
Abstract
Objective. Education is inversely associated with coronary heart disease (CHD) risk; however the mechanisms are poorly understood. The study objectives were to evaluate the extent to which rarely measured factors (literacy, time preference, sense of control) and more commonly measured factors (income, depressive symptomatology, body mass index) in the education-CHD literature explain the associations between education and CHD risk. Method. The study sample included 346 participants, aged 38 to 47 years (59.5% women), of the New England Family Study birth cohort. Ten-year CHD risk was calculated using the validated Framingham risk algorithm that utilizes diabetes, smoking, blood pressure, total cholesterol, high-density lipoprotein cholesterol, age, and gender. Multivariable regression and mediation analyses were performed. Results. Regression analyses adjusting for age, race/ethnicity, and childhood confounders (e.g., parental socioeconomic status, intelligence) demonstrated that relative to those with greater than or equal to college education, men and women with less than high school had 73.7% (95% confidence interval [CI; 29.5, 133.0]) and 48.2% (95% CI [17.5, 86.8]) higher 10-year CHD risk, respectively. Mediation analyses demonstrated significant indirect effects for reading comprehension in women (7.2%; 95% CI [0.7, 19.4]) and men (7.2%; 95% CI [0.8, 19.1]), and depressive symptoms (11.8%; 95% CI [2.5, 26.6]) and perceived constraint (6.7%, 95% CI [0.7, 19.1]) in women. Conclusions. Evidence suggested that reading comprehension in women and men, and depressive symptoms and perceived constraint in women, may mediate some of the association between education and CHD risk. If these mediated effects are interpreted causally, interventions targeting reading, depressive symptoms, and perceived constraint could reduce educational inequalities in CHD.
As shown in a 2011 systematic review and meta-analysis, education is inversely associated with coronary heart disease (CHD) risk (Manrique-Garcia, Sidorchuk, Hallqvist, & Moradi, 2011); however, controversy exists whether the relationship is independent of infrequently measured confounders, and if it is, what are the underlying mechanisms (Falkstedt & Hemmingsson, 2011; Fujiwara & Kawachi, 2009; Gilman et al., 2008; Loucks et al., 2012; Madsen, Andersen, Christensen, Andersen, & Osler, 2010). For example, the contributions of several potential explanatory mechanisms are poorly understood, including literacy, time preference, and sense of control. Furthermore, few studies account for prospectively assessed early life potential confounders such as childhood intelligence, chronic physical illness, body mass index (BMI), or socioeconomic position (SEP; Loucks et al., 2012). Understanding the mechanisms helps identify potential targets for intervention and etiologic knowledge of how education could influence CHD.
There are a number of novel potential mediating mechanisms by which education could influence CHD (Figure 1). For example, literacy is influenced by education and may influence health through several ways, such as improved understanding of public health messages, instructions from health professionals, and ability to understand medication instructions (Baker et al., 2007; Martin et al., 2011). A second potential mechanism is “time preference,” which refers to abilities to delay gratification when costs and benefits of a behavior fall at different time points (Fuchs, 2004). For example, those with future-oriented time preference may be less likely to smoke cigarettes to reduce likelihood of developing CHD or other diseases in the future compared with those with present-oriented time preference. Education may change people’s time preference to become more future-oriented, through training individuals to prepare for, and anticipate, careers they will not experience until the future. Alternatively, those with future-oriented time preference may be more likely to obtain more schooling, thereby delaying immediate gratification of wages in the hopes for higher wages and autonomy in the future (Fuchs, 2004). A third potential mechanism is sense of control, which can be operationalized as two dimensions: personal mastery (a person’s sense of efficacy or effectiveness in carrying out goals) and perceived constraints (the extent to which one believes there are obstacles or factors beyond one’s control that interfere with reaching goals; Lachman & Weaver, 1998). Higher levels of education are associated with greater sense of control in most studies (Mirowsky & Ross, 2007). Education imparts skills, knowledge, and economic returns that may lead to one having a greater sense of control over one’s life, which could then improve health behaviors (e.g., diet, smoking, medication adherence) that influence CHD risk. Further potential mechanisms include income, obesity, and depression, all of which are typically associated with education and are CHD risk markers (Lorant et al., 2003; Manrique-Garcia et al., 2011; McLaren, 2007; Nemeroff & Goldschmidt-Clermont, 2012). The goal of the study was to evaluate potential mechanisms by which education may influence CHD risk. We considered the extent to which rarely measured factors (literacy, time preference, sense of control) and more commonly measured factors (income, depressive symptomatology, body mass index) in this literature may explain the association between education and CHD risk.
