may be positive or negative (pros and cons) and can be divided into the social, physical, and emotional. The positive emotional outcome expectancies are particularly supposed to facilitate intention formation (Schwarzer, 2008).
Perceived self-efficacy refers to individuals’ optimistic self-beliefs in their abilities to control challenging demands and is influential at all stages of the behavior change process (Bandura, 1997). Therefore, stage-specific adaptations of the wording of self-efficacy measures are useful. For instance, maintenance self-efficacy refers to the perceived ability to maintain a newly adopted behavior and cope with unexpected barriers during the maintenance phase of behavior (Luszczynska & Schwarzer, 2003).
Planning is an important step in the creation of conditions for initiating behavior and includes specific plans on when, where, and how to perform the behavior; the anticipation of barriers; and the design of alternative actions that may help to attain one’s goals despite barriers. As such, planning serves as an operative mediator between intentions and behavior (Koring et al., 2012).
Self-regulatory constructs other than planning and self-efficacy might help to further explain post-intentional processes of health behavior change. For instance, action control, an in situ self-regulatory strategy that enables the comparison of actual behavior with one’s own standards, has been found to improve the predictive value of the model in some cases (Sniehotta, Scholz, & Schwarzer, 2005). Research on the interplay of the different underlying self-regulatory mechanisms has also improved the predictive value of the HAPA, and condom use has been found to depend on planning, mainly in self-efficacious men (Teng & Mak, 2011).
The development of self-regulatory skills plays a major role in the adoption and maintenance of behavior. For condom use, one of the most important self-regulatory strategies is the performance of preparatory behaviors, which implies a sequence of actions, such as purchasing and carrying condoms, thus increasing individuals’ control over condom use (Bryan et al., 2002).
Predictors of Condom Use: The Role of Preparatory Behaviors
Several behavior change models have conceptualized predictors of condom use (Albarracín, Johnson, Fishbein, & Muellerleile, 2001). One meta-analysis concluded that three preparatory behaviors were among the strongest determinants of condom use: purchasing condoms, having them available, and discussing condom use with a sexual partner (Sheeran et al., 1999). However, there appears to be a lack of studies investigating the applicability of both the pre-intentional factors, such as positive outcome expectations, and the post-intentional factors, such as preparatory behaviors, in condom use behavior. Sheeran et al. (1999) suggested that preparatory behaviors “emerge as medium-to-strong predictors of condom use” (p. 118), and some studies have tested the hypothesized mediational role of preparatory behaviors on condom use and have demonstrated that adolescents who intended to use condoms and prepared themselves to do so (buying, carrying, and discussing condom use with a sexual partner) were more likely to actually use condoms (Bryan et al., 2002; van Empelen & Kok, 2006, 2008; Gebhardt, Kuyper, & Dusseldorp, 2006; Zimmerman et al., 2007).
Our study expands these results, contributing to the understanding of the role of preparatory behaviors in the context of the HAPA model, one of the few models to incorporate volitional influences on behavior (Conner, 2008). Preparatory behaviors are, therefore, studied along with pre-intentional factors, such as outcome expectancies, as well as post-intentional factors, such as maintenance self-efficacy. Furthermore, data were collected at three measurement points in time, more suited to a mediation model of this type, in which preparatory behavior was assessed before condom use. This procedure was chosen over the more common two measurement points in time used in many longitudinal studies, where preparatory behavior and condom use are measured concurrently, such as in the studies of Bryan et al. (2002), Zimmerman et al. (2007), and van Empelen and Kok (2006, 2008).
Moreover, whereas inclusion of the planning construct has received significant empirical support (Schwarzer, 2008) and has been studied as a cognitive antecedent of action, actually buying condoms and having them available constitutes a preparatory behavior that might help initiate and maintain condom use, which, up to now, has been seldom studied as a salient aspect of planning. Planning, as a preparatory behavior, might facilitate the adoption of a health behavior, as barriers are minimized and cues to action are encountered more frequently (Koring et al., 2013).
