
Abstract
The DELTA PREP Project aims to reduce risk for intimate partner violence (IPV). It engaged leadership and staff from 19 statewide domestic violence coalitions in building capacity to prevent IPV before it occurs (rather than solely responding to IPV). This article describes the process and outcomes associated with action planning to create coalition organizational change related to preventing IPV. Coalition staff and leadership planned for organizational changes in six goal areas: leadership, structures and processes, staffing, resource development, partnership development, and member agency development. Action planning was conducted during 2-day, in-person sessions that involved (a) review and refinement of coalition vision and mission statements, (b) interpretation of coalition assessments (for prevention capacity), (c) identification of specific organizational changes to be sought, and (d) specification of action steps for each proposed organizational change to be sought. The results show overall increases in the amounts, and variations in the kinds, of organizational changes that were facilitated by coalitions. Challenges related to action planning and future directions for capacity building among statewide IPV prevention coalitions are discussed.
The National Public Health Performance Standards Program identifies one of the essential public health services for localities and states as, “develop policies and plans that support individual and community health efforts” (Centers for Disease Control and Prevention, 2010). Action planning is one approach to developing plans that has shown promise for enabling local and state-level organizations to promote health. Action planning refers to the process of identifying and planning for specific changes to organizations, communities, and systems, including new or modified programs, policies, and practices (Fawcett, Schultz, Watson-Thompson, Fox, & Bremby, 2010). Action planning is a participatory process, involving key stakeholders of health initiatives—individuals who represent the program or organization, and often, those who will benefit from the intervention (Cornwall, Lall, Kennedy, & Owen, 2003). It involves developing a written plan with action steps that specify who will do what to bring about specific changes by when. Action planning is typically one component of health initiatives; often, it is combined with assessment (Bailie et al., 2007; Matthews et al., 2011), technical assistance (Gilliam, Davis, Barrington, Lacson, & Uhl, 2002; Slep & Heyman, 2008), and monitoring and evaluation (Leisner & Wonch, 2006). Some (but not all) action planning approaches focus almost exclusive attention to adoption of evidence-based approaches (e.g., Getting to Outcomes—Chinman, Imm, & Wandersman, 2004 and Communities that Care—Social Development Research Group, n.d.).
Systematic reviews have identified action planning as a critical process, associated with increases in changes in communities and broader systems (e.g., Roussos & Fawcett, 2000). Action planning has been a key component in a variety of public health interventions including those addressing neighborhood development (Watson-Thompson, Fawcett, & Schultz, 2008), cardiovascular diseases (Schulz et al., 2011), and tobacco control (Kreisler, Snider, & Kiernan, 1997). On the citywide level, Thompson, Peck, and Brandert (2008) describe action planning efforts that occurred across large metropolitan cities (Los Angeles, Nashville, and Hartford). Process results show that action planning was associated with a variety of changes to community health including expanding community knowledge and reach of health services. Action planning has also enabled programs and organizations to facilitate local change. On the organizational level, action planning has been associated with numerous types of improvements; for instance, multidisciplinary trauma centers bringing about changes in hiring practices (Reed, Gerhardt, Fonseca, & Robertson, 2009), Aboriginal community health centers improving provision of preventive health services (Bailie et al., 2007), and veterans affairs health care networks implementing electronic medical record systems (Leisner & Wonch, 2006).
DELTA PREP Program
The DELTA PREP program focused on assisting 19 statewide domestic violence coalitions to increase their organizational capacity for the primary prevention of intimate partner violence (IPV); the program is described in detail, elsewhere (Freire, Zakocs, Le, Hill, Brown, & Wheaton, 2015). The DELTA PREP initiative’s theory of change involved (a) resources provided to the 19 statewide coalitions, (b) action planning for building organizational capacity, (c) intermediate outcomes for the coalitions (i.e., increase capacity for primary prevention), and (d) longer-term outcomes (including decreases in risk factors and increases in protective factors related to IPV).
