
Abstract
As resources for health promotion become more constricted, it is increasingly important to collaborate across sectors, including the private sector. Although many excellent models for cross-sector collaboration have shown promise in the health field, collective impact (CI), an emerging model for creating larger scale change, has yet to receive much study. Complementing earlier collaboration approaches, CI has five core tenets: a shared agenda, shared measurement systems, mutually reinforcing activities, continuous communication, and a central infrastructure. In this article, we describe the CI model and its key dimensions and constructs. We briefly compare CI to community coalition action theory and discuss our use of the latter to provide needed detail as we apply CI in a critical case study analysis of the Tenderloin Healthy Corner Store Coalition in San Francisco, California. Using Yin’s multimethod approach, we illustrate how CI strategies, augmented by the community coalition action theory, are being used, and with what successes or challenges, to help affect community- and policy-level change to reduce tobacco and alcohol advertising and sales, while improving healthy, affordable, and sustainable food access. We discuss the strengths and weaknesses of CI as a framework for health promotion, as well as the benefits, challenges, and initial outcomes of the healthy retail project and its opportunities for scale-up. Implications for health promotion practice and research also are discussed.
Keywords
Health promotion and public health are rooted in understanding and addressing the primary causes of health problems, and collaboration has long been a crucial component of these efforts. Such collaboration is often driven by an organization or a group of individuals realizing that they can better tackle a shared concern together. Increasingly, however, funders are encouraging or even mandating collaboration in proposals to address complex health and social problems. The Centers for Disease Control and Prevention (CDC; Martin et al., 2009) and over half of the divisions within the National Institutes of Health have called for proposals encouraging community engagement in research (Mercer & Green, 2008). Similarly, both large philanthropic entities such as the W. K. Kellogg Foundation and many regional and local foundations now welcome applications from community-engaged partnerships to study and address health inequities (Mercer & Green, 2008; Wallerstein, Stone, Garcia, & Minkler, in press).
Despite these positive signs, the large chasm between funding availability and public health need continues to encourage single entities (e.g., a health department or university-based research team) to compete for limited financial support. Testing new theoretical approaches and building the evidence base on the effectiveness of cross-sector collaboration are therefore critical.
Many excellent collaborative models and theories have demonstrated utility in health promotion and related fields. Key among these are Butterfoss and Kegler’s (2009) “Community Coalition Action Theory” (CCAT; Butterfoss, 2013); Bandura’s (2004) theory of collective efficacy; Lasker, Weiss, and Miller’s (2001) Partnership Synergy; and Wolff’s (2010) Power of Collaborative Solutions. Arguably, the most rigorously developed of these models in health promotion and education is the CCAT, with its clearly laid out constructs, definitions, and propositions and proven track record in the study of action-focused coalitions. As Butterfoss (2013) suggests, however, CCAT and other collaborative approaches in health promotion may usefully contribute to a promising new approach—collective impact (CI)—that to date has received little testing in public health and health promotion.
As described below, CI (Hanleybrown, Kania, & Kramer, 2012; Kania & Kramer, 2011) is an emerging model for creating large-scale social change. Like CCAT, it is action oriented and engages organizations and individuals affected by the issue of concern, as well as those influencing the issue. Similarly, both models aim to create sustained change in diverse sectors, with CI placing a special accent on public–private partnerships. Several of CIs five core tenets—a common agenda, shared measurement, mutually reinforcing activities, continuous communication, and backbone organization—and basic phases also show similarities to CCAT, with the latter providing more detail on ways to build, improve or sustain the backbone organization, while also emphasizing advocacy—a missing piece of the CI model.
Despite some limitations discussed later, the CI model is gaining adherence in the fields of health promotion and public health more broadly, as suggested in the recent choice of this model as the theme of the 2015 national Childhood Obesity Conference and of the California Tobacco Control Project Director’s Meeting (2013). Such attention underscores the importance of exploring the utility and drawbacks of CI through a health promotion lens.
Reflecting the newness of the model, few articles have applied CI in health promotion research and practice, despite hundreds of applications of the more generic term, collective impact, to indicate interdisciplinary work, public–private partnerships, and the like (Flood, 2013). Two exceptions are Shape Up Somerville, an effective, evidence-based citywide obesity prevention initiative in Massachusetts (FSG, 2013) and the Alcohol, Nutrition and Tobacco (ANTS) program in Sonoma, California (Ronshausen, Newman-Fields, Swendlberg, & Maceado, 2014). Although a full discussion of these interventions (Burke et al., 2009; Economos et al., 2007; Flood, 2013; FSG, 2013; Ronshausen et al., 2014) is beyond the scope of this article, both have applied the core tenets of the CI model. Shape Up Sommerville, for example, is a collaborative of 15 community, public, and private partners who, with a city government backbone organization, have successfully improved infrastructure and championed policies to reduce childhood obesity through increased physical activity and healthy eating. ANTS similarly has the local health department as its backbone organization and has engaged cross-sector partners to transform 16 food retail outlets to date into healthier retail establishments. Both programs have demonstrated success employing this framework; however, their use of CI has been discussed in the gray, rather than peer-reviewed, literature and does not include critical appraisal of CI in these contexts.
To augment the sparse literature to date applying the CI model in health promotion, we critically examine the model’s utility as a framework for a case study analysis of a collaborative effort to study and address high tobacco outlet density and poor access to healthy foods in San Francisco’s Tenderloin district and its scale-up through a citywide healthy retail program. Although other approaches, and particularly the CCAT, have been more thoroughly tested and found relevant for use in evaluating coalition processes and outcomes, our goal was to critically apply and test the newer CI model precisely because it is increasingly discussed in health promotion circles but without much empirical investigation. As our case study application suggests, CI appears to have utility as a conceptual framework in health promotion but one that may usefully be augmented by some “tried and true” insights and strategies from CCAT.
We begin by describing CI and its core tenets and phases and briefly comparing CI to CCAT. Following background on the San Francisco’s Tenderloin district and its Tenderloin Healthy Corner Store Coalition (TLHCSC or “the Coalition”), we describe the multimethod case study approach (Yin, 2003) used in this study. We then describe and critically analyze the Coalition and its processes and outcomes within a CI framework, with supplementation from CCAT. We discuss the challenges and benefits of CI, as well as implications for its potential further use, ideally in conjunction with the more developed CCAT or other collective action models in health promotion research, practice and policy.
The Collective Impact Model
Developed initially in business (Hanleybrown et al., 2012; Kania & Kramer, 2011), CI was designed as a model for collaboration to address complex problems by aligning partners across government, nonprofit, philanthropic, and private sectors and fully engaging members of the community. CI attempts to eliminate duplication of efforts while enhancing impact by attacking an issue from multiple angles with coordination and sharing of lessons learned (Kania & Kramer, 2011). The model includes several prerequisites to its three phases (Hanleybrown et al., 2012)—initiating action, organizing for impact, and sustaining action and impact—as well as the five core tenets discussed below (see Tables 1 and 2).
The Collective Impact Model: Phases and Core Tenets.
