
Abstract
Objectives. In a sample of primary care participants with chronic physical conditions and comorbid depressive symptoms: to describe the cross-sectional and longitudinal associations of activation and self-efficacy with demographic, physical and mental health status, health behaviors, depression self-care, health care utilization, and use of self-care tools; and to examine the effects of a depression self-care coaching intervention on these two outcomes. Design/Study Setting. A secondary analysis of activation and self-efficacy data collected as part of a randomized trial to compare the effects of a telephone-based coached depression self-care intervention with a noncoached intervention. Activation (Patient Activation Measure) was measured at baseline and 6 months. Depression self-care self-efficacy was assessed at baseline, at 3 months, and at 6 months. Principal Findings. In multivariable cross-sectional analyses (n = 215), activation and/or self-efficacy were associated with language, birthplace, better physical and mental health, individual exercise, specialist visits, and antidepressant nonuse. In longitudinal analyses (n = 158), an increase in activation was associated with increased medication adherence; an increase in self-efficacy was associated with use of cognitive self-care strategies and increases in social and solitary activities. There were significant improvements from baseline to 6 months in activation and self-efficacy scores both among coached and noncoached groups. The self-care coaching intervention did not affect 6-month activation or self-efficacy but was associated with quicker improvement in self-efficacy. Conclusions. Overall, the results for activation and self-efficacy were similar, although self-efficacy correlated more consistently than activation with depression-specific behaviors and was responsive to a depression self-care coaching intervention.
Activation can be defined as a multidimensional construct that refers to peoples’ knowledge, skill, and confidence to manage their health and health care in general (Chen, Mullins, Novak, & Thomas, 2016). Self-efficacy, in contrast, refers to peoples’ confidence to carry out specific behaviors to control a specific health condition (Bandura, 2004). Activation is not disease- or condition-specific, whereas self-efficacy is. It is therefore important to determine which of these constructs is more relevant to clinicians and researchers when implementing interventions that aim to improve self-management among people with chronic conditions. These interventions can be challenging among those who suffer from chronic physical conditions with comorbid depressive symptoms, who typically have low levels of self-efficacy and activation (Magnezi, Glasser, Shalev, Sheiber, & Reuveni, 2014; Stepleman et al., 2010). While some have advocated that measures of activation can be used at the individual patient level to tailor interventions and assess changes (Hibbard, Stockard, Mahoney, & Tusler, 2004), there is little evidence to support this assertion. Similarly, there appears to be little clinical use of self-efficacy measures.
We have conducted a single blind, individually randomized, pragmatic trial of a coaching intervention for depression self-care among primary care participants with a chronic physical illness and comorbid depressive symptoms. The intervention was designed on cognitive–behavioral therapy principles and adapted following promising results of a feasibility study (McCusker, 2012). Both study groups received a depression self-care toolkit; the coached group also received regular telephone calls by a trained lay coach. In analyses of the primary outcome, depressive symptoms, we found that the coaching improved the severity of depressive symptoms at 3 months but not at 6 months (McCusker et al., 2015). Specific objectives of the current secondary analysis of trial data were to (1) describe the cross-sectional associations of activation and self-efficacy with demographics, physical and mental health status, health behaviors, depression self-care, and health care utilization; (2) describe the longitudinal associations of changes over time in activation and self-efficacy with changes in health behaviors and use of the Toolkit; and (3) determine whether the coaching intervention increased activation and/or self-efficacy at follow-up. We hypothesized that (1) activation and self-efficacy would be associated with health-promoting behaviors at baseline; (2) improved health behaviors over time would be associated with increases in activation and self-efficacy; (3) coaching would have a positive impact on both measures.
Method
Design and Participants
The trial protocol was registered (McCusker, 2012) and approved by the St. Mary’s Hospital Research Ethics Committee; the methods are reported in detail elsewhere (McCusker et al., 2015). Participants were recruited in the practices of 41 Montreal-area family doctors. Eligibility criteria included age 40 years or more; at least one self-reported doctor-diagnosed chronic physical condition or chronic pain of at least 6 months duration; Patient Health Questionnaire-9 (PHQ-9) score of five or more, indicating at least mild depression symptoms (Lowe, Kroenke, Herzog, & Grafe, 2004); not suicidal; community dwelling; able to read in either English or French; at most mild cognitive impairment (score of less than 10 on the six-item Blessed Orientation-Memory-Concentration [BOMC] test; Davous, Lamour, Debrand, & Rondot, 1987); and no visual, hearing, or other physical impairment that would prevent participation in the intervention. Because of the pragmatic intent of the trial, we did not exclude participants who were taking antidepressant medications or were receiving counseling. However, because the intervention was cognitive–behavioral therapy based, we excluded participants who were receiving this type of treatment. Following written informed consent, a baseline structured interview was conducted (either in person or by telephone) by a research assistant. Follow-up telephone interviews were conducted at 3 and 6 months after randomization by a second research assistant who was blinded to the randomization assignment.