Aims of the Study
The goal of the current longitudinal study was to test the mediational role of preparatory behaviors as a volitional factor between intention and condom use within the HAPA framework, using three measurement points in time, among a sample of heterosexual young men. We hypothesized that (a) outcome expectancies will be determinants of intentions to use condoms, (b) intentions and maintenance self-efficacy will be determinants of the performance of preparatory behaviors, and (c) preparatory behaviors will be the proximal determinant of condom use. The sample consisted of young men based on the premise that young men are particularly vulnerable to ISDs. Indeed, the Centers for Disease Control and Prevention (CDC) estimates that nearly half of the 20 million new ISDs in the United States occur among young people ages 15 to 24 years (CDC, 2013).
Method
Participants and Procedure
A total of 470 sexually active young men, recruited in Portugal from several vocational training centers, participated in the study at Time 1 (T1). 1 To be eligible, they needed to be between 18 and 25 years of age and identify themselves as being heterosexual. At Time 2 (T2), the questionnaire was answered by 218 (46%) and at Time 3 (T3) by 150 men (32%). The present study includes only the longitudinal sample with 150 participants.
The mean age of the men was 19 years (SD = 1.71), and while 76% of them reported 10 to 12 years of schooling, 24% reported 9 years or less. The participants were mostly Portuguese (87.3%); some were African (6.7%), Brazilian (2.7%), or from other European countries (3.3%).
After participants had been notified of the aims of the study, they gave informed consent and completed the first computer-based questionnaire in class. The remaining two computer-based questionnaires were sent by e-mail, with 2-week intervals. All students were entitled to a raffle ticket for a gift check in return for their participation.
To increase adherence to all measurement points in time, we used a computer-based data collection procedure, based on the evidence that participants, when responding to a web questionnaire, as opposed to a paper-and-pencil questionnaire, are less biased by social desirability (Gosling, Vazire, & Srivastava, 2004). The study was approved by the ethics committees of the institution involved.
Measures
Focus groups were conducted in a previous study, prior to the construction of the questionnaire, and items were adapted in terms of the language, cultural characteristics, and age of the men.
Outcome expectancies, intention, maintenance self-efficacy, preparatory behaviors, condom use, and social desirability were assessed using 6-point Likert scales ranging from 1 (strongly disagree) to 6 (strongly agree).
In the same manner as other health behaviors have been measured (Schwarzer et al., 2007), condom use was assessed by two items at T1 and T3: “In the last month, how often have you always used a condom whenever you have had sexual intercourse (vaginal and/or anal)?” and “In the last month, how often was condom use part of your habitual sexual practices?” The internal consistency was α = .86 (T1) and α = .86 (T3).
Positive outcome expectancies of condom use were measured by four items at T1 (α = .77) (e.g. “When I use a condom, I feel safe”; “When I use a condom I feel that I’m protecting my partner”), emphasizing the emotional aspects of this behavior (Kelly, 1995; White, Terry, & Hogg, 1994).
Three items used to measure intention, adapted from Schwarzer (2008), were administered at T1 (α = .93), for example, “From now on, I intend to always use a condom,” and “ I intend to use a condom the next time I have sex.”
Maintenance self-efficacy was measured at T2 by seven items asking men to evaluate their confidence in maintaining condom use when faced with barriers, as mentioned in the literature on condom use (Kelly, 1995; White et al., 1994). Example items were “I think I can always maintain the use of condoms even if I am under the influence of substances (drugs and /or alcohol)” and “I believe I can maintain the systematic use of condoms, even if my partner is very attractive.” The internal consistency in the present study was α = .87.
Preparatory behaviors, such as buying and carrying condoms, were measured at T2 using three items adapted from Bryan et al. (2002): “I buy/acquire a condom when I expect the possibility of sex,” “I have a condom with me when sex is a possibility,” and “I keep condoms around whenever intercourse may occur.” The internal consistency in the present study was α = .93.
Given the sensitivity of the studied subject, social desirability was measured at T1 and used to inspect whether data collected on the other measures were associated with social desirability. The five-item Socially Desirable Response Set Survey (Hays, Hayashi, & Stewart, 1989) was used to assess the tendency to describe oneself in favorable terms. Responses above 5 indicate a tendency toward socially desirable responses in answering the questionnaire. The internal consistency in the present study was α = .69.
Data Analysis
Structural equation modeling with AMOS 19.0 (Arbuckle & Wothke, 1999) was performed using the maximum likelihood estimation. The model fit was assessed by examining the χ2, χ2/df, comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the Tucker-Lewis Index (TLI). A satisfactory model fit is indicated by χ2/df (<2), a high CFI and TLI (>.90), and a low RMSEA (<.08) (Tabachnick & Fidell, 2001). The model was specified with condom use at baseline as a predictor of all variables.
