
Abstract
Challenges posed by infectious disease outbreaks have led to a range of participatory mobile phone–based innovations that use the power of crowdsourcing for disease surveillance. However, the dynamics of participatory behavior by crowds in such interventions have yet to be examined. This article reports results from a baseline evaluation of one such intervention called Mo-Buzz, a mobile-based crowdsource-driven socially mediated system developed to address gaps in dengue surveillance and education in Colombo, Sri Lanka. We conducted a 30-minute cross-sectional field survey (N = 404) among potential users of Mo-Buzz in Colombo. We examined individual, institutional, and cultural factors that influence their potential intention-to-use Mo-Buzz and assessed if these factors varied by demographic factors. Descriptive analysis revealed high perceived ease-of-use (PEOU; M = 3.81, SD = 0.44), perceived usefulness (PU; M = 4.01, SD = 0.48), and intention-to-use (PI; M = 3.91, SD = 0.46) among participants. Analysis of variance suggested participants in the 31 to 40 years age group reported highest PEOU, whereas the oldest group reported high perceived institutional efficacy (M = 3.59, SD = 0.64) and collectivistic tendencies. Significant differences (at the p < .05 level) were also found by education and income. Regression analysis demonstrated that PU, behavioral control, institutional efficacy, and collectivism were significant predictors of PI. We concluded that despite high overall PI, future adoption and use of Mo-Buzz will be shaped by a complex mix of factors at different levels of the public health ecology. Implications of study findings from theoretical and practical perspectives related to the future adoption of mobile-based participatory systems in public health are discussed and ideas for a future research agenda presented.
Keywords
Over the past decade, challenges posed by infectious diseases have spawned various innovative interventions utilizing the ubiquitous, cost-effective, and personable attributes of mobile phones (Lester et al., 2011). From an epidemiological standpoint, many of these interventions utilize “crowdsourcing,” allowing users to participate in the surveillance process by reporting disease-related incidents in real-time using mobile phones (Chunara et al., 2012; Freifeld et al., 2010). Our study seeks to understand the fundamental psychosocial mechanisms that underlie such participative behavior among smartphone users for dengue prevention in Sri Lanka. The article commences with a review of crowdsource-based surveillance interventions for infectious diseases, whereupon we describe our intervention, Mo-Buzz, designed to strengthen dengue prevention practices in Colombo, Sri Lanka. Our conceptual framework, drawing on behavioral theories from technology adoption studies and sociology, leads to a baseline evaluation of our intervention using a field survey approach. The article concludes by discussing the implications of our findings for the future of participatory mobile health (or mHealth) interventions from theoretical and applied perspectives.
Mobile Health Interventions for Infectious Disease Prevention
As witnessed in the context of HIV/AIDS, mHealth interventions serve several functions like facilitating access to treatment, disseminating health education, and ensuring adherence to clinical appointments and treatment regimens (Catalani, Philbrick, Fraser, Mechael, & Israelski, 2013). Air-borne and vector-borne infectious diseases like influenza, malaria, and dengue have invoked the development of crowdsource-based surveillance strategies where volunteers can now report disease-related incidents, events, or symptoms through mobile phones, a phenomenon also referred to as “participatory epidemiology.” The earliest examples of such interventions can be traced to Frontline SMS and Ushahidi (Freifeld et al., 2010), which enabled pandemic influenza surveillance through a simple short messaging service (SMS application) for health care professionals to update health departments in developing countries (Li, Moore, Akter, Bleisten, & Ray, 2010). Other examples of participatory systems include Flu Near You (2015) and Influenzanet (2015) that together reportedly boast nearly 100,000 volunteers (Hay, George, Moyes, & Brownstein, 2013). Both interventions provide a mobile application and/or website that allows volunteers to report influenza-like illnesses and symptoms. The gathered data are processed using algorithms that populate flu maps and dynamic infographics, critical information that health authorities can use to strategize actions and the public can use for self-protection. Outbreaks Near Me (HealthMap, 2015) is another intervention that invites the general public to report knowledge and experiences related to a range of infectious diseases through an iPhone and Android application (see Table 1 for a summary of these initiatives).
Existing mHealth Interventions for Infectious Diseases.
