
Abstract
Although some popular press and nonscholarly sources have claimed that weight is largely unchangeable, the relationship between this belief and objective measures of health remains unclear. We tested the hypothesis that people who believe weight is unchangeable will have poorer objective and subjective health, and fewer exercise behaviors and poorer eating habits, than people who believe weight is changeable. Participants were 4,166 men and 4,655 women enrolled in the National Health and Nutrition Examination Survey in the 2007 to 2010 iterations. Believing that weight was uncontrollable was negatively related to exercise and healthful dietary practices and positively related to unhealthful eating. Lack of exercise and unhealthful eating were, in turn, associated with poor physical health. Age, but not gender, moderated the relationships between belief in weight changeability and exercise behaviors, healthful eating, and unhealthful eating. This study suggests that believing weight is unchangeable is associated with poor health behaviors and poorer physical health.
Rising rates of obesity are one of the most important public health concerns in the United States (Flegal, Carroll, Kit, & Ogden, 2012; Panzer, 2006; Throp, Owen, Neuhaus, & Dunstan, 2011; Y. C. Wang, McPherson, Marsh, Gortmaker, & Brown, 2011; White House Task Force on Childhood Obesity Report to the President, 2010) and abroad (Karnik & Kanekar, 2012; Y. C. Wang et al., 2011; Withrow & Alter, 2011). Obesity and obesity-predictive behaviors, such as sedentary lifestyles and poor dietary decisions, are associated with health conditions including type 2 diabetes, cardiovascular disease, some types of cancer, back pain, depression, body image disturbance, and sleep disorders (Akinnusi, Saliba, Porhomayon, & El-Solh, 2012; Boutelle, Hannan, Fulkerson, Crow, & Stice, 2010; Coates, Slattery, Potter, Quesenberry, & Edwards, 1998; Schwartz & Brownell, 2004; Shiri, Karppinen, Leino-Arjas, Solovieva, & Viikari-Juntura, 2010; Y. C. Wang et al., 2011). Whether a person engages in health-promoting behaviors and maintains physical health can be affected by a variety of factors, including their beliefs about weight (Burnette, 2010; Clark, Abrams, Niaura, Eaton, & Rossi, 1991; Kitsantas, 2000; Linde, Rothman, Baldwin, & Jeffry, 2006; Saltzer, 1982). Some writers in the field of obesity and health work have advocated that body weight is overwhelmingly determined by genetic influence and that individuals have little to no control over their weight; this position is especially prominent within the “Healthy at Every Size” movement (Bacon, 2008; Bacon & Aphamor, 2011; O’Hara & Gregg, 2010; Rothblum, 2014). However, belief that weight is not controllable may be associated with decreases in healthful behaviors and increases in unhealthful behaviors. The present study tested the hypothesis that believing that weight is changeable will be associated with better physical health and that this relationship will be mediated by more healthful dietary practices, fewer unhealthful dietary practices, and more exercise behaviors.
Because of the rise in popular books and online forums (Dean, 2013) claiming that weight is primarily genetic, that individuals can do little to influence weight, and that dieting and exercise are ineffective for controlling weight, some individuals may be skeptical about recommendations to engage in behaviors that would facilitate weight loss. It is possible that such beliefs may be negatively related to health behaviors (such as healthful dietary practices and exercise behaviors); if an individual believes weight to be outside of the influence of diet and exercise, she or he may engage in more behaviors that are rewarding in the short term (e.g., eating unhealthful foods, avoiding exercise) rather than healthful behaviors with more long-term benefits for weight management. Although health care providers’ advice to lose weight positively influences patient health behaviors and facilitate weight loss (Rose, Poynter, Anderson, Noar, & Conigliaro, 2013), patients’ beliefs in the unchangability of weight may act to decrease the influence of expert advice or evidence contrary to their beliefs (Davies, 1997), akin to self-efficacy beliefs within the health belief model (Rosenstock, Strecher, & Becker, 1988; Strecher, DeVellis, Becker, & Rosenstock, 1986).
Implicit Theories
Previous research has shown that whether people believe a particular attribute is changeable has extensive implications for goal pursuit in that domain. Belief in the changeability of a particular attribute is referred to as an implicit theory that is either incremental (the attribute is changeable) or entity (the attribute is unchangeable; for a review, see Dweck, Chiu, & Hong, 1995). People who believe they can increase their intelligence (incremental theorists) are more likely to attribute failure to lack of effort, are more likely to continue to try to improve after failure, and ultimately improve more over time compared with people who believe intelligence is fixed (entity theorists; Blackwell, Trzesniewski, & Dweck, 2007; Hong, Chiu, Dweck, Lin, & Wan, 1999).
