
Abstract
This pilot study was conducted to explore the associations between stressors related to homelessness and modifiable health risk factors (poor diet, insufficient physical activity, and overweight/obesity) and to provide direction for future research. Participants (N = 57) were homeless adults enrolled in a smoking cessation program. Analyses were conducted to characterize the sample as well as the relations between relevant stressors (discrimination, chronic stress, and fear and mistrust) and health risk factors. Inadequate daily consumption of fruits, vegetables, and fiber was common. High-fat diet and insufficient physical activity were also prevalent, and the majority of participants were overweight/obese. Participants commonly endorsed discrimination, fear of victimization, mistrust of others, and several other stressors. Greater endorsement of stressors was associated with a high-fat diet. Results suggest that lifestyle interventions and policy changes may be warranted in homeless shelters to attenuate the potential effects of stressors on high-fat dietary consumption among smokers.
Poor health is commonplace among homeless adults. Mortality rates are at least three times greater among homeless adults than the general population (Hibbs et al., 1994). Modifiable health risk factors, such as smoking and obesity-related behaviors (e.g., poor diet and insufficient physical activity), are likely contributors to disease in this population. Specifically, cigarette smoking is normative among homeless individuals, with reported prevalence rates greater than 70% (Baggett & Rigotti, 2010). Less is known about obesity and homelessness, though recent research suggests that rates of overweight and obesity are comparably high to rates in the general population (Koh, Hoy, O’Connell, & Montgomery, 2012). In addition, some research indicates that homeless individuals have nutritionally inadequate diets (Luder, Boey, Buchalter, & Martinez-Weber, 1989) and most do not engage in daily exercise (Chau et al., 2002). Critically, the combination of smoking and obesity substantially increases mortality risk above and beyond either risk factor alone (Koster et al., 2008). Consequently, more research is needed to understand the frequency and correlates of dietary risk factors, insufficient physical activity, and overweight/obesity among homeless adults and particularly among those who smoke.
Homelessness is likely associated with a variety of stressors that may plausibly increase the likelihood of poor diet, insufficient physical activity, and overweight/obesity. For example, greater perceived discrimination has been linked with consuming a less healthy diet (Brodish et al., 2011), and eating to manage stress (Johnson, Risica, Gans, Kirtania, & Kumanyika, 2012) in domiciled samples. However, surprisingly little is known about how discrimination and other social stressors related to homelessness might influence diet, physical activity, and overweight/obesity in this vulnerable population.
The current exploratory pilot study was conducted to (a) describe the dietary characteristics (i.e., fruit/vegetable, fat, and fiber consumption), physical activity, and frequency of overweight/obesity in a sample of homeless adult smokers; (b) characterize the stressors experienced by this understudied group; and (c) examine associations between participant characteristics, stressors, and health risk factors. Results could yield important information about modifiable disease risk factors among homeless adults and provide direction for future research. Although the sample is restricted to homeless smokers, the exceedingly high prevalence of smoking among homeless adults suggests that findings might generalize to the majority of this population. Consequently, findings may have implications for shelter-based interventions and policy change.
Method
Participants and Procedures
Data were collected as part of a study designed to characterize the process of smoking cessation among homeless adults. Homeless adults (N = 57) were recruited to participate as they enrolled in a smoking cessation program at a homeless shelter in Dallas, TX. Eligibility criteria related to the smoking cessation study included the following: >6th grade English literacy level to ensure that participants were able to complete study assessments, willingness to quit smoking, age of ≥18 years, smoking level of ≥5 cigarettes per day, an expired carbon monoxide level ≥8 ppm suggestive of current smoking, and willingness to attend weekly smoking cessation treatment sessions. The current study analyzed data collected at baseline (i.e., prequit), with the exception of dietary risk factors, which were collected 1 week postenrollment (on the quit day).
Measures
Participant Characteristics
Participant characteristics measured in the current study included sociodemographics, smoking characteristics, and cardiovascular disease status. Sociodemographic information included age, sex, race, partner status, educational attainment (years), months of homelessness, and health insurance status. Smoking characteristics included years of smoking, number of cigarettes smoked per day, and time to first cigarette in the morning after waking. The Heaviness of Smoking Index was calculated based on cigarettes smoked per day and time to first cigarette (Borland, Yong, O’Connor, Hyland, & Thompson, 2010), with higher scores indicating greater nicotine dependence. Expired carbon monoxide level was assessed with a portable Vitalograph ecolyzer and reported in parts per million. Finally, participants were asked about their cardiovascular disease status (yes/no).
