
Abstract
The inclusion of parents in adolescent-targeted interventions is intended to benefit the adolescent. Limited research has explored whether parents participating in these programs also benefit directly. We examined the impact of Caribbean Informed Parents and Children Together, the parenting portion of an adolescent-targeted HIV prevention intervention, on parent-reported measures. Bahamian parent–youth dyads (N = 1,833) participating in the randomized control trial were assigned to receive one of four conditions. Parents were assessed longitudinally at baseline and 6 and 12 months later. Through 12 months follow-up, parents exposed to Caribbean Informed Parents and Children Together showed higher knowledge of condom use skills, perceptions of improved condom use competence on the part of their youth, and perceived improved parent–child communication about sex-related information. Although youth were the targeted beneficiary, parents also benefited directly from the sexual risk reduction parenting program. Parents demonstrated improved perceptions and knowledge that would enable them to more effectively guide their child and also protect themselves from sexual risk.
Keywords
Rapid changes in social, physical, and cognitive development during adolescence present a wide array of challenges, potentially leading to health-compromising situations as evidenced by data showing that adolescents and young adults make up a third of new cases of HIV (Centers for Disease Control and Prevention [CDC], 2012). Reviews of HIV prevention intervention programs serving youth highlight the value of including family and communities (Burrus et al., 2012; CDC, 2012). Historically, parents have been one of the few sources of information regarding sexual health for adolescents; the inclusion of parents in adolescent sexual risk reduction programs is intended to open discourse on this topic between parents and youth and to increase the likelihood that the information parents are providing is accurate (Stanton et al., 2004; Villarruel, Cherry, Cabriales, Ronis, & Zhou, 2008).
Traditionally, adolescent risk prevention intervention trials, including those with a parent component, are designed to determine if there is benefit to the child (Hutchinson, Jemmott, Jemmott, Braverman, & Fong, 2003; Stanton et al., 2004). The main objective has been to assess whether parents can effectively act as a source of knowledge and guidance for their child as measured by improvements in the adolescent’s behavior and knowledge. A few studies have found that following their participation in such interventions, parents display improved perceptions of their relationship and communication skills with their adolescent and increased perceived benefit to the child (Bogart et al., 2013; Hutchinson et al., 2003). Increased knowledge related to sexual health has also been explored to a lesser extent (Baptiste et al., 2009).
To date, limited research has been designed to assess the impact on parents’ skills such as those related to proper condom use. Such information is important to enable parents to accurately reinforce knowledge and skills being transmitted from risk reduction interventions to their children and to feel confident in their ability to do so. Moreover, increased experience in communicating sex-related information may result in more open communication about a wider array of challenges facing youth. Finally, parents themselves may face potentially sexually risky situations and/or may be in a position to advise other adults or youth. Thus, the potential beneficiaries of these interventions extend beyond the individual targeted youth or context.
Implementation of parent-targeted interventions has been challenged by issues related to recruitment and retention (Spoth, Clair, Greenberg, Redmond, & Shin, 2007). Many programs are long, consisting of numerous hours over a single session (Baptiste et al., 2009) or numerous sessions within a period of weeks or months, resulting in incomplete intervention exposure (Armistead et al., 2014).
To address these issues, the current study examined the impact of a brief parenting intervention component (1-hour session plus booster sessions 6 and 12 months later) of a school-based randomized control trial of an adolescent sexual risk reduction intervention. We hypothesized that parents exposed to the parenting intervention would exhibit increases in condom use skills knowledge and positive perceptions of their parental monitoring and parent–adolescent communication about sex-related topics and of their adolescent’s condom use skills.
Method
Data
Participants included 1,833 parents of Grade 10 youth sampled from all 8 government high schools on the island of New Providence, The Bahamas. All participants were of African descent. The parents and youth were recruited to participate in a randomized trial of Bahamian Focus on Older Youth (BFOOY; Dinaj-Koci et al., 2012). Youth were randomized to receive one of two conditions, BFOOY or the Health and Family Life Education (HFLE) curriculum during their health period class taught by trained teachers. BFOOY is a 10-session risk reduction intervention based on the protection motivation theory (Maddux & Rogers, 1983) designed to improve threat and coping appraisals of risk-related situations and increase HIV-related skills and knowledge (see Dinaj et al., 2012; Wang, Stanton, Deveaux, Li, Dinaj-Koci, & Lunn, 2014, for intervention details). HFLE, the current standard of care in The Bahamas, provides a broad range of health-related knowledge and facts including sexual health topics.
