
Abstract
Social ecological models of health often describe multiple levels of influence that interact to influence health. However, it is still common for interventions to target only one or two of these levels, perhaps owing in part to a lack of guidance on how to design multilevel interventions to achieve optimal impact. The convergence strategy emphasizes that interventions at different levels mutually reinforce each other by changing patterns of interaction among two or more intervention audiences; this strategy is one approach for combining interventions at different levels to produce synergistic effects. We used semistructured interviews with 65 representatives in a cross-site national initiative that enhanced health and outcomes for patients with diabetes to examine whether the convergence strategy was a useful conceptual model for multilevel interventions. Using a framework analysis approach to analyze qualitative interview data, we found three synergistic themes that match the convergence strategy and support how multilevel interventions can be successful. These three themes were (1) enhancing engagement between patient and provider and access to quality care; (2) supporting communication, information sharing, and coordination among providers, community stakeholders, and systems; and (3) building relationships and fostering alignment among providers, community stakeholders, and systems. These results support the convergence strategy as a testable conceptual model and provide examples of successful intervention strategies for combining multilevel interventions to produce synergies across levels and promote diabetes self-management and that may extend to management of other chronic illnesses as well.
Keywords
Social ecological models of health assume that individuals exist within broader environments and systems that influence their behavior and their health (e.g., McLeroy, Bibeau, Steckler, & Glanz, 1988; Stokols, 1992; Stokols, Allen, & Bellingham, 1996). These models often describe multiple levels of influence on which to intervene, including the individual, interpersonal, organizational, community, and policy levels (McLeroy et al., 1988). These multilevel interventions incorporate levels of influence that interact to affect health and well-being. The social ecological perspective implies that interventions that target multiple levels of influence reinforce one another and should yield greater and more sustainable effects than interventions that target only one level of influence (Stokols, 1992; Stokols et al., 1996).
Although social ecological models support the benefits of using multilevel interventions, and this perspective is widely accepted among public health practitioners, it is still common for intervention activities to target only one or two of these levels of influence and to focus on individual and interpersonal levels, in particular (Golden & Earp, 2012). In recent years, there has been an increased focus on intervening on more macro levels of influence—the organizational, community, and political levels of social ecological models—and on targeting a greater number of levels of influence within one intervention (Richard, Gauvin, & Raine, 2011). For example, Kegler et al. (2015) conducted an intervention targeting organizational, community, and political levels of influence to prevent stroke and cardiovascular disease. Furthermore, Golden, McLeroy, Green, Earp, and Lieberman (2015) offer an “inside-out” adaptation of the social ecological model that illustrates how organizational-, community-, and political-level interventions produce change. These researchers provide examples of multilevel research and theoretical frameworks to guide research; however, they do not present models with hypotheses that can be tested empirically (Kelly, 2006; Weiner, Lewis, Clauser, & Stitzenberg, 2012). Furthermore, they do not provide specific guidance on how to combine intervention activities to yield the greatest multilevel intervention effects (Weiner et al., 2012).
Because intervening at more levels does not necessarily mean the intervention will have a greater impact, it is important to combine interventions at different levels in a way that produces complementary or synergistic effects. Weiner et al. (2012) presented five testable strategies for combining interventions to produce synergistic effects: accumulation, amplification, facilitation, cascade, and convergence. With the accumulation strategy, each intervention level has a separate and independent impact on the outcome. With the amplification strategy, the impact of one or more intervention levels is dependent on another intervention level, with one intervention making the target more receptive to the other intervention. The facilitation strategy is similar to amplification strategy in that one or more intervention levels is dependent on another; but, instead of heightening its influence, the conditional intervention simply clears the pathway for the other intervention to make its impact. With the cascade strategy, the outputs of one intervention become the inputs of the next intervention. The convergence strategy uses intervention strategies at different levels of influence that reinforce each other by changing patterns of interaction among two or more intervention levels or targets, such as patients, health care providers, health systems, and communities. This particular strategy matched the Alliance approach (see Figure 1 for an example of the convergence strategy). The researcher selects a specific strategy based on research and/or theory related to the topic under investigation.