Stressors
Three types of stressors thought to be particularly relevant to homeless populations and potentially tied to modifiable risk factors were assessed: discrimination, chronic stress, and fear and mistrust. Discrimination was assessed with the Detroit Area Study Assessment of Everyday Discrimination, a 10-item self-report measure about the frequency of day-to-day experiences of discrimination (e.g., treated with less courtesy, people act as if they are afraid of you; Williams, Yu, Jackson, & Anderson, 1997). Chronic stress was assessed with the Urban Life Stress Scale, a 21-item self-report checklist of potential sources of chronic stress that may be experienced by individuals living in medium to large cities (Jaffee et al., 2005). Responses to each item ranged from 1 = No stress at all to 5 = Extremely stressful—More than I can handle. Fear and mistrust was assessed with the Fear & Mistrust scale, a 7-item self-report questionnaire that measures fear of being victimized (3 items) and mistrust of others (4 items; Ross & Jang, 2000). Some items were modified slightly to be appropriate for the current sample. Frequency of experiencing each item over the previous week was assessed from 1 = Never to 4 = Often.
Dietary Risk Factors
Three dietary risk factors were assessed using the National Health Interview Survey 2000-Diet, a 15-item questionnaire used to assess frequency of food intake in 16 broad categories to estimate intakes of fruits and vegetables, percentage of energy from fat, and fiber (Thompson et al., 2004). Inadequate fruit and vegetable consumption was indicated by an average of <5 servings of fruits and vegetables consumed per day (not including French fries) during the previous month. Inadequate fiber consumption was indicated by an average of <25 grams of fiber intake per day. A high-fat diet was indicated by a daily average of >35% energy intake from fat.
Insufficient Physical Activity
Physical activity was assessed using 7 items from the Behavioral Risk Factor Surveillance System Questionnaire: Physical Activity, which measured the quantity and frequency of moderate and vigorous leisure time physical activity over the previous week (Centers for Disease Control and Prevention, 2006). Insufficient physical activity was indicated by <150 minutes of moderate physical activity or <75 minutes of vigorous physical activity (or less than an equivalent combination of the two).
Overweight/Obesity
Body mass index (BMI) was calculated (kg/m2) based on staff-administered height and weight measurements (BMI ≥ 25 was overweight/obese, BMI ≥ 30 was obese).
Data Analyses
Descriptive statistics were used to examine participant characteristics, stressors, and modifiable health risk factors. Chi-square analyses assessed interrelations between the health risk factors. Participant characteristics and stressors were examined as predictors of health risk factors in a series of unadjusted logistic regressions. Finally, significant predictors of health risk factors were additionally examined in adjusted logistic regression analyses. Because four participants did not attend the quit date visit, the analyzable sample size was reduced (N = 53) for dietary outcomes.
Results
Participant Characteristics and Reported Stressors
Participants (N = 57) were predominantly non-White (54.4% Black; 3.5% Latino; 5.3% more than one race) and male. Most participants (89.5%) reported experiencing some discrimination (i.e., score >9), and major sources of discrimination, chronic stress, and fear and mistrust were related to homelessness. See Table 1 for participant characteristics and reported stressors.
Participant Characteristics and the Prevalence of Self-reported Stressors (N = 57).