Research on implicit theories of physical ability has shown that people who believe physical ability is malleable have lower anxiety, have higher self-efficacy, and engage in less self-handicapping when completing physical activities than people who believe physical ability is fixed (Ommundsen, 2001a, 2001b; C. K. J. Wang, Chatzisarantis, Spray, & Biddle, 2002). This provides evidence that incremental theories can have positive effects for physical abilities.
Although having an incremental theory (whether measured or manipulated) is often related to high self-efficacy (Komarraju & Nadler, 2013; Martocchio, 1994; Taberno & Wood, 1999), implicit theories are distinct from self-efficacy and behavioral control. Implicit theories reflect participants’ beliefs about the malleability of a particular outcome (intelligence, weight), whereas self-efficacy and behavioral control reflect participants’ beliefs about their ability to enact particular behaviors (Ajzen & Madden, 1986; Bandura, 1977). Individuals could believe that they could change their eating habits if they wanted, but believe that weight is unchangeable.
Implicit Theories of Weight and Health Behaviors
Because implicit theories affect goal-directed behavior, beliefs about the changeability of weight likely play a role in whether people engage in healthful behaviors. Controlling weight is one reason that people engage in physical activity and avoid unhealthful foods (Fotopoulos, Krystallis, Vassallo, & Pagiaslis, 2009; Glanz, Basil, Maibach, Goldberg, & Snyder, 1998; Pollard, Steptoe, & Wardle, 1998). Most relevant to the present study, a recent article identified implicit theories of weight as a significant predictor of weight loss intentions and behavior (Burnette, 2010). Participants who were randomly assigned to read an article claiming that weight was unchangeable reported less intention to exercise than participants who read an article claiming that weight was changeable. Furthermore, in a study of participants who expressed interest in losing weight, having an entity theory of body weight (as measured by items such as “You have a certain body weight, and you can’t really do much to change it”) was associated with lower expectations of weight loss success, more avoidant coping when faced with setbacks in their weight loss, and, ultimately, less weight loss, even when controlling for nutrition self-efficacy and exercise self-efficacy. This study provided evidence that believing weight is unchangeable was associated with decreased intentions to engage in healthy behaviors, lower beliefs in one’s ability to maintain diet and exercise routines, and ultimately decreased success in weight loss plans. This research laid important groundwork on implicit theories of weight and health behaviors.
The Present Study
The present study was designed to build on previous research on implicit theories of weight by using objectively measured weight, measuring additional health variables, and testing for moderation by age and gender. Because previous research on implicit theories of weight relied entirely on self-reported weight, it remains possible that participants who believed weight was changeable felt greater pressure to report weight loss (regardless of actual weight loss) than participants who believed weight was out of their control. Because self-reported weight is sometimes inaccurate (Gorber, Tremblay, Moher, & Gorber, 2007) and participants may be motivated to provide information that confirms their beliefs, we sought to test the relationship between beliefs about weight changeability and investigator-measured body mass index (BMI). We further extended previous research by including other health measures in addition to BMI (fasting blood glucose and subjective ratings of health). In addition, we sought to extend previous findings on the relationship between weight changeability beliefs and health by testing gender and age as moderators in a large, nationally representative sample. Some research has suggested that these two factors may affect weight-related behaviors; for example, women are more likely than men to report weight control as a motivation for exercise (Furnham, Badmin, & Sneade, 2002; Kilpatrick, Hebert, & Bartholomew, 2005; K. McDonald & Thompson, 1992), and weight as a motivation for exercise has been found to decrease with age (Davis, Fox, Brewer, & Ratusny, 1995; Tiggemann, 2004). The present research sought to test whether gender and age moderate the relationship between weight implicit theories and health or if the relationships between weight implicit theories and health are consistent across various genders and ages.
This study was designed to test the hypothesis that believing weight is changeable will be related to better health (as indicated by BMI, fasting glucose levels, and subjective ratings of health) in a large nationally representative sample. Furthermore, we predicted that the relationship between fixed weight beliefs and physical health would be mediated by healthful dietary practices, unhealthful dietary practices, and exercise behaviors. We also assessed for moderation of this relationship by gender and age.