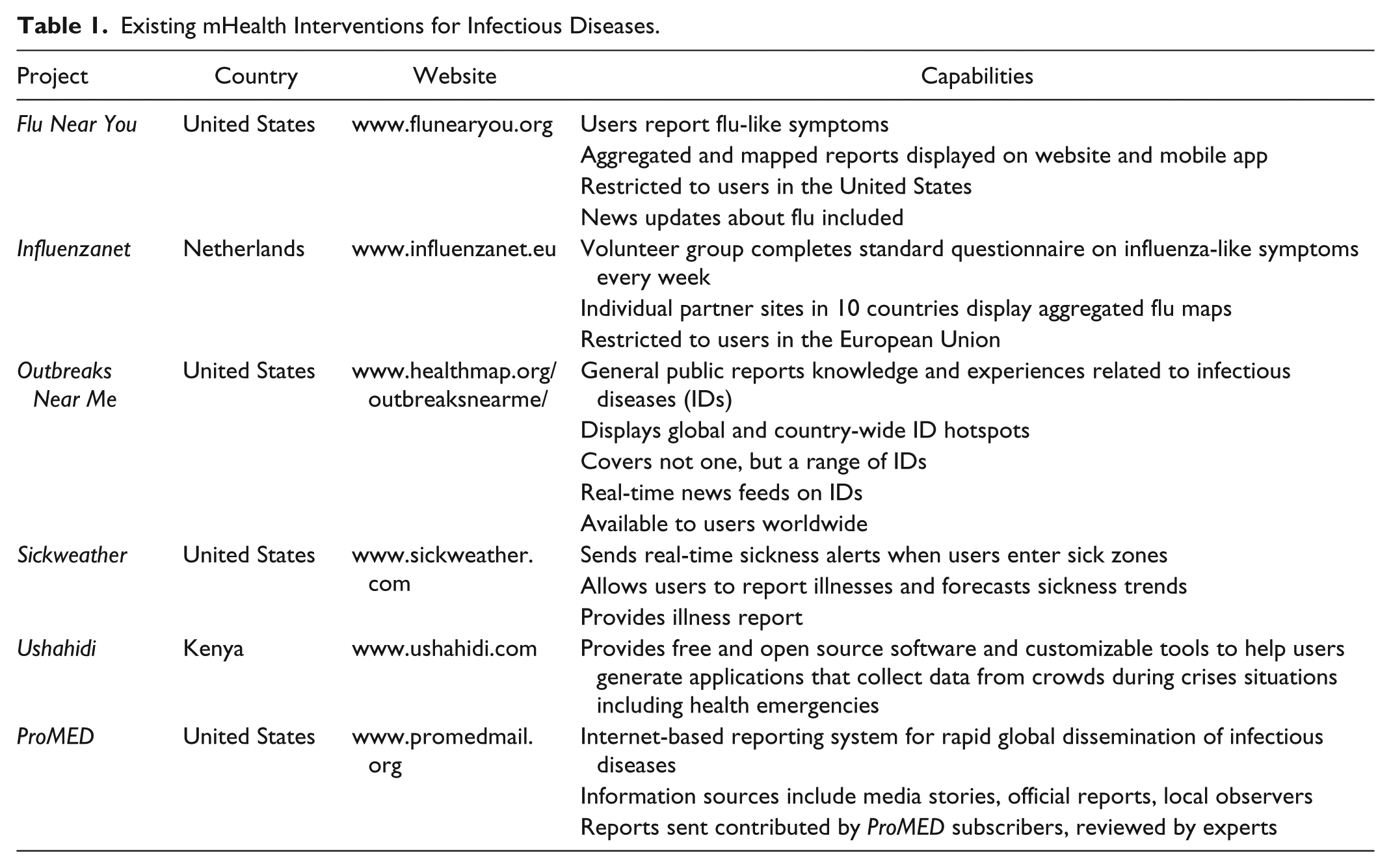
The performance of these innovations depends on the participation of the target users. While public health scholars are increasingly chronicling such initiatives, there is a surprising lack of answers to the core behavioral questions underpinning them. Specifically, we have yet to understand the motivational sources for users to participate in such systems and send their reports. What are the contextual considerations that influence people’s participation in such a system and how can we use an understanding of the underlying behavioral dynamics to shape future mHealth intervention design? We sought answers to these questions by conducting a baseline evaluation of a participatory mHealth system for dengue prevention, called Mo-Buzz, which was launched in February 2015 for the general public in Colombo, Sri Lanka.