Figure 1 displays the DELTA PREP theory of change model. Action planning was conducted in two stages throughout the DELTA PREP Project—once to plan for organizational changes (focused on building coalition capacity for the primary prevention of IPV) and again to plan for prevention efforts (focused on building state and community-level capacity to prevent IPV and in turn, reduce risk factors for IPV while increasing protective factors for healthy relationships). Studies that involve action planning typically provide little (if any) description of how action planning was carried out. This article (a) describes the action planning process (focused on building coalition capacity for the primary prevention of IPV), (b) examines the immediate results of action planning (i.e., types of organizational changes that were planned for), (c) examines the implementation of the action plans (i.e., organizational changes that were actually accomplished), and (d) examines the rate of organizational changes that the coalitions accomplished over time.

DELTA PREP theory of change.
Method
Participants
In the fall of 2009, representatives from 19 statewide domestic violence coalitions participated in one of four action planning sessions held in separate regions of the United States. Coalitions were asked to have at least two individuals attend the action planning session—a leadership-level member (e.g., the executive director) and a staff-level member. Each of the action planning sessions also involved five to eight peer “coaches” from statewide domestic violence coalitions that had been previously funded. The coaches helped facilitate the action planning process, provided feedback on action plans, and shared their experiences. The action planning sessions were led by members of The University of Kansas Work Group for Community Health and Development (KUWG), with support from the DELTA PREP Training and Evaluation Team, including staff from the CDC Foundation, program evaluators, and other university partners.
Action Planning Overview
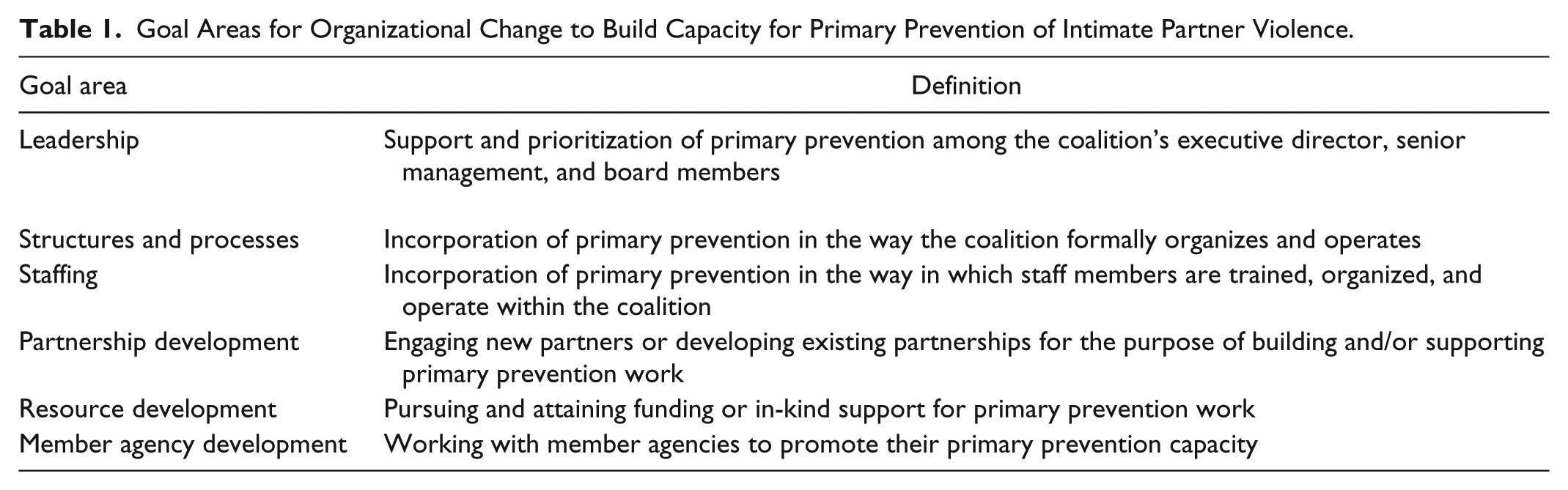
Action planning trainings occurred over a 2-day period. The sessions involved supporting materials (i.e., a workbook and a capacity assessment of each coalition’s readiness for primary prevention). Following the action planning session, coalitions drafted their action plans “back home” with other members of their coalition, received individualized technical assistance, and revised their plan based on feedback from the CDC Foundation (both written and oral). Action plans were implemented over the project period (with a follow-up or “refresher” session 2 years into the project). Following the completion of the action planning training, the KUWG team facilitated training on using the field-tested Online Documentation and Support System (ODSS) to capture organizational changes (Fawcett & Schultz, 2008). The ODSS enabled coalition members to enter brief written descriptions of organizational changes that their coalition implemented, and to classify each organizational change by related goal area: (a) leadership, (b) structures and processes, (c) staffing, (d) resource development, (e) partnership development, or (f) member agency development. Table 1 provides a definition of each goal area. Participants received written training materials that included criteria for what constituted an organizational change and the operational definition (“changes the coalition makes to improve its organizational capacity for primary prevention of intimate partner violence”). Two and a half hours were scheduled to train coalition participants to use the ODSS.