Method
Participants
Participants were 4,166 men and 4,655 women enrolled in the National Health and Nutrition Examination Survey (NHANES) in the 2007-2008 and 2009-2010 iterations (different participants were enrolled in the separate iterations and thus the data are cross-sectional and not longitudinal). NHANES is an annual national study of health in the United States, and the data are publically available for researchers (Centers for Disease Control, 2007, 2009). For each location sampled, local government members were notified about the upcoming data collections and residents of the area were sent letters notifying them about the study. Potential participants were then interviewed briefly at their homes to determine eligibility. Participation was facilitated by transportation assistance to the testing center, financial compensation, and a personalized report of medical findings from individual tests. The unweighted response rates were 78.4% (interview) and 75.4% (examination) for 2007-2008 and 79.4% (interview) and 77.3% (examination) for 2009-2010. The current analyses were conducted using participants aged 18 to 79 years. Pregnant participants were excluded from the analysis. Demographic data for the sample are presented in Table 1.
Demographic Data (N = 8,821).

Note. DG veg = dark green vegetables; R2E meals = ready-to-eat meals; BMI = body mass index.
Data for continuous variables are presented as mean (standard deviation).
Procedures
Participants completed informed consent procedures administered by the NHANES research team. Computer-assisted interviews were conducted in participant homes. Participants were asked each question by an interviewer, and their responses were immediately logged on a computer. After the interview was complete, participants were asked to schedule an appointment to visit the mobile testing center where health measurements (e.g., height and weight measurement, blood draws) were completed.
Instruments
Demographic Moderators
Gender was assessed via a single, forced choice item between “male” and “female.” Age was assessed with a forced response for age, though individuals 80 years and older were coded as 80 in the NHANES data set. Because participants coded as 80 for age may be significantly older than 80, only data from participants up to age 79 were used in the present study.
Beliefs About Weight
Participants were asked to indicate their agreement with the statement, “Some people are born to be fat and some thin; there is not much you can do to change this” on a scale of 1 (strongly agree) to 5 (strongly disagree). In the present study, the coding of this item was reversed such that higher scores indicated greater agreement with the item (i.e., higher scores indicated greater entity beliefs).
Physical Activity
Participants were asked to indicate (with a “yes” or “no”) whether they (1) engage in vigorous intensity recreational activities (defined in the survey as “any vigorous-intensity sports, fitness, or recreational activities that cause large increases in breathing or heart rate like running or basketball for at least 10 minutes continuously”); (2) engage in moderate-intensity recreational activities (defined in the survey as “any moderate-intensity sports, fitness, or recreational activities that cause a small increase in breathing or heart rate such as brisk walking, bicycling, swimming, or golf for at least 10 minutes continuously”); and (2) walk or bicycle for at least 10 minutes each day. Higher values indicate greater physical activity.
Healthful Eating
Participants were asked to indicate, on a scale of 1 (always) to 5 (never), how often they (1) use the nutrition facts panel on food, (2) have fruits available at home, and (3) have dark green vegetables available at home. For the present study, values were recoded so that higher values indicated greater healthful eating.
Unhealthful Eating
Participants were asked to indicate how many “ready to eat foods” (e.g., deli foods) they ate in the past 30 days, how often they ate frozen meals or frozen pizzas in the past 30 days (ready-to-eat and frozen food consumption were banded into units of 10s to improve normality of the variables), and how many meals they ate away from home (e.g., at restaurants, fast food places, or food stands) in the past 7 days. Higher scores indicate greater unhealthful eating.
Poor Health
BMI was calculated based on height and weight as measured by a health technician. Height was measured with a digital stadiometer; participants were asked to remove their shoes. In the event that they refused to remove their shoes a correction was applied after measuring the height of the shoe heel. Weight was measured by a health technician in pounds using a digital scale; participants in the mobile examination center wore a disposable shirt, pants, and slippers; participants who refused to remove their shoes were coded as missing; participants with limb amputations were coded as missing. To measure fasting blood glucose (grouped into ≤69 mg/dL, 70-99 mg/dL, 100-126 mg/dL, and 126 mg/dL and over; corresponding to recommendations for low, normal, prediabetes, and diabetes-indicating levels; American Diabetes Association, 2011), a health technician collected blood from participants after a 9-hour fast. Subjective health was measured using two questions: the number of days their health was not good with regard to physical illness or injuries in the past 30 days (banded into units of 5 days to improve normality of the variable) and their general health on a scale of 1 (excellent) to 5 (poor). Higher scores on this variable indicate poorer health.
Analysis
Analyses were conducted in Mplus, Version 6 (Muthén & Muthén, 2010) using full information maximum likelihood estimation to account for missing data under normal methodology for using NHANES data (Centers for Disease Control, 2013). The model was run using COMPLEX model type, required for large survey data with weights, strata, and clusters. Sampling weights, strata, and clusters from the NHANES data set were included in analyses as per requirements of using large national data sets in general, and NHANES data in particular. Sample sizes required for structural equation modeling are generally accepted to be at least 200 participants (Tabachnick & Fidell, 2007) and thus the present sample exceeded minimum sample size requirements.