We randomized participants individually, within strata defined by clinic, family doctor, and method of referral (self-referred vs. physician-referred) using random block sizes of two or four with an allocation ratio of 1:1. Sequences were generated with SAS (version 9.3) software. The randomization assignment was given in a sealed, opaque envelope to the research assistant who opened the envelope following the baseline interview.
Interventions
Immediately after randomization all participants received a Toolkit comprising three core tools recommended for everyone (Antidepressant Skills Workbook in both paper and audio versions [Bilsker & Paterson, 2010], a Mood Monitoring Tool, and an informational DVD). Three supplemental tools (relaxation CD, information on medications, and on emotional eating) and additional self-help resources were also included, and recommended according to participant-reported problems and symptoms. Additional information (reading materials, Internet sites, community groups, and a booklet on depression to share with a family member or friend) was also provided.
Participants randomized to the Intervention group were assigned a trained lay coach, whose role was to guide and encourage them in the use of the Toolkit. Coaches were trained and supervised by a clinical psychologist who monitored the fidelity of the intervention by reviewing coach logs and listening to a sample of audiotaped sessions. Each successive coach contact was scripted and had an agenda. After the first two sessions in which the Toolkit was introduced and participants were encouraged to try the three core tools, participants were offered short (~10 minute) weekly calls for up to 3 months, followed by monthly calls up to 6 months. Coaches used the PHQ-9 at each session to monitor the severity of depressive symptoms and to tailor the intervention to specific symptoms or problems reported during the session. Specific interventions were matched to reported problems as described in the coaching manual.
Measures
Activation
The 13-item Patient Activation Measure (PAM–Chronic Disease version; Hibbard et al., 2004) was administered at baseline and at 6 month follow-up. Each item has a 4-point Likert-type response scale (strongly disagree to strongly agree); the total weighted score of the 13-item scale, using a proprietary algorithm, ranges from 0 to 100. The PAM-13 is a reliable and valid scale (Hibbard, Mahoney, Stockard, & Tusler, 2005). We translated the PAM-13 into French, with an independent back-translation to validate the translation. For our sample, Cronbach’s alpha values were .76 and .83 for the English and French versions, respectively.
Self-Efficacy
Self-efficacy specific to depression self-care was a four-item scale adapted from a validated diabetes self-efficacy scale (Williams, Freedman, & Deci, 1998), measured with the same response scale as the PAM: “I am able to carry out daily activities that can keep my mood positive”; “I feel confident that I can recognize situations that will bring my mood down”; “I feel able to meet the challenges of learning and practicing new skills to control my mood”; and “I am capable of stopping my mood from becoming negative.” Cronbach’s alpha was .73. The self-efficacy score was converted to a 100-point scale to facilitate comparison with the PAM. For our sample, Cronbach’s alpha values were .55 and .83 for the English and French versions, respectively. Deletion of single items did not improve the alpha level in either language.
The correlation of the self-efficacy scale with the PAM at baseline was .51 (n = 215) and at follow-up .67 (n = 158). The minimal clinically important difference has not been established for either the PAM or the self-efficacy scale.
Health Behaviors at Baseline and at 6 Months
Exercise
We used two measures of exercise during the previous week (Craig et al., 2003): number of times participated in group exercise activities (e.g., dance, bowling) and number of days with individual exercise (e.g., walking, gardening).
Activities
Participants reported the frequency (number of times or number of days) of 13 everyday activities during the week before the interview, adapted from those used in previous research (Aartsen, Smits, van Tilburg, Knipscheer, & Deeg, 2002; Glass, De Leon, Bassuk, & Berkman, 2006; Menec, 2003; Scarmeas, Levy, Tang, Manly, & Stern, 2001). These include three types of activity: social (e.g., visits with family), solitary (e.g., hobbies), and productive (e.g., housework). The frequency of the activities was summed within each of the three groups.
