
Abstract
Background. The family and home environment is an influential antecedent of childhood obesity. The purpose of this study was to pilot test The Enabling Mothers to Prevent Pediatric Obesity through Web-Based Education and Reciprocal Determinism (EMPOWER) intervention; a newly developed, theory-based, online program for prevention of childhood obesity. Method. The two-arm, parallel group, randomized, participant-blinded trial targeted mothers with children between 4 and 6 years of age. Measures were collected at baseline, 4 weeks, and 8 weeks to evaluate programmatic effects on constructs of social cognitive theory (SCT) and obesity-related behaviors. Process evaluation transpired concurrently with each intervention session. Results. Fifty-seven participants were randomly assigned to receive either experimental EMPOWER (n = 29) or active control Healthy Lifestyles (n = 28) intervention. Significant main effects were identified for child physical activity, sugar-free beverage consumption, and screen time, indicating that both groups improved in these behaviors. A significant group-by-time interaction was detected for child fruit and vegetable (FV) consumption as well as the SCT construct of environment in the EMPOWER cohort. An increase of 1.613 cups of FVs (95% confidence interval = [0.698, 2.529]) was found in the experimental group, relative to the active control group. Change score analysis found changes in the home environment accounted for 31.4% of the change in child FV intake for the experimental group. Conclusions. Child physical activity, sugar-free beverage consumption, and screen time improved in both groups over the course of the trial. Only the theory-based intervention was efficacious in increasing child FV consumption. The EMPOWER program was robust for inducing change in the home environment leading to an increase in child FV intake (Cohen’s f = 0.160).
Keywords
Obesity affects children worldwide and remains a formidable public health challenge (World Health Organization, 2000). Interventions for preventing childhood obesity have been implemented in a variety of environmental contexts, generally producing small to medium effects (Cook-Cottone, Casey, Feeley, & Baran, 2009; Waters et al., 2012). The family and home milieu is an influential, etiological antecedent of childhood obesity (Tabacchi, Giammanco, La Guardia, & Giammanco, 2007). Parents and family play a salient role in instilling healthy attitudes and behaviors for physical activity and nutrition in young children (Berry et al., 2004). Psychosocially, these factors are cultivated through vicarious learning and environmental determinants, such as resource availability and accessibility (Arredondo et al., 2006).
A systematic review of family- and-home-based childhood obesity programs identified four salient barriers confronting advancement of this stream of intervention: (a) indeterminant efficacy of theory-based, family- and-home-based interventions; (b) deficit in theoretical construct measurement; (c) lower program participation and higher attrition rates; and (d) absence of intervention process evaluation (Knowlden & Sharma, 2012a, 2012b). The Enabling Mothers to Prevent Pediatric Obesity through Web-Based Education and Reciprocal Determinism (EMPOWER) trial was designed to begin addressing these deficiencies. The purpose of this study was to detail the efficacy of the randomized control trial and to describe the capacity of EMPOWER to address the four identified barriers.
Method
Study Design
The EMPOWER trial was a two-arm, parallel group, randomized, participant-blinded trial conducted online at the University of Cincinnati, Ohio, United States. Study methods have been detailed in a published protocol (Knowlden & Sharma, 2012b). There were no major deviations from the published study protocol.
Participants
Within the context of the home environment, parents are hypothesized to be the primary facilitators of behavior change in children. Based on prior family- and-home-based childhood obesity research, mothers were selected as the agents of change for the pilot study (Ayala et al., 2010; Brophy et al., 2009; Clark, Goyder, Bissell, Blank, & Peters, 2007; Harvey-Berino & Rourke, 2003; Jain et al., 2001). Children between 4 and 6 years were targeted because health behaviors in this age range have been found to be a strong predictor of future health (Brophy et al., 2009; Gardner et al., 2009).
A single cohort of 57 eligible participants was recruited in February 2013. Mothers were recruited by posting flyers that advertised the program in participating preschools, day cares, and health care organizations. Training in the use of technology was not provided for this program. Subsequently, enrollment was conducted online to ensure participants possessed sufficient technology skills to adequately engage in a fully online program. As part of the enrollment process, interested participants first watched an introductory video that explained the purpose of the study, the composition of the two programs, the timeframe of the study, and the total estimated time for program completion. Next, interested participants completed an online, prescreening questionnaire that ensured they were eligible for the study. Eligibility was limited to English-speaking mothers with Internet access, e-mail, an accessible telephone, and at least one child in the age range of 4 to 6 years. Exclusion criteria included pregnant mothers, mothers with a child in the age range of 4 to 6 years with a disability that would interfere with engagement in daily physical activity, a child with a medical condition associated with weight gain, a child prescribed medication associated with weight gain, and/or a child currently enrolled in a weight management program. Participants with more than one child in the age range of 4 to 6 years were requested to complete the intervention in reference to their oldest child. After prescreening, eligible participants were directed to sign a consent form that detailed their rights and described that they would be randomly assigned to either the experimental or active control program. Finally, eligible, consenting participants completed baseline measurement and were randomly assigned to either the EMPOWER or Healthy Lifestyles intervention. The assignment protocol was based on simple randomization, with assignments selected using a random group assignment generator created in Microsoft Excel 2010. The first author was responsible for generating the random allocation sequence, enrolling participants, and assigning participants to the interventions. Participants were blinded as to which cohort they were assigned to strengthen internal validity.