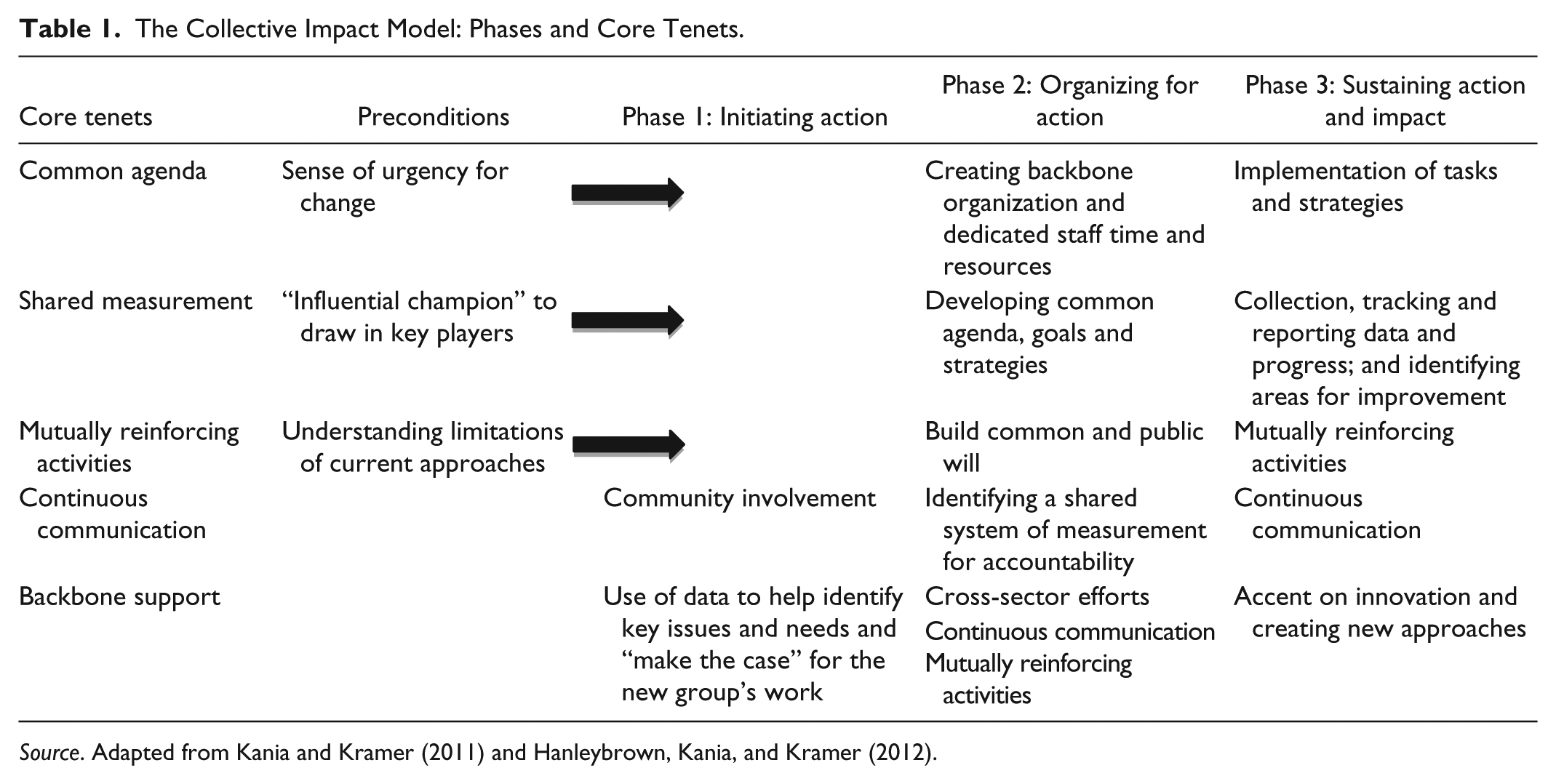
Source. Adapted from Kania and Kramer (2011) and Hanleybrown, Kania, and Kramer (2012).
Core Tenets and Conditions of Collective Impact.
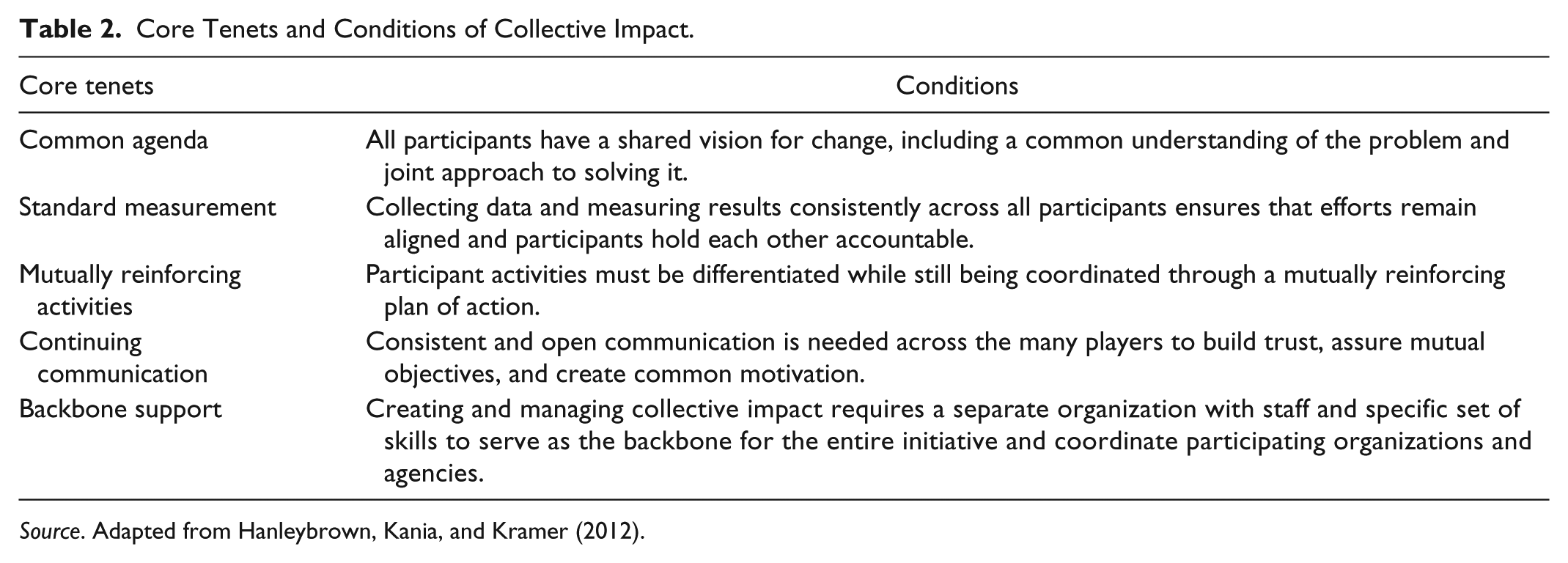
Source. Adapted from Hanleybrown, Kania, and Kramer (2012).
Phases and Core Tenets of Collective Impact
Preconditions
Hanleybrown et al. (2012) discuss several prerequisites needed for CI’s successful application: adequate financial resources, an “influential champion” to engage decision makers and stakeholders across sectors, a “sense of urgency” for change, and an understanding that current approaches are insufficient.
Phase 1: Initiating Action
As Hanleybrown et al. (2012) note, “Initiating action requires an understanding of the landscape of key players and the existing work underway, baseline data on the social problem to develop the case for change, and an initial governance structure that includes strong and credible champions” (p. 6). Many of these preconditions continue in Phase 1, when the collaborative is convened and the structure of communication and decision making is created. The influential champion continues engaging cross-sector leaders and decision makers from diverse organizations with a stake in the issue. Community involvement also is critical, and facilitation of community outreach is therefore a key part of CI’s first phase. Data play an important early role, as analysis of data helps the group identify key issues and needs and make the case for their efforts (Hanleybrown et al., 2012).