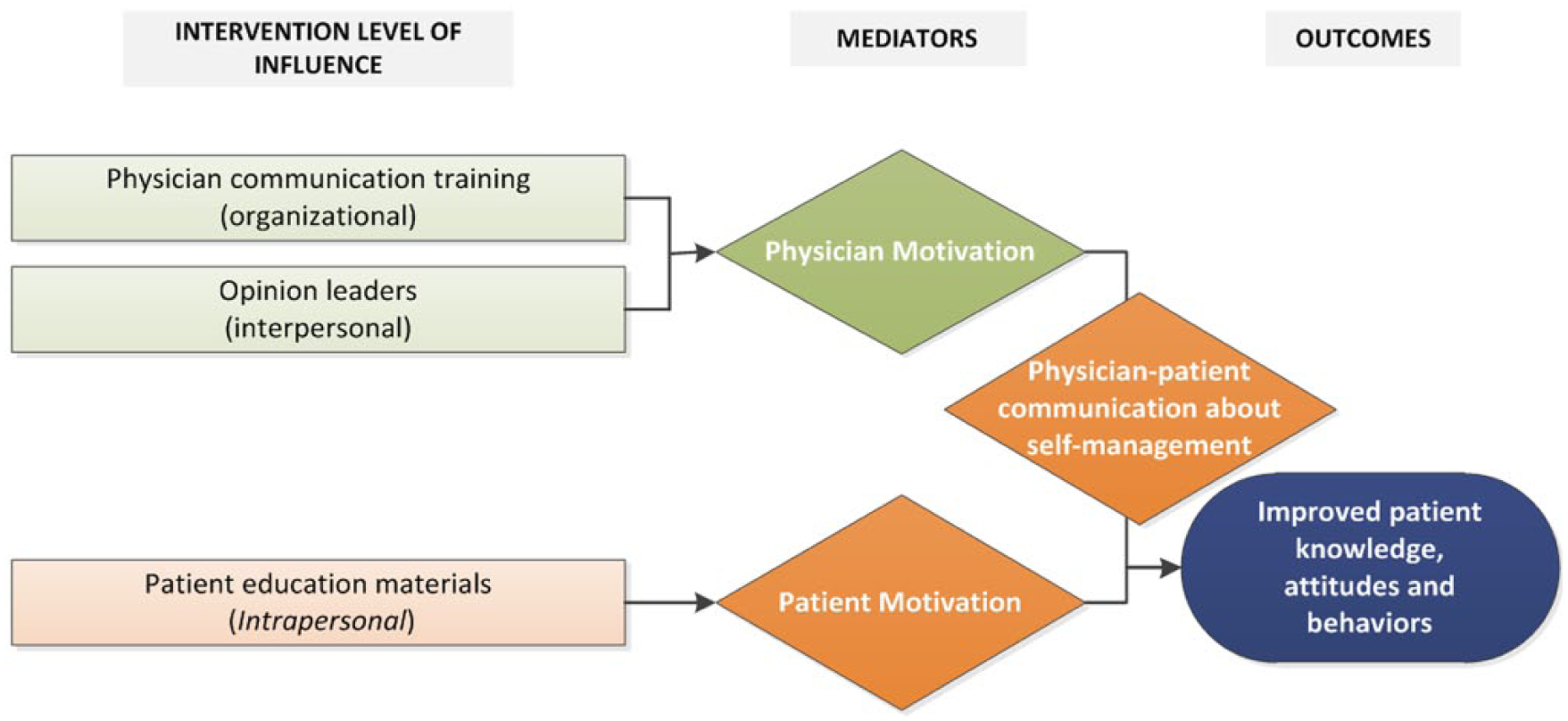
General illustration of the convergence strategy.
A commonly used framework to guide health interventions that mirrors the convergence strategy is the Chronic Care Model (Coleman, Austin, Brach, & Wagner, 2009). It posits that combining patient-centered interactions between informed, activated patients and families (e.g., individual-level intervention) with a prepared, proactive practice team (e.g., interpersonal-level and organizational-level intervention) leads to improved health outcomes. Although this framework is suggestive of the importance of these levels, it does not provide a testable conceptual model that can help explain how interventions at these levels interact to produce health and well-being. Researchers need practical examples of how the social ecological perspective can be used to yield the greatest effects.
To fill this gap, we illustrate how the convergence strategy was used drawing from multilevel interventions implemented as part of the Alliance to Reduce Disparities in Diabetes (The Alliance). The Alliance comprised five sites across the United States that used multilevel, multicomponent programs in 47 clinics to improve health outcomes and reduce health care disparities for type 2 diabetes (Clark et al., 2011). Although the specific content of the interventions varied across the programs, each intervention focused on three core components: patient change, clinician change, and system change. The Alliance used the Chronic Care Model (Coleman et al., 2009) as a guiding framework but did not prescribe the intervention levels or strategies to be used. Instead, each of the five Alliance sites embraced unique strategies to best serve its priority populations and communities, including use of (1) clinical champions who advocated for practice changes that enhanced health care quality, patient care, and systems redesign; (2) partnerships with health care systems to share information and better identify high-risk patients; (3) faith-based outreach and faith leaders who engaged their communities to address diabetes care; (4) cross-community coalitions that united community members and patients at risk for diabetes and advocated for cultural change; and (5) a unified vast network of volunteer physicians to provide free care to community members and patients in need.