Parents of youth participating in the BFOOY trial who agreed to participate in the parent component of the trial were randomized to receive one of three parent intervention conditions (see Figure 1). The first intervention condition, Caribbean Informed Parents and Children Together (CImPACT), is a one-session intervention in which the parents and their child watch a short video (~20-minute) on communication about sex-related topics and parental monitoring (Dinaj-Koci et al., 2012; Stanton et al., 2004). Discussion and two parent–child role-play vignettes follow, and the session concludes with a condom use demonstration and practice. In total, the primary intervention was approximately 1 hour in length. At 6 and 12 months postintervention, these parents and youth were invited to engage in 40-minute booster sessions reinforcing information about communication, monitoring and condom use through a small-group discussion consisting of parents and youth. The second condition (attention-control), Goal for It (GFI), included a ~20–minute video informing parents about career planning, whether for themselves, their children, or someone else, followed by a discussion regarding the skills presented in the video. A 40-minute booster session at 6 months consisting of a lecture/discussion reinforcing intervention lessons was offered. In the third condition (current standard of care), parents received no intervention.
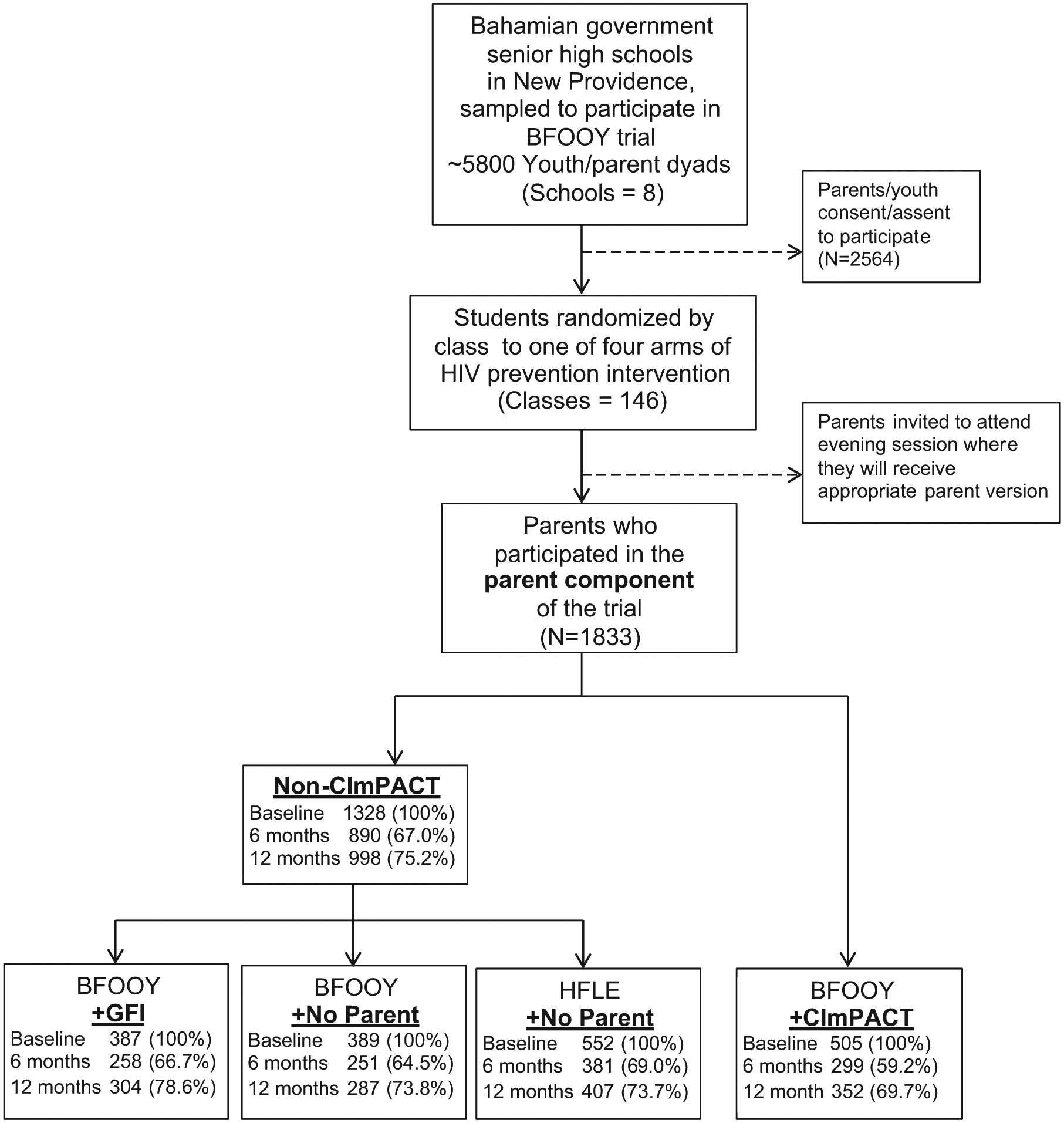
CONSORT (Consolidated Standards of Reporting Trials) diagram for parent participants of CImPACT study.