Phase 2: Organizing for Impact
Phase 2 involves establishing a process for the group, including creating a backbone/infrastructure for organizing the partners, establishing a common agenda with outlined goals and strategies, developing shared metrics and the overall approach to measurement, creating workgroups and tasks, and continuing to engage the community and build public will. Creating a central infrastructure or backbone requires assigning dedicated, adequate staffing, and financial resources to organize the group. Creating a common agenda is a facilitated process requiring the group to define a mutual desire for change focused on solving a specific problem (Bandura, 2004; Hanleybrown et al., 2012). Each entity may have different perspectives on how best to address that issue, which should be discussed as a part of setting the common agenda. However, to promote unity and enable true impact, individual agendas must be replaced or amended to include a collective one. Identifying a shared system for measurement holds the group accountable to its goals and ensures that cross-sector efforts remain aligned.
Phase 3: Sustaining Action and Impact
Once the group process is established, the focus shifts to implementation of tasks and strategies identified in Phase 2, as well as to collection, tracking, and reporting of progress data. Engagement and advocacy among the affected community remain critical during this phase, as does continuous communication, which helps the group refine and further its work. Finally, as part of the refinement process, the group must create a method for reflecting on its process and identifying improvements. For instance, the collaborative might discuss how frequently it meets, who is regularly engaged, who is missing from the table, and how that may be influencing the collaborative’s progress—or lack of progress—toward reaching the ultimate goal, or shared agenda.
Mutually reinforcing activities and continuous communication are fully employed during this phase. Members of the collaborative engage in different activities that work toward the same goal, so that all parts of the continuum of the issue are changing simultaneously. Innovation is important in this stage, as CI is based on creating an approach instead of adopting an existing approach to a problem (Hanleybrown et al., 2012). Innovation relies on continuous communication and learning via feedback loops among the organizations.
Collective Impact and Community Coalition Action Theory: A Brief Comparison
The CI model’s three phases—initiating action, organizing for impact, and sustaining action and impact—bear many similarities to those of the CCAT—formation, maintenance, and institutionalization. In Phase 1, both models stress the importance of multiple constituents, with CCAT placing an even stronger emphasis on community. As Butterfoss and Kegler (2012) note, “Members are the life blood of a coalition—they set its vision, course and outcomes, and reflect the authentic voice of the community” (p. 322). The CI model’s emphasis on sufficient resources to do the work is also stressed in the CCAT, whose authors indicate the imperative for resources supporting the backbone organization staff’s ability to devote significant time to the coalition, independent from their preexisting work. Additionally, the CCAT emphasizes the importance of the backbone organization’s provision of “technical assistance, . . . credibility and valuable networks/contacts” for the collaborative as a whole (Butterfoss & Kegler, 2012, p. 318).
The mutually reinforcing activities and continuous communication highlighted also appear similar to those outlined in more detail in the CCAT. The latter theory emphasizes, for example, “open and frequent communication among staff and members” making “collaborative synergy more likely though member engagement and pooling of resources” (Butterfoss & Kegler, 2012, p. 318). Finally, the CI model’s five core tenets (Hanleybrown et al., 2012) include several (e.g., a common agenda, mutually reinforcing activities, and a backbone organization) also stressed in CCAT and other models for collaboration (Bandura, 2004; Lasker et al., 2001; Wolff, 2010).
Despite the similarities, however, a number of critical differences exist between the models. First, the CCAT is, by definition, concerned with community-based coalitions in which resident involvement is key. Although at least two health promotion applications of CI have engaged community members (Shape Up Sommerville and ANTS), CI efforts typically bring together CEOs of nonprofit organizations with business leaders and funders to help study and address social problems (Hanleybrown et al., 2012). Second, as discussed below, the CI model is not explicitly focused on policy, and indeed the word “advocacy” does not appear in articles by CI’s authors (Hanleybrown et al., 2012; Kania & Kramer, 2011). Since many community coalitions are deeply concerned with advocacy and policy change (Minkler, 2010), this omission may be problematic. In this respect too, the CCAT offers important additional precepts and strategies for collaborative efforts that seek to “increase community capacity [while improving] health and social outcomes” (Butterfoss & Kegler, 2012, p. 317).
Given these realities, we approached using CI as a framework carefully, aware of the model’s limitations, yet also aware that it resonated with members of the TLHCSC, as well as with a growing number of health promotion and education practitioners. Fostering dialogue about its utility and limitations, in part through its application to a case study with additional insights from the CCAT, seemed a logical next step.
Overview of the Tenderloin and Its Healthy Corner Store Coalition
The Tenderloin is one of San Francisco’s poorest neighborhoods, with 35% of its 35,000 residents living below the federal poverty line, compared to 14% citywide (city data, 2011). With no full-service grocery store and 70 corner stores primarily stocking prepackaged food, tobacco, alcohol, and sodas, food access is a significant problem contributing to the neighborhood’s high rates of heart disease, cancer, and premature death (San Francisco Department of Public Health [SFDPH], 2012).
The precursor to the TLHCSC (www.healthyTL.org) evolved in 2011 out of a tobacco-free initiative. Several local groups and organizations came together after a youth-driven assessment graphically illustrated the high tobacco advertising and availability and extremely poor access to healthy foods in neighborhood corner stores. In addition to a wide range of organizational and individual members, the Coalition, which formalized the following year, included five “Food Justice Leaders” (FJLs). Modeled in part on the Food Guardians of South East Food Access (SEFA; www.southeastfoodaccess.org) in the Bayview–Hunters Point (BVHP) neighborhood, the FJLs are Tenderloin residents hired and trained as food systems researchers and advocates. Their detailed store assessments, resident surveys, and merchant and resident education, together with the work of the larger Coalition, have been complemented by their use of data and personal stories to effect policy change. The group’s community-based participatory research (CBPR) and advocacy were described by policy makers as playing an important role in the passage and implementation of the city’s 2013 “Healthy Food Retailer Incentive Program” legislation (sfsbdc.org/HealthyRetailSF), dubbed “Healthy Retail SF” (HRSF). The program, housed in the Office of Economic and Workforce Development (OEWD) in partnership with the SFDPH, collaborates closely with the Coalition, which selected stores to receive “redesigns” and other benefits in exchange for making health-promoting changes. The Coalition’s help is increasingly being sought out for related healthy retail measures, including a recent soda tax measure.
Method
To study the Coalition, we used Yin’s (2003) case study method, which involves “empirical investigation of a contemporary phenomenon within its real life context [using] multiple sources of evidence” (p. 23). Data collection methods included in-depth interviews (total n = 9) with Coalition members (n = 7) and policy makers (n = 2) interested in healthy retail; a focus group with the FJLs (n = 5); participant observation at Coalition meetings, community forums, hearings, and meetings of the city’s HRSF Advisory Committee; and archival review of internal documents, media coverage, and other sources.
With approval from University of California (UC) Berkeley’s Institutional Review Board, two UC researchers, who also became Coalition members, collected data from fall 2013 through summer 2014. Consistent with the principles of CBPR (Israel, Eng, Schulz, & Parker, 2013), provisions for shared ownership of data and community partner coauthorship were established.