Goal Areas for Organizational Change to Build Capacity for Primary Prevention of Intimate Partner Violence.
The action planning process consisted of four segments occurring across 2 days, with the first three segments occurring the first day and the fourth segment occurring the second day. Each of these segments was scheduled to last from 1 to 2 hours. Table 2 provides brief descriptions and the materials used to support each aspect of action planning. This general approach to action planning involved (a) presenting key concepts to coalition participants, (b) allowing time for participants to dialogue in small groups (i.e., with other members of their coalition and other coalitions), and (c) coalition representatives sharing the highlights of their dialogue with the all members of the action planning session. Each participant received an “Action Planning Workbook” which served as a place to record ideas that emerged during small group dialogues. The section that follows describes each of the four segments and the supporting materials.
Action Planning Components and Support Materials.

Segment 1: What and Why
The first portion provided an overview of the action planning process. The facilitator (the KUWG partner from the Training and Evaluation team) used a PowerPoint to guide each of the four segments. This segment began with a review of the DELTA PREP Project’s theory of change that guided the initiative from assessment and implementation to desired (longer term) outcomes. Reviewing the theory of change provided a context for the action planning process within the broader DELTA PREP Project. During this segment, the facilitator also described the action planning process and led a brief group dialogue, inviting coalition representatives to discuss how action planning would help their coalition bring about organizational changes to further primary prevention of IPV. In addition, coalition participants reviewed their coalition’s vision and mission statements; the facilitator led another dialogue about how organizational changes related to primary prevention could help the coalition address their vision and mission.
Segment 2: Review of Coalition Assessment
This segment provided time for coalition participants to review their “Coalition Prevention Capacity Assessment.” The assessment provided a baseline measure of the coalition’s capacity to support the primary prevention of IPV in their state. Participants were given time to review the assessment with other members of their coalition and were assisted by DELTA coaches and the DELTA PREP Project team. The assessment helped participants consider and record ideas in their Action Planning Workbook related to (a) “Relative Strengths and Ways to Enhance Them” and (b) “Relative Challenges and Ways to Address Them.”
Segment 3: Identifying Organizational Changes to Be Sought
This segment involved identifying organizational changes to be sought by the coalition, for instance, making changes in the coalition’s mission statement to incorporate primary prevention or changes in the coalition structure to engage more prevention partners. This began with a review of potential organizational changes that coalitions might target and plan for; these example changes were listed in an “Inventory of Potential Changes in Your Organization.” This inventory provided 61 examples of organizational changes, sorted by each of the five goal areas (e.g., leadership, structures and processes, etc.). Coalition participants reviewed the “Inventory” and considered the findings of their coalition assessment, as well as their working knowledge of the coalition, to determine a list of candidate organizational changes to be sought. Finally, coalition participants worked together to prioritize the candidate list of organizational changes. This involved rating the importance of each candidate change on a 1-to-5 scale (1 = low, 5 = high) as well as the feasibility of bringing about each change on the same 1-to-5 scale. The desired outcome was to have a list of prioritized organizational changes that represented important and feasible contributions to increasing the coalition’s capacity for primary prevention of IPV.