A longitudinal observational quantitative cross-site evaluation showed that these programs significantly improved participants’ health behaviors and clinical outcomes; namely, diabetes competence, self-management behaviors, quality of life, hemoglobin A1c, and blood pressure (Lewis, Bann, et al., 2014). The current analysis extends our previous analysis of these programs that showed how sites successfully implemented diabetes self-management programs (Lewis, Williams, et al., 2014) and how they embedded and expanded program features to foster sustainability in health care coordination (Fitzgerald et al., 2016). This article further describes how the grantees successfully combined multilevel interventions using the convergence strategy and explains how they executed the strategy, typically targeting three or four levels of influence, as well as how the interactions in the multilevel interventions were beneficial.
Method
We interviewed Alliance program representatives at five grantee sites across the United States and identified themes within these interviews. The five Alliance grantees included (1) Improving Diabetes Care and Outcomes on the South Side of Chicago, University of Chicago, Chicago, Illinois; (2) Camden Citywide Diabetes Collaborative, Camden, New Jersey; (3) Diabetes for Life Program, Memphis, Tennessee; (4) Reducing Diabetes Disparities in American Indian Communities, Wind River Indian Reservation, Wyoming; and (5) The Diabetes Equity Project, Dallas, Texas.
Procedure
We conducted three site visits, corresponding with the beginning, middle, and end of the 5-year initiative. We interviewed and audio-recorded 65 representatives during 97 interviews, with some being interviewed more than once. Representatives included chief executive officers (CEOs), medical directors, principal investigators (PIs), project managers, clinicians, allied health professionals, and other essential project team members (Lewis, Bann et al., 2014; Table 1; see Lewis, Williams, et al., 2014, for a detailed description of the study procedures).
Overview of Framework Analysis, Approach, and Application.
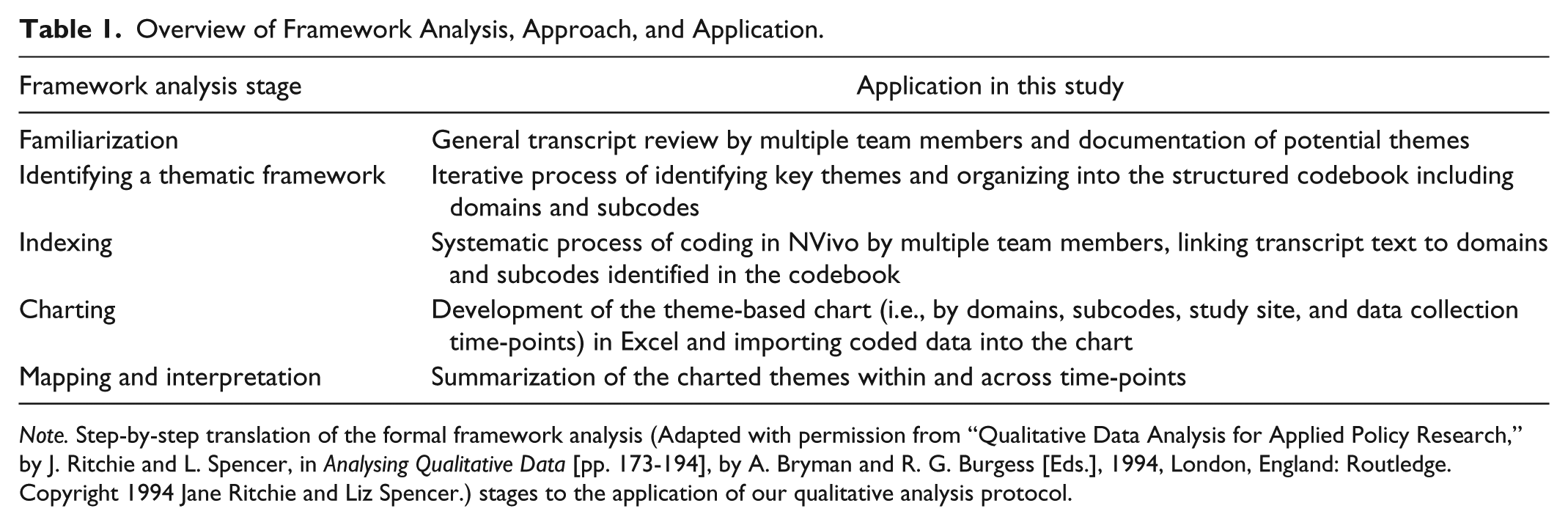
Note. Step-by-step translation of the formal framework analysis (Adapted with permission from “Qualitative Data Analysis for Applied Policy Research,” by J. Ritchie and L. Spencer, in Analysing Qualitative Data [pp. 173-194], by A. Bryman and R. G. Burgess [Eds.], 1994, London, England: Routledge. Copyright 1994 Jane Ritchie and Liz Spencer.) stages to the application of our qualitative analysis protocol.