The 40 to 60-minute semistructured interviews were conducted in person or by phone, and the 15-minute policy maker interviews by phone. The focus group occurred during a FJL weekly meeting. Participant observation occurred over 9 months, and multisource archival review provided context for interviews, observations, and focus group findings.
The interviews and focus group addressed key domains (e.g., partnership genesis, adherence to CI tenets, capacity building, success factors and barriers, and perceived contributions to healthy retail at local and/or policy levels). Recordings were transcribed and analyzed independently by the two UC researchers, who identified emergent themes related to the CI tenets and preconditions. Successes and challenges were also explored thematically, with key themes compared and reconciled, and with each theme analyzed alongside data from meeting observations and archival review for contextualization and triangulation. Following this process, two key Coalition leaders and coauthors provided member checking and help with data interpretation.
Applying the Collective Impact Model to the TLHCSC
The TLHCSC was officially created in 2012 by local agencies and organizations concerned about lack of healthy food access and prevalence of alcohol and tobacco advertising and sales in the neighborhood. Although the Coalition did not intentionally invoke CI, it became clear to the researchers, who joined the group several months after its creation, that the Coalition appeared to be engaging in a CI approach. After Coalition members attended either the CI-themed California State Project Directors’ Tobacco Control Meeting or the training offered by the UC researchers, the group as a whole decided that CI’s framework aligned well with its work. We agreed to examine the genesis, goals, leadership, functioning, and initial outcomes of the Coalition using a CI framework, both to explore the model’s utility and to “tell the story” of the Coalition.
Preconditions for Collective Impact
An influential champion is important, even before the formal Coalition begins, in helping to engage multiple and key decision makers. Although not a formal Coalition leader, a respected member of SFDPH, who earlier had helped catalyze partnerships in the BVHP neighborhood (Breckwich et al., 2007; Hennessey-Lavery et al., 2005), was viewed by many interviewees as playing this role. Her introduction of the Tenderloin organizations to the BVHPs, SEFA, and “Food Guardians”—young people conducting research, education, and advocacy—was particularly helpful in spurring cross-fertilization and partnerships across neighborhoods. Even before the Coalition came into being, however, members of the Vietnamese Youth Development Center (VYDC) served as influential champions, collecting and sharing data showing the high prevalence of tobacco and lack of access to healthy food in the neighborhood (see Table 3). Another critical precondition to CI is sense of the urgency of change, along with realization of the limitations of existing, typically siloed, approaches (Hanleybrown et al., 2012). In the Tenderloin, multiple agencies were attempting to address, independently and in their own ways, the problems of food access, alcohol and tobacco, safety, and preventable diseases. A sense of urgency was identified and catalyzed by the VYDC’s above-mentioned short assessment in half the neighborhood’s corner stores (n = 35), selected from a list of those with tobacco retail licenses. Focused on tobacco and healthy food, the youths’ findings were illustrated in a map with images of a full or half apple or, in the great majority of cases, a rotten apple core, signifying quality and availability of healthy food, tobacco advertising, and related factors (Figure 1). The “apple map” was presented to city agencies and others, who were alarmed by the findings. One of these organizations, the local Community Benefits District, then hosted a well-attended meeting that was the genesis of what would become the TLHCSC.
Collective Impact Model Applied to the Tenderloin Healthy Corner Store Coalition.

Source. Collective impact model adapted from Hanleybrown, Kania, and Kramer (2012).
Note. VYDC = Vietnamese Youth Development Center; TNDC = Tenderloin Neighborhood Development Corporation; CBPR = community-based participatory research; FJLs = Food Justice Leaders; CX3 = Community of Excellence in Nutrition, Physical Activity, and Obesity Prevention Project. Core tenets of collective impact model are in boldface and other important model features are in italics.
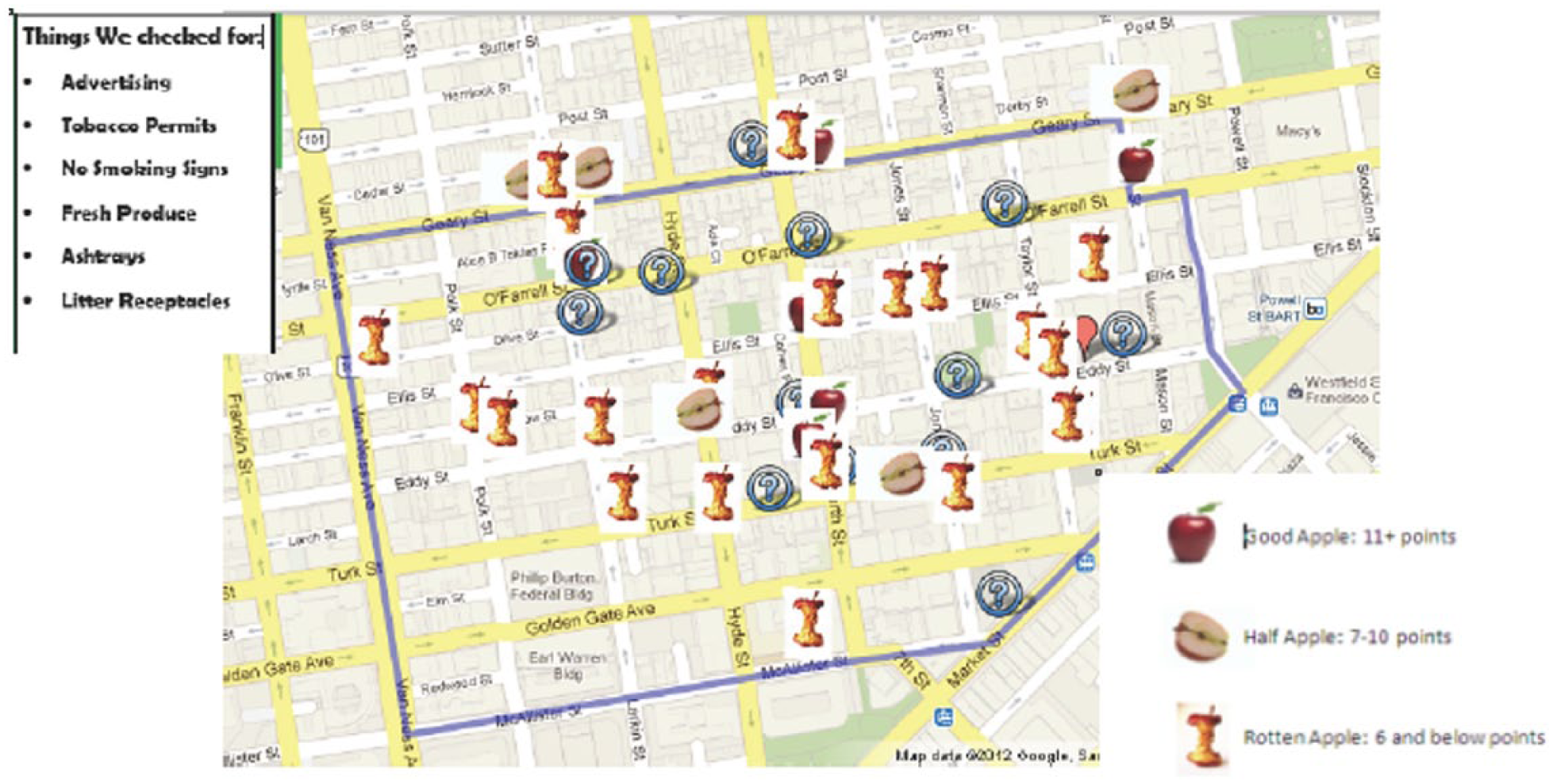
Tenderloin youth “apple map” of corner stores (n = 35).