Segment 4: Creating Action Steps and Bringing It Back Home
This final segment involved identifying action steps for each of the priority organizational changes that the coalition participants identified. For each priority organizational change to be sought, participants worked with others from their coalition to determine (a) action steps needed to bring about the change, (b) the person(s) responsible for each action step, (c) the date by which the action step was to be completed, (d) the resources required to facilitate each action step, and (e) communication/collaborators (i.e., who else should know about this action step). After considering action steps for each organizational change, coalition participants were instructed to consider how they could build consensus with other members of their coalition (not present at the training) regarding the draft plan, and how they could use the action plan when they returned to their state.
Evaluation of the Action Planning Process
Evaluation of the action plans for the present article involved a review of the completed plans submitted by coalitions as well as a review of accomplishments—changes in the organization that were documented in the ODSS by the coalitions as they carried out their action plans. Coalitions submitted their action plans to the CDC Foundation in December 2009, November 2010, and November 2011. Annually, members of the Training and Evaluation Team reviewed the amount and kind of documented changes with two (or more) members of each coalition.
Results
Descriptive Data on Organizational Changes Planned
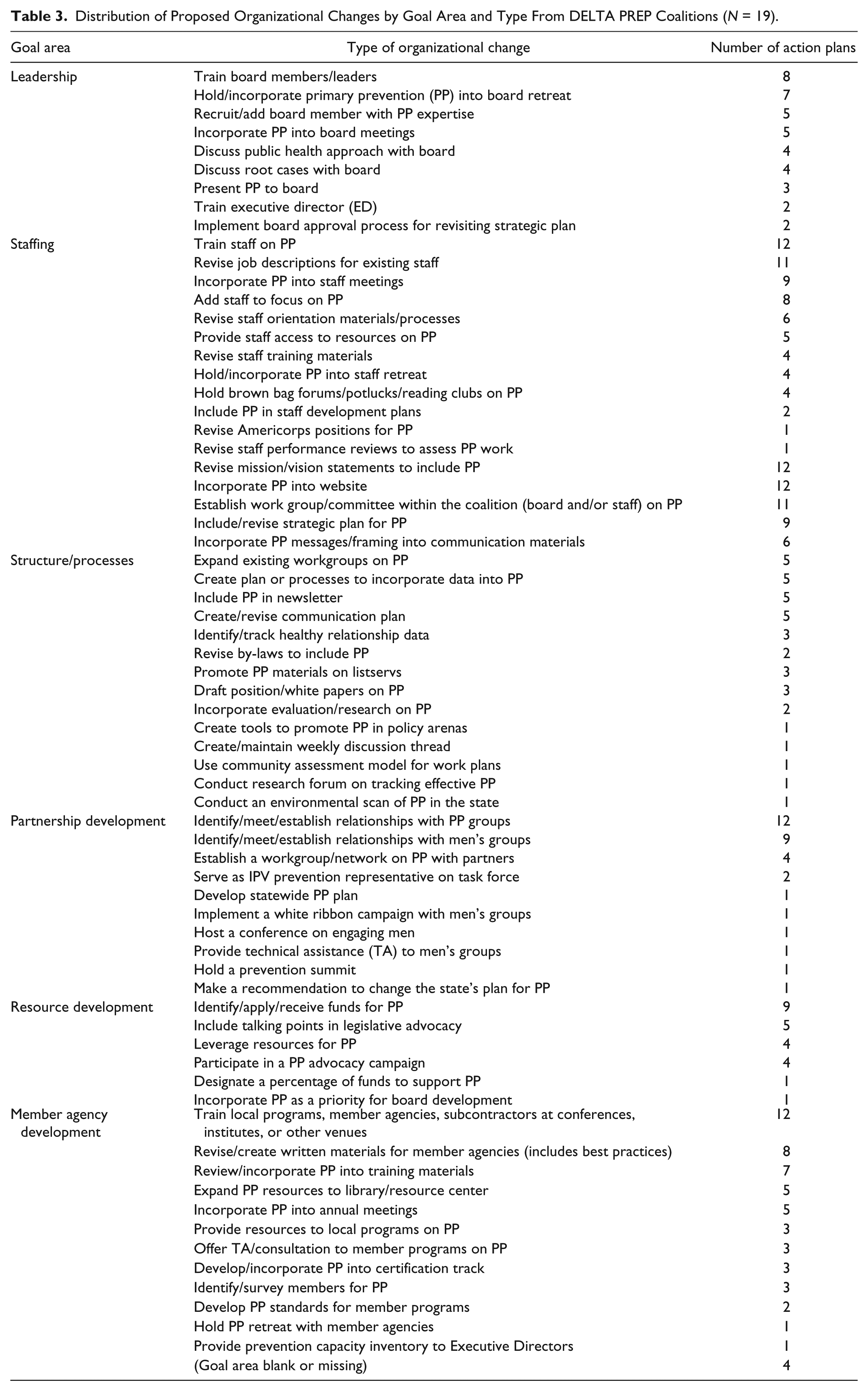
A total of 68 types of organizational changes were identified across the 19 action plans. Table 3 displays organizational changes represented in action plans by goal area and type. Approximately 60% of organizational changes appearing in action plans came from the “Inventory of Potential Organizational Changes to be Sought”; the other 40% were not listed in the inventory. Coalitions typically addressed multiple goal areas in their action plans. More than 50% (N = 10) of the action plans proposed at least one organizational change across all six goal areas. Approximately one quarter (N = 5) of the action plans targeted five goal areas, 10% (N = 2) targeted four goal areas, and two did not identify goal areas for the proposed organizational changes. Coalitions tended to propose a greater variety of organizational changes for internal dimensions such as leadership, staffing, and structures/processes; fewer organizational changes were targeted for external dimensions such as partnership and resource development. Table 4 provides an example change across the six goal areas.
Distribution of Proposed Organizational Changes by Goal Area and Type From DELTA PREP Coalitions (N = 19).
Examples of Organizational Changes Across Each of the Goal Areas.

Ratings on the Action Planning Process