Previous analyses have found improvement in condom use skills knowledge, condom use self-efficacy, and parent–adolescent communication among youth whose parents were exposed to CImPACT compared to youth whose parents were not exposed to CImPACT (Dinaj-Koci et al., 2012; Wang et al., 2014). The focus of the current study is to examine the impact of the parent intervention, CImPACT, on parent outcomes.
The trial included four possible combinations of parent and youth intervention exposure: BFOOY + CImPACT, BFOOY + GFI, BFOOY + No parent intervention, and HFLE + No parent intervention. Because initial analyses found minimal differences between the three non-CImPACT groups (see columns BFOOY + No Parent, BFOOY + GFI, and HFLE + No Parent of Table 1), these groups were subsequently combined to examine the effect of having received or not having received CImPACT on parent outcomes.
Effect of CImPACT on Parent Skills and Perceptions.

Note. CImPACT = Caribbean Informed Parents and Children Together; HFLE = Health and Family Life Education; BFOOY = Bahamian Focus on Older Youth; GFI = Goal for It.
Parents not exposed to any intervention only received assessment. bIncludes all parents not exposed to CImPACT (i.e., Goal for It and no intervention).
p < .10. *p < .05. **p < .01.
Following randomization, parents were invited to attend the after-school session at their child’s school. Parents completed the questionnaire described below prior to receiving the assigned intervention or booster. Assessments were completed at baseline and 6 and 12 months postintervention for all parents. Protocols for this study were approved by Human Subjects Review Board of the Bahamas Ministries of Health and of Education and Wayne State University.
Measures
The condom use skills checklist (Stanton et al., 2009) is a validated and reliable proxy for condom skills. The checklist presents 16 statements from which the parents were asked to mark the eight correct steps regarding condom use procedure (Cronbach’s α ranged from .43 to .48). Scores were based on the percentage correctly marked.
Parents’ perceptions of youth condom use efficacy were measured on a 5-point Likert-type scale (yes, he/she could, maybe he/she could, don’t know, probably he/she could not, no, he/she could not). The seven-item scale was adapted from the condom use self-efficacy items in the Youth Health Risk Behavior Inventory (Stanton et al., 1995) for the purpose of assessing whether parents believed that their youth could effectively use condoms to protect themselves from sexual risk. For example, items asked if they thought that their youth could obtain condoms, negotiate condom use with a partner, and use a condom correctly (Cronbach’s α ranged from .77 to .80).
An eight-item parental monitoring (Small & Silverberg, 1991) scale assessed whether the parents believed that they knew the whereabouts of their youth and were involved in their youth’s activities (Cronbach’s α ranged from .82 to .86). Responses were on a 5-point Likert-type scale (always, most of the time, sometimes, hardly ever, never). Example items include “I know where my child is after school” and “When my child goes out I ask where they are going.”
Parent–adolescent communication about sex was measured on a 5-point Likert-type scale (none, a little, some, a lot, extensive) assessing how much information the parent provided their youth regarding sexual risk topics including HIV, condom use, and coping with sexual pressure (Cronbach’s α = .92 at all three assessments).
Results
Intervention effect was assessed using the general linear modeling procedure, PROC GLM, from SAS 9.4. Analyses controlled for age (mean age = 14.5 years, SD = 0.7) and gender of youth (44.6% male), parent gender (87.3% mothers, 11.7% fathers, <0.01 missing) and baseline scores. The attrition rate was higher in CImPACT (40.8%) than non-CImPACT (33.0%) at 6 months (χ2 = 9.79, p < .05) and CImPACT (30.0%) was higher than non-CImPACT (24.9%) at 12 months (χ2 = 5.59, p < .05) found at 12 months. At baseline, those who were lost at follow-up had lower condom use skills knowledge and parental monitoring.
At baseline parents did not differ by intervention condition (Table 1). Postintervention, parents who received CImPACT compared to parents in the non-CImPACT group showed greater increases in condom use skills knowledge at 6 months, F(1, 1,104) = 14.07, p < .001, d = 0.26, and 12 months, F(1, 1,240) = 6.77, p < .01, d = 0.20, and at 12 months perceived their youth to be more competent in their ability to use condoms (condom use efficacy), F(1, 1,311) = 11.00, p < .01, d = 0.24, and improved communication about sex, F(1, 1,315) = 4.59 p < .05, d = 0.11. Parental monitoring did not differ by groups. Results of the analyses examining all subgroups of the non-CImPACT exposed were similar to the results of the combined non-CImPACT group and are reported in Table 1.