Several interviewees remarked on the organic, grassroots nature of the initial gathering, which occurred without official recruitment. In one participant’s words, “People really want to own what’s going on in this neighborhood,” a fact that helped catalyze the initial meeting. The original group met several more times, with members taking turns hosting meetings, and then together hosting a community meeting attended by about 60 residents and agency representatives. As one Coalition member commented, “We had various topics for the community to give input on, but converting the corner stores from something negative into having a positive influence . . . had the greatest support.”
Phase 1: Initiating Action
Following the community event, informal meetings with rotating heads continued, and members, including committed residents, decided on a name—the TLHCSC—to give the group an identity and enable it to apply for grants. The VYDC and the Tenderloin Neighborhood Development Corporation (TNDC) served as coleads, and a diverse group of community-based organizations, government agencies, and local residents became members. This first phase of CI includes developing “an understanding of the landscape of other key players” (Hanleybrown et al., 2012). Key partners included the Tenderloin Community Benefit District, the National Council on Alcoholism–Bay Area, the Central City SRO (Single Room Occupancy) Collaborative, The Asian Pacific Islander Wellness Center, the Al-Sabeel Mosque, and a member whose “day job” involved promoting small businesses (see Figure 2). An additional critical partner was the AAIMS project (Alleviating Atypical Antipsychotic-Induced Metabolic Syndrome), a group that trains local residents in nutrition and how to prepare affordable dishes with limited cooking facilities.

Composition of the Tenderloin Healthy Corner Store Coalition.
Phase 2: Organizing for Impact
The second phase of CI involves a multifaceted process, well illustrated in the unfolding of the Coalition, in which membership and visibility increased substantially. The AAIMS project brought in more of its own members, who, in addition to their regular participation, prepared at each Coalition meeting healthy and affordable foods, reinforcing the importance of the Coalition’s work and providing refreshments, which can be an important incentive for coalition attendance (Butterfoss, 2013). Additional partners from UC San Francisco and UC Berkeley rounded out Coalition membership during this phase, and while not “regulars,” several members of the private sector, including corner store owners and the CEO of a store redesign firm, sometimes attended the monthly meetings. The latter member, who had provided some store redesign work in the BVHP, learned of the TLHCSC from a leader in the other neighborhood’s healthy store efforts and quickly became “a critical component of the [TLHCSC].”
When asked about the Coalition’s backbone organization, most participants noted that one member each from the VYDC and the TNDC provided the administrative, coordination, and management support for the Coalition. Both organizations were described as highly committed to bettering the Tenderloin and therefore willing to support staff members’ time to support the Coalition. Together, the coleads devoted 100 hours per month to the Coalition. Although SFDPH also was mentioned as critical to the Coalition’s functioning, it clearly was seen as being intentionally in the background. Both CI and CCAT emphasize the importance of a single backbone organization, with dedicated fiscal and other resources to enable staff to devote sufficient time to the work (Butterfoss & Kegler, 2009; Kania & Kramer, 2011). Although a subsequent (2014) large grant enabled 50% salary support for a project coordinator and other resources for a single backbone organization (TNDC), the former arrangement was described as working well during this earlier period.
The creation of a process for collaboration, emphasized in both CI and CCAT, was well demonstrated by the Coalition. The two backbone organizations arranged for meeting space for monthly and weekly Coalition and FJLs meetings, respectively. A nine-member Steering Committee was established, which met monthly to develop an agenda for the upcoming Coalition meeting that reflected new developments and ongoing concerns. The Coalition coleads were described as particularly effective cofacilitators of these meetings with “a very, very, very wide range of people,” maximizing community participation. Decision making concerning important issues was, from the outset, undertaken by the full Coalition through open discussion, followed by a majority vote.
Movement toward a shared goal occurred prior to formalizing the Coalition, born of the members’ unifying belief that “food is a health equity issue” (Gomez et al., 2013). An initial survey of 640 residents conducted in four languages by a number of its participating organizations, illustrated the process the Coalition’s use of mutually reinforcing activities. The survey had previously been developed and used by SEFA and adapted and used by a community-led partnership in Kansas City (Mabachi & Kimminau, 2012). To learn more about where residents shopped for various foods and their perceived needs, Coalition members used their own networks to survey their clients or fellow residents. The TNDC distributed the survey to its housing units, and the Central City SRO Collaborative trained its tenant leaders to conduct the survey during tenant meetings. The Coalition’s survey showed that most participants reported purchasing staples (fruit, vegetables, meats, dairy, and grains) outside the neighborhood, amounting to about half their grocery dollars. Staff at the TNDC estimated the loss of about $11 million annually from the local economy (Gomez et al., 2013).
These stark realities, and the fact that 80% of respondents reported that they would buy healthy food locally if available and affordable, and not in venues with a plethora of tobacco and alcohol products and advertising, were seen by the Coalition as underscoring the need for healthier, more comprehensive food options locally, which could restore lost revenue for the neighborhood. Building on these data, and lessons learned from the BVHP, the Coalition further honed in on improving food access and decreasing the emphasis on tobacco in a form that made sense within the community: Turning corner stores into community assets through conversion to healthy retail. The common agenda was to improve the quality of foods available in a way that put decision making in the residents’ hands and kept revenue in the community. Although members worked toward the goal in different ways, all got on board. As one Coalition leader remarked,
Everyone has other deliverables and things they have to do, but this does overlap with their work. It made sense for an alcohol prevention group to work on healthy retail . . . to be part of a greater movement . . . This [bigger cause] is something we all call our own . . . (Table 2)
Strategies for achieving a common agenda also were established: (1) training, educating, and helping empower Tenderloin resident leaders to advocate for community food justice; (2) collecting data on availability of fresh and healthy food in the neighborhood, evaluating specific ways to improve, and creating standards to measure food stores; and (3) improving the overall community by investing in and changing some of the Tenderloin’s least healthy elements—corner (mostly liquor and tobacco) stores—into vital community resources (Gomez et al., 2013). Critical to these strategies was the Coalition’s hiring and training of five residents as FJLs, ranging in age from their 20s to 60s. As in the BVHP, and supported by two small foundation grants, FJLs participated in a 6-week training on food systems, food access, nutrition, food labeling, and research. The FJLs then conducted much of the Coalition’s community-driven research, community education, and policy advocacy. As Butterfoss and Kegler (2012) note with respect to the corresponding second stage in CCAT, “the maintenance stage also includes implementation of multilevel strategies of sufficient duration and intensity to have an effect” (p. 320).