Smoking, alcohol, medication adherence
Information on current smoking and alcohol consumption was collected using structured interview questions (Berkman, Breslow, & Wingard, 1983). Adherence to medication (any medication, not just antidepressants) was determined using a four-item, ordinally scaled questionnaire (Morisky, Green, & Levine, 1986). Total scores range from 0 to 4 (high nonadherence).
Depression Self-Care Behaviors
These behaviors were coded from responses to an open-ended question at 6-month follow-up: “Since participating in this project, have you tried to change something in your daily life to help you feel better? If yes, can you please tell me what these changes were?” Responses were coded by consensus among two investigators (JM and MC) and grouped into two categories: cognitive skills (e.g., realistic thinking) and increased activation (e.g., making time for personally rewarding activities). Participants who reported any change were asked whether they discussed it with their family doctor.
Use of Self-Care Tools
Use of the tools provided in the Toolkit was assessed at 3- and 6-month follow-up and was coded as (1) number of paper tools used (0-4: workbook-paper version, mood monitoring, medication misuse, and emotional eating); (2) whether or not notes were written in either the Workbook or Mood Monitoring tool; (3) number of audiovisual tools used (0-3: DVD, workbook-audio version, and relaxation CD); and (4) use of any additional resources (yes-no; e.g., websites, books, or community groups).
Physical and Mental Health Status
The PHQ-9 was selected as the primary outcome measure of the severity of depressive symptoms in the randomized controlled trial, based on its brevity, widespread use (Kroenke, Spitzer, Williams, & Lowe, 2010), established severity ranges, and sensitivity to change (Lowe et al., 2004). Other health status measures included in the baseline and 6-month interviews were the SF-12 Physical Component Summary (PCS) and SF-12 Mental Component Summary (MCS) scores (Ware, Kosinski, & Keller, 1996), and the General Anxiety Disorder–7 items (GAD-7; Spitzer, Kroenke, Williams, & Lowe, 2006). At baseline only, we assessed the Charlson Comorbidity Index coded from self-reported diagnoses (D’Hoore, Bouckaert, & Tilquin, 1996) and the BOMC test for mild cognitive impairment (Davous et al., 1987). We used the CAGE questionnaire (an acronym of its four questions: Cut-down, Annoyed, Guilty, Eye-opener) with a score of one or more to denote possible alcohol abuse (Dhalla & Kopec, 2007).
Sociodemographics and Health Care Service Utilization
At baseline, we collected data on age, sex, educational attainment (less than high school, high school completed, or university completed), preferred language (English or French), birthplace (Canada or other), and health services utilization (hospitalizations, doctor and ED visits, and homecare services during previous 3 months). Self-reported treatments at baseline included counseling interventions and use of antidepressant medications.
Data Analysis
We compared the following 10 baseline covariates (prespecified in the initial randomized controlled trial: age, sex, education, PHQ-9 score, SF-12 PCS, Charlson Comorbidity Index, GAD-7 score, self-efficacy, current antidepressant medications, and counseling) and the following additional variables that were relevant to this secondary analysis (SF-12 MCS, current psychotropic medications other than antidepressants, and total number of prescribed medications) to identify variables with potentially clinically significant baseline imbalances across intervention and control groups.
Objective 1: Cross-Sectional Associations
We conducted linear regressions separately for PAM and self-efficacy (Neter, Wasserman, & Kutner, 1985), using the Bayesian information criterion to guide variable selection (Harrell, 2001; Schwarz, 1978).
Objective 2: Longitudinal Associations
We developed regression models to study the association between the change from baseline to 6 months in PAM/self-efficacy and 6-month outcomes (health behavior changes, depression self-care behaviors, and use of self-care tools). Linear, ordinal, or logistic regression was applied, respectively, for continuous, ordinal, or binary outcomes (Hosmer & Lemeshow, 1989; Neter et al., 1985), with adjustment for baseline values of the activation or self-efficacy score and the outcome (if available).
Objective 3: Responsiveness
For each study group, follow-up time, and outcome, we computed the effect size of the change over time with its 95% confidence interval (Kadel & Kip, 2012).