Interventions
Design for both interventions has been previously detailed (Knowlden & Sharma, 2012b; Knowlden & Sharma, 2014). Briefly, the EMPOWER trial contained two intervention arms: a social cognitive theory (SCT)-based program (experimental arm) and a knowledge-based program (active control arm). Both interventions were conceptualized and designed by the authors to assist mothers in helping children achieve four behaviors posited to contribute to primary prevention of childhood obesity: (a) 120 minutes of daily, structured and unstructured physical activity; (b) daily consumption of five cups of fruits and vegetables; (c) substitution of sugar-sweetened beverages with sugar-free beverages; and (d) restriction of screen time (sedentary time spent in front of a television, computer screen, or portable electronic device) to no more than 120 minutes per day (National Association for Sport and Physical Education, 2002; Rao, 2008). Both interventions were composed of five educational sessions, with one session dedicated to each child behavior. Between posttest and follow-up measurement, a comprehensive booster session was delivered. Educational modalities for each session included a 10- to-15-minute audiovisual presentation, an interactive worksheet, and a discussion board post. Process evaluation data were collected after each session using telephone counseling and online surveys.
EMPOWER Program
The EMPOWER program (Knowlden & Sharma, 2012b) was designed to reify and improve five SCT constructs in mothers: environment, emotional coping, expectations, self-control, and self-efficacy (Bandura, 1986, 1989, 1998, 1999, 2004; Baranowski, Cullen, Nicklas, Thompson, & Baranowski, 2003; Birch, 1998; Galloway, Fiorito, Francis, & Birch, 2006; Hearn et al., 1998). Improvement of these constructs in participating mothers was posited to change the four child behaviors prioritized in this trial.
For reifying the environment construct, methods for role modeling each of the child behaviors, the significance of home-based engagement in promoting each of the child behaviors, and methods for constructing a home environment conducive to encouraging the child behaviors were provided (Arredondo et al., 2006). For example, intervention objectives for mediating change in the maternal-facilitated environment for child fruits and vegetables construct focused on the importance of maternal role modeling of fruit and vegetable consumption and creating a home environment conducive to child consumption of fruits and vegetables.
For reifying the emotional coping construct, mothers were informed that stress may accompany adoption of each of the four behaviors in their children (Birch, 1998). Subsequently, emotional coping strategies applicable to each of the child behaviors were provided to counteract potential distress (Bandura, 2004; Galloway et al., 2006). For example, intervention objectives for mediating change in the maternal-facilitated emotional coping for child physical activity construct focused on the importance of adopting enjoyable parent–child structured physical activities, involving the child in the decision-making process related to activity adoption and development, and applying verbal reinforcement to reduce stress associated with increases in child physical activity.
In reifying expectations, behavioral objectives for each of the child behaviors were defined and the associated health benefits of achieving the objectives were described (Bandura, 2001; Resnicow et al., 1997). For example, intervention objectives for mediating change in the maternal-facilitated expectations for child physical activity construct in the experimental group centered on personalizing health benefits of a child achieving adequate physical activity, the importance of instilling healthy attitudes toward physical activity in children at a young age, and how the physical activity health behaviors children acquire at a young age tracks with them into adolescence and adulthood.
Procedures for increasing self-control focused on assisting participating mothers in developing goals and plans for achieving each of the child behaviors (Baranowski et al., 2003). For example, intervention objectives for mediating change in the maternal-facilitated self-control for child sugar-sweetened beverages included developing plans and goals to replace sugar-sweetened beverages with sugar-free beverages. The self-efficacy construct was reified by reducing achievement of each maternal-facilitated child behavior into smaller, manageable, components. Strategies for increasing participant confidence in achieving each of the four maternal-facilitated child behaviors were also provided (Bandura, 2006; Corwin, Sargent, Rheaume, & Saunders, 1999). For example, intervention objectives for mediating change in self-efficacy for the experimental group focused on development and incorporation of unstructured physical activities.
Healthy Lifestyles Program
The Healthy Lifestyles program was a knowledge-based program (Knowlden & Sharma, 2012b). Health Lifestyles also prioritized the four child behaviors; however, the active control arm did not focus on modification of SCT constructs. Instead, the program centered on delivery of general health knowledge regarding the four behaviors. Audiovisual presentations complemented each module for the Healthy Lifestyles program, but did not include theory-based interactive components to induce behavior change. Interactive online worksheets and discussion board postings designed to increase knowledge supplemented each module. For example, intervention objectives for the child physical activity session included being able to define structured and unstructured physical activity. Additional intervention objectives included identifying four basic types of fruits and vegetables, distinguishing between sugar-sweetened and sugar-free beverages, and identifying mediums of screen time. Table 1 summarizes session topics, session durations, and sample objectives for the EMPOWER and Healthy Lifestyles interventions.
Session Topics, Session Durations, and Sample Objectives for the EMPOWER and Healthy Lifestyles Interventions.