Results
Consistent with recommendations for conducting structural equation modeling (R. P. McDonald & Ho, 2002; Weston & Gore, 2006), we first tested a measurement model by constraining indicators to load onto intended latent variables, and freeing all covariances among latent variables and the born fat/thin item. This model was an acceptable fit to the data, χ2(68) = 411.07, p < .001, comparative fit index [CFI] = .95, root mean square error of approximation [RMSEA] = .02. Indicators loaded into their intended latent constructs at p < .01, and covariances among latent constructs and the born fat/thin item were significant at p < .05.
Because the measurement model was an acceptable fit to the data, we tested the structural model (see Figure 1). This model was a good fit to the data, χ2(69) = 441.23, p < .001, CFI = .98, RMSEA = .03. Standardized path coefficients are presented in Figure 1, and unstandardized path coefficients, standard errors, and standardized path coefficients are presented in Table 2. The model R2 for the latent health variable was 0.85.
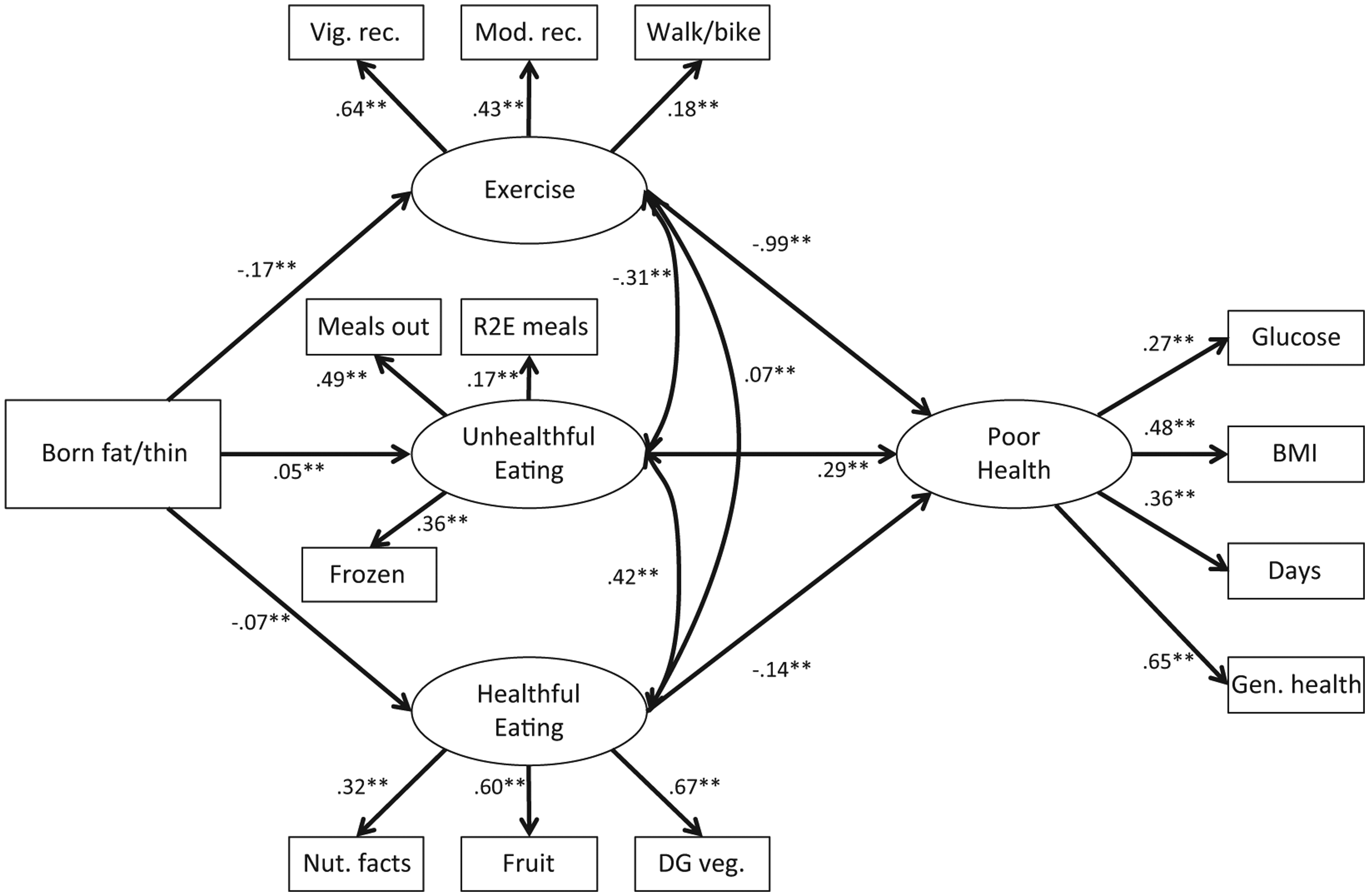
Structural equation model.