For the TLHCSC, this second phase also saw the use of CBPR in the development of a rigorous shared metrics and measurement approach. SFDPH introduced a 54-item “Corner Store Standards for Health and Sustainability Tool,” tailored by FJLs and Coalition leads to the Tenderloin. After pilot testing the tool outside the neighborhood, the FJLs used their networks and personal relationships with store owners to obtain permission to assess 56 of the neighborhood’s 70 corner stores. Shared measurement was made possible by SFDPH’s Feeling Good Project (San Francisco Nutrition Services, 2013), which collected rigorous community assessment data in four neighborhoods, including the Tenderloin, using the Community of Excellence in Nutrition, Physical Activity, and Obesity Prevention Project (CX3) measurement tool (Ghirardelli, Quinn, & Sugerman, 2011), which bore many similarities to the original store assessment tool used by FJLs. The Feeling Good staff cross-checked their findings against the FJL’s and found strong similarity between the assessments, adding credibility to the latter’s research, the findings of which were then translated into a “Shopping Guide” for local residents. The Guide included photos of each store, its one- to four-star rating, “healthy highlights” such as availability of whole grains, and acceptance of food stamp electronic benefits cards (www.healthyTL.org). As discussed later, FJLs conducted a repeat assessment in most of these stores (n = 50) in spring 2014, with the academic and SFDPH partners working with FJLs to craft additional items on tobacco and e-cigarette display and advertising. Regular check-ins with the backbone organization cochairs and other Coalition Steering Committee members offering input on preliminary findings and data analysis further contributed to measurement processes.
Although shared measurement of Coalition process has been largely limited to informal check-ins at monthly meetings and the participatory evaluation components of the analysis on which this article is based, more formal evaluative processes will begin in January 2015 and continue over the next 3 years (see Phase 3).
Building community will, which is critical to this second phase of CI, was enhanced by a process that also illustrates mutually reinforcing activities. The FJLs built good will of local merchants by returning to all stores assessed with individualized feedback packets, the Shopping Guide, and resources for improving healthy food sales and future guide ratings (Table 1). Both these processes were repeated 1 year later with similarly large-scale community and store involvement (see the Outcomes section) and more opportunities for interested stores to apply for help with store redesign.
In both 2013 and 2014, and following individual meetings with merchants, the Coalition held community-gatherings to release and distribute the annual Tenderloin Neighborhood Shopping Guides. These events engaged hundreds of residents and merchants with interactive activities, cooking demonstrations, speakers, and information about healthy food in the neighborhood. They were also highly collaborative, with Coalition members planning, tabling, translating, and volunteering. Finally, the annual community meetings helped build public will, with city supervisors invited to attend to talk about the proposed HRSF Ordinance on which they had worked closely with the Coalition. The city program would provide technical assistance with store redesigns and other benefits for selected stores that signed a memorandum of understanding to take steps (store redesign, shifting business plans) to meet the legislation’s definition of a healthy retailer. The definition included devoting ≥35% of selling space to healthy foods and ≤20% to alcohol and tobacco, while removing specified amounts of cigarette and alcohol advertising (www.healthyretailsf.org).
Phase 3: Sustaining Action and Impact
An important component of the refinement process in CI’s final stage involves conducting a more detailed assessment of the collaborative’s process and how it might be improved. Although Coalition forums and other events have been formally evaluated, and reflective discussions of process have sometimes taken place at Coalition and FJL meetings, the first annual Steering Committee retreat took place in December 2014. Its objectives were to celebrate past successes, identify what still needs to be done (e.g., identifying weaknesses and community members/residents to still engage), reflect on changes, and refocus on tasks in the coming year.
The participatory case study analysis on which this article was based has provided some process data, and the more rigorous and ongoing 3-year participatory and conventional evaluation process beginning January 2015 will help fill this void. To date, however, lack of time and staffing for more regular and detailed assessments of progress has been a weakness.
The Coalition appeared far more successful, in its strong accent on continuous communication, which is key to effectiveness in the Sustaining Action and Impact phase of the CI model and a core proposition of the CCAT as well. By Phase 3, 20 to 30 members typically attended monthly Coalition meetings, with 200 on the active listserv. Illustrating use of the listserv well beyond alerting members to meetings/events, a colead commented, “If someone needs a letter of support from member organizations, they will get at least 8 to 10 letters each time.” Members also call 40 to 50 Coalition members, including the local police captain, to be sure that they know about, and ideally can attend, upcoming meetings and events. The Coalition website (www.healthyTL.org), developed by a resident, also communicates to a wider audience while enabling members to stay current. Finally, community event planners intentionally loop back to the general community about key points in the process, to insure a constant feedback cycle and high-level community engagement. Such events and activities, moreover, aligned well with CCAT’s third stage (institutionalization) in which there is recognition that
sustainability does not depend on one strategy, policy, or approach, but instead requires developing community understanding and leadership to embed new solutions in institutions—literally institutionalizing policies and organizational practices within communities. (Butterfoss & Kegler, 2012, p. 324)
A clear and important difference between CI and CCAT and other frameworks for building and assessing collaboratives (Lasker et al., 2001; Wolff, 2010) is the CI model’s disinclination to look at changing governmental policy as a means of addressing social problems (Hanleybrown et al., 2012; Judith Bell, personal communication, November 3, 2014). In contrast, the CCAT includes, as part of a Coalition’s long-term sustainability, “having a long-term plan for assuring the viability of an organization or a community-led initiative that manages several policy, systems, and environmental change strategies” (Butterfoss & Kegler, 2012, p. 325). To achieve the TLHCSC’s ambitious healthy retail agenda, policy change was critical. Coalition members had already used their data and considerable knowledge of healthy retail to work with city supervisors and other partners in crafting the HRSF Ordinance. During this third phase of the CI process, they scaled up this work. In the words of a supervisor cosponsor of the measure,
The Coalition was extremely influential in drafting, refining, and then passing the healthy retailer ordinance last September [2013]. . . . They held meetings with the Land Use Committee and the full board. They brought members in to educate the legislators. They had very clear ideas in working with our staff to develop the HRSF Ordinance.
Concurrently with this work on the ordinance, an increased accent on public–private partnerships, including frequent communication with store owners, an architectural firm that does redesigns, and others in the private sector, proved critical. Through a small Dignity Health Foundation grant, a process was initiated to select the first Tenderloin store for a redesign, even before passage of the HRSF Ordinance. During this process, public–private partnerships were again illustrated, with a member of the local Arab American Grocers Association and the owner of an independent local store coming to the Coalition to make their case for selection. The CEO of the store redesign firm, which would lead the actual redesigns, attended Coalition and other relevant meetings and presented his feasibility analysis, which, together with residents’ safety concerns, data on merchants’ motivation, and other factors, led to the selection, in fall 2013, of one store—Radman’s Produce Market—for the first redesign.
The Coalition’s two backbone organizations were very active during this redesign, overseeing communication with the store’s owner, developing and solidifying the memorandum of understanding, managing the contractors, and planning a reopening event. Concurrent with the redesign process, Radman’s participated in OEWD’s façade improvement program, which enhanced the redesign and further linked the Coalition’s work to the new HRSF program. Similarly, as HRSF began its store selection process, the OEWD/SFDPH sponsored an initial outreach workshop for Tenderloin store owners for which a backbone organization (TNDC) helped engage local businesses. Nine of the 56 stores that had participated in the FJL’s store assessments and subsequent individualized feedback sessions attended this workshop and applied for the city’s new store redesign program.
The CI model’s emphasis on mutually reinforcing activities also was well illustrated during this third phase: For the grand opening of the first redesigned store, Coalition members decided with the store owner to have this launch coincide with the Tenderloin’s “Sunday Streets.” A daylong celebration in April 2014, this event showcased the neighborhood and its businesses and offered entertainment. The Coalition coleads also helped arrange congratulatory remarks by two district supervisors in front of Radman’s, to commend the store and introduce attendees to the work of the FJLs and the Coalition. The Supervisors also talked about both HRSF and a city Soda Tax initiative, which, if passed, would have provided a major new source of funding for the program.