Mo-Buzz: Socially Mediated Dengue Surveillance and Education System
The Mo-Buzz system (Lwin et al., 2014), currently available on the Android platform to one million residents of Colombo, integrates three components of dengue prevention: (1) Crowdsource-based surveillance: Mo-Buzz enables users to contribute to surveillance of mosquito breeding sites in the city. The user can take an automatically geo-tagged picture of the breeding site, add remarks, and send this report to the Colombo Municipal Council (CMC) with the click of a button. The report is automatically assigned to the nearest Public Health Inspector who can carry follow-up actions (such as spraying pesticides) and report actions taken back to the user. (2) Digital mapping of dengue cases: This component uses a color-coded Google map to alert users of possible dengue hotspots based on real dengue cases and offers users the option to telephonically call the Medical Officer for Health in their area with questions or concerns. (3) Health education: Mo-Buzz offers graphics-based information about dengue focusing on dengue statistics, modes of transmission, list of danger sites at home and public areas, symptoms, and treatment and prevention. Such information can be shared by users with their social networks using social media channels.
Conceptual Framework
We investigate Mo-Buzz through the theoretical lens of behavioral change related to technology adoption. The classical Technology Acceptance Model (TAM) by Davis (1989) offered perceived usefulness (PU) and perceived ease-of-use (PEOU) as determinants of perceived intention-to-use (PI) the technology. Venkatesh and Bala (2008) synthesized scientific evidence on TAM and proposed that individual differences, system characteristics, social influence, and facilitating conditions influence PU and PEOU. When applied to Mo-Buzz, the modified TAM enables the examination of the extent to which potential users in a city with high mobile phone penetration, such as Colombo, would find Mo-Buzz useful and easy-to-use (International Telecommunication Union, 2015b). At the individual level, we draw from the Protection Motivation Theory (Rogers & Prentice-Dunn, 1997) to assess whether perceived severity of and susceptibility to dengue in their city bears on perceived usefulness. Where facilitating conditions are concerned, we examine whether users’ beliefs about the ability of the Colombo Municipal Council (CMC) to respond effectively (perceived organizational efficacy) to breeding site reports, and their trust in the CMC (institutional trust) shapes attitudes toward the technology. From the social influence standpoint, we examine whether cultural dimensions (individualism vs. collectivism) interact with PU to influence behavioral intention. According to Hofstede (1984), these dimensions allow for the assessment of how personal needs and goals are prioritized against those of the group/clan/organization. Hence, users would be more inclined to report breeding sites and share health educational content if they believed it would protect those in their social network and communities from dengue. Our baseline evaluation of Mo-Buzz is driven by three research questions:
Method
Study Setting
Sri Lanka has grappled with dengue epidemics for the past 5 years with the Ministry of Health reporting more than 44,000 cases in 2014. Our evaluation was conducted through a field survey of potential Mo-Buzz users in the political capital of Colombo, located in the western province, which bears more than half of Sri Lanka’s dengue burden. Interestingly, Sri Lanka’s rising dengue threat has coincided with the growth of a mobile phone industry that boasts one of the fastest penetration rates and cheapest cellular services in the developing world, thus providing a fertile environment for our intervention (International Telecommunication Union, 2015a).
Procedures
We assessed responses to questions via in-person pen-and-paper survey of mobile phone users in Colombo. Using a snowball sampling approach, respondents were recruited through mass emails and word-of-mouth by students and staff from University of Colombo, People’s Bank, Mobitel, and Rupavahini Corporation. After small groups of 10 to 15 participants were invited to a meeting room in their respective premises, research staff briefed them on the study purpose and sought informed consent. The three functionalities of Mo-Buzz were subsequently illustrated and explained using demonstrations with mobile devices. Research staff allowed those participants with further questions or doubts to briefly use the application on one of three mobile devices (two tablets, one mobile phone) and experience it for themselves. Following this, participants were requested to respond to a 30-minute survey questionnaire. On completion of the questionnaire, each participant was provided a shopping voucher worth Sri Lanka Rs 1,500 (~US$11.00) as a token of appreciation for participation. The study was approved by Nanyang Technological University’s Institutional Review Board.
Sample Size
A G*Power analysis (Faul, Erdfelder, Lang, & Buchner, 2007) indicated an optimal sample size of 372 for the study’s statistical validation. The analysis was conducted to test for the sample size required to perform analysis of variance tests and multiple regressions at a 99% confidence interval so as to avoid compromising statistical validity. The researchers collectively decided to increase the required sample size to account for missing data points.