Discussion
There is strong evidence that youth benefit from parental communication and monitoring interventions regarding sexual risk reduction (Armistead et al., 2014; Baptiste et al., 2009; Stanton et al., 2004; Villarruel et al., 2008). The present study reveals that parents also received direct benefits through participation in a brief communication and monitoring portion of an adolescent HIV prevention program; over time, they demonstrated higher condom use skills knowledge, perceived improvement in communicating sex-related topics, and also perceived their adolescent to have greater condom use efficacy.
Increases in parent skills are presumed to improve youth outcomes. Our previous research revealed that parental participation in CImPACT improved adolescent health-related outcomes demonstrated by increased knowledge of condom use skills and perceived condom use self-efficacy (Dinaj-Koci et al., 2012) and reported parent–child communication about sex (Wang et al., 2014) among adolescents participating in the BFOOY trial. The present findings suggest possible mechanisms that lead to these improvements in youth health behavior; parents showed the greatest improvements in their perceptions of parent–youth communication about sex and enhanced parental condom use skills knowledge. These new skills and knowledge may allow them to be more confident in discussing condom use with their children. While parents may be perceived as more knowledgeable than their adolescent, the parental improvements in condom use skills knowledge found in the present study indicate that there is always an opportunity for improvement. Additionally, results show that youth exposure to the sexual health intervention alone did not improve parent scores when compared to parents who received CImPACT. Although youth could potentially transfer their newly acquired knowledge from the intervention to their parent, parents derive greater benefit from their own direct participation in an intervention. Parents are expected to (and want to) provide their youth with information regarding safe sexual practices; such programs would ensure that they have the knowledge and ability to convey the right information to their youth. As well, this information could potentially be used in their own sexual decision making or in their parenting of other children, thus extending the impact beyond the targeted adolescents.
Parents also perceived increases in their adolescent’s condom use efficacy, which may influence their perceptions of the efficacy of the program and affect their future participation. Parent participation can also be hampered by issues such as time constraints. A strength of CImPACT is that it is brief in comparison with many other programs that include parents (Akers, Holland, & Bost, 2011). Our findings with CImPACT indicate that programs can be implemented in easily accessible settings such as the students’ classrooms and need not require substantial time commitments to confer benefit to both the parents and youth. While greater exposure may further increase benefits, even a brief intervention can be effective, which may be useful in resource-limited environments.
Differences in improved perceptions of adolescent condom use skills knowledge and parent communication of sex-related information were significant at 12 months postintervention but not 6 months. CImPACT parents may have found it more developmentally appropriate to discuss these topics when the adolescent was older. It is also possible both non-CImPACT- and CImPACT-exposed parents may have initiated discussing sex-related topics at the first follow-up; however, the CImPACT parents may have felt more successful and comfortable continuing these discussions through the second follow-up. Further research is needed to understand how parent interventions affect the trajectory of parent–child sexual health discussions.
A limitation of this study is the use of self-report measures of perceptions, which may produce biased findings due to social desirability (Hebert, Clemow, Pbert, Ockene, & Ockene, 1995). Moreover, the high parental monitoring scores reported by all groups may have resulted in a “ceiling effect,” limiting necessary variance needed to detect differences. The condom use skills checklist, however, is an objective assessment of the parent’s knowledge of condom use and showed significant improvement in the CImPACT group (Stanton et al., 2009). The relatively low reliability scores using Cronbach’s alpha seen with the condom use scale in this study compared to prior studies have been observed with other knowledge scales that can vary greatly from sample to sample due to the propensity to guess or not answer affecting the internal consistency (Mondak, 2001). Finally, attrition rates were higher in the CImPACT group. While youth were expected to attend the baseline session with their parents for all intervention conditions, their presence was strongly encouraged for CImPACT at 6 and 12 months, while there was less emphasis on subsequent youth attendance for the other groups. Thus CImPACT parents may have been reluctant to attend without their child, a feeling not shared by the parents in the other groups. This differential attrition may bias results.
Our findings highlight the importance of including parents in adolescent intervention programs, in this case a program emphasizing skills and communication regarding sexual risk reduction. As indicated by the effect of the intervention, CImPACT, these programs provide parents with the opportunity to become more knowledgeable and skilled for more complex issues such as protection against sexual risk.
Footnotes
Acknowledgements
We thank the National Institute of Mental Health (R01 MH069229) and the Bahamian Ministries of Health and Education for their support. We would also like to thank Nanika Braithwaite for her help with data management, and the families and schools for their participation in our study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support from the National Institute of Mental Health (R01 MH069229) and the Bahamian Ministries of Health and Education.