Through such events and its day-to-day functioning, the Coalition was described as operating with transparency about its goals, the work done in and outside regular meetings, and funding sought. There were still “side-bar” conversations within the community that could leave out some Coalition members, for example, the SFDPH, but representatives of those groups accept this because, as one noted, “It is really up to the community to define and implement the solutions” that SFDPH and others can help support and guide.
Reflecting back on the Coalition’s process, one member remarked that there is “a real collaboration between agencies involved, key people, and community members.” Similarly, an FJL commented, “At the end of the day we’re all the same, at the beginning of the day too.”
Challenges and Obstacles Faced
Our analysis of the TLHCSC suggests that it was highly effective in achieving many of its goals and objectives, while also developing and maintaining its role as a strong and diverse collaboration. At the same time, many challenges and obstacles were described. A Steering Committee member emphasized the challenge posed by the immense diversity of the neighborhood, where seven major languages are spoken and parts of the community could not be engaged because of linguistic barriers. The striking diversity of Coalition members in income, education, race/ethnicity, age, and resident versus outsider status also sometimes led to tensions at meetings, based in part on power differentials. Although the cochairs and other members proved adept at ensuring broad and respectful participation, occasional outbursts occurred, sometimes necessitating mediation. Yet Coalition participants overwhelmingly stressed a feeling of community and safety in the group, including feeling that they could safely air disagreements yet be treated with respect. Furthermore, the commitment of the full team to equalizing participation (e.g., though votes of the full Coalition on every major decision) enhanced its democratic functioning. In the words of one member, the TLHCSC is “probably one of the healthiest coalitions I have ever been a part of. Nobody is stepping on anyone else’s toes. We all come at it from different angles but have the same goal.”
As with many coalitions, funding has proven a major obstacle and, until recently, was limited to partial support from the department of public health for a Coalition colead, small grants, paying part-time salaries of FJLs, and covering community events and assessment processes and with little left over for the Coalition’s day-to-day functioning. A new 3-year grant from the Tobacco-Related Disease Research Program, with most funds dedicated to the backbone organization and the Coalition, has substantially improved this picture. Similarly, while scale-up of the Coalition’s work though more store conversions was hurt by the city’s failure to pass a soda tax that would have greatly increased annual funding for this work, the OEWD’s continued commitment to store redesigns and an agreement by The California Endowment to help support one to two additional Tenderloin store conversions in the next 2 years have maintained momentum.
Yet, as a longtime leader in the healthy store movement notes,
The food environment is complex. The Tenderloin and neighborhoods like it . . . have suffered decades of disinvestment where unhealthy choices predominate. To stem that tide takes time . . . and it takes a comprehensive approach . . . to make the healthy choice the easy choice. (Hannah Burton Laurison, personal communication, November 10, 2013)
A related challenge has involved engaging some of the neighborhood’s retail stores and helping interested small store owners shift their business model from a dependence on tobacco, alcohol, and junk food to stocking fresh and healthy items. The participation of 56 of the 70 corner stores in the first assessments and follow-up feedback and education sessions with FJLs, with 9 of these stores then taking part in additional group information sessions on HRSF, was impressive and spoke again to the strong relationships built by the FJLs with these stores and to the latter’s own desire to improve their business models and sales. Yet, as a Coalition leader pointed out, “Many of the stores are small, independent, family-run establishments with little or no staffing,” such that participation in an effort like this does not seem feasible. Furthermore, “the introduction of fresh and healthy foods requires training and an ongoing commitment to the ‘daily touch’ needed for fresh produce”—a fact also seen by some store owners as making this change problematic. However, as another Coalition member noted, “More and more small stores are shifting their business model to include healthy and fresh foods [and] being able to show [non-participating stores] that they can be competitively profitable really helps.”
Outcomes
The TLHCSC is only in its third year, and while much of its focus has been on the “short-term sustainability” needed to keep strategies in place, (e.g., building leadership and a strong community base, and getting buy-in from key decision makers; CDC, 2011),—there is also evidence of contributions to longer term sustainability and community and policy change. As noted above, key among these were widely disseminating findings from the Coalition’s research and the use of this, along with effective media and policy advocacy, to help in the crafting, passage, and implementation of the city’s HRSF Ordinance. As a Steering Committee member remarked, “Every step of the way, the community has been directly involved in decision making . . . an empowering experience for the resident FJLs who are now advocates at City Hall and involved in City-wide policy development.”
Decision makers’ appreciation of the role of the Coalition in the passage, rollout, and early implementation of the HRSF legislation was also demonstrated in the selection of three Coalition members to serve on the HRSF Advisory Committee, which meets quarterly in City Hall. Finally, when momentum was needed for a statewide healthy stores effort and a proposed city soda tax, both city supervisors and other key stakeholders sought help from the Coalition, which increasingly was seen as a “player” in the move to change food, beverage, and tobacco environments in San Francisco. In the words of one supervisor,
I included [the Coalition] in other efforts like the ‘healthy stores, healthy communities’ initiative, which is now operating at the statewide level. This is an example of how they’ve helped with [regional and statewide] efforts. They also were very helpful on the soda tax on the November [2014] ballot. They’ve been instrumental in bringing their base out, in other communities and in linking junk food and junk drinks with alcohol and tobacco.
Another outcome of the Coalition’s work, and one easier to quantify, involved an increase in the number of corner stores improving their ratings on the FJLs’ annual store assessments, which translated into improved ratings in the Coalition’s “Shopping Guide” for residents. Between 2013 and 2014, the number of stores with just one star decreased from 12 to 3; the number with two stars declined from 31 to 24, while the number of three-star stores nearly doubled, from 12 to 23; and the number with all four stars increased from 1 to 2. Although higher ratings may have been somewhat inflated due to several new questions on tobacco and e-cigarettes on the second assessment instrument, the magnitude of the changes seen over a single year was substantial. An anticipated “ripple effect” was thus observed, as even many stores not participating in the healthy retail program made positive changes in their business practices to improve their scores, and hopefully their patronage, because of continued relationship building with and education by the FJLs and the larger Coalition.
Both the CI and the CCAT emphasize the critical importance of adequate resources to support a collaborative’s work (Butterfoss, 2013; Kania & Kramer, 2011). Although the TLHCSC was remarkably successful in operating “on a shoestring” for much of its history, it recently brought in a 3-year grant, previously described, with .50 FTE (full-time equivalent) for the project coordinator, rent, and other support for the now sole backbone organization (TNDC); a doubling of the number of FJLs; and greater staff and consultant resources for more rigorous data collection and analysis, as well as support for new store redesigns. With several Coalition members on the advisory board of HRSF, the city’s commitment to the Tenderloin as the primary neighborhood in which store redesigns will take place, and new fiscal support from The California Endowment, this new development also bodes well for the continued growth and sustainability of TLHCSC’s work. Finally, neighborhood and citywide coordination continues to be strengthened by these efforts as the citywide healthy retail program continues to evolve. HRSF (HealthyRetailSF.org) is now established firmly in city government and bundles a variety of city services to support stores in three areas: physical environment improvements, improvements in businesses’ operations, and community engagement and marketing. The Coalition coordinator now serves as the community engagement coordinator for the city program and is able to further link city services to the Tenderloin. For example, a food security program will now invest in HRSF and TLHCSC work by focusing its fresh produce voucher distribution in the Tenderloin. Residents can use these vouchers in local stores participating in HRSF, including the next three Tenderloin stores to be redesigned.