The effects of the coaching intervention on PAM at 6 months, and self-efficacy at 3 and 6 months, was assessed by t tests and linear regression models (Brown & Prescott, 1999; Neter et al., 1985), with adjustment for baseline variables. We tested the following interactions: between study group and baseline PAM and self-efficacy for 6-month PAM and self-efficacy; and between study group and baseline PAM for 6-month PHQ-9 (a significant interaction between study group and baseline self-efficacy was previously reported for the PHQ-9; McCusker et al., 2015). All interactions terms were tested at α = .10. Intervention effect sizes were computed as the difference between the two estimated means divided by the pooled standard deviation (Cohen, 1988); 95% confidence intervals (CIs) and p values were calculated (Borenstein, Hedges, Higgins, & Rothstein, 2009; Hedges, 2009). Note that the trial was powered to detect an intervention effect size of at least 0.4.
SAS version 9.4 and Stata 13 software were used to conduct the statistical analyses. No adjustment was made for multiple testing. We did not include random terms for clinic or doctor in the models, because the Intraclass correlation coefficients were small (<1%) and not statistically significant (Snijders & Bosker, 1999).
Results
Participants’ Characteristics
Among 223 randomized participants, 215 (96.4%) completed PAM and self-efficacy measures at baseline. Among these 215, 158 (73.5%) completed both measures at 6 months. Table 1 shows characteristics of the sample at baseline, by study group. The intervention group was more highly educated, was less depressed, but more often on antidepressant medications; the control group more often was receiving other psychotropic medications and counseling. These variables were considered in subsequent regression models.
Patient Baseline Characteristics by Randomization (N = 215).

Note. PHQ-9 = Patient Health Questionnaire; SF-12 PCS = 12-item Short Form Physical Composite Score; SF-12 MCS = 12-item Short Form Mental Composite Score; GAD-7 = Generalized Anxiety Disorder; PAM = Patient Activation Measure.
One missing.
Objective 1: Cross-Sectional Associations
In multivariable analyses, high mean PAM scores were associated with French language, born outside Canada, more frequent individual exercise, higher MCS score, and lower comorbidity (Table 2). Among those born outside Canada, PAM scores were not associated with country of birth or number of years living in Canada (data not shown).
Univariate and Multivariable Analyses of Variables Associated With Activation and Self-Efficacy at Baseline (N = 215).

Note. Bold values are statistically significant, p < 0.05. CI = confidence interval; SF-12 PCS = 12-item Short Form, Physical Composite Score; SF-12 MCS = 12-item Short Form, Mental Composite Score; PHQ-9 = Patient Health Questionnaire; GAD-7 = Generalized Anxiety Disorder; ER = emergency room; FP = family physician; BIC = Bayesian information criterion.
Both measures range from 0 to 100; Beta are the estimates computed from linear regression model. Multivariable model also include the variables that were selected after the application of the BIC criteria in each block of variable for each outcome.
p < .05. ~p < .01.
In multivariable analyses, the following variables were associated with higher self-efficacy: higher MCS score, a zero comorbidity score, nonpsychiatric specialist visits, and nonuse of antidepressants (Table 2).
Objective 2: Longitudinal Associations
Among depression self-care behavior changes at 6 months, the number of cognitive changes was associated with increased self-efficacy (Table 3). Among the changes in health behaviors from baseline to 6 months, increased medication adherence was associated with an increase in the PAM score; increases in social and solitary activities were associated with increases in self-efficacy scores.
Six-Month Outcomes Associated With Changes in Activation and Self-Efficacy From Baseline to 6 Months.