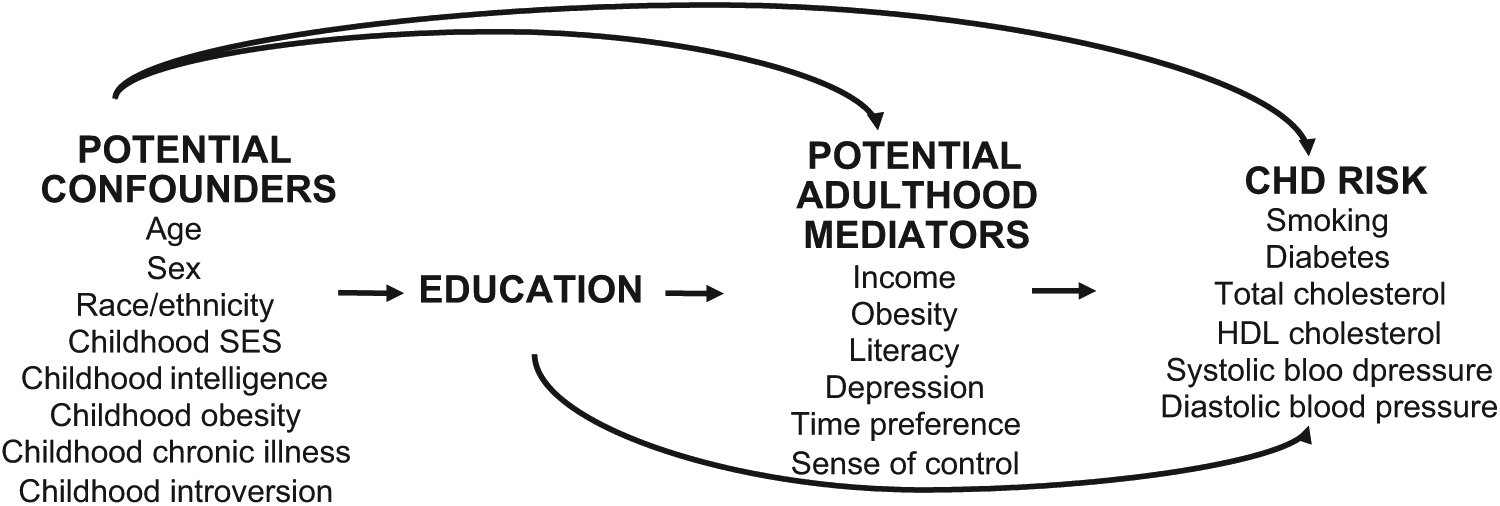
Directed acyclic graph (DAG) representing the hypothesized direction of effect from education to CHD risk, including plausible mediators and confounders.
Materials and Method
Sample
Study participants were from the New England Family Study (NEFS), which comprises 17,921 offspring of pregnant women in the Collaborative Perinatal Project (CPP) at the Providence, Rhode Island, and Boston, Massachusetts, sites (United States) between 1959 and 1974 (Niswander & Gordon, 1972). The current NEFS substudy, named the EdHealth Study, comprised NEFS participants selected with preference for racial/ethnic minorities and having either low or high educational attainment. There were 914 participants selected, of which 898 were eligible (e.g., living, not incarcerated), and 618 participated, resulting in a 68.8% response rate. All independent and dependent variables, as well as potential mediators, were assessed during 2005 to 2007 at mean age 42 years. The potential childhood confounders were assessed at study visits occurring between the prenatal period and age 7 years. Of the 618 participants, we excluded 42 participants not interviewed in person (did not complete physiological assessments) and 136 participants without blood samples (e.g., due to refusal, difficulty with blood flow from veins); an additional 11 participants were excluded due to missing more than or equal to one Framingham risk algorithm component. We further excluded participants with more than or equal to one missing covariate (n = 83). Accordingly, the analytic sample size was 346. The study protocol was approved by the Harvard School of Public Health Institutional Review Board.
Independent Variable
Education was determined as self-reported highest degree completed, categorized as: “less than high school” (GED or less than high school), “more than or equal to high school, less than college” (high school degree, schooling after high school including completing some college course work for credit, technical/trade/vocational school, associate’s degree, or certificate program), and “more than or equal to college” (e.g., bachelor’s degree, graduate degree).
Dependent Variable
Ten-year CHD risk was calculated as a percentage using the validated Framingham risk algorithm (Wilson et al., 1998). This algorithm uses Cox regression models that incorporate diabetes status, total and high-density lipoprotein (HDL) cholesterol, systolic and diastolic blood pressure, smoking, age, and gender, described in detail elsewhere (Wilson et al., 1998). The c-statistic for prediction of CHD events in the Framingham Heart Study is 0.74 in men and 0.77 in women, suggesting good predictive validity (Wilson et al., 1998). External validity tests on White and Black participants perform reasonably well (D’Agostino, Grundy, Sullivan, & Wilson, 2001).