Overall, coalition representatives reported that the action planning process provided clear direction for their efforts to develop an action plan. At the conclusion of the 2-day regional training in which action planning occurred, coalition participants responded to a confidential survey. Participants were to respond on a 1-to-5 scale with their level of agreement where 1 = not at all, 3 = somewhat, and 5 = very. When asked, “Did the training provide clear guidance on how to develop an action plan for organizational change?” participants (N = 45) provided an average rating of 4.7 on a 5-point scale (SD = 0.47). Data from focus groups at the end of the DELTA PREP Project period, among representatives from all 19 coalitions, suggested that action planning helped accelerate their work in a variety of ways, including (a) by helping coalitions focus on prevention work, (b) by helping coalition members remain accountable, and (c) by breaking down the process of creating change.
Data on Organizational Changes Implemented and Association With Action Planning
The 19 DELTA PREP coalitions documented a total of 309 organizational changes during the 3-year project period. About 81% of all documented changes were stated in the action plan (when action planning was conducted 2 years later, an additional 48 organizational changes were planned). To assure data quality, DELTA PREP staff reviewed documented entries quarterly with each coalition, and discussed disagreements in documentation until consensus was established on each organizational change that was documented. On average, coalitions facilitated (and documented) 16.3 organizational changes across the project period (SD = 7.2, Mdn = 15, range = 6, 29). The online data also revealed that the coalitions targeted a variety of goal areas in their efforts to build capacity for primary prevention of IPV. Out of the 309 organizational changes, coalitions targeted structures/processes most frequently (28.5% of the organizational changes). This was followed by member agency development (20.1%), staffing (18.1%), partnership development (15.9%), resource development (8.8%), and leadership (7.4%); four organizational changes did not have a goal area assigned.
Figure 2 displays the aggregate number of organizational changes brought about by month of the project, across all 19 coalitions. The 2-day action planning sessions (facilitated across four regional workshops) occurred in September and October of 2009. Final versions of the action plans were due to the DELTA PREP Training and Evaluation Team in December of 2009. In the 4 months that followed the plans’ due date of December of 2009, there was a general increasing trend in the aggregate number of organizational changes implemented. This pattern of monthly increase generally occurred until the aggregate number of organizational changes by month peaked at 22 in November of 2010.