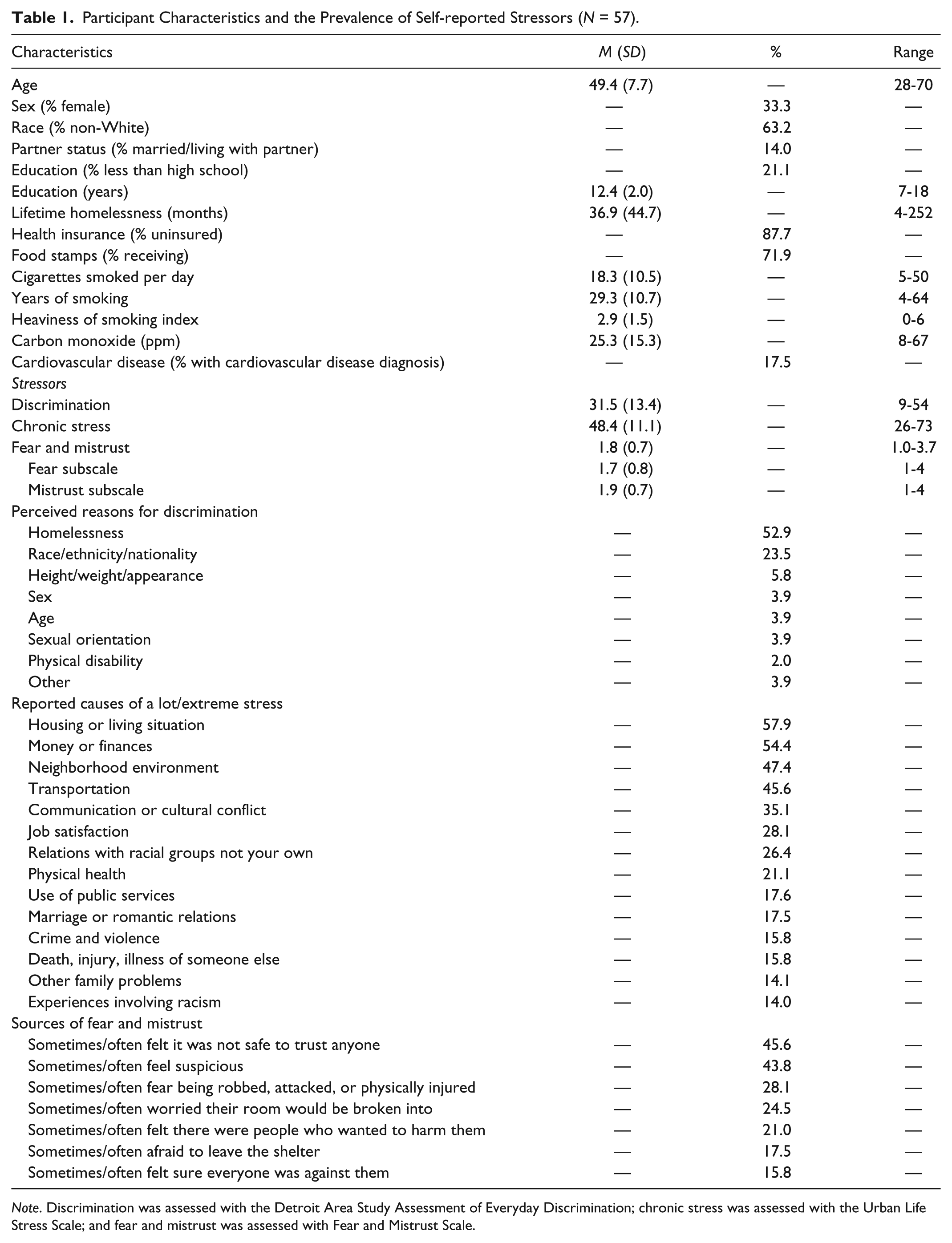
Note. Discrimination was assessed with the Detroit Area Study Assessment of Everyday Discrimination; chronic stress was assessed with the Urban Life Stress Scale; and fear and mistrust was assessed with Fear and Mistrust Scale.
Health Risk Behaviors and Their Interrelations
Over the previous month, 41.5% of participants reported consuming a high-fat diet (M = 37.0% daily energy from fat, SD = 8.8%), 77.4% reported eating less than five servings of fruits and vegetables per day (M = 4.4 daily servings, SD = 3.2), and 86.8% reported consuming <25 grams of fiber per day (M = 22.2 grams per day, SD = 34.7). During the previous week, 26.3% did not meet recommended physical activity guidelines. A total of 69.4% of participants were overweight or obese (29.8% obese), with a mean BMI of 28.1 (SD = 5.5). Males were more likely to be overweight/obese than females (p = .05; 73.7% vs. 47.4%), non-White individuals were more likely to be overweight/obese than Whites (p = .04; 75% vs. 47.6%). Having more years of education was associated with a high-fat diet (p = .047). Age was not related to dietary factors, physical activity, or overweight/obesity.