Two-person teams used semistructured interviews to gather multiple perspectives on program implementation. Interview length varied from 30 to 90 minutes. Topics discussed included program implementation, program reach, perceived effectiveness, barriers and facilitators experienced by programs, partnerships, sustainability, and lessons learned. Sample questions specific to gathering feedback regarding implementation of the Alliance multilevel intervention included the following:
What are the challenges to implementing interventions at multiple levels? How have you resolved them? PROBES: What facilitates implementing interventions at multiple levels? What are the opportunities afforded by implementing interventions at multiple levels?
How would you say the patient, provider, system (and community, if applicable) components fit together in your program to produce better care and reduce disparities? PROBE: Were components implemented all at once, or sequenced differently during implementation?
Our institutional review board reviewed and approved this research.
Data Analysis
We transcribed the audio-recorded interviews and loaded them into NVivo 10.0 for qualitative analysis. As the foundation for the analysis, we used a qualitative framework analysis method (Ritchie & Spencer, 1994) that provides a systematic, five-stage approach to coding, analyzing, and interpreting qualitative data. Lewis, Williams, et al. (2014) describe this approach in detail, and Table 1 provides a simplified overview of how we applied this method to our study.
Ultimately, we defined themes as the same salient idea echoed by multiple interviewees, both within the same program and across sites, as well as over time. We specifically examined data for thematic references that seemed to invoke the integration of multiple levels when describing program functioning or how program outcomes were affected. We also provide supporting quotes from representatives in a variety of roles across the programs to illustrate themes.
Results
Three themes described the synergy between these multilevel, multicomponent programs and were congruent with the convergence strategy across the program sites: (1) enhancing patient and provider engagement and access to quality care; (2) facilitating communication, information sharing, and coordination among providers, community stakeholders, and health systems; and (3) building relationships and fostering alignment among providers, community stakeholders, and systems (Figure 2, column 2). Programs achieved these synergies by using a variety of specific intervention strategies that ultimately helped improve clinical outcomes, increase multilevel engagement, and create greater interdependence that helped facilitate program success (Figure 2, column 1).
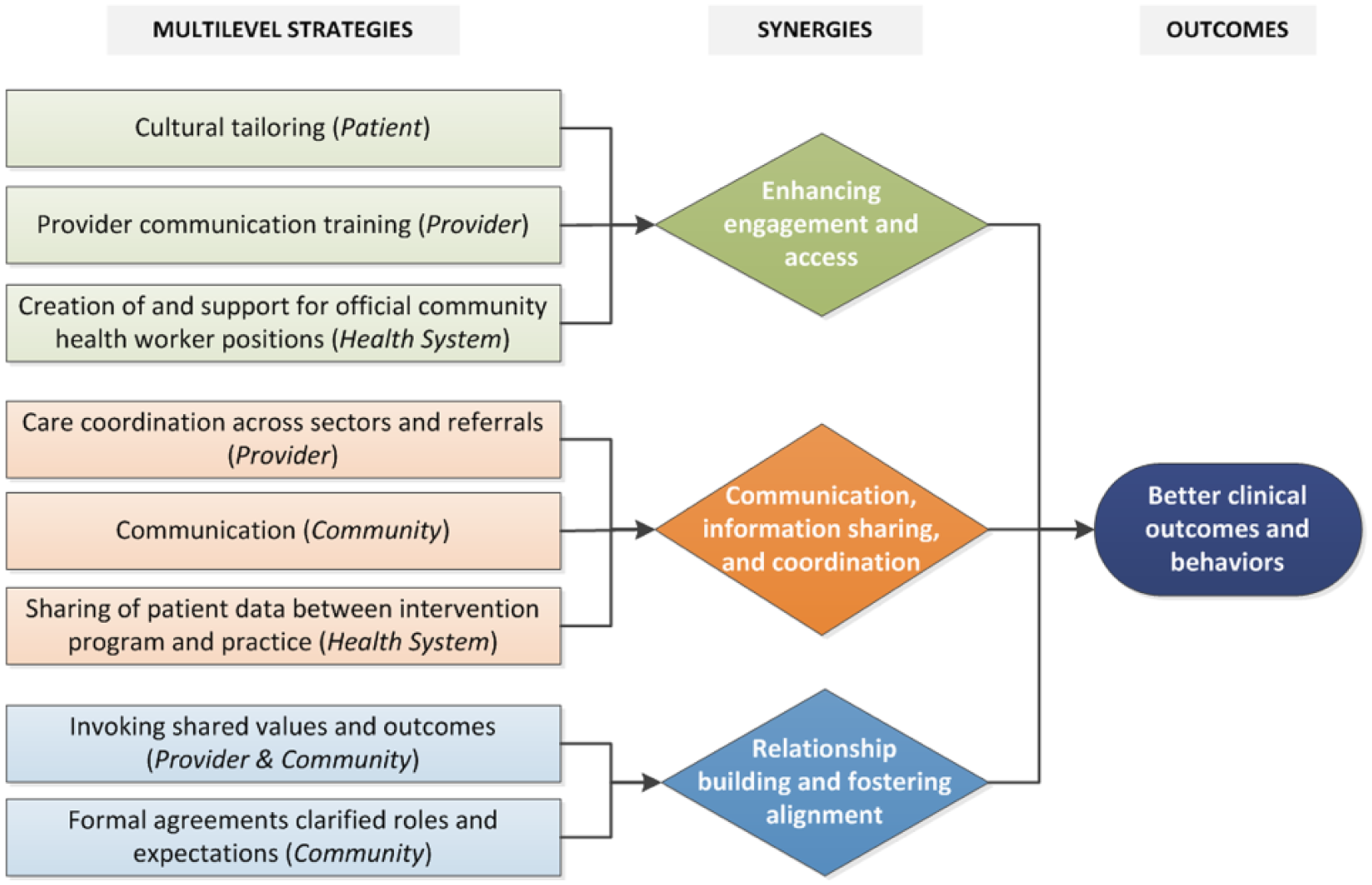
Illustration of how the Alliance grantees combined and executed multilevel interventions using the convergence strategy, targeting multiple levels of influence, which resulted in beneficial outcomes.
Enhancing Patient and Provider Engagement and Access to Quality Care
Three intervention strategies emerged as essential to enhancing patient and provider engagement and increasing access to care: cultural tailoring for patients, provider communication training, and health system support for community health workers (CHWs).
Patients enrolled in the Alliance programs represented diverse communities, including African American, Hispanic/Latino, and Native American. Consequently, each program observed unique cultures and traditions that had an impact on patient interactions with the health care system and providers, and the ability of patients to integrate diabetes management practices into their daily lives. To address these needs, programs adapted health messages and materials to each patient community (Lewis, Williams, et al., 2014). Culturally adapted messages facilitated increased patient empowerment, engaged patients with relatable intervention materials, integrated the teachings into patients’ daily lives, and facilitated patient adherence and self-management. In this regard, two representatives noted the following: [P]eople are learning how to manage their own diabetes. . . . [W]hen they go into their physicians or into their primary care people, . . . they go in with questions that are pertinent to their diabetes and not just saying, “Yes, yes, yes.” (Diabetes Educator, Round 3) And so that was an additional way to teach patients about nutrition. It’s a really neat class, it’s put on by the. . . . Food Bank and it’s led by a nutritionist and a chef and they teach culturally, like relevant, . . . typical foods but in a healthy format and on a budget. (Project Coordinator, Round 3)