Unstandardized, Standardized, and Significance Levels for Models.

We investigated the hypothesized moderators of the relationship between the born fat/thin variable and the mediators. First, we assessed for a moderating influence of gender (Figure 2). An unconstrained model with gender as the grouping variable indicated acceptable fit to the data, χ2(153) = 1016.42, p < .001, CFI = .96, RMSEA = .04. The constrained model (with the three paths from the born fat/thin variable to the three mediators constrained to equality between groups) was also a good fit to the data, χ2(156) = 1015.21, p < .001, CFI = .96, RMSEA = .04; the models did not differ, χ2(3) = 1.21, ns, indicating that there were no gender differences among those three paths. Unstandardized path coefficients, standard errors, and standardized path coefficients for the two groups are presented in Table 2.
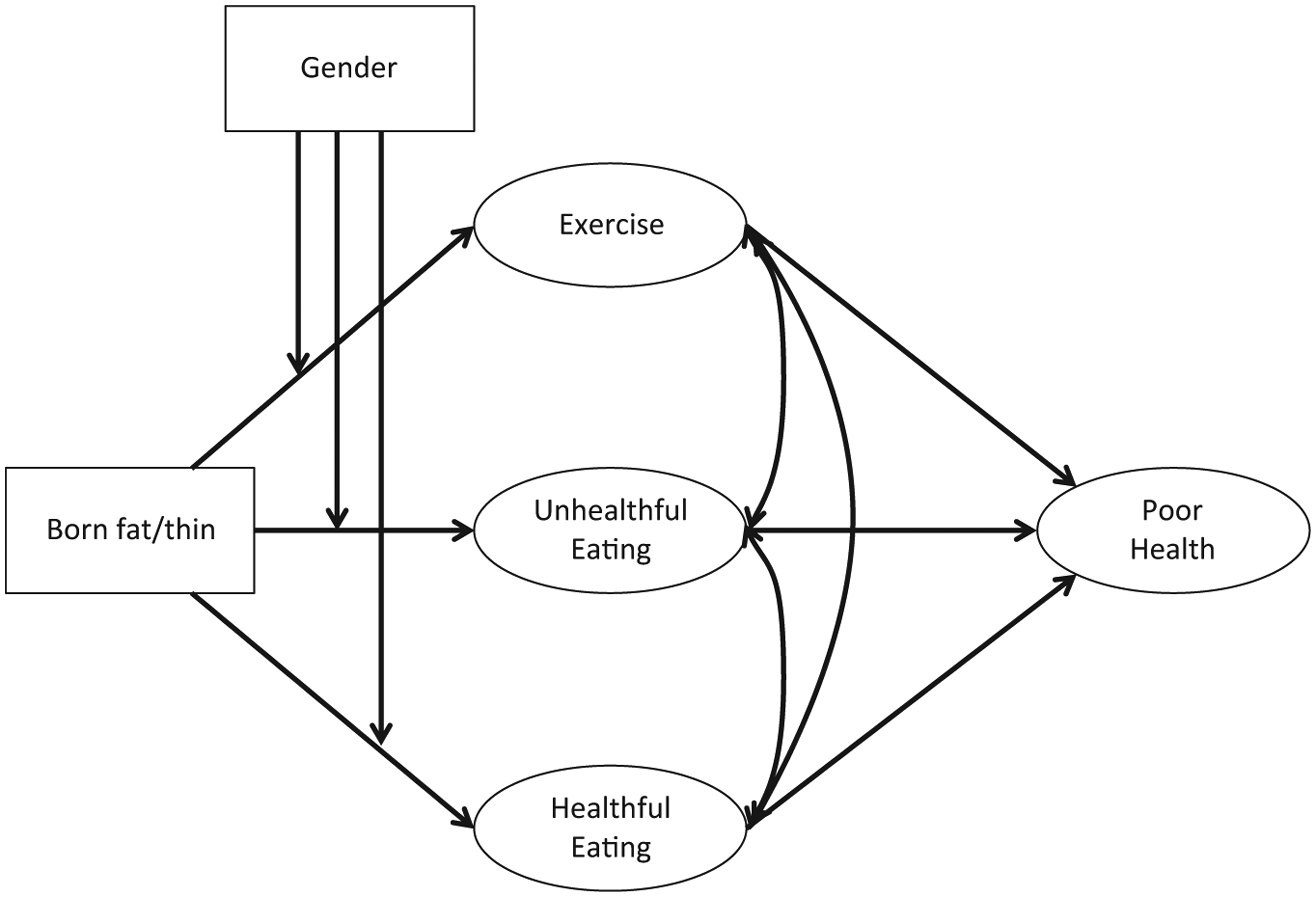
Moderation by gender.