Current smoking was based on self-report (yes/no). Lipids were measured in nonfasting plasma samples at CERLab (Harvard Medical School, Boston, MA) using a Hitachi 911 analyzer, and participating in the CDC/NHLBI Lipid Standardization Program. Total cholesterol (CV = 1.7%) and HDL cholesterol (CV = 3.3%) were measured enzymatically, described elsewhere (Allain, Poon, Chan, Richmond, & Fu, 1974; Rifai et al., 1998). Presence of diabetes was assessed by self-report as ever having been told by a doctor or health professional that participant has diabetes (nongestational). Five systolic and diastolic blood pressure measurements were obtained over 1-minute intervals in participants seated, after 5 minutes rest, in the right arm at heart level, using automated blood pressure monitors (VSMedTech BpTru, Coquitlam, British Columbia, Canada) demonstrated to have good validity and reliability compared with the auscultation method (Mattu, Heran, & Wright, 2004). Systolic and diastolic blood pressure values were calculated as the mean of the lowest three systolic or diastolic blood pressure readings, excluding the first recorded blood pressure.
Potential Childhood Confounders
Potential childhood confounders were obtained prenatally through age 7 years. Parental socioeconomic position was assessed, using a weighted percentile of both parents’ educational attainment, occupation, and income relative to the U.S. population prenatally and at age 7 (Myrianthopoulos & French, 1968). Childhood chronic medical conditions were derived from physical examinations by CPP pediatricians at ages 1 and 7 years, obtained via mothers’ reports at each visit, and extracted from medical records at ages 1 and 7. Summaries of childhood health conditions were compiled by CPP pediatricians. The current study used a summary score of number of chronic physical health conditions (including abnormalities of the liver, cardiovascular conditions, hematologic conditions [e.g., anemia], lower respiratory tract abnormality [e.g., asthma], neoplastic disease, neurologic abnormality, and prolonged/recurrent hospitalization) that excluded psychological or behavioral problems, coded for analytic purposes as 0 or ≥1 medical conditions. Childhood intellectual development at age 7 was defined using the Full-Scale Intelligence Quotient (FSIQ) score from the Wechsler Intelligence Scale for Children and the Wide Range Achievement Test (Jastak & Jastak, 1965; Wechsler, 1949). Age 7 height and weight were evaluated directly by CPP study technicians and converted into BMI (kg/m2). Childhood BMI was included as a potential confounder due to evidence that obesity may limit upward social mobility (i.e., dampen increases in SEP across the life course; Finkelstein, Ruhm, & Kosa, 2005).
Potential Mechanisms
Time preference was measured using a three-item scale based on a short version of the Consideration of Future Consequences Scale, modified to simplify the language due to concerns that the scale required high literacy levels (Gurmankin Levy, Micco, Putt, & Armstrong, 2006; Strathman, Gleicher, Boninger, & Edwards, 1994). Participants were asked how strongly they agreed with the following three questions, with 7-level Likert-type response options (1 = strongly disagree, 7 = strongly agree): “I only deal with things that are happening now, and assume that the future will take care of itself”; “Convenience is a big factor in the decisions I make or the actions I take”; and “I often ignore problems in my life because I think they are unlikely to become a big deal.” Scores (1-7 for each item) were averaged, with lower scores indicating more future-oriented time preference. The three-item scale had reasonable internal consistency (Cronbach’s α = .59) but, due to modified language, did not have other assessments of validity and reliability.
Sense of control was measured using two dimensions—personal mastery and perceived constraints—both measured using items developed by Lachman and Weaver (Lachman & Weaver, 1998) as an extension of the Pearlin and Schooler Mastery Scale (Pearlin & Schooler, 1978). Response options were on a 7-point Likert-type scale (1 = strongly disagree, 7 = strongly agree). Within each of the personal constraints and personal mastery scales, items were reverse scored as needed, and the mean scores were calculated, where higher scores represented higher personal constraints and higher personal mastery. Internal consistency (Cronbach’s α) was .84 and .71 for the personal constraints and personal mastery scales, respectively.
Four literacy skills were assessed. Reading comprehension, oral language (speaking), and aural language (listening) were assessed using subtests of the Woodcock Johnson III Tests of Achievement, a standardized test normed against a representative U.S. population (Martin et al., 2011; Woodcock, McGrew, & Mather, 2001). Numeracy was assessed using an eight-item scale adapted from Lipkus, Samsa, and Rimer (2001), described elsewhere (Martin et al., 2011). Analogously to Lipkus et al. (2001), our group conducted a factor analysis for the numeracy items using the 8 × 8 matrix of tetrachoric correlations, which are used to assess the correlation among dichotomous variables. Factor analysis confirmed a one-factor solution, with all 8 items loading on the first factor (individual loadings each exceeded 0.4). The first factor accounted for 86.3% of the variance.
Adulthood height and weight were assessed by trained technicians using standardized protocols, engaged in regular quality control/quality assurance, and converted to BMI (kg/m2). Depressive symptomatology was evaluated using the established Center for Epidemiologic Studies Depression 10-item scale, calculated as a sum of the 10 items (range 10-40; Kohout, Berkman, Evans, & Cornoni-Huntley, 1993). Family income was assessed via the poverty income ratio.