Participants
As seen in Table 2, our final sample consisted of 404 adults aged at least 18 years old (34.90% female and 64.60% male) who participated in this study. More than half of the participants in this study were aged 30 or younger and almost all of them were Sinhalese (the majority racial group in Sri Lanka). More than 80% of the sample had received a certificate or diploma in their education and majority of them reported monthly household income between Rs 25,001 and 75,000 (US$189-378).
Demographics of the Respondents (N = 404).

Measures
The questionnaire commenced with demographic questions and proceeded to capture variables at the individual, organizational, and societal levels. First, PEOU (e.g., It is easy to educate myself about dengue using this application), PU (e.g., Reporting dengue breeding sites or dengue symptoms to civic authorities will ensure they take the required action), and intention to use Mo-Buzz (e.g., I intend to find out more information about this dengue mobile application) were adapted from the classical TAM (Davis, Bagozzi, & Warshaw, 1989). Perceived severity (e.g., Dengue is a serious disease), perceived susceptibility (e.g., I feel that I am at high risk of getting dengue now), and behavioral control (e.g., It is entirely up to me to decide whether to use this application or not) were adapted from the protection motivation theory (Rogers & Prentice-Dunn, 1997) and the theory of planned behavior (Ajzen, 1991). Perceived credibility (e.g., I believe the authorities will monitor this system regularly), adapted from West’s (1994) study, and institutional efficacy (e.g., The authority will take investigation on the breeding sites reported), adapted from Wright, Pratt, Lowenkamp, and Latessa’s (2013) study, were used to capture participants’ trust on local health authority/institution. Last, psychometric scales adapted from Singelis, Triandis, Bhawuk, and Gelfand (1995) measured participants’ individualism (e.g., One should live one’s life independently of others) and collectivism (e.g., It is important to maintain harmony within my group). All constructs comprised three 5-point Likert-type scale items except perceived susceptibility, individualism, and collectivism, which contained only two items each. All scales were validated through exploratory factor analysis with eigenvalues larger than one and yielded moderate to high reliability with Cronbach’s α ranging from .55 to .75. Perceived severity was excluded after this phase as the scale items demonstrated low factor loadings.
Analysis
Data were analyzed using SPSS Version 21 (IBM Corp, 2012). We first captured participants’ demographic profile using simple frequencies and means analyses. Interitem correlations (Table 3) were assessed between variables of interest and ranged from −0.04 to 0.46 establishing minimum potential for multicollinearity. Bivariate analyses of demographic differences were conducted through analysis of variance. Our analysis culminated with a stepwise linear regression that examined predictors of PI. Only variables that demonstrated statistical significance and lent themselves to reasonable theoretical explanations were retained in the final model.
Correlations for Constructs Used in Regression Model.

Note. N = 404.
p < .05. **p < .01. ***p < .001.
Results
Research Question 1 and Research Question 2: Demographic Differences in Intention-to-Use and Factors Determining Behavioral Intention
As reported in Table 4, an overall descriptive analysis of key variables of interest revealed highest mean scores for perceived usefulness, followed by collectivism and intention to use Mo-Buzz. We next present demographic analysis of key independent and outcome variables.
Descriptive Statistics for All Constructs.