Results
Dropout Analysis
To examine whether the longitudinal subsample was representative of the initial sample, the T1 answers of the participants who completed all three questionnaires (n = 150) were compared to those who did not (n = 320). No significant differences were found regarding age, educational level, nationality, type of relationship in which they were involved, type of relationship at the time of the first act of intercourse, and condom use at baseline. There was a difference only in the age at the point of first intercourse, χ2(2) = 22.47, p < .01. Participants who completed all three questionnaires had their first act of intercourse later (>17 years old) than those who did not complete the three questionnaires (<17 years old).
Preliminary Analysis
A confirmatory factor analysis of the measurement model revealed that the original structure was maintained in the present sample, χ2(173) = 268.13, χ2/df = 1.52, CFI = .97, TLI = .95, RMSEA = .06. All factor loadings were higher than .50.
Main Results
All participants had already had sexual relationships, and 16% of them had had their first intercourse at age 14 or earlier, 43% at age 15 or 16, and 41% at age 17 or later. Six was the mean number of lifetime partners reported. Participants at T3 were in a steady (51%), casual (15%), or both types of relationships (15%), and 19% were involved in none. However, during the period under review, they were sexually active. Twelve percent of the sample did not report using condoms at all in the past month, at baseline.
In Table 1, the means and standard deviations are presented as well as the correlations for the latent variables outcome expectancies, intentions, and behavior at T1; maintenance self-efficacy and preparatory behavior at Time 2; and condom use at Time 3. All correlations among variables were significant, with the exception of social desirability. Apart from past behavior, the highest correlation emerged for preparatory behavior and condom use.
Correlations of Latent Variables.

Note. T1 = Time 1; T2 = Time 2; T3 = Time 3.
p < .05. **p < .01.
In the model, preparatory behavior was specified as a predictor of condom use. It was hypothesized that intentions and maintenance self-efficacy would predict preparatory behavior and that maintenance self-efficacy would have an indirect effect on behavior through preparatory behavior (Figure 2). The fit indices confirmed that the model represented the data appropriately, χ2(180) = 280.44, χ2/df = 1.55, CFI = .95, TLI = .94, RMSEA = .06.

Structural equation model with standardized parameter estimates.
Outcome expectancies, β = 0.24, p < .05, were a predictor of intentions and accounted for 44% of the variance in intentions. The direct path from intentions to condom use proved not to be significant, β = 0.14, p = .10, which indicates a full mediation by preparatory behavior.
As shown in Figure 2, intentions predicted preparatory behaviors, β = 0.33, p < .01, whereas preparatory behaviors predicted condom use, β = 0.24, p < .01. The indirect effect of intention on behavior through preparatory behavior was β = 0.08 (ZSobel = 2.32, p = .01). Maintenance self-efficacy, in turn, was a predictor of preparatory behavior, β = 0.29, p < .01, but was not a predictor of condom use, β = −0.14, p = .31. The indirect effect of maintenance self-efficacy on behavior through preparatory behavior was β = 0.06 (ZSobel = 2.32, p = .01). With baseline behavior included, the model explained 64% of the condom-use variance, while without the baseline, it explained 40% of condom-use variance.
Discussion
The present study has examined the mediational role of preparatory behaviors as a volitional factor between intention and condom use within the HAPA framework, among a sample of heterosexual young men. The model provides a good fit to the longitudinal data. It was shown that (a) positive outcome expectancies were determinants of intentions to use condoms, (b) intentions and maintenance self-efficacy were determinants of the performance of preparatory behaviors, and (c) a post-intentional volitional factor, namely, preparatory behaviors, predicted condom use.
Intention and maintenance self-efficacy were shown to predict condom use through preparatory behaviors. Consistent with previous research (Sheeran et al., 1999), these findings suggest that these variables are proximal predictors of condom use in heterosexual young men. Given that outcome expectancies were a powerful predictor of intention, results also suggest that in order to successfully persuade individuals to use condoms, presenting and emphasizing the positive emotional outcomes of safer sex may be effective in increasing condom use.