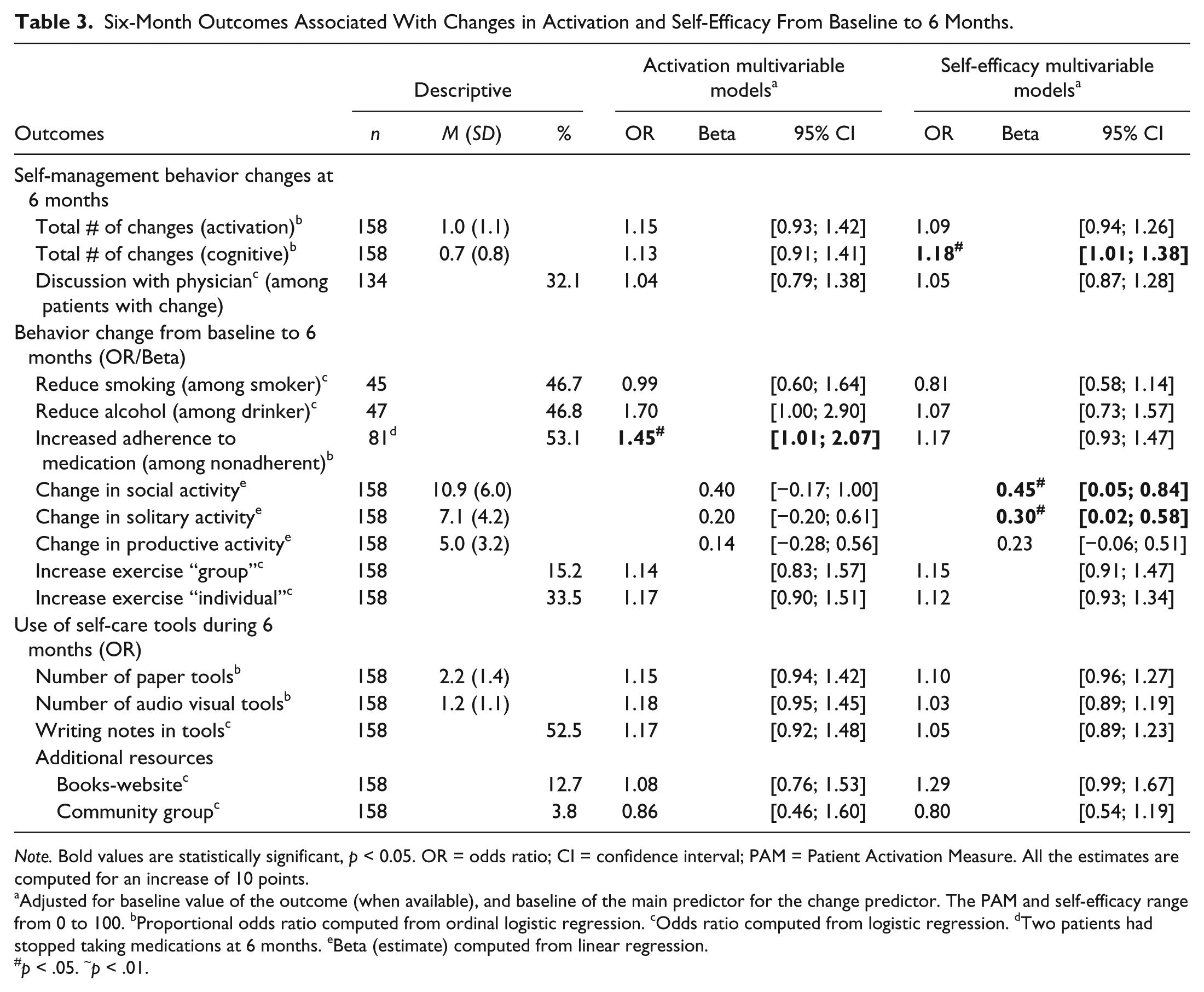
Note. Bold values are statistically significant, p < 0.05. OR = odds ratio; CI = confidence interval; PAM = Patient Activation Measure. All the estimates are computed for an increase of 10 points.
Adjusted for baseline value of the outcome (when available), and baseline of the main predictor for the change predictor. The PAM and self-efficacy range from 0 to 100. bProportional odds ratio computed from ordinal logistic regression. cOdds ratio computed from logistic regression. dTwo patients had stopped taking medications at 6 months. eBeta (estimate) computed from linear regression.
p < .05. ~p < .01.
Objective 3: Responsiveness
Increases over time in mean PAM and self-efficacy scores were of similar magnitude and statistically significant in both study groups (Table 4). While the coaching intervention had no significant effect on 6-month PAM and self-efficacy scores, the linear mixed effect model for self-efficacy using the three time points indicated a significant quadratic effect of time (p = .008) and a significant interaction between time and study group (p = .034), indicating that the increase in self-efficacy in the intervention group occurred more quickly than in the control group.
Effect of the Coaching Intervention on Activation and Self-Efficacy at Follow-Up (N = 158).