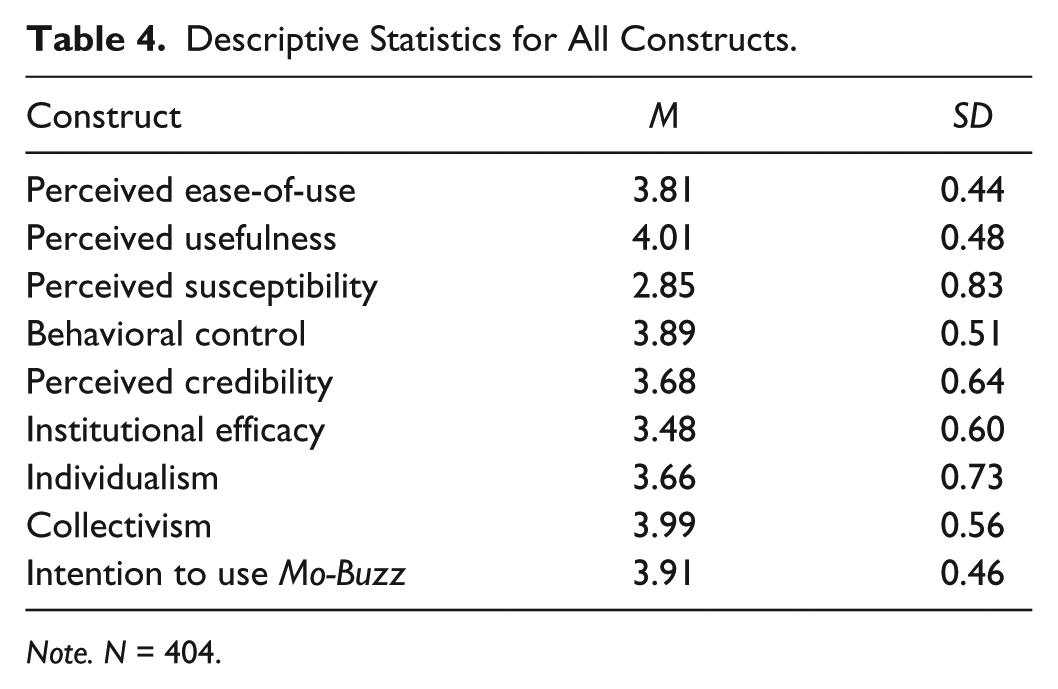
Note. N = 404.
Gender (Table 5)
None of the key variables demonstrated significant differences by gender. Participants across both genders reported relatively high perceived usefulness (≥4.00), collectivism (≥3.90), and intention to use Mo-Buzz (≥3.90).
Comparisons for All Constructs by Gender.

Note. N = 402. a and b denote p < .05 using Tukey’s HSD post hoc tests.
Age (Table 6)
Participants in the 31 to 40 years age group reported highest scores in both perceived ease-of-use and individualism. However, participants aged 41 years and older were found to have significantly higher institutional efficacy and collectivism than people in the 18 to 30years age group. Intention-to-use Mo-Buzz did not differ significantly by age.
Comparisons for All Constructs by Age.

N = 404. a, b, and c denote p < .05 using Tukey’s HSD post hoc tests.
p < .05. **p < .01. ***p < .001.
Education (Table 7)
Certificate or diploma holders were found to have significantly higher intention to use Mo-Buzz, perceived susceptibility, and institutional efficacy than the other two groups. On the other hand, university graduates tended to report better behavioral control than those who finished secondary school. Last, participants finished secondary school or attained a certificate or diploma were more individualistic than people who were educated at the university level.
Comparisons for All Constructs by Highest Educational Level.

Note. N = 401. a, b, and c denote p < .05 using Tukey’s HSD post hoc tests.
p < .05. **p < .01. ***p < .001.
Income (Table 8)
Intention-to-use did not differ significantly among income groups, neither did other variables except perceived susceptibility and institutional efficacy. Participants earning between Rs. 51,001 and Rs. 75,000 reported significantly lower perceived susceptibility than those in lower income brackets. Also, respondents earning Rs. 25,000 and below believed the health authority/institution to be efficient than participants earning more than Rs. 50,001.
Comparisons for All Constructs by Monthly Household Income.