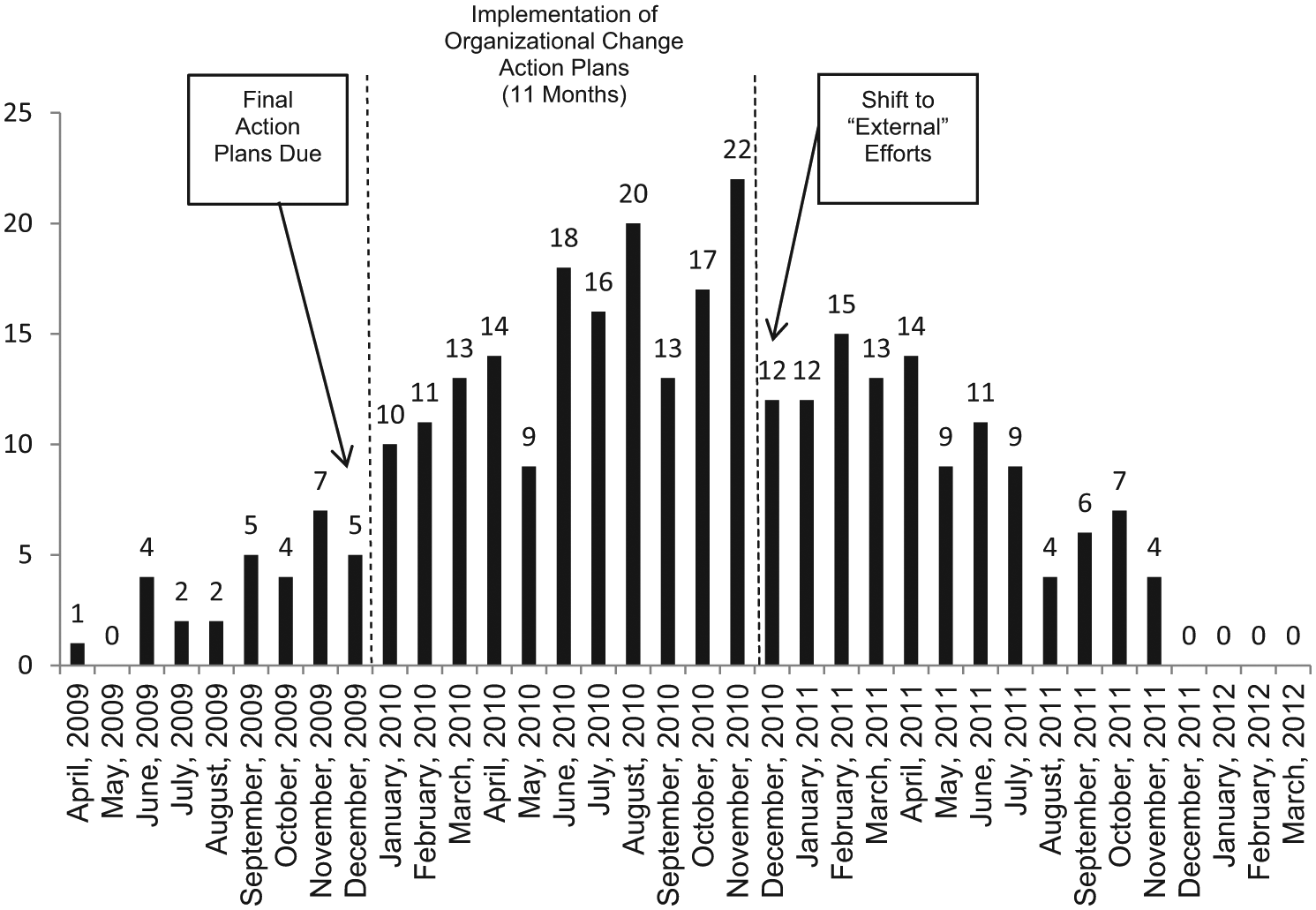
Aggregate number of organizational changes implemented per month for all 19 DELTA PREP coalitions.
Initially, action planning focused on organizational changes “internal” to the coalition to improve capacity for primary prevention. In November of 2010, the project shifted its focus to facilitating prevention efforts “external” to the coalition. These prevention efforts included actions to initiate, support, or modify community and state-level programs, policies, and advocacy work related to IPV. The shift to “external” prevention efforts coincided with an observed decrease in “internal” efforts (i.e., organizational changes) which can be seen in the data (Figure 2).