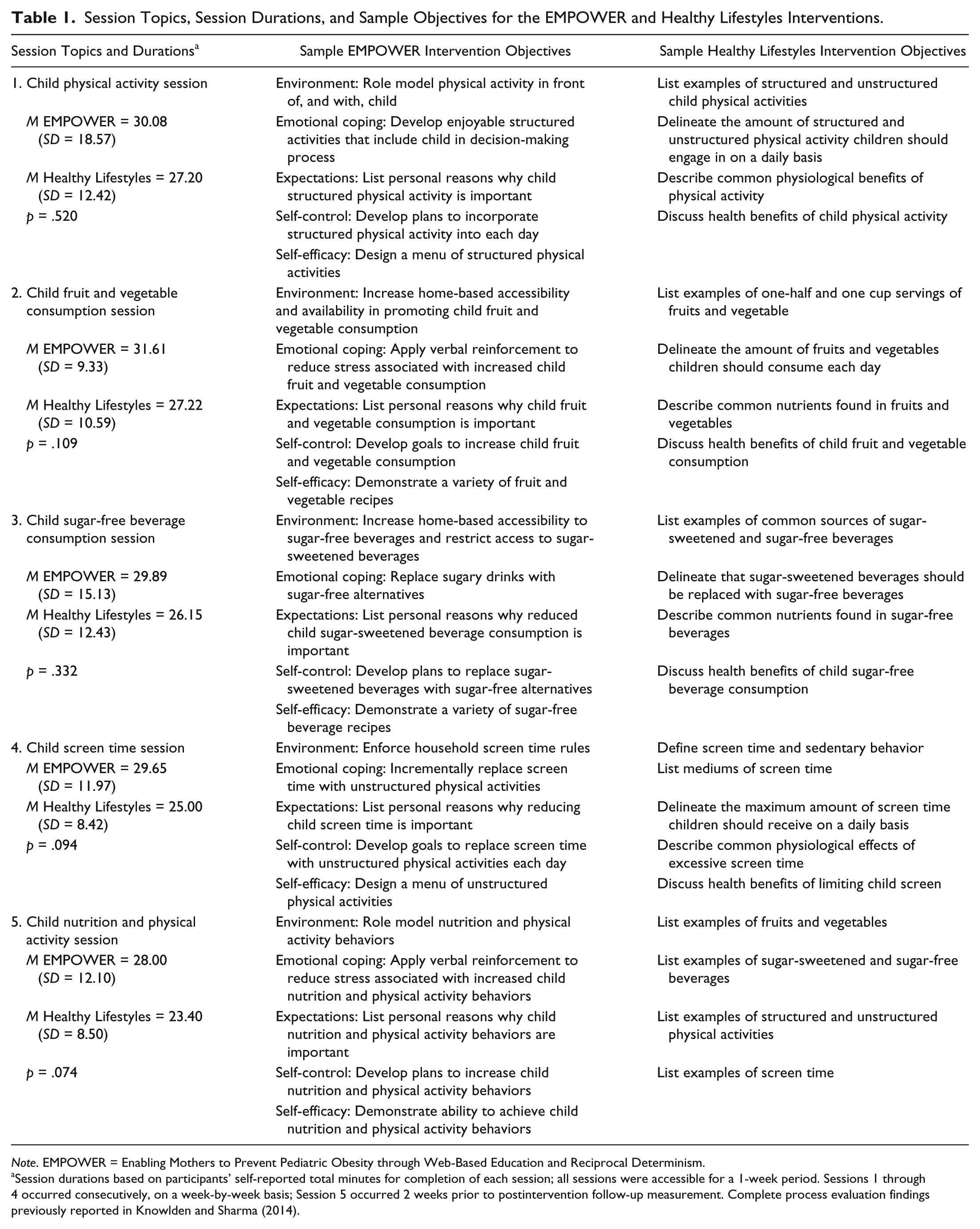
Note. EMPOWER = Enabling Mothers to Prevent Pediatric Obesity through Web-Based Education and Reciprocal Determinism.
Session durations based on participants’ self-reported total minutes for completion of each session; all sessions were accessible for a 1-week period. Sessions 1 through 4 occurred consecutively, on a week-by-week basis; Session 5 occurred 2 weeks prior to postintervention follow-up measurement. Complete process evaluation findings previously reported in Knowlden and Sharma (2014).
Outcome Measures
Outcome measures for the study included the following:
Four child behaviors associated with prevention of obesity: physical activity, fruit and vegetable consumption, sugar-free beverage consumption, and screen time.
Scores of five maternal-facilitated constructs of SCT: environment, emotional coping, expectations, self-control, and self-efficacy for each behavior.
Outcome measures were collected from both groups at baseline (March 2013), Week 4 at posttest (April 2013), and Week 8 at follow-up (May 2013), using an online version of a valid and reliable instrument developed for the study. Data for establishing instrument validity and reliability were collected prior to the trial, from a separate sample of 224 participants over three phases. Phase 1 of instrumentation encompassed face and content validity by a panel of six experts over two rounds. Phase 2 assessed test–retest reliability of the instrument by having the same group of participants (n = 31) complete the instrument two separate times with 2 weeks between administrations. Finally, construct and predictive validity of the instrument were evaluated at Phase 3 through structural equation modeling. Results suggested adequate convergent validity of the five-factor, SCT measurement models assessing instrument reliability. The ability of the measured constructs to account for variance in the four child behaviors ranged from 14% to 25%. Table 2 summarizes sample scale items, descriptive, reliability, and validity statistics of the instrument employed to measure the EMPOWER trial.
Sample Scale Items, Descriptive Statistics, Reliability, and Validity Statistics of the Instrument Employed to Measure the EMPOWER Trial.

Note. EMPOWER = Enabling Mothers to Prevent Pediatric Obesity through Web-Based Education and Reciprocal Determinism; CR = Composite reliability; AVE = Average variance extracted; Instrumentation conducted with a unique sample of mothers (n = 224) prior to beginning EMPOWER trial. To calculate a test–retest correlation coefficient, 31 respondents from the sample completed the instrument a second time, 2 weeks following the first administration.
Ethics
Reporting adhered to the Consolidated Standards of Reporting Trials (CONSORT) Statement (Rennie, 2001). The university institutional review board approved the study protocol with a status of minimal risk to participants. Consent was obtained from each participant prior to intervention delivery. To bolster commitment, a monetary incentive of US$55.00 was offered to participants that completed the full program.
Sample Size and Power
Based on previous studies, significance criteria were set at an alpha of 0.05, a power at 0.80, and an effect size at 0.20 (Collins et al., 2011; Okely et al., 2010). The number of groups was established at two and the number of measurements at three. Inputting these criteria into G*Power statistical power analysis software resulted in a total sample size of 42 (Faul, Erdfelder, Buchner, & Lang, 2009). Sample size was inflated by 35% to account for potential attrition, resulting in a total sample size of 57 (Warren et al., 2007).