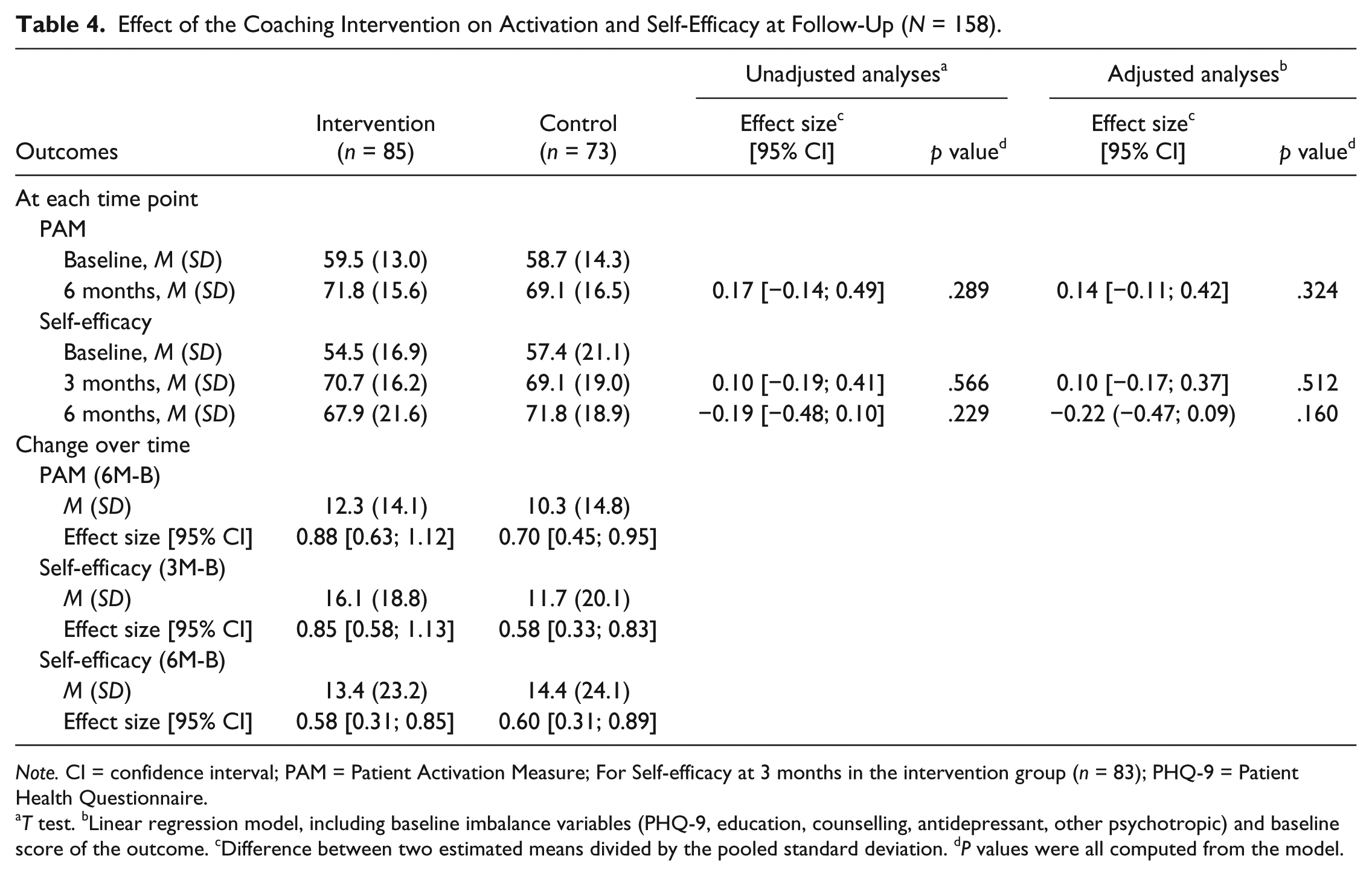
Note. CI = confidence interval; PAM = Patient Activation Measure; For Self-efficacy at 3 months in the intervention group (n = 83); PHQ-9 = Patient Health Questionnaire.
T test. bLinear regression model, including baseline imbalance variables (PHQ-9, education, counselling, antidepressant, other psychotropic) and baseline score of the outcome. cDifference between two estimated means divided by the pooled standard deviation. dP values were all computed from the model.
None of the other interactions tested was statistically significant (p > .10).
Discussion and Conclusions
This study, in a sample of primary care participants with chronic physical conditions and comorbid depressive symptoms, aimed to better understand the role of activation and self-efficacy in health behavior change and the effects of a coaching intervention.