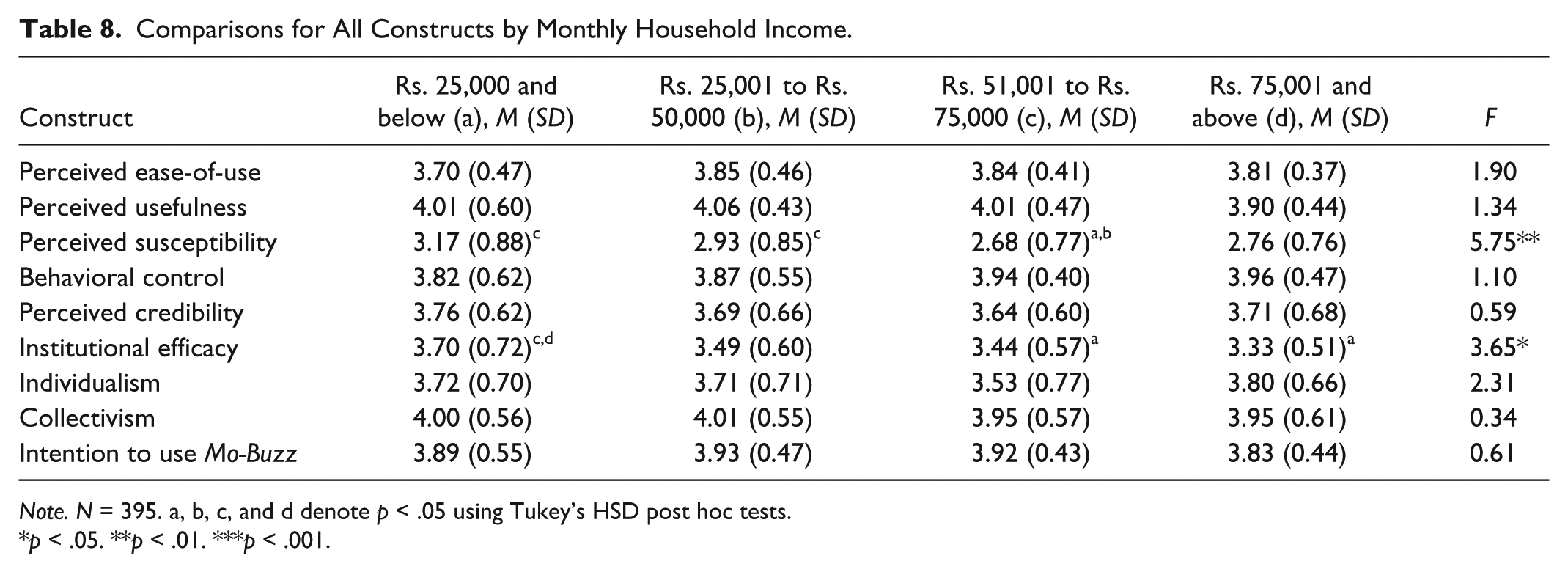
Note. N = 395. a, b, c, and d denote p < .05 using Tukey’s HSD post hoc tests.
p < .05. **p < .01. ***p < .001.
Research Question 3: Determinants of Behavioral Intention-to-Use (PI)
As seen in Table 9, we examined determinants of intention-to-use Mo-Buzz by conducting a three-stage hierarchical multiple regression model. The first stage comprised four demographic variables—gender, age, education, and income—none of which contributed significantly to the model that explained 1% of the variance in the dependent variable. The second stage, controlling for demographic variables, and including a range of factors at different levels explained 32% of the variance in intention-to-use. Among individual factors, PEOU and behavioral control contributed significantly to the predictive ability of the model while PU was a marginally significant predictor. Under organizational factors, institutional efficacy was a significant predictor of intention-to-use. Of the factors examined at the societal level, collectivism was found to significantly predict intention-to-use. Based on TAM literature, we further explored the possibility of interaction effects between TAM variables and other behavioral determinants. Our analysis showed no significant interaction effects with Model 3 contributing only an additional 2% to the predictive ability of Model 2 despite the addition of five new interactions. In the interest of parsimony and statistical rigor, we retained Model 2 as the final model.
Regression on Intention to Use Mo-Buzz.
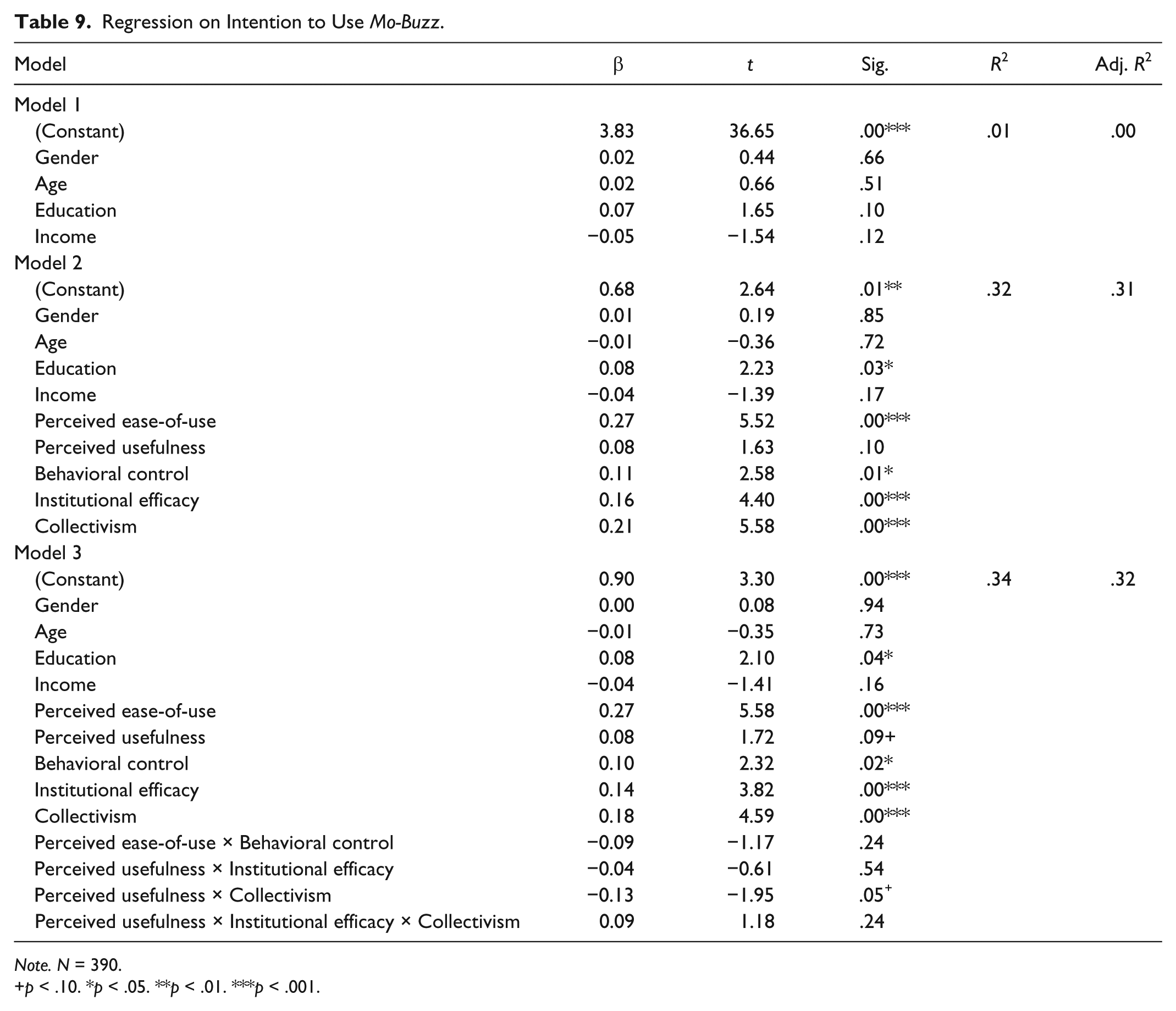
Note. N = 390.
p < .10. *p < .05. **p < .01. ***p < .001.
Discussion