Statistical Methods
Repeated measures models were used to determine the main effects attributed to differences by group (two levels), time (three levels), and the group-by-time interactions. Child behaviors were tested with repeated measures analysis of variance (ANOVA). SCT constructs were tested using repeated measures multivariate analysis of variance (MANOVA). Modeling tested whether the group-by-time interactions were significant as this would indicate groups performed differently over time. If results were nonsignificant, it was assumed that both groups had identical or near identical patterns over time. Post hoc analyses applying a Bonferroni adjustment for multivariate comparisons were conducted to identify differences in significant interactions and main effects. Cohen’s ƒ values were calculated using G*Power Version 3.1.2 to evaluate effect sizes for significant interactions and main effects. In interpreting f, Cohen’s (1988) criteria of 0.1 to 0.24 = small, 0.25 to 0.39 = moderate, and 0.4 to 1.0 = large effect sizes were applied. Data remained untransformed and all available data were used for analysis. Significance levels for rejecting null hypotheses were set a priori at p < .05.
Results
Participant Retention
Of the 61 respondents recruited, 4 were excluded from the trial for failing to meet the eligibility criteria. Among the remaining 57 consenting, eligible participants, 29 were randomly allocated to the experimental, EMPOWER intervention and 28 were randomly allocated to the active control, Healthy Lifestyles intervention. In total, 7 participants were lost to attrition over the course of the trial. Figure 1 illustrates the flow of participants through the randomized control trial.
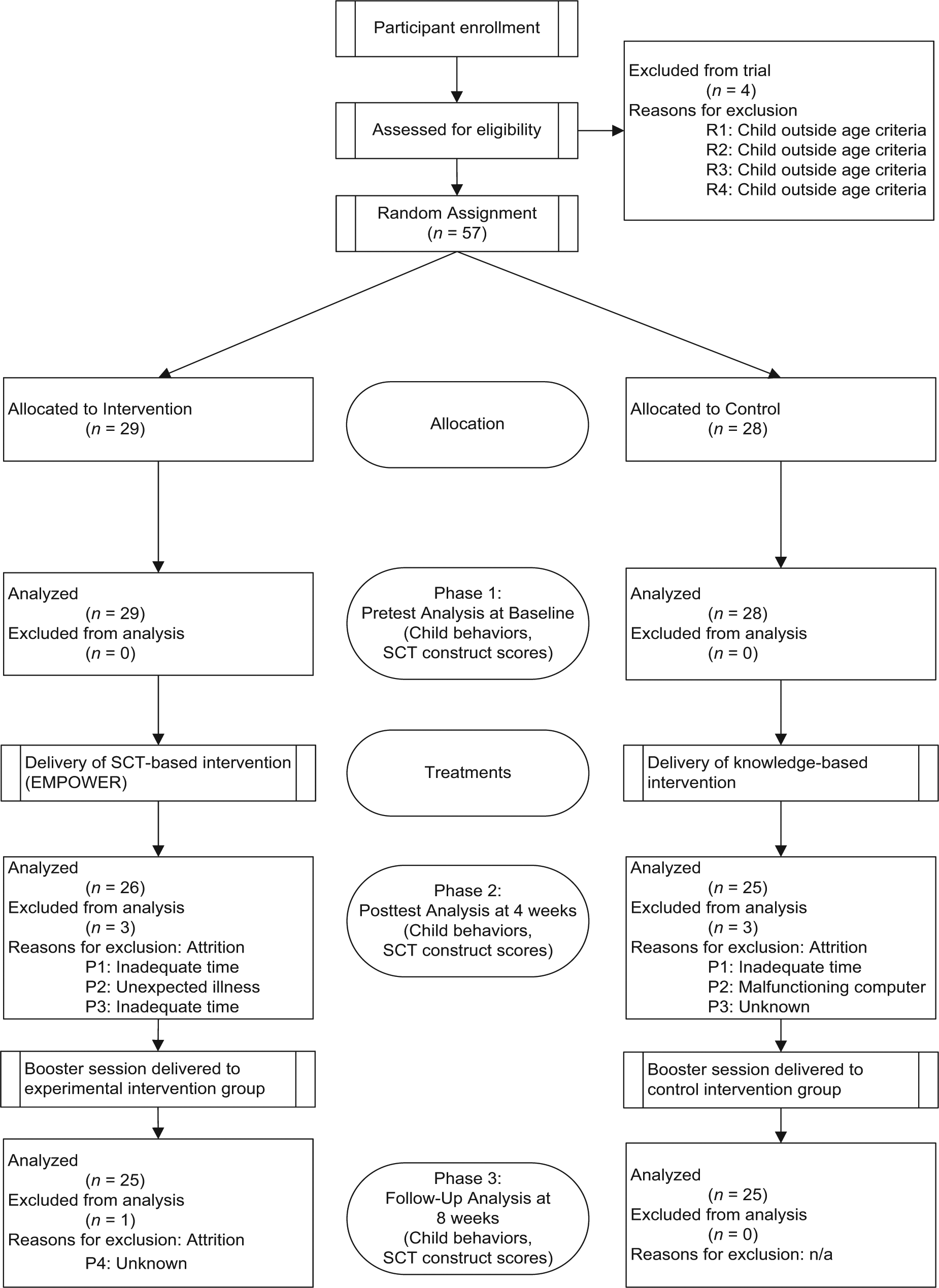
Flowchart of participants through the randomized control trial.
Baseline Assessment
Three layers of baseline analyses were conducted to determine pretest equivalency between the experimental and control groups. The first analysis modeled all continuous study and demographic variables with a one-way MANOVA. Results of the omnibus test indicated there were no between-group differences when all continuous variables were assessed simultaneously, F(27, 29) = 0.832, ΛPillai = .437, p = .683). The second analysis used one-way ANOVAs to model each continuous variable separately. Results of the analysis found no significant between-group differences. The final analysis modeled all categorical demographic variables with Fisher’s exact test and the chi-square test. Results found no significant between-group differences. Subsequently, it was determined that study hypotheses could be tested without controlling for covariates. Table 3 summarizes baseline demographics of the participants.