We had hypothesized that both activation and self-efficacy would be associated with health-promoting behaviors at baseline. We found that study participants with better physical and mental health, who engaged in more frequent individual exercise, were more activated, corroborating previous research (Magnezi et al., 2014; Skolasky et al., 2011; Stepleman et al., 2010). New findings were that use of antidepressant medication was associated with lower self-efficacy, and nonpsychiatric specialist visits were associated with higher self-efficacy, even after adjustment for severity of depressive symptoms. The majority of participants with mild to moderate depression prefer counseling over medication (Dwight-Johnson, Sherbourne, Liao, & Wells, 2000); people who are more confident in their ability to control their depression symptoms may be more likely to question the need for antidepressant medications. As specialists require a referral from the family doctor, the association of self-efficacy with nonpsychiatric specialist visits may indicate that more confident people request referral for evaluation and/or treatment of their physical conditions. Both activation and self-efficacy scores were higher among participants born outside Canada, possibly due to a “healthy immigrant” effect (Gee, Kobayashi, & Prus, 2004) or to an acquiescence response bias (Saris, Revilla, Krosnick, & Shaeffer, 2010). We found language differences for activation, but not self-efficacy: French-speaking participants had higher PAM scores than English speakers. Item analysis of agree–disagree response scales in French versus English suggests the translation of the response scale may affect item difficulty levels (Haggerty, Bouharaoui, & Santor, 2011).
We had hypothesized that improved health behaviors over time would be associated with increases in activation and self-efficacy. We found, in longitudinal analyses, that there were increases in health behaviors targeted by the intervention: improvement in medication adherence was associated with increased activation, and increases in the frequency of social and solitary activities were associated with increased self-efficacy. Similar improvements have been observed among people receiving other self-care interventions (Deen, Lu, Rothstein, Santana, & Gold, 2011; Lawson et al., 2013; Wallace et al., 2009). Use of the cognitive skills targeted by the intervention (e.g., realistic thinking) were associated with increased self-efficacy.
We had hypothesized that coaching would have a positive impact on both activation and self-efficacy. Scores on both measures improved significantly from before to after the intervention, suggesting that both scales were responsive to the intervention. Although coaching did not have a differential impact on 6-month measures, there was a short-term (3 month) effect on self-efficacy, as found for depressive symptoms (McCusker et al., 2015). In randomized controlled trials of self-management interventions, activation scores do not consistently differ between intervention and control groups (Alegria et al., 2008; Alegria et al., 2014; Hibbard et al., 2005; Maindal, Sandbaek, Kirkevold, & Lauritzen, 2011).
Several study limitations should be acknowledged. First, the study sample comprised self-selected participants in a study of a depression self-care intervention; the results cannot be generalized to the population with chronic physical conditions and comorbid depressive symptoms. Second, there was no control group that did not receive the Toolkit. Third, the PAM was not administered at 3 months, to reduce respondent burden. Fourth, all participants had a regular source of care, a factor that has been associated with greater activation (Chen, Mortensen, & Bloodworth, 2014). Fifth, the depression self-efficacy scale has not previously been validated (although it was adapted from a validated scale) and had only moderate reliability among English-speaking participants. Despite this limitation, the depression-specific self-efficacy scale performed better than the nonspecific activation scale, suggesting that self-efficacy is more relevant than activation to depression self-care. Sixth, the depression self-care behavior measure was an open-ended question that had not been previously validated.
Implications for Research and Practice
This research has implications for four areas of future research and practice on depression self-care interventions. First, further research is needed on how best to tailor interventions to individual levels of activation and self-efficacy. Coaching effectiveness was modified by baseline self-efficacy (McCusker et al., 2015) but not by baseline activation. Those with lower levels of self-efficacy may require different approaches such as motivational interviewing (Rubak, Sandbaek, Lauritzen, & Christensen, 2005). Second, booster coaching contacts may be needed to increase the duration of intervention effects. Third, informal support from family or friends can be enlisted to strengthen the intervention (Sussman et al., 2014; Sussman et al., in press). Fourth, further psychometric work is warranted in an effort to improve the performance of both activation and self-efficacy measures for future use in research and clinical practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded under a grant from the Fonds de la recherche du Québec-Santé (FRQ-S), 2009-2016.