Next, we tested for a moderating influence of age (Figure 3). Because age was a continuous variable, an interaction term approach was used. This model was an acceptable fit to the data, χ2(89) = 672.31, p < .001, CFI = .93, RMSEA = .03. Age significantly predicted exercise (B = −0.03, SE = 0.00, β = −0.61, p < .001), healthful eating (B = 0.00, SE = 0.00, β = −0.17, p < .001), and unhealthful eating (B = −0.04, SE = 0.00, β = −0.39, p < .001). Age was associated negatively with exercise behaviors, unhealthful eating, and healthful eating. There was also a significant interaction between belief and age on exercise (B = 0.00, SE = 0.00, β = 0.14, p < .01), between belief and age on healthful eating (B = 0.00, SE = 0.00, β = −0.08 p < .001), and between belief and age on unhealthful eating (B = 0.00, SE = 0.00, β = −0.06, p < .05). Among younger participants, exercise behaviors remained stable (and high) across implicit theories; among older participants, exercise behaviors declined among those who had entity, rather than incremental, implicit theories of weight. Among both younger and older participants, unhealthful eating increased slightly with entity beliefs though this association was weaker for older adults. Among younger participants, healthful eating was not associated with incremental beliefs while among older participants, healthful eating was negatively associated with entity beliefs. Simple slopes of these relationships are presented in Figure 4 (simple slopes were defined using the standard procedure of assessing values at one standard deviation about the means). Unstandardized path coefficients, standard errors, and standardized path coefficients are presented in Table 2.
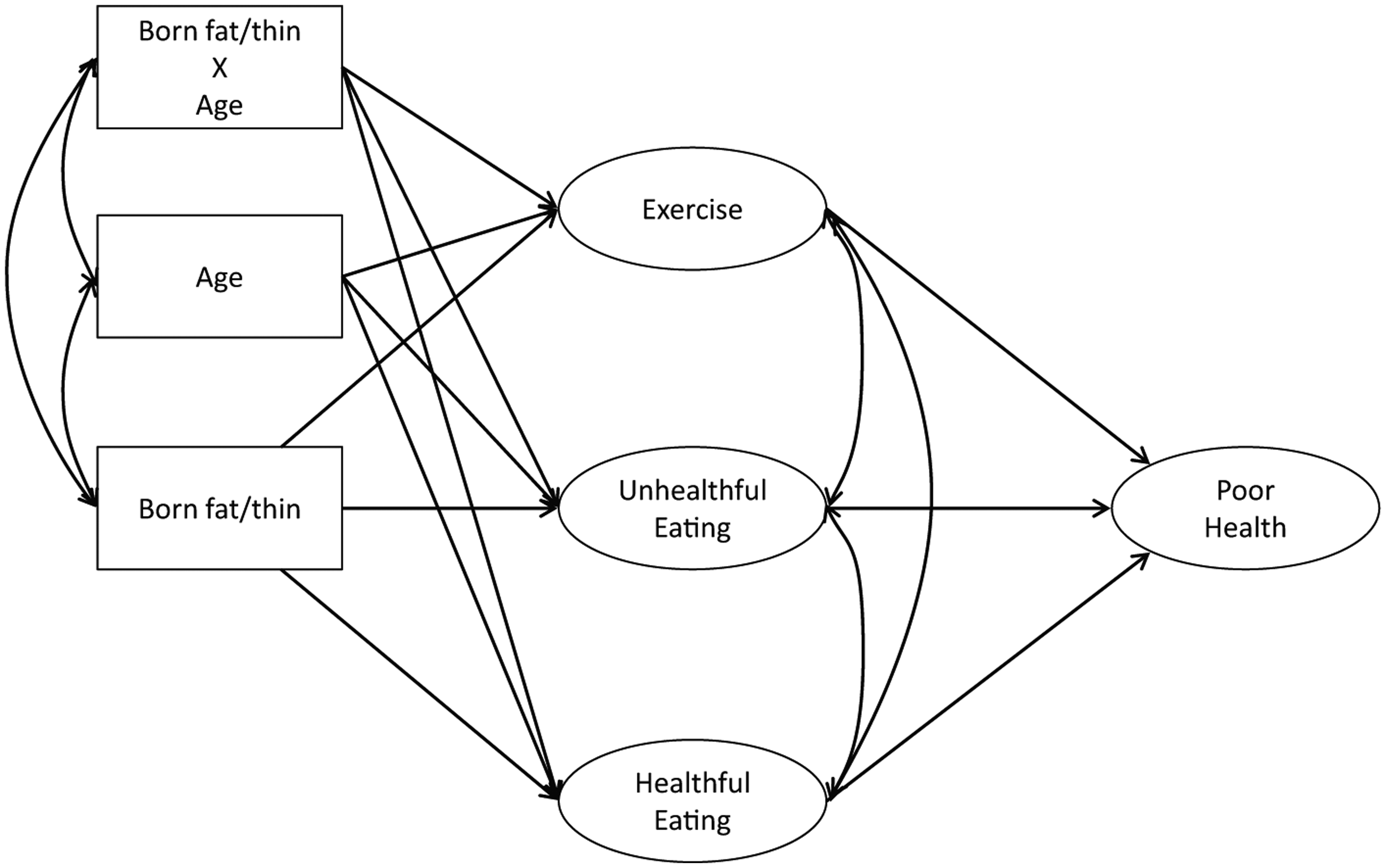
Moderation by age.
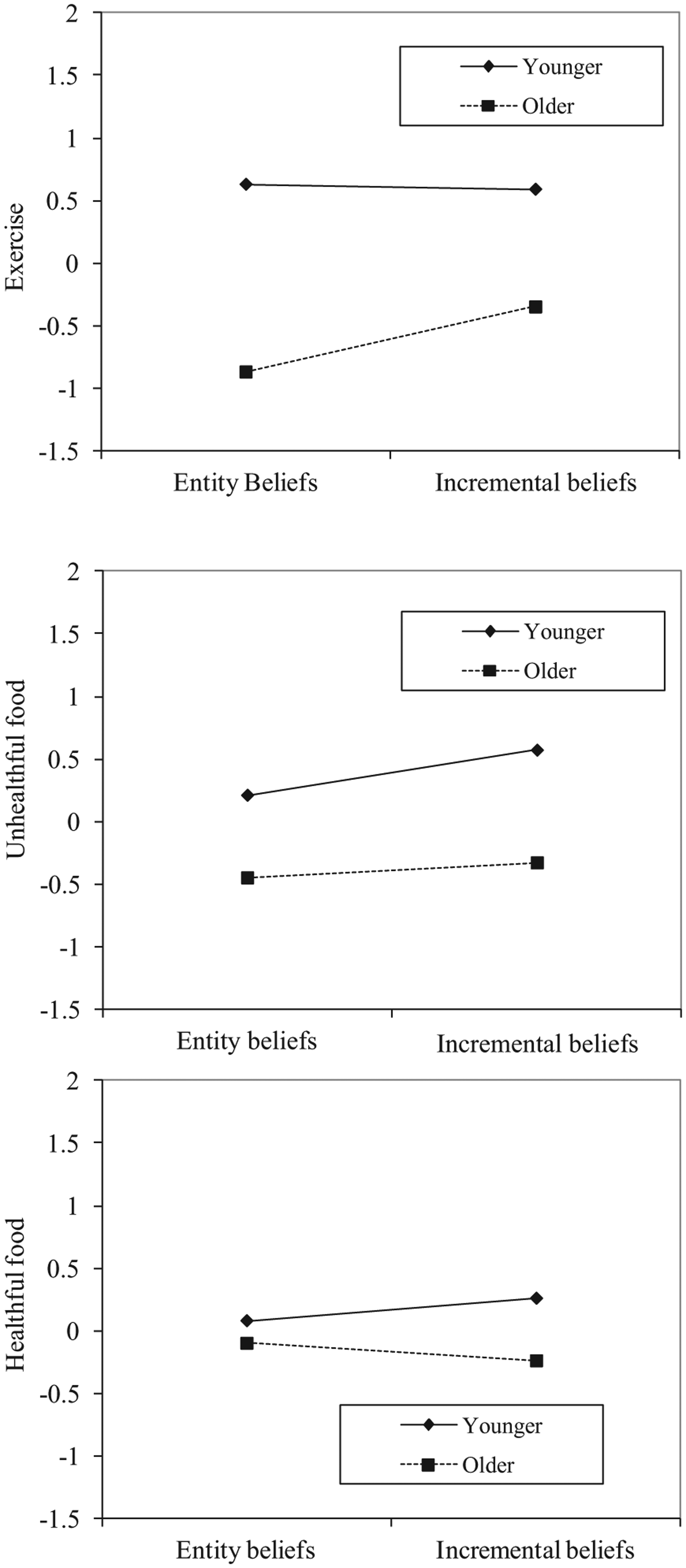
Interactions.