Comparison of Categorical Demographic Variables Between Participants in the Experimental (n = 29) and Control (n = 28) Groups Modeled with Chi-square Tests of Independence and Fisher’s Exact Test at Baseline.
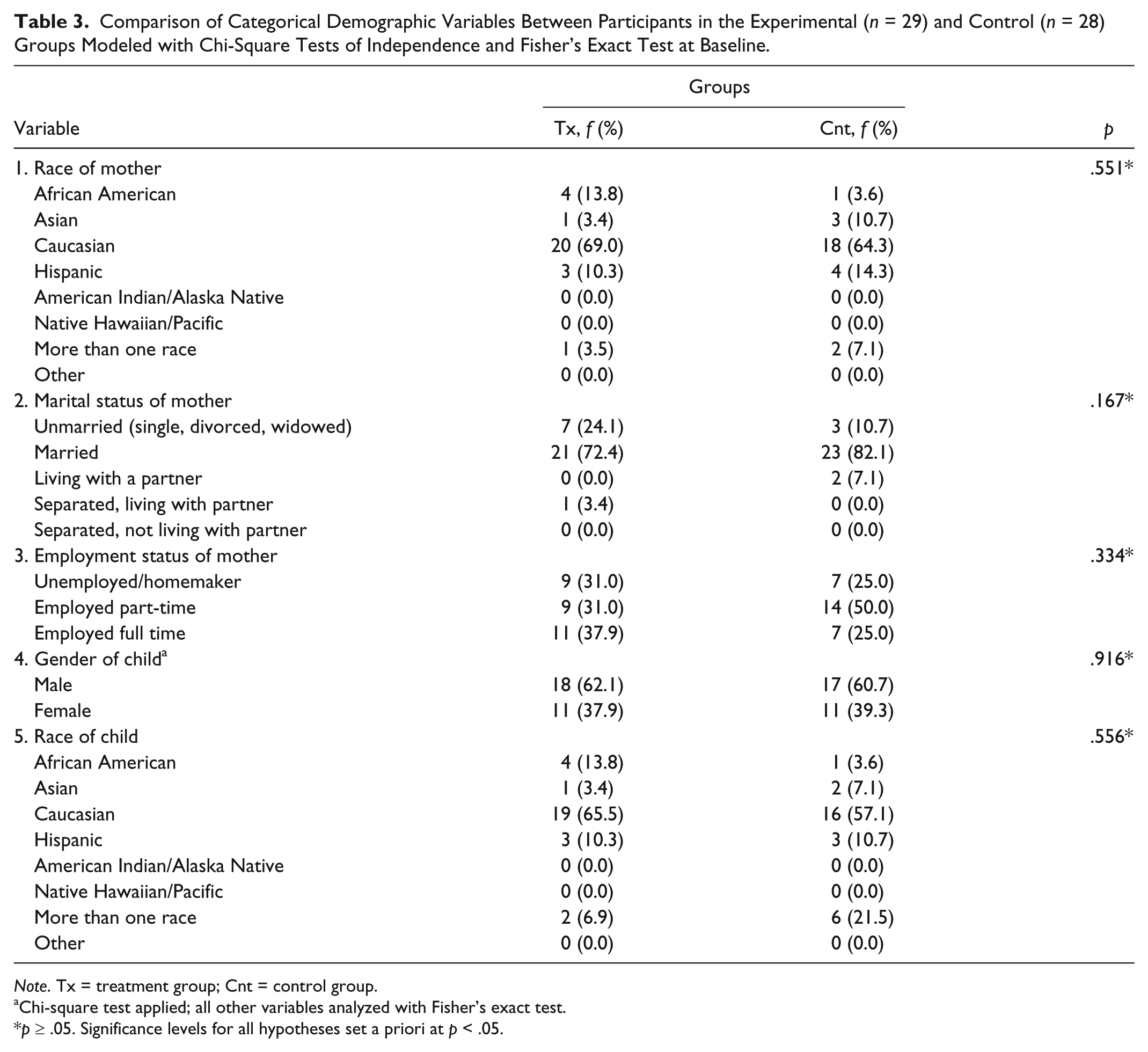
Note. Tx = treatment group; Cnt = control group.
Chi-square test applied; all other variables analyzed with Fisher’s exact test.
p ≥ .05. Significance levels for all hypotheses set a priori at p < .05.
Process Evaluation
To assess implementation accuracy of the two tested interventions, data for six measures of process evaluation were collected using telephone counseling and online surveys. Details of process evaluation have been described in detail elsewhere (Knowlden & Sharma, 2014). Measures included program fidelity, dose delivered, dose received, reach, recruitment, and context. Program implementation indexes indicated program fidelity, dose delivered, dose received (exposure), reach, and context exceeded the a priori 0.90 level of implementation excellence for both groups (Saunders, Evans, & Joshi, 2005). Dose satisfaction and recruitment time were evaluated through one-way ANOVA tests. Results indicated absence of statistically significant differences between the two groups for dose satisfaction, recruitment effort, and recruitment time. Overall, process evaluation results suggested that both programs were equivalent and administered as planned. Consequently, it was determined that hypothesis testing could ensue without accounting for programmatic differences.
Repeated Measures Analyses
Table 4 summarizes comparisons for the child behaviors and maternal-facilitated SCT constructs by group and by time for the sample of mothers.
Summary of Comparisons for All Maternal-Facilitated Social Cognitive Theory Constructs and Child Behaviors by Group and by Time for the Sample of Mothers.