Analytic Methods
Multivariable-adjusted linear regression analyses evaluated associations of education with calculated 10-year CHD risk. Formal statistical tests of product terms between education and sex demonstrated significant effect modification (p = .02), consequently analyses were performed separately for males and females. Analyses used generalized estimating equations to account for clustering by family.
We assessed whether literacy, sense of control, time preference, income, body mass index, or depressive symptomatology were potential mediators of the association between education and 10-year CHD risk using a multiple mediation model. This model simultaneously estimates associations between each mediator and the education exposure, along with change in the outcome (10-year CHD risk) associated with the mediator in the fully adjusted model, and calculates an indirect effect using the product of coefficients method described elsewhere (Hayes, 2009; Preacher & Hayes, 2008; Valeri & Vanderweele, 2013). The indirect effect is the reduction in the association of the exposure on the outcome due to the potential mediator. Examining the indirect effect provides evidence of whether education may exert effects uniquely through any of the potential mediators. Confidence intervals were estimated by using bias-corrected bootstrapping procedure with 5,000 resamples (Hayes, 2009; Preacher & Hayes, 2008). Analyses were conducted using SAS version 9.1.3 (SAS Institute, Cary, NC).
Results
A comparison between included (n = 346) versus excluded (n = 272) participants found that included were slightly younger (42.2 vs. 42.8 years, respectively; p < .001), more likely to be White race/ethnicity (74% vs. 81%, respectively; p = .03), and had higher reading comprehension (12.9 vs.11.8 correct answers, respectively; p = .008) and numeracy (5.6 vs. 5.3 correct answers, respectively; p = .03). There were no significant differences (p > .05) between included and excluded participants for gender, education, systolic blood pressure, diastolic blood pressure, total cholesterol, HDL cholesterol, smoking, diabetes, or childhood covariates (parental SEP, childhood intelligence, chronic illness, BMI).