Discussion
The present study provided evidence that believing weight was unchangeable was negatively related to exercise and healthful dietary practices, and positively related to unhealthful eating. Exercise, unhealthful eating, and healthful eating were, in turn, associated with physical health. Furthermore, we found evidence that the relationship between changeability beliefs about weight and exercise, healthful eating, and unhealthful eating differs by age.
Although previous research has found gender differences in weight as a motivation for exercise and healthful eating, we did not find evidence that gender moderated the relationship between health beliefs and activity or healthful eating. Previous research has shown that gender differences in exercise and weight control motivation for exercise decrease with age (Brunet & Sabiston, 2011; Davis et al., 1995). The discrepancy between past results and our findings could be due, in part, to the fact that our sample is somewhat older (M = 46.78; SD = 17.05) than studies that have found gender differences in weight control as a motivation for healthful behaviors, many of which focus on adolescents or young adults (Furnham et al., 2002; Kilpatrick et al., 2005; K. McDonald & Thompson, 1992). We did find evidence of moderation of relationships by age, such that holding entity theories (i.e., believing that weight is not changeable) was associated with less exercise among older participants and less healthful eating among younger participants, though incremental beliefs were associated with greater unhealthful eating among younger and older participants, and less healthful eating among older participants. Believing weight was unchangeable was generally associated with less healthy behaviors than believing weight was changeable, though some moderation was observed with age.
Our research builds on previous work on the relationship between changeability beliefs about weight and weight loss in a number of ways. First, previous work on the relationship between weight changeability beliefs and diet and exercise has used self-report measures of weight (e.g., Burnette, 2010). Because people are often inaccurate when self-reporting their weight and height (Gorber et al., 2007), the present study used height and weight as measured by the NHANES study personnel rather than self-reported weight. Our study also measured health by assessing factors other than weight: fasting glucose and subjective health. By using the NHANES data set, we were able to test the relationship between changeability beliefs and health using a large, nationally representative sample. This research also builds on previous research by showing that the effects of beliefs about weight may differ with age.
The results of the present study must be interpreted in light of its limitations. First, the present study is cross-sectional, and longitudinal research on the relationship between implicit theories of weight, health behaviors, and physical health is needed. Second, although the present study used some objective measures of health (investigator-measured BMI and blood glucose levels), exercise, healthful eating, and unhealthful eating were assessed with self-report and thus may be open to incorrect responding, or inaccurate perception, by participants. Finally, the present study assessed implicit theories of weight with only a single item. In future research, researchers may want to combine current scales designed to measure implicit theories of weight (Burnette, 2010) with objective measures of health.
Despite the limitations of this study, it does have implications for research and clinical work. Although the present research does not determine causal direction between health beliefs and behaviors, it builds on previous experimental research showing participants who are given information supporting an entity theory of weight report being more likely to quit dieting after a setback than participants who are given information supporting an incremental theory (Burnette, 2010). Experimental studies might build on this work by giving participants materials supporting either incremental or entity implicit theories, and assess the impact of such manipulations on health behaviors such as exercise persistence or food choice. Another way to improve health may be to focus on whether people with motivations other than weight management to exercise and eat healthfully are protected against the effects of weight beliefs on behavior. Such work might occur in conjunction with studies on attrition in dieting and exercise studies or effectiveness of diet and exercise programs. Encouraging the belief that weight is changeable and encouraging nonweight motivations for healthy behaviors may both be effective strategies for improving health behaviors. Finally, the etiology of entity theories about weight may be further explored to assess whether and how those beliefs develop and can be changed.
With regard to clinical applications, the present results found that the popular belief that weight is almost entirely genetic and uncontrollable is associated with poor health. Psychologists, physicians, dietitians, and other health care providers might have the opportunity to discourage the belief that weight is uncontrollable or emphasize the importance of other motivations for healthful eating and exercise (Panzer, 2006). By fighting the perception that weight is unchangeable, health care providers may be able to increase healthful behaviors among their patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.