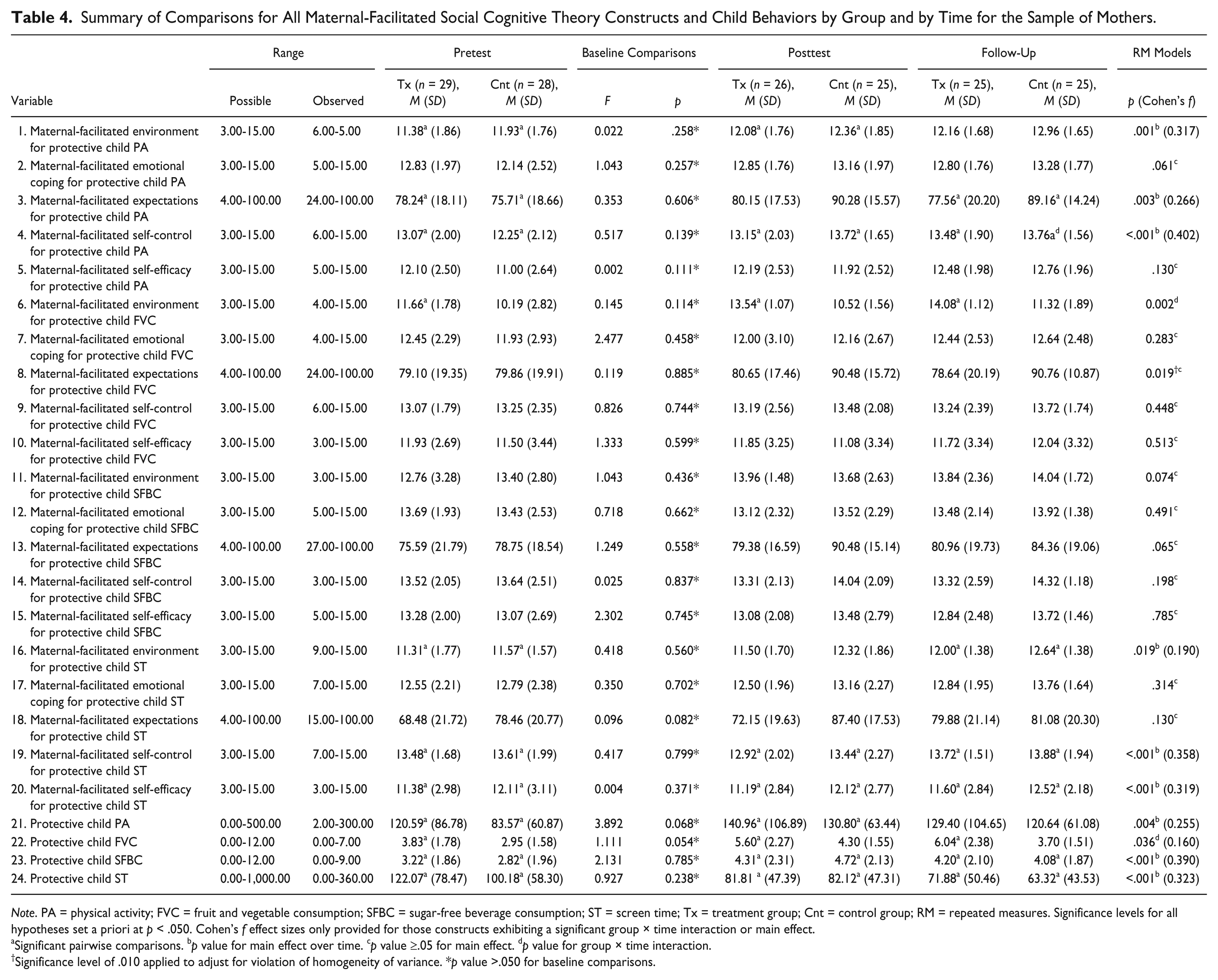
Note. PA = physical activity; FVC = fruit and vegetable consumption; SFBC = sugar-free beverage consumption; ST = screen time; Tx = treatment group; Cnt = control group; RM = repeated measures. Significance levels for all hypotheses set a priori at p < .050. Cohen’s f effect sizes only provided for those constructs exhibiting a significant group × time interaction or main effect.
Significant pairwise comparisons. bp value for main effect over time. cp value ≥.05 for main effect. dp value for group × time interaction.
Significance level of .010 applied to adjust for violation of homogeneity of variance. *p value >.050 for baseline comparisons.
Child Behaviors
Analysis of child fruit and vegetable consumption found baseline total cups increased in the experimental group at posttest (M experimental = 5.60, SD = 2.27) and continued to increase through postintervention follow-up (M experimental = 6.04, SD = 2.38). Alternatively, total cups increased in the control group at posttest (M control = 4.30, SD = 1.55) and then decreased at postintervention follow-up (M control = 3.70, SD = 1.51). Repeated measures ANOVA indicated the behavior changes were significant, eliciting a group-by-time interaction of small effect size (p = .036; Cohen’s f = .160). Post hoc analyses indicated that significant changes in the behavior occurred from pretest to posttest (p < .001) and from pretest to postintervention follow-up (p < .001), suggesting an increase of 1.613 cups (95% confidence interval [CI] = [0.698, 2.529]) in the experimental group, relative to the control group.
Analysis of child physical activity found baseline total minutes increased in both the theory-based and knowledge-based groups at posttest (M experimental = 140.96, SD = 106.89; M control = 130.80, SD = 63.44). This increase was sustained through postintervention follow-up (M experimental = 129.40, SD = 104.65; M control = 120.64, SD = 61.08). Behavior increases were not sufficient to elicit either a group-by-time interaction (p = .309) or a group main effect (p = .381); however, a main time effect of moderate size was detected (p = .004), implying a significant increase in child physical activity behavior for both groups. Post hoc analyses indicated that significant changes in the behavior occurred from pretest to posttest (p = .006) and then remained statistically static, suggesting an overall increase of 32.660 minutes (95% CI = [7.716, 57.604]) of child physical activity in both groups over the duration of the intervention.