As mobile-driven participatory mechanisms of infectious disease prevention continue to mushroom, our study highlights behavioral dynamics underlying “participation—the construct that determines their success or failure. In doing so, we studied the Mo-Buzz intervention that not only enables mobile-based crowdsourced surveillance for dengue but also integrates it with shareable health education and digital disease mapping. Additionally, while most crowdsource-based initiatives are geared toward a global audience and invite voluntary reporting of disease-related incidents to a generic mobile or web platform, Mo-Buzz facilitates a clear communication channel between the user and civic authorities. Here, the user knows that his report directly reaches the public health department that is authorized to respond to his complaint, and is able to track the actions taken by the CMC on his report. From a behavioral standpoint, this process involves a unique interaction of conscious participation by an individual with how highly he perceives the health agency to be efficacious in its response, how highly he perceives himself at risk for dengue, and possibly his level of concern vis-à-vis the larger community. In this context, our key objective was to generate a baseline assessment of the intention to use Mo-Buzz among potential users, and gain an understanding of the psychosocial context impact the users’ beliefs about the technology. We were encouraged by an overall high intention to use (PI) and identified a mix of demographic and psychosocial factors that shaped users’ attitudes toward the system’s potential adoption.
Being among the first studies of its kind in Sri Lanka, this research was hampered by two main limitations. First, adopting a convenience sampling strategy instead of randomized stratified sampling compromised the generalizability of our results, a problem partially addressed by maximizing our sampling frame. Second, the lack of superior reliabilities of our scales limited the internal consistency of our survey, an expected constraint given most of the constructs were not used in this study context previously. Our factor analysis helped address this limitation and ensured acceptable reliabilities for our scales.