Patient–provider relationships were also strengthened through more effective communication and collaborative care planning (Fitzgerald et al., 2016). For example, to make explicit the information patients were receiving and ways in which providers could support and engage patients more effectively, programs offered provider communication training about shared decision-making materials for patients. Programs also worked extensively to engage providers to ensure that they were fully informed about patients’ Diabetes Self-Management Education classes and their progress, and providers were encouraged to initiate a dialogue with patients about the program. Two representatives conveyed the following: Thanks to that now I’m more focused on . . . what the patient is going through in their house instead of just the numbers, thanks to that training . . . it’s easier for me to ask them questions about what’s going on with their life. (Allied Health Professional, Round 1) [T]here’s a couple things that we do that sort of get physicians more ready for the patients. So we tell them that their patients are enrolled in the first place so it’s not a surprise. We ask them to encourage their patients, . . . we’re sort of trying to open and close that loop so people know that their doctors are happy about it. . . . We ask the doctors if they can to stop by the classes, just stop in, wave, give a shout-out so it’ll get people, “Oh, that’s my doctor and he’s happy I’m here!” So again, trying to align as much as possible the patient experience or the provider experience just around that communication training. (Co-PI, Round 2)
CHWs—also referred to as diabetes educators or diabetes health promoters in some programs—were introduced and meaningfully integrated into care teams, as evidenced by health care system support for these team members, including intensive training and certification, formalized supervision, and the establishment of formal CHW job codes for reimbursement of time with patients (Fitzgerald et al., 2016). Introducing trained and “validated” CHWs into clinics and the community alleviated some of the burden of care on providers and enhanced professional trust between health care team members. Ultimately, reinforcing the health care team with CHWs enhanced patients’ experiences through more personalized, in-depth care from health care providers and an enriched medical encounter. One representative’s comment on how these clinician extenders fostered collaboration and supported the health system included the following: The practice has been able to work directly with certified diabetes educators and that link and collaboration back and forth, it’s become a much more close looped system. It’s not this . . . nebulous place where they go [for diabetes education] and then they come back and there’s no records of what happened there. . . . It’s really communicative between the diabetes educator and the practice and we’re very aware as a practice of what patients’ goals are. (Clinician, Round 3)
Communication, Coordination, and Information Sharing Among Community Stakeholders, Providers, and Health Systems
Program synergy around communication, coordination, and information sharing between various health care team members and organizations relied on three key strategies: conversations with community stakeholders, provider care coordination, and information sharing between the intervention program and provider practices.