Descriptive statistics demonstrated that a number of childhood factors were associated with later life educational attainment including measures of cognitive function (Wide Range Achievement Test score and FSIQ scores), parental socioeconomic position, and in men only, race/ethnicity (Tables 1 and 2). Furthermore, education was associated with 10-year estimated CHD risk, smoking and diabetes in both men and women, and HDL cholesterol, systolic blood pressure, and diastolic blood pressure in women only (Tables 1 and 2). With respect to potential mediators, education was associated with poverty–income ratio and all literacy measures (oral, aural, numeracy, reading comprehension) in both men and women, as well as with adulthood BMI, depressive symptomatology, and sense of control (perceived constraints) in women (Tables 1 and 2).
Women: Descriptive Characteristics Showing the Outcome Variables, Potential Confounders, and Potential Mediators by Education Level.
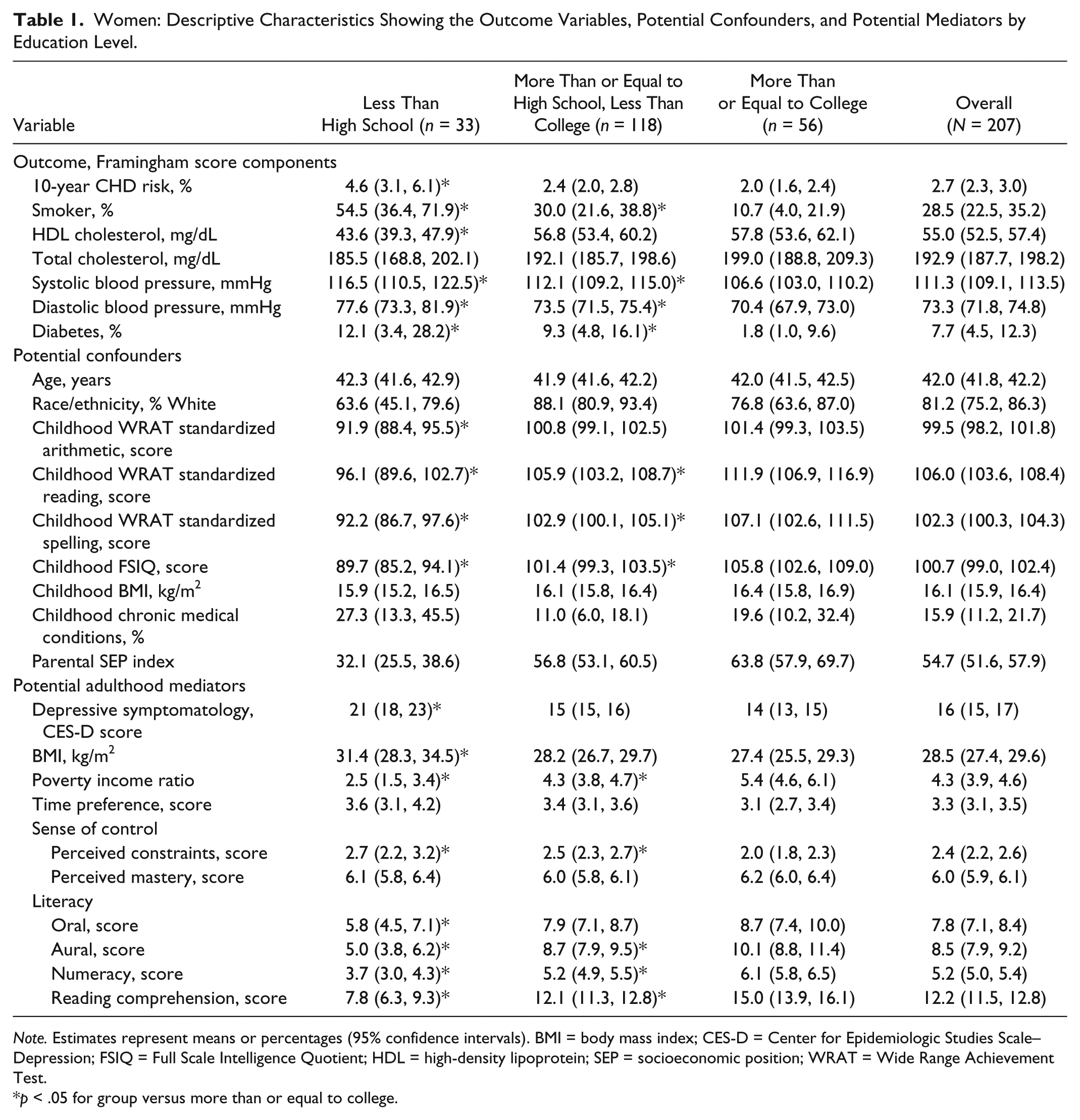
Note. Estimates represent means or percentages (95% confidence intervals). BMI = body mass index; CES-D = Center for Epidemiologic Studies Scale–Depression; FSIQ = Full Scale Intelligence Quotient; HDL = high-density lipoprotein; SEP = socioeconomic position; WRAT = Wide Range Achievement Test.
p < .05 for group versus more than or equal to college.
Men: Descriptive Characteristics Showing the Outcome Variables, Potential Confounders, and Potential Mediators by Education Level.
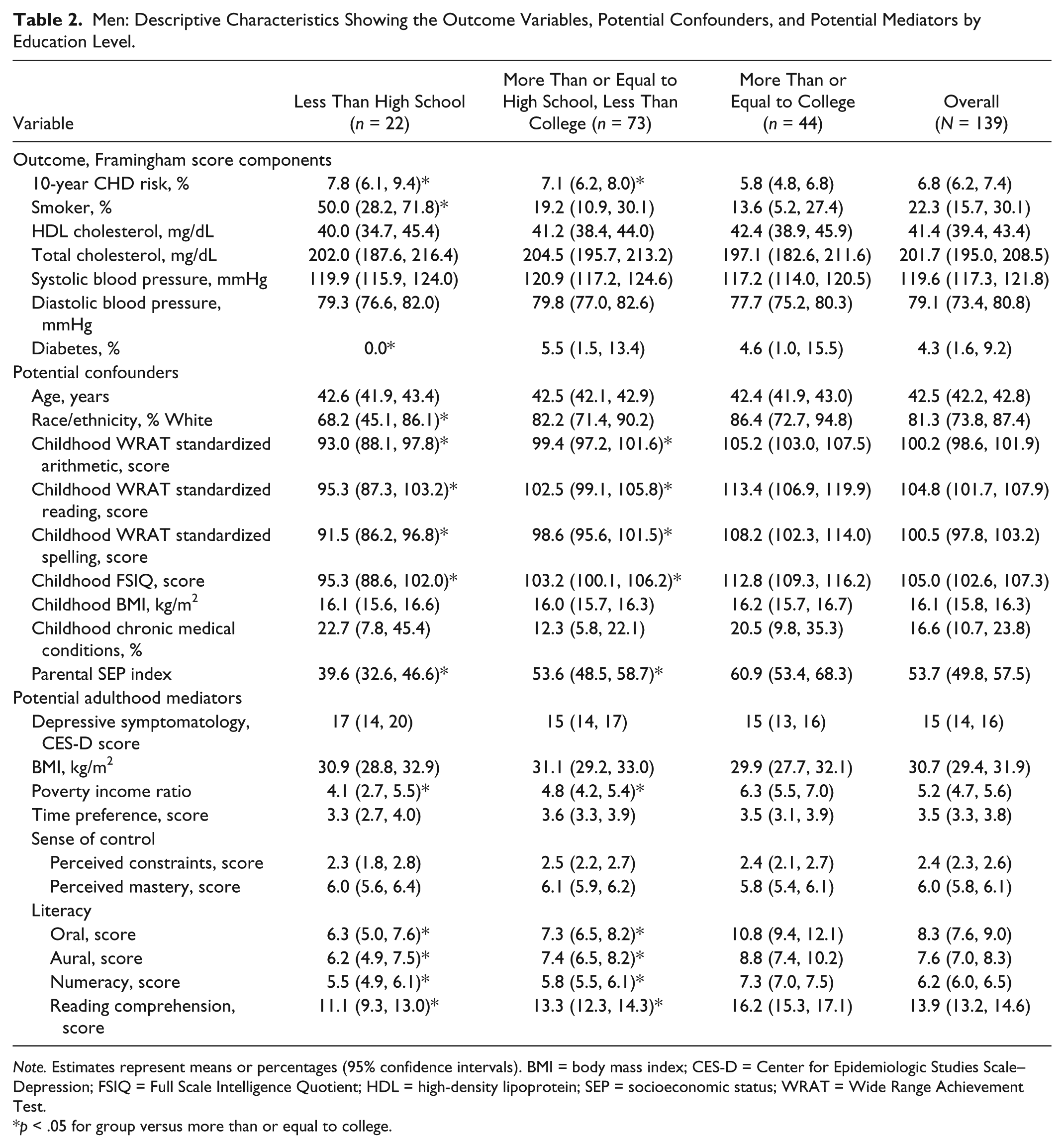
Note. Estimates represent means or percentages (95% confidence intervals). BMI = body mass index; CES-D = Center for Epidemiologic Studies Scale–Depression; FSIQ = Full Scale Intelligence Quotient; HDL = high-density lipoprotein; SEP = socioeconomic status; WRAT = Wide Range Achievement Test.
p < .05 for group versus more than or equal to college.