While PI was high at baseline, a complex psychosocial process, involving factors at multiple levels of the social ecosystem, underlies future participation in an intervention like Mo-Buzz. At the individual level, our study reinforced current wisdom in technology adoption literature by demonstrating the significant contribution of PEOU and PU to predicting PI. Demographically speaking, younger participants found Mo-Buzz easier to use than their older counterparts. Although previous TAM research demonstrated an ambivalent impact of age on PEOU (Morris & Venkatesh, 2000), we notice this pattern given that the penetration of smartphones has yet to reach greater levels in Sri Lanka, especially so among the older population. PU, nevertheless, remained consistently high among demographic groups and fortified our belief in the utility of our intervention for the general public. Perceived behavioral control, another significant predictor of behavioral intention, increased with educational level. This trend can be explained by the possible ability of highly educated participants to afford smartphones and possess the requisite self-confidence to use the application independently.
At the organizational level, our analyses revealed that older participants reposed greater faith in the CMC’s ability to respond to the mosquito reports sent through Mo-Buzz. But as we have seen above, younger participants perceived Mo-Buzz as easier to use as opposed to the older participants. These contrasting patterns pose a challenging adoption conundrum where potential users who find Mo-Buzz easier to use might be less inclined to use it on account of lower institutional efficacy. The CMC can apply these insights to utilize our intervention as a mechanism to strengthen public perceptions by, for instance, recruiting younger community members as official volunteers or health champions who can strengthen CMC’s surveillance through Mo-Buzz.
From variables at the societal level, the significant contribution of collectivism in predicting behavioral intention was expected given that Sri Lanka is identified as a collectivistic culture according to Hofstede’s cultural dimensions (Itim International, 2014). Collectivistic tendencies increased with age, a pattern possibly explained by the fact that cultural influences gradually shape people as they grow older (Boone, Meng, & van der Velden, 2007). In the Mo-Buzz context, we postulate that high collectivism scores among the oldest participants must be considered in concert with this group reporting highest perceived institutional efficacy and high perceived usefulness of the application.
Describing the big data revolution in public health, Hay et al. (2013) remarked on users’ participation in crowdsourced surveillance initiatives that “motivating people to devote some of their cognitive surplus to crowd sourcing is possible, so long as the products and benefits are immediately available to all for the common good” (p. 3).Although we recognize the spirit of this observation, our acceptance of it from a behavioral perspective is cautious and nuanced. We argue, instead, that the “immediate availability of products and benefits”—largely based on the construct of proximal gratifications from behavioral economics literature—might be one of the many motivators in a complex web of factors as demonstrated by our study. Also, the relative influence of these factors on the acceptance and use by intended users might depend on the type of participatory mHealth intervention. For instance, the behavioral dynamics between a global, generic intervention like Outbreaks Near Me might differ from those for a locally tailored intervention like Mo-Buzz. The exact nature of these differences needs to be examined urgently by health behavior scholars if the imminent proliferation of mHealth participatory interventions as part of the big data phenomenon in the future must positively benefit vulnerable populations.
The study’s findings bear important implications for our intervention design moving forward. For instance, the CMC may consider communication campaigns through mass media or community workshops aimed at training elderly residents in using Mo-Buzz with a view to enhance PEOU, and through their positive attitudes, reach networks of younger groups. Similarly, the CMC may engage in stronger public relations initiatives that periodically update local communities about the number of actions they have initiated in response to mosquito reports. Such programs might achieve the twin objectives of strengthening CMC’s image among populations cutting across age groups, while increasing the user base resulting in more efficient surveillance.
Conclusion
Utilizing the power of mobile phones to capture the intelligence of crowds for strengthening infectious disease prevention and management is an exciting idea for public health professionals and researchers but is beset with complex challenges. The foremost of these is their elementary dependency on people’s participation, which, as demonstrated by our study, involves complex behavioral considerations. As public health grapples with the big data wave, the future design of such interventions will require a conscious incorporation of psychosocial considerations at different levels of the public health ecosystem in a manner that enhances popular motivation. Future research must examine the inherent challenges in catalyzing participation from other theoretical lenses and using more robust methodologies, so as to inform our understanding and insights in a manner that benefits future interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the National Research Foundation, Prime Minister’s Office, Singapore under its International Research Centres in Singapore Funding Initiative and administered by the Interactive Digital Media Programme Office.