Discussion and Conclusion
The DELTA PREP initiative enabled participating coalitions to improve their organizational capacity for primary prevention of IPV. The results showed that coalitions were able to create action plans for organizational change to support the primary prevention of IPV. An analysis of the action plans revealed that about 60% of the changes planned were similar in function to changes listed in the “Inventory of Potential Changes to be Sought.” This support material may have prompted coalitions to identify organizational changes appropriate to their situation. This study’s action planning approach was more participatory. It provided a list of promising organizational changes to seek, while allowing coalition members to determine what changes were both important and feasible in their context.
Although participant ratings and the data suggest that the process was effective overall, there is room for improvement. For example, when the action plans were submitted in December 2009, many of the plans contained more general strategies for organizational change (e.g., “increase staff knowledge on primary prevention”) rather than specific organizational changes to be sought (i.e., “include primary prevention in staff development plans”). Plans were refined using feedback from CDC Foundation staff, mentoring (from other “coaches”), and additional training as needed. This suggests the importance of technical assistance in implementing action planning—one of the other key resources provided to the DELTA PREP coalitions.
Coalitions were able to follow through on their action plans; they brought about 309 organizational changes, more than 16 organizational changes per coalition on average, related to changing their coalition’s programs, policies, and practices to build capacity for the primary prevention of IPV. More frequently, organizational changes addressed the structures/processes of the coalition and least frequently, it targeted the leadership of the coalition. This suggests that coalitions found organizational changes related to structures/processes to be more important and/or feasible, while they found organizational changes related to leadership to be less important and/or feasible in their context.
Action planning was associated with rather immediate and marked increases in the rate of organizational changes overall. Following the submission of action plans in December of 2009, there was a steady increase in the number of changes these coalitions implemented. The total number of organizational changes brought about by the DELTA PREP coalitions increased 7 out of 11 times from month-to-month during the “Implementation of Organizational Change Action Plans” phase. However, other factors may have also influenced coalitions’ facilitation of organizational change (e.g., other training). Furthermore, action planning represented only one of the multiple resources coalitions were given in the DELTA PREP Project.
This study reveals associations between documented levels of organizational changes and the action planning intervention. The components of action planning included training and technical assistance, contingencies on plan submission, feedback on quality of plans, and systematic reflection on the amount and type of organizational changes actually facilitated. As an observational study, conclusions about cause and effect regarding action planning and the rate of organizational changes are not possible. However, 81% of the organizational changes that were documented in the system came from the action plans. This suggests that the majority of the changes that were recorded (and met the operational definition, and inclusion/exclusion criteria) were planned for during the action planning component of the initiative. Furthermore, the 19 DELTA PREP coalitions applied for CDC Foundation grant funding in an open, competitive process. Since selection of the 19 DELTA PREP coalitions was based on assessed readiness to address the project’s goals, these findings may not be representative of what might be seen with typical state-level coalitions. Future research might use stronger experimental designs, such as an interrupted time series design or a control group design with random assignment, to permit clearer conclusions about whether action planning led to observed changes. Such future research could help rule out confounding variables, such as other training experiences, and could help extend the generality of findings to a broader sample of coalitions. Overall, action planning was integral to DELTA PREP’s theory of change: that training, technical support, and coaching can help coalitions build their capacity for the primary prevention of IPV and assure conditions in which all people live in communities where healthy relationships are the norm.
Footnotes
Authors’ Note
The first author was a graduate research assistant at The University of Kansas Work Group for Community Health and Development when he completed this study.
Theme Section Note
This article is part of a Health Education & Behavior theme section on the DELTA PREP Project, sponsored by the Centers for Disease Control and Prevention (CDC) National Center for Injury Prevention and Control, Division of Violence Prevention. Funding for DELTA PREP and the issue was provided by the CDC Foundation through a grant from the Robert Wood Johnson Foundation. The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention, the CDC Foundation, or the Robert Wood Johnson Foundation. The theme section articles are available open access via ![]() .
.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.