Overweight/obesity was significantly associated with insufficient physical activity (p = .040). Specifically, 10% of those with a BMI in the normal rage (BMI < 25) were not meeting physical activity guidelines, compared with 35.1% of overweight/obese (BMI ≥ 25) participants. Greater BMI (p = .049) and obesity (p = .04) were significantly associated with a high-fat diet, but not with inadequate consumption of fruits and vegetables or fiber, or insufficient physical activity. Specifically, 32.4% of nonobese participants (BMI < 30) reported consuming a high-fat diet, compared with 58.8% of obese (BMI ≥ 30) participants.
Predictors of Health Risk Factors
Higher scores on the discrimination (p = .04), fear and mistrust (p = .03), and chronic stress (p = .05) measures were associated with consuming a high-fat diet (see Table 2). Associations between key sociodemographic variables (age, gender, race, education, and BMI) and high-fat diet were examined, though only BMI and education were significantly associated with high-fat diet. Thus, additional logistic regression analyses adjusting for BMI and education, as well as models adjusting for all key sociodemographic variables (age, gender, race, education, and BMI), were conducted. Findings were similar to unadjusted analyses (see Table 2). Participant stressors were not associated with inadequate fruit/vegetable or fiber consumption, physical activity, or overweight obesity.
Associations Between Stressors and High-Fat Diet Among Homeless Adults (N = 53).
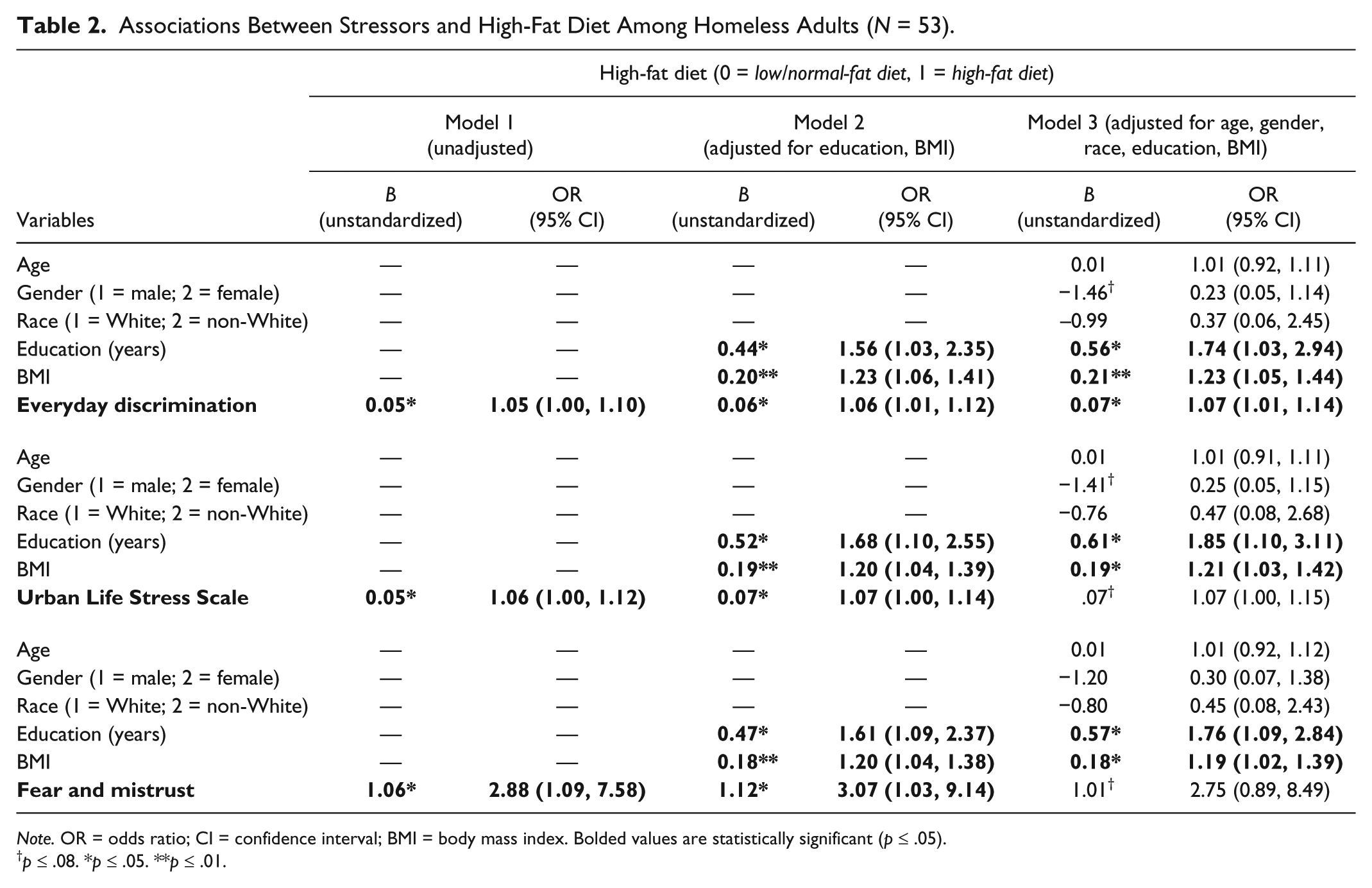
Note. OR = odds ratio; CI = confidence interval; BMI = body mass index. Bolded values are statistically significant (p ≤ .05).