In multivariable-adjusted analyses, models that adjusted for age, race/ethnicity, and potential childhood confounders (parental socioeconomic index, age 7 intelligence, childhood chronic illnesses, and age 7 BMI) demonstrated that men and women with less than high school education had 73.7% (95% CI [29.5, 133.0]) and 48.2% (95% CI [17.5, 78.6]) higher 10-year CHD risk compared with those with at least a college degree, respectively (Table 3). In women, formal tests for mediation provided evidence of significant indirect effects for reading comprehension (7.2%; 95% CI [0.7, 19.4]), depressive symptoms (11.8%; 95% CI [2.5, 26.6]), and perceived constraint (6.7%; 95% CI [0.7, 19.1]; see Table 4), suggesting these factors explain some of the association between education and CHD risk. As an example for interpreting indirect effects, for the case of reading comprehension, the mediation estimate can be interpreted as of the total effect of 73.7% increase in CHD risk for women with less than high school education versus those with at least a college degree, 7.2% may be mediated through reading comprehension while the remaining 66.5% (i.e., 73.7% − 7.2%) may occur through other mechanisms. In men, mediation tests provided evidence of significant indirect effects of education through reading comprehension (indirect effect: 7.2%; 95% CI [0.8, 19.1]; see Table 4). In both men and women, there was less evidence for mediation by other factors such as adulthood BMI, income, perceived mastery, time preference, aural language, oral language, or numeracy (Table 4).
Multivariable Adjusted Associations of Education With 10-Year Estimated CHD Risk.
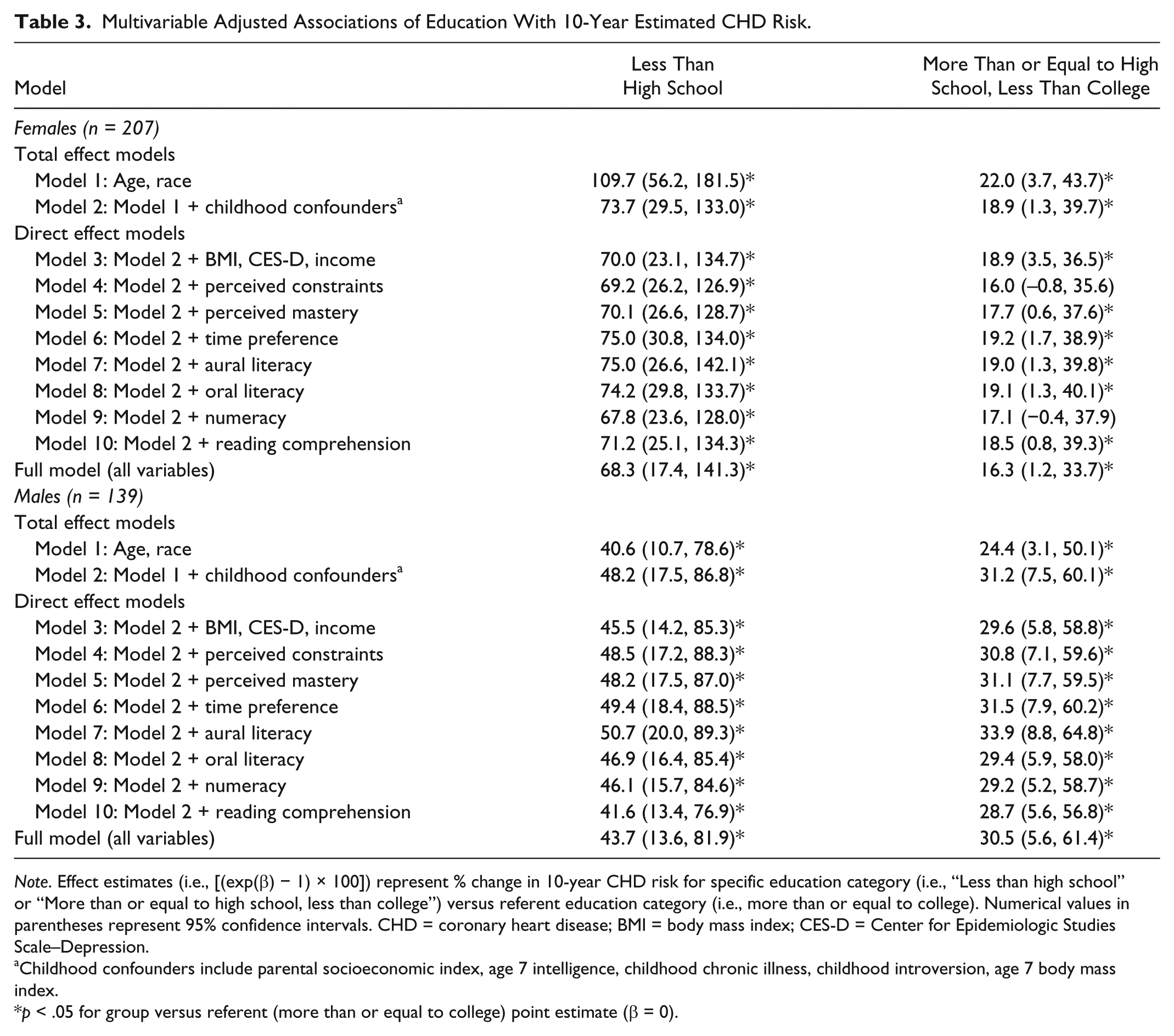
Note. Effect estimates (i.e., [(exp(β) − 1) × 100]) represent % change in 10-year CHD risk for specific education category (i.e., “Less than high school” or “More than or equal to high school, less than college”) versus referent education category (i.e., more than or equal to college). Numerical values in parentheses represent 95% confidence intervals. CHD = coronary heart disease; BMI = body mass index; CES-D = Center for Epidemiologic Studies Scale–Depression.
Childhood confounders include parental socioeconomic index, age 7 intelligence, childhood chronic illness, childhood introversion, age 7 body mass index.
p < .05 for group versus referent (more than or equal to college) point estimate (β = 0).
Mediation Tests Evaluating Indirect Effects of Education on 10-Year Estimated CHD Risk, Stratified by Gender.