Examination of child sugar-free beverage intake found baseline cups increased in both the theory-based and knowledge-based groups at posttest (M experimental = 4.31, SD = 2.31; M control = 4.72, SD = 2.13) and then slightly decreased at postintervention follow-up (M experimental = 4.20, SD = 2.10; M control = 4.08, SD = 1.87). Behavior changes were not sufficient to elicit either a group-by-time interaction (p = .252) or a group main effect (p = .989); however, a main time effect of moderate size was detected (p < .001), implying a significant increase in child sugar-free beverage intake for both groups. Post hoc analyses indicated that significant changes in the behavior occurred from pretest to posttest (p < .001) and from pretest to postintervention follow-up (p = .003), suggesting an overall increase of 1.070 cups of sugar-free beverages (95% CI = [0.324, 1.816]) in both groups over the duration of the intervention.
Analysis of child screen time found baseline total minutes decreased in both the theory- and knowledge-based groups at posttest (M experimental = 81.81, SD = 47.39; M control = 82.12, SD = 47.31). This decrease was sustained through postintervention follow-up (M experimental = 71.88, SD = 50.46; M control = 63.32, SD = 43.53). Behavior increases were not sufficient to elicit either a group-by-time interaction (p = .373) or a group main effect (p = .386); however, a main time effect of moderate size was detected (p < .001), implying a significant decrease in child screen time behavior for both groups. Post hoc analyses indicated that significant changes in the behavior occurred from pretest to posttest (p = .019) and from pretest to postintervention follow-up (p = .002), suggesting an overall decrease of 39.000 minutes (95% CI = [−65.164, −12.836]) of child screen time behavior in both groups over the duration of the intervention.
Maternal-Facilitated Constructs
Repeated measures MANOVA and ANOVA identified a significant univariate group-by-time interaction of moderate effect size for maternal-facilitated environment for child fruit and vegetable consumption (p = .002; Cohen’s f = .274). Post hoc analysis indicated that significant changes in the construct occurred at each of the three time levels, for an overall increase of 2.253 units (95% CI = [1.539, 2.967]) in the experimental group, relative to the control group (p < .001). There were no additional significant group-by-time interactions for the remaining maternal-facilitated SCT constructs (p > .05). Examination of time effects found significant improvements in both groups for the maternal-facilitated physical activity constructs of environment, expectations and self-control as well as the maternal-facilitated screen time constructs of environment, self-control, and self-efficacy (p < .05).
Change Score Analysis
A priori conditions limited change score analysis to those behaviors and SCT constructs found to have significant group-by-time interactions. Thus, analysis was limited to evaluating the predictive capacity of the environment construct to account for variance in child fruit and vegetable consumption in the EMPOWER group. In building the models, change scores in child fruit and vegetable consumption were regressed on the change scores in the environment across the three time levels. The first path model examining pretest to posttest changes (p = .191), as well as the second path model examining posttest to follow-up changes (p = .446), found no predictive relationship between the maternal-facilitated environment construct and child fruit and vegetable consumption. The third path model examining pretest to follow-up identified a significant direct path between changes in the environment construct and changes in child fruit and vegetable consumption (p < .001). The model examining pretest to follow-up suggested the change in environment accounted for 31.4% of the variance in the change in child fruit and vegetable consumption from pretest to follow-up.
Discussion
The purpose of the EMPOWER trial was to address salient design (efficacy of theory-based approaches), implementation (high attrition), and evaluation (construct measurement, fidelity) barriers confronting advancement of family- and-home-based childhood obesity interventions. Key study dependent variables included four child behaviors (physical activity behavior, fruit and vegetable consumption behavior, sugar-free beverage consumption behavior, and screen time behavior) and five maternal-facilitated constructs of SCT related to each behavior (environment, emotional coping, expectations, self-control, and self-efficacy).
To evaluate the efficacy of theoretical, family- and-home-based programs, a newly designed, experimental, theory-based intervention (EMPOWER) was compared against an active control, knowledge-based intervention (Healthy Lifestyles). Both arms of the trial demonstrated improvement in child physical activity, sugar-free beverage consumption, and screen time behaviors. Several potential explanations may account for the improvement in these behaviors. First, it is possible that an intervention effect could have occurred in both groups. Both intervention groups were provided with specified amounts of daily physical activity, sugar-free beverages, and screen time quantities required for prevention of childhood obesity. In the experimental group, theory-based approaches for accomplishing behavior change were provided, whereas in the control group only information about the importance of the behaviors was transmitted. However, both groups self-reported moderate to high levels of expectations, emotional coping, self-control, and self-efficacy at baseline for these behaviors (see Table 2). That both intervention arms demonstrated improvement in these behaviors suggests that even generalized, knowledge-based programs may be efficacious if adequate behavior change skills are present at baseline.
Additionally, seasonality may be partially responsible for the improvements in child physical activity and screen time behaviors, independent of any intervention effect (Tucker & Gilliland, 2007). Common environmental factors that can threaten an intervention’s internal validity include changes to the physical environment (i.e., seasonal changes that occur during and between measurement periods) and/or social environment (i.e., competing programs that directly or indirectly target similar behaviors). The most prominent change to the physical environment that occurred during the intervention was spring break. For some participants, spring break may have created a temporal anomaly in which their children were exposed to greater opportunities to engage in physical activity. Additionally, pretest measurement occurred in early March 2013. There were several bouts of inclement winter weather throughout the month of March for much of the Midwest (locale of most participants); whereas, by the posttest and follow-up measurement periods, the weather became warmer and more conducive to outdoor activity. Interventions that distinguish between self-efficacy for indoor and outdoor structured activity should be considered in future research. Furthermore, seasonality could be accounted for through long-term follow-up evaluation.