Regular communication with community stakeholders—such as community centers, food pantries, churches, pharmacies, grocery stores, and fitness centers—included discussing the recruitment and enrollment of patients and provider partnerships (i.e., to help develop appropriate and effective approaches for each unique group), creating marketing opportunities around program and community events, identifying patient resources (e.g., available fresh fruits and vegetables, exercise facilities, vision screening), disseminating educational materials, and generating unique opportunities for collaboration. Positive outcomes from regular, collaborative dialogue with community partners included heightened engagement in program implementation and outcomes and providing opportunities to generate new ideas and realistic solutions to complex challenges, as well as opportunities for reciprocal learning, as indicated by these participant comments.
I think it’s a tremendous value because what happens is that you get a better buy-in. You also get, it’s going to make better inroads into the community. . . . I think it gives it legitimacy and gives you the inroads into other settings that you might not have or you might not have even thought of. (Community Partner, Round 1) [T]he multifaceted nature and the creative ways that we’re trying to build these partnerships allows us to take really somewhat intractable problems and start chipping away at them with solutions that are realistic for the people that need to take them on. (Program Manager, Round 2)
Care coordination, the deliberate and strategic approach to collaborative patient care by multidisciplinary health care teams, consisted largely of four elements: clinic–community collaboration, integration of CHWs, sharing of electronic data, and provider buy-in (Fitzgerald et al., 2016). Care coordination served to reduce provider burden, improve referral processes and rates, and enhance the patient experience with higher quality interactions with their health care team. One participant shared the following: So the care management meeting is actually a meeting that consists of social workers and providers and other professionals across the healthcare system here, ranging from home health aides to nursing homes to the hospital. So they all come together once a month and they discuss specific cases where they think that a patient could benefit from a variety of those services . . . (Project Coordinator, Round 2)
The exchange of patient information between the program and practices facilitated comprehensive understanding of patients’ histories and needs, and helped identify high-need patients who require more attention and intensive education. Communication and coordination were fostered by making health care systems changes—for example, using electronic medical records (EMRs), providing health information exchanges, developing registries, or defining clear roles and responsibilities in multidisciplinary health care teams. These system changes helped to support and coordinate care, as noted by the following representatives: I have very seldom seen a coalition that was as active or as engaged in sharing information, sharing resources, really working together to try to institutionalize a system of care . . . where people share information and work with each other and are always looking forward to how they can continually be improving the system. (Evaluator, Round 2) It’s such a seamless and easy way for providers to access patient data, you know, and have a better picture of their patient’s health. They, through their EMR, won’t know whether or not their patient went to three hospitals, you know, so this health information exchange serves that need and it’s real time data. They don’t have to wait for the fax of the discharge summary when a patient is discharged from the hospital. (Co-PI, Round 3)
Relationship Building and Fostering Alignment Among Providers, Community Stakeholders, and Health Systems
Programs reported multilevel synergy around relationship building and fostering alignment among providers, community stakeholders, and health systems through multiple strategies, including invoking shared values with provider and community partners and enacting formal business agreements.