Note. Point estimates (indirect effects= [(exp(β) − 1) × 100]) represent % change in relative 10-year risk for specific education category versus referent education category, due to the addition of the mediator into the model. Numerical values in parentheses represent 95% confidence intervals. All models are adjusted for age, race/ethnicity, and childhood confounders (parental socioeconomic index, age 7 intelligence, childhood chronic illness, childhood introversion, age 7 body mass index).
p < .05 for group versus referent (More than or equal to college) point estimate (β = 0).
Discussion
This study’s findings suggested that reading comprehension in women and men, and depressive symptoms and perceived constraint in women, explain part of the association between education and CHD risk.
Prior Literature
While studies showed associations of education with the potential factors explored in this study (i.e., literacy, sense of control, time preference, BMI, depressive symptomatology, income; Guthrie, Butler, & Ward, 2009; Kutner, Greenberg, Jin, & Paulsen, 2006; Lorant et al., 2003; McLaren, 2007; Mirowsky & Ross, 2007), and associations of these factors with CVD risk (Baker et al., 2007; Manrique-Garcia et al., 2011; Martin et al., 2011; Nemeroff & Goldschmidt-Clermont, 2012; Surtees, Wainwright, Luben, Khaw, & Day, 2006), there has been little exploration of whether these factors may mediate or confound the relation between education and CVD risk.
With regard to literacy, a study using structural equation modeling suggested functional health literacy was a mediator between socioeconomic position and perceptions of the importance of various behaviors that influence cancer risk (e.g., smoking, diet, physical activity, overweight; Adams et al., 2013). Our study found evidence of mediation between education and CHD risk for reading comprehension, and less evidence for numeracy, aural, and oral literacy as mediators. Very little is known about contributions of individual literacy components as mediators. Reading comprehension may be the most important literacy factor linking education to CHD risk, but findings should be replicated.