As EMPOWER and Healthy Lifestyles were targeted, rather than tailored interventions, their full utility may be more adequately gauged in populations that self-report lower SCT construct scores at baseline. Nevertheless, the pilot findings lend support for the home environment as an effective leverage point for prevention of childhood obesity. The theory-based, EMPOWER intervention was exclusive in demonstrating efficacy for improving child fruit and vegetable consumption. Analysis attributed a significant portion of this effect to the intervention, which bolsters empirical verification of the application of SCT-based interventions targeting child fruit and vegetable intake. Based on the change score analysis, a significant portion of the increase in child fruit and vegetable consumption was attributed to improvement in the environment construct. Subsequently, it can be concluded that reification of the maternal-facilitated home environment, from a social cognitive perspective, is beneficial for increasing child fruit and vegetable consumption.
To attenuate the gap in construct measurement for family- and-home-based theoretical interventions, five constructs of SCT were operationalized and measured in both interventions (Bandura, 2004). The instrument developed for this study demonstrated the utility of construct measurement for uncovering the source of intervention effects. Through operationalization of SCT, it was determined that a significant proportion of variance for the increase in child fruit and vegetable consumption was explained by changes to the maternal-facilitated home environment. The ability to attribute behavior changes to specific theoretical constructs removes ambiguity of outcomes and promotes evidence-based decision making.
Attrition rates have been a primary concern for family- and-home-based programs, typically falling between 20% and 50% (Warren et al., 2007). To determine the capacity of web-based programs for reducing attrition rates, both interventions were delivered online. The dropout rate for the EMPOWER trial was notably lower at 13.8% in the experimental and 10.7% in the control group, which lends credence to the flexibility of web-based interventions for targeting parents. To reduce the risk for committing type III errors, six measures of process evaluation were collected over the course of the trial (Basch, Sliepcevich, Gold, Duncan, & Kolbe, 1985; Glasgow, Magid, Beck, Ritzwoller, & Estabrooks, 2005). Results suggested that both programs were equivalent and administered as planned (Knowlden & Sharma, 2014). The average time spent completing the entire EMPOWER (experimental) intervention was 149.21 minutes. The average time spent completing the full Healthy Lifestyles (control) intervention was 127.50 minutes. These durations were near the estimated dose of 2.5 hours (150 total minutes; approximately 30 minutes per session), set for the program.
Limitations
Several limitations must be considered in interpreting the results of this study. The home environment was operationalized through three items querying availability and accessibility to fruits and vegetables. The home environment for nutrition is multifaceted and it may not be feasible to measure such a complex milieu with only three items. As the current study was a pilot investigation, instrument parsimony was desired. Because of the density of the home environment for promoting child fruit and vegetable consumption, inclusion of additional items is recommended for future research, particularly for interventions seeking to emphasize the home environment (Spurrier, Magarey, Golley, Curnow, & Sawyer, 2008).
The instrument measuring maternal-facilitated environment for child fruit and vegetable consumption construct combined aspects of the physical and social environment (Hearn et al., 1998). Future studies should consider dichotomizing physical and social aspects of the environment to evaluate the individual effects of these two components. The influence of environment could be further enhanced by requesting mothers to self-report their own fruit and vegetable intake. Correlations between mother and child fruit and vegetable consumption would be beneficial for modeling vicarious learning (Goldman, Radnitz, & McGrath, 2012).
Data were collected through self-report and the time frame for evaluation was relatively short. Future research should incorporate objective measures, such as body mass index, and longer evaluation periods to fully assess the prevention capacity of online, family- and-home-based interventions. Because of the length of the instrument, education level and income data were not collected from participants. Future research should request these demographic data, as both are established confounders of obesity interventions. Despite these measurement limitations, the instrumentation process was rigorous and included several layers of validity and reliability testing. The mean time for completion of the instrument at pretest was 14.56 minutes. Considering there were 91 items on the instrument, the time for completion was relatively brief, which speaks to the flow of the instrument. Future research might also examine study designs with multiple arms, including a nontreatment control group. By including a nontreatment control group, potentially confounding effects, such as seasonality, could be controlled (Tucker & Gilliland, 2007). The current study did not directly test the effect of the web as a contributor to behavior change. Future research should consider comparing the same intervention across a variety of delivery mechanisms. In this way, the effect attributed to delivery medium could be directly measured and contrasted against any detected behavior change. For example, participants could be randomly allocated to receive EMPOWER online, on-site, a hybrid mixture of online/on-site, and/or assigned to a wait-list control.
Implications for Practice
From a programmatic perspective, mothers assume an important role in facilitating change in antecedents of childhood obesity and should be a central component for interventions targeting the family and home milieu. Practitioners are advised to evaluate changes in reified constructs from before to after an intervention using psychometrically valid and reliable instruments. Practitioners seeking to include parents in childhood obesity prevention programs should consider incorporating web-based delivery of program modalities to reduce attrition, particularly if higher intervention dosages are required. When designing online interventions, practitioners should focus on navigability and mobile accessibility to improve retention. Tangibility of web-based programs can be improved through the incorporation of home visitations from trained health educators. The ability to attribute program outcomes to the intervention prescription is essential to the advancement of program evaluation. Therefore, it is strongly recommended that practitioners collect process evaluation data throughout the duration of the intervention lifecycle. Process evaluation data for web-based interventions can be collected through telephone counseling, online surveys, and data mining metrics.
Footnotes
Authors’ Note
Portions of this research were presented at the 2012 Society for Public Health Education Annual Conference as well as the 2012 and 2013 American Public Health Association Annual National Conventions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a University of Cincinnati Graduate School Distinguished Dissertation Completion Fellowship. The Fellowship did not provide direct funding for the study but provided the first author with a stipend to work full-time on the research project as part of his dissertation research.