Maintenance self-efficacy seems to play an important role in the performance of preparatory behaviors for condom use also. Within the context of this model, maintenance self-efficacy functioned as an indirect factor through which preparatory behaviors exerted their influence on condom use. This construct emphasizes the confidence in dealing with difficulties when preparing or executing an action. High confidence in the ability of condom use encourages people to try harder to come up with more strategies when one strategy fails (Teng & Mak, 2011). In order to change habitual behavior and condom use, active self-regulation is necessary since the habits to be overcome are strongly elicited by situational cues (Sutton, 1994). From this stance, the perceived ability to maintain one’s behavior mirrors an optimistic belief in competent self-regulation. The effect of maintenance self-efficacy on preparatory behavior is, therefore, in line with these considerations.
The proposed model provides a possible explanation of pathways to condom use among heterosexual young men, underscoring the findings by Teng and Mak (2011) that the HAPA could be applied successfully to condom use in homosexual men. Nevertheless, it would be useful to replicate the present findings in other samples beyond heterosexual young men, for example, in men who have sex with men. The relevance of preparatory acts may also be generalized to other health behaviors, as Koring et al. (2013) found that the acquisition of a pedometer represents a preparatory behavior that also facilitates physical activity.
There are a number of approaches to promote condom use among people at high risk of sexual transmission of HIV, namely, individual-level interventions and group-level interventions. These interventions directly address knowledge, attitudes, skills, and behaviors related to condom use (e.g., Noar, 2008), and some emphasize preparatory behaviors. Objective measures of condom availability have proven to be associated with increased condom use (CDC, 1999). Our findings, in turn, confirm that it is important to assess preparatory behaviors and examine the mechanisms involved in the self-regulatory sequence leading from goal setting to goal pursuit. The findings also suggest some general guidelines for the design of educational interventions to promote condom use among sexually active young men. Such interventions should increase positive emotional expectancies associated with condom use and target volitional self-efficacy beliefs, since they have proven to facilitate intention formation and preparatory behaviors. These interventions should also ensure that young men not only are motivated to use condoms but also to plan to do so, through buying and carrying them, given the mediational role of preparatory behaviors found in the study.
Some limitations need to be addressed. First, condom use was measured by self-reports only, which may have been biased by social desirability. However, the average rate of social desirability in our study was not very high, and it is consistent with the idea that high desirability is not associated with condom use (Teng & Mak, 2011). Second, the results should be generalized with caution, due to the specific sociocultural characteristics of the participants (e.g., low level of education). Future studies should include more representative samples of young men to test the universality of the mechanisms found in this study. A third limitation stems from the high dropout rate, which was perhaps due to the lack of financial compensation. Although the high attrition rate was high, it is close to the average 40% response rate that was identified in a meta-analysis on Internet-based studies (Cook, Heath, & Thompson, 2000). Furthermore, participants in the longitudinal sample did not differ from those who had filled out only the first questionnaire, with the exception of the age at first intercourse. However, there may always be differences in relevant unmeasured variables. For example, analyzing the role played by substance abuse and relationship status might have revealed relevant associations among the present model variables.
Nevertheless, the innovative aspect of the current study lies in the evaluation of the HAPA model for condom use in young heterosexual men. Findings contribute to the understanding of the role of preparatory behaviors in the context of this process model that incorporates motivational and volitional influences on behavior.
The act of buying condoms and having them on hand at the time of intercourse are preparatory behaviors that one must carry out for condom use to occur. Thus, enacting preparatory behaviors may be considered necessary in order to facilitate the desired behavior. The findings point to the convenience of assessing preparatory behaviors and of examining the mechanisms that are involved in the self-regulatory sequence leading from goal setting to goal pursuit. Preparatory action, reflecting initiative, has been neglected in most health behavior theories, although it constitutes an obvious proximal predictor of action. Interventions may well have succeeded in motivating individuals to prepare for action; however, this positive effect has remained invisible, as only target behaviors have been assessed, failing to include such antecedents as useful indicators of treatment success. For practitioners, this study may also facilitate HIV prevention strategies to equip young men with the necessary skills (e.g., to increase confidence in dealing with difficulties in condom use and to plan how and when to purchase and carry condoms) to effectively mitigate many of the condom-use barriers. Further research and practice, therefore, should consider preparatory action as one of the aims and outcomes of interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.