Invoking shared values nurtured the establishment of meaningful and effective relationships, created interdependent outcomes, fostered respect among key stakeholders, and enhanced reciprocity. Developing businesslike relationships through formal agreements and crystalizing partner roles and expectations helped community partners more clearly understand the potential benefit of being involved with the program. By developing formal agreements, providers were better able to depend on partner contributions to their program to engage patients; for example, providers could prescribe fruits and vegetables that could be purchased from local community partners. Building relationships with community partners helped to extend program benefits beyond the clinic setting and to create a synergistic effect by making it possible for providers’ messages and program teachings for patients about healthy living to be applied in daily life and in the community. Partners were able to understand the potential benefit of participation and felt valued, rather than exploited, for resources. This had the beneficial effect of linking the program’s clinical and community components, as indicated by the following representatives: Everybody has their place and it has to work like a big wheel. Nobody oversteps their boundaries, everybody’s working as a team. You know, it’s not just one person trying to take care of a client, it’s multiple people and being able to network on that same level. You kind of pass that client off to one another and knowing that you can rely on the other person’s going to take care of them in their specialty field. (Program Coordinator, Round 2) I think the magic sauce for our project is the principle of reciprocity, which is that I’m not just taking from you as a partner, I’m giving to you as well, and it’s not just always money. So the value proposition’s got to go both directions and you’ve got to be clear, you’ve got to be able to clearly define what those are. (PI, Round 3)
Grantees allowed clinics to tailor the implementation of particular program components to better reflect shared values and meet local clinic needs. This resulted in clinics being better able to implement programs that matched their organizational structures, policies, and procedures. This process fostered inclusion, acknowledged that busy clinics had multiple obligations, and helped build respect, as shown by the following participant’s comment: I think that’s what made it so magical for us, is the grant request fit close to what we were already doing and we were already in motion around that. . . . It was just a very small scale that would never have got to the scale we achieved without the external funding. And so it was . . . a good marriage between those two. (PI, Round 3)
Grantees worked hard to integrate and align programs by instituting policies and procedures that supported program implementation. They also made program functioning consistent and mutually reinforcing with larger organizational values and structures in which the programs operated, as reflected by the following representative’s comments: There needs to be some shared responsibility, and it could be coupled with creating some kind of incentive to get people more engaged in trying to be successful with achieving certain . . . clinical outcomes. But I think there has to be a system kind of approach to share the responsibility. (CEO, Round 2)
Discussion
This article identifies a testable model, the convergence strategy, as one approach for successfully combining multilevel interventions, and specific intervention strategies used at each level to promote better diabetes care in communities and clinical contexts. Currently, there is a paucity of information in the literature on how interventions can be combined to produce synergies across levels. Social ecological models (McLeroy et al., 1988; Stokols, 1992; Stokols et al., 1996) and the Chronic Care Model (Coleman et al., 2009), which emphasize the importance of using multilevel interventions to produce effects, do not provide testable models. The strategies implemented by grantees throughout the initiative validated the convergence strategy proposed by Weiner et al. (2012) and may explain how the sites achieved the significant clinical and patient-reported outcomes (Lewis, Bann, et al., 2014). Our work extends the Chronic Care Model by demonstrating how multilevel interventions produce synergistic effects to affect health and well-being. Our findings suggest that the convergence strategy may be a fruitful way to intentionally design and plan multilevel interventions.
The three key synergies that contributed to the success of the Alliance—engagement and access; communication, information sharing, and coordination; and relationship building and fostering alignment—have also been proposed as important in managing other chronic health conditions and initiatives across health care. Because of this greater application, engagement and access are recurring intervention targets in care improvement and access initiatives. For example, The Affordable Care Act of 2010 (ACA) recognizes patient engagement as an evidence-based strategy for improving health outcomes and care experiences and for lowering costs for patients across chronic care conditions (Hibbard & Greene, 2013).
Engagement and access are also shown to be important in managing other chronic health conditions, such as HIV infection (Cheever, 2007; Galvan, Bing, & Bluthenthal, 2000; Gardner, McLees, Steiner, del Rio, & Burman, 2011; Girardi, Sabin, & Monforte, 2007; Mugavero, Amico, Horn, & Thompson, 2013). Increasing focus is being directed to interventions to improve engagement of people living with HIV at every step of the HIV care continuum to increase testing uptake, retention in care, and viral suppression (Gardner et al., 2011; Girardi et al., 2007).