Sense of control is another potential mediator. A prospective study of 3,888 participants showed associations between education and incident CHD were reduced by 27% after adjusting for sense of control (Bosma et al., 2005). In another study, associations between education and incident mortality were reduced by 54% after adjusting for perceived control (Bosma, Schrijvers, & Mackenbach, 1999). These findings supported ours showing evidence of mediation for perceived constraint in women. Prior studies did not show gender-specific findings, although the 2005 study (Bosma et al., 2005) found no significant effect modification by gender. Studies to date have not reported findings separately for perceived constraint versus perceived mastery (Bosma et al., 2005). It may be that perceived constraint is a more important mediator between education and CHD risk as shown in the current study, but these results should be replicated.
With regard to time preference, there has been little evidence in the few studies to date that time preference may be an explanatory mechanism between education and health, with health measured via health behaviors (e.g., smoking, obesity) and self-rated health, and time preference assessed using closed-ended intertemporal choices to elicit time preference for monetary outcomes or the Zimbardo Time Perspective Inventory (Guthrie et al., 2009; van der Pol, 2011). This is consistent with our findings. The field is still new, and potential for findings remain, perhaps with more sophisticated assessments of health outcomes and time preference and larger sample sizes.
Depressive symptomatology is a potential mediator. A large number of prospective studies demonstrated that depression is positively associated with CHD risk (Frasure-Smith & Lesperance, 2010; Nicholson, Kuper, & Hemingway, 2006). With regard to potential mediation of the association between education and CHD by depression, a study in NHANES I showed a 9% reduction in effect size in the relation between education and incident CHD after further adjustment for depressive symptomatology (Thurston, Kubzansky, Kawachi, & Berkman, 2006). The current study results add to the literature evidence that depressive symptomatology may be a mediator between education and CHD risk, particularly in women. The observed indirect effect of 11.8% through depressive symptomatology represents 16% of the total effect (i.e., 11.8% indirect effect/73.7% total effect = 16.0% of the total effect). This small to medium indirect effect size is expected, given the large number of potential mediators. With regard to adulthood BMI, little is known about the role specifically of BMI as a mediator between education and CVD risk. Findings in this study do not show significant evidence of adulthood BMI as a mediator between education and CHD risk. Evidence for income as a potential mediator in a previous study on 22,688 U.S. participants showed that further adjustment for income reduced the strength of effect between education and incident CVD events by 8% (Albert, Glynn, Buring, & Ridker, 2006). This suggests that impacts of education on CVD may be somewhat independent of income, similar to findings in this study.
Strengths and Limitations
There are several limitations. First, the CHD risk algorithm is not as accurate a measure of CHD as the measurement of CHD events themselves. However, given the relatively young age of the participants (38-47 years), it is too early in the life course to evaluate associations with CHD events in this study. Educational attainment may have an effect on a wide range of CHD risk factors. Consequently, by utilizing a validated CHD prediction algorithm that encompasses a variety of CHD risk factors, it allows for evaluation of a number of risk factors that may be simultaneously influenced by education. A second limitation is that the mediators and outcome were measured simultaneously, as such these analyses could not rule out associations between the exposure, mediators, and outcome being due to reverse causation. Furthermore, the relatively small sample size (n = 346) likely resulted in more imprecise estimates and increased the chances of random error compared to what would be possible with larger sample sizes. Finally, other potential mechanisms were not explored in this study such as use of preventive medical care, diet, and physical activity (Sundquist, Winkleby, & Pudaric, 2001), and could be the focus of future research.
Strengths of the study include accurate measurement of biological measures (including cholesterol, blood pressure, and BMI), using substantial internal and external quality control protocols. Furthermore, the birth cohort study design offered a unique ability to statistically account for directly assessed uncommonly measured prior common causes such as childhood intelligence, socioeconomic position, and chronic illness.
Conclusion
This study provided evidence that reading comprehension in women and men, and depressive symptoms and perceived constraint in women, may explain some of the association between education and CHD risk. Findings from this study should improve etiologic knowledge about the potential mechanisms by which education could influence CHD risk. If these mediated effects are interpreted causally, evidence-based interventions targeting reading (e.g., reading comprehension courses), depressive symptoms (e.g., counseling, medication), and perceived constraint could reduce educational inequalities in CHD. Other plausible interventions may include addressing education itself through improvements in quality and/or quantity of education. Education interventions that have been shown to affect health are lacking, although there have been some compelling randomized controlled trials on the quality of early childhood education (Campbell et al., 2014; Muennig, Schweinhart, Montie, & Neidell, 2009) and natural experiments on the quantity of grade school education (Albouy & Lequien, 2009; Lleras-Muney, 2005).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by National Institutes of Health (National Institute on Aging) grants R01AG023397 and R01AG048825.