p ≤ .08. *p ≤ .05. **p ≤ .01.
Discussion
The current exploratory study was conducted to characterize the dietary intake, physical activity, and frequency of overweight/obesity in a vulnerable population of homeless smokers, and to better understand how discrimination and other relevant social stressors might relate to associated health risk factors. Results indicated a high prevalence of poor diet (e.g., inadequate fruit/vegetable, fiber consumption, and high-fat diet), insufficient physical activity, and overweight/obesity. In addition, participants endorsed high levels of stress related to discrimination experiences, fear and mistrust, and numerous other specific stressors related to homelessness (e.g., housing/living situation, money/finances). Importantly, a key finding was that higher scores on measures of stress (i.e., everyday discrimination, fear and mistrust, and chronic life stress) were associated with a high-fat diet.
This is the first study to link measures of stress relevant to homelessness with a high-fat diet, thereby providing evidence of a behavioral pathway through which stress may have a negative impact on health. This finding is consistent with animal models of stress and feeding behavior indicating that consumption of highly palatable and energy dense “comfort foods” increase in response to stress (Pecoraro, Reyes, Gomez, Bhargava, & Dallman, 2004). In animal models, increased consumption of comfort foods appears to attenuate hypothalamic–pituitary–adrenal axis activity. Thus, it is possible that “comfort food” may also attenuate the physiological effects of stress among homeless adults. Further study is needed to characterize obesity-related health behavior and the link between stress and high-fat diet in a larger, representative sample of homeless adults. Longitudinal studies that collect information on the sources of high-fat foods (e.g., shelters, fast food restaurants, convenience stores), the types of foods consumed, and the associated context of consumption (e.g., acute vs. chronic stress) will be especially important to increase understanding in this area.
High levels of chronic stress are likely to have effects on health behavior and health over time, and therefore may warrant attention through changes in the shelter environment (e.g., increased security presence) and individual-level intervention to reduce stress and/or the effects of stress (e.g., coping skills training) in this homeless population. Plausibly, such actions may influence homeless smokers’ dietary intake, including fat consumption. In addition, excesses in dietary fat and deficiencies in fruit, vegetable, and fiber consumption may possibly be attenuated by offering more nutritious foods at the shelter (i.e., increasing access to nutritious foods), and encouraging shelter residents to limit meals from fast food restaurants. Shelter residents may benefit from nutrition and lifestyle counseling, on-site exercise equipment, and encouragement to increase walking or other lifestyle activities. The findings of the current exploratory study are intriguing, though more research is needed to increase understanding of the factors that influence diet and physical activity among homeless adults. Practical intervention strategies may be beneficial to the health of homeless adults, such as providing fresh fruits/vegetables as snacks along with pedometers and walking goals (e.g., homeless adults may be more likely to walk for transportation) at the shelter. Although shelter-based environmental changes may increase costs in the short term, it is possible that such changes may decrease health care costs and improve health in the longer term.
Footnotes
Acknowledgements
We are grateful for the contributions of the following research team members, Erica Cuate, Anshula Kesh, and Insiya Poonawalla, who were integral in the data collection and database design.
Authors’ Note
This research was approved by the University of Texas Health Science Center Committee for the Protection of Human Subjects, and informed consent was obtained from all participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by the University of Texas Health Science Center, School of Public Health. Data analysis and manuscript preparation were additionally supported through American Cancer Society grants MRSGT-10-104-01-CPHPS (to DEK) and MRSGT-12-114-01-CPPB (to MSB).