Communicating with community stakeholders, care coordination, and information sharing have been implemented in other initiatives across a spectrum of health conditions as well. For example, enhanced care coordination has been shown to improve outcomes for numerous chronic conditions, including depression, heart disease (McDonald et al., 2007), and diabetes (Haw, Venkat Narayan, & Ali, 2015; Stellefson, Dipnarine, & Stopka, 2013). The importance of care coordination as a key strategy for improving the quality and efficiency of health care in the United States is evidenced by the financial incentives for care coordination efforts included in payment reforms related to the ACA (Corrigan & Adams, 2003; Farrell et al., 2015) and the patient-centered medical home model (Davis, Schoenbaum, & Audet, 2005; Rittenhouse & Shortell, 2009), which has been connected to improved quality and clinical indicators (Bojadzievski & Gabbay, 2011).
Formal agreements clarifying roles and expectations and invoking shared values and outcomes constituted the third synergy of the Alliance around relationship building and fostering alignment. Improvements to the U.S. health care system will require alignment of representatives at all levels of the system (Ferlie & Shortell, 2001), especially as the ACA becomes more widely accepted and implemented. Benefits of partnerships include innovation, engagement of community stakeholders, multidisciplinary services, and multilevel interventions (Lasker, Weiss, & Miller, 2001).
Collaboration between stakeholders is a key feature of many multilevel initiatives to improve patient outcomes and health care delivery, including in the Alliance. Analysis of six sites in the Robert Wood Johnson Foundation’s Aligning Forces for Quality initiative underscored the importance of building consensus around goals, leadership, and trust between members (Hearld, Alexander, Beich, Mittler, & O’Hora, 2012). Furthermore, the Colon Health Program of Greater Seattle expanded access to colorectal screening, improved completion and follow-up rates, and secured funding to continue the program in the state of Washington (Phillips-Angeles et al., 2013) by building commitments, collaboration, and trust; and invoking shared values.
This article highlights the strategies used at different levels of the social ecological framework to address diabetes self-management. Developing and testing multilevel interventions is a complex endeavor. Our article contributes to this area by demonstrating how the convergence strategy can be used to conduct these types of interventions. In addition, it highlights specific intervention components that when used in combination may create synergy when different levels are targeted for change. To design multilevel interventions, a thorough understanding of epidemiology, barriers to change at targeted levels, and empirical support for intervention approaches can lead to “high-leverage” intervention approaches (Stokols, 1992; Weiner et al., 2012). In addition, combining this knowledge with the use of intervention planning approaches such as PRECEDE–PROCEED (Green & Kreuter, 2005) and intervention mapping (Bartholomew, 2006) can increase the effectiveness of a systematic and effective intervention approach. Documenting the development, implementation, and impact of these types of interventions will help advance our understanding of complex intervention development. Evaluations that include both a well-developed descriptive approach, such as the one used here, to supplement outcome and impact evaluations will contribute to our understanding of how these complex interventions have their effects.
Limitations
We used a post hoc analysis to map the multilevel approach across sites to a convergence model that identifies potentially synergistic effects of multilevel programs. Our main focus was on understanding the perspective of program implementers rather than patients who benefited from these programs, although we recognize that the perspectives of patients are important (Scholle, Torda, Peikes, Han, & Genevro, 2010). The data included individual-level interventions in our description of the programs, but the input on these were provided by program implementers. Additionally, this research occurred as part of a broader examination of changes in diabetes health care disparities via the Alliance programs; consequently, the application to other chronic health conditions is not entirely clear. Using testable multilevel conceptual models prospectively will further advance this area of research.
Conclusion
As interventions grow in complexity to address challenging health and social problems, multilevel interventions need testable models to advance research and practice. The social ecological perspective provides a broad framework for understanding determinants of health problems at multiple levels of analysis, but it does not indicate how these levels should be combined to produce the greatest effects. This article points to one strategy for moving forward by demonstrating an approach for interventions addressing type 2 diabetes that suggests the importance of using a convergence approach to guide multilevel interventions. The approach could apply to the management of other chronic illnesses as well. Future research needs to examine the combination of processes that may account for significant intervention effects in other health programs and contexts.
Footnotes
Acknowledgements
We would like to thank the organizations involved in the Alliance to Reduce Disparities in Diabetes, the grantees, and their program staff who participated in interviews, the National Program Office representatives, and the Merck Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for the research and authorship of this article was funded by the Merck Foundation.