Discussion
In today’s challenging fiscal climate, cross-sector collaboration, including community members, organizations, government officials, and for-profit entities, is becoming increasingly common—and necessary—in health education and promotion. We endeavored to describe and critically assess an increasingly popular model for collaboration—CI—and to illustrate, through a case study, the utility and drawbacks of the model, as well as the added value when it is augmented by insights and strategies from CCAT. Although a single case study is highly limited in what it can demonstrate, we believe the phases and most key tenets of the CI model are reasonably well illustrated through the work and functioning of the TLHCSC, as are some of the model’s weaknesses. The few other applications of CI in health promotion to date (Burke et al., 2009; Economos et al., 2007; FSG, 2013; Ronshausen et al., 2014), as well as newer efforts as they unfold, should be carefully analyzed and a more rigorous assessment undertaken of the model’s applicability for health education and promotion (Flood, 2013).
In the meantime, several lessons learned about advantages and challenges of the CI model in the Tenderloin case study may be instructive. Key among these was the importance of creating a common agenda, where each partner examines the problem and identifies solutions through the same lens. Such a process will not be successful if done through coercive compromise (Butterfoss & Kegler, 2009; Israel et al., 2005; Mabachi & Kimminau, 2012). However, as PolicyLink President Judith Bell has suggested, for coalitions with a focus on advancing health and social equity, often through policy change,
the need for the backbone organization to have a point of view is one of the elements . . . CI has missed. The work must be [led] by an organization that has a broader mission, vision and values that reflect and embrace the CI effort. (Personal communication, November 3, 2014)
The TLHCSC appeared illustrative of a collaborative with a true common agenda, yet one whose backbone organization(s) also played a leadership role in stressing the broader vision within which this agenda was embedded. The CCAT was seen to provide valuable strategies for strengthening this collaborative’s backbone organization (e.g., by increasing fiscal and other resources to enable dedicated staffing by a single organization, which also provides credibility, a range of contacts, and technical assistance to the collaborative as a whole; Butterfoss & Kegler, 2012).
As Butterfoss (2013) notes, “Diverse representation and engagement [across sectors] will ensure that [coalition] strategies are carried out efficiently and effectively” (p. 35). However, power imbalances among a collaborative’s members and tensions between shared goals and the unique perspectives and knowledge that each partner brings, can be a challenge when following participatory principles and practices (Butterfoss, 2013; Cargo & Mercer, 2008; Chavez, Duran, Baker, Avila, & Wallerstein., 2008; Green, 2000; Israel et al., 2005; Rodgers et al., 2014), including tenets of CI. Although tensions sometimes emerged at Coalition meetings, the skills of the coleads in building group trust and addressing tensions when they arose, and the commitment of the full team to equalizing participation (e.g., through “one member, one vote”), greatly enhanced group dynamics and functioning and may hold relevance for other health promotion coalitions.
Having various means for continuous communication is essential to building trust among group members and moving forward (Austin, 2000). In this respect, too, the Coalition, with its open communication with merchants, government partners, and potential partners, demonstrated the high value placed on effective, multilayered communication. Additionally, Coalition members intentionally took steps to communicate with and provide feedback to the communities it represented. However, CI provided little detailed advice about how this is best accomplished, and other models, particularly the CCAT, offer more specific information on achieving this goal.
Additional information also would have been helpful on the explicit meaning and intended means of CI’s “shared measurement.” Although we identified one example of this—the FJL’s use of a detailed store assessment tool, which a SFDPH/Coalition member complemented through cross-checking with a similar tool—more typically, as in this participatory case study, multiple methods of inquiry are used. Furthermore, as Boumgarden and Branch (2013) suggest in a recent critique of CI from a business perspective, shared measurement may be “attractive for the accountability it creates” but may also “fail to test the right things” holding different entities accountable to “a common denominator of standards” (p. 2). This aspect of the model, too, needs careful testing and reconsideration in health promotion and education, ideally with the comparison of like projects using shared versus a diversity of measurement tools and metrics.
CI’s emphasis on funding and support enabling one entity to provide the administrative backbone for moving the group forward also has been widely stressed by other health education and health promotion models (e.g., Butterfoss, 2013; Butterfoss & Kegler, 2009; Wolff, 2010). Although the Coalition was, until recently, run by two coleads from separate organizations, their close collaboration and strong facilitation skills enabled them to “act as one” in providing support and managing an exceedingly diverse group, while building trust and transparency. However, the lack of a single lead organization fully supporting the effort was problematic from a fiscal perspective, as demonstrated by the TLHCSC’s need to seek multiple small grants to support its work. Receiving a large 3-year grant, funding a sole Coalition backbone organization, and supporting new research, advocacy, and evaluation will enhance sustainability and growth and make possible a more detailed assessment of the Coalition’s processes and outcomes, and of CI and other theoretical models for assessing the work.
As discussed earlier, a major limitation of the CI model for those in fields like health promotion involves its failure to address policy and advocacy as important elements and outcomes of the work (Minkler, Brechwich, Tajik, & Petersen, 2008; Wolff, 2010). Reflecting, in part, the business roots of the model, this omission is both understandable and problematic. Models such as the CCAT (Butterfoss & Kegler, 2009) and the Power of Collaborative Solutions (Wolff, 2010) may be a better overall fit for policy-focused coalitions while CI continues to evolve. A forthcoming issue of the Journal of Community Development, focused on applications of CI to that field and refinement of the original CI model undertaken by PolicyLink (J. Bell, personal communication, November 3, 2014) and others, should help improve the relevance of the model for new fields, including health promotion and health education.
In the meantime, and augmented by precepts and lessons from CCAT, we believe the CI has shown relevance for this case study of the TLHCSC and its work on both the community and policy levels to improve retail environments in low resource neighborhoods. We further believe that the strength of the Coalition and its contributions to community building were well demonstrated though this analysis. As a Coalition leader remarked, “While there have always been a number of CBOs [community-based organizations] and other organizations in the Tenderloin, the TLHCSC was able to bring them together in a way where they communicate and function very efficiently.” She added,
Resident involvement and empowerment are key. The FJLs learn valuable skills in advocacy, community organizing, nutrition and food systems. [They] build community connections not only with their neighbors, but with store owners and other resident leaders trying to improve their neighborhood.
Local policy makers have identified the Coalition as “powerful” in helping shape policy and as a group they will continue to work with in the future, while Coalition members also expressed their belief in the power of their organization. In one member’s words, “Putting aside our own agendas when we come to the table, to me that is Collective Impact.”
Footnotes
Acknowledgements
We gratefully acknowledge the Tobacco-Related Disease Research Program of the Office of the President, University of California, for its support of this research. The Dignity Health Foundation and the San Francisco Foundation also helped support the work of the Tenderloin Healthy Corner Store Coalition, as did the San Francisco Department of Public Health. We acknowledge our colleagues on the Coalition, and particularly colead Ryan Thayer and members of the Tenderloin Neighborhood Development Corporation and the Vietnamese Youth Development Center. Graduate students at UC San Francisco’s PRIME program and at UC Berkeley’s School of Public Health also made important contributions, and we are grateful for their generous assistance. Finally, thanks are due the Tenderloin residents, organization and agency representatives, city policy makers, and others who agreed to participate in this research. Your commitment to food justice, tobacco control, and health equity has been an inspiration.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Johnna Falbe was supported by the American Heart Association Postdoctoral Fellowship 14POST20140055.