
Abstract
This study is the first to analyze public response to a drug take-back program, the American Medicine Chest Challenge, in a single state over a period of 3 years (2010-2012). The study utilized a three-wave repeated cross-sectional design and an annual phone survey conducted with a representative sample of adults (N = 906 in 2010, N = 907 in 2011, and N = 906 in 2012), which assessed exposure to the campaign, drug disposal behaviors, possible mediators of campaign effects (risk appraisal, personal agency, normative influence, and interpersonal talk), and potential confounders. Logistic regression and causal mediation analysis were employed to estimate confounder-adjusted direct and mediated effects of the campaign. Results showed that the campaign reached a sizable portion (50% to 60%) of state adults and that campaign exposure was associated with increased likelihood of having conversations with others about this topic. About 55% of all adults in the state reported taking at least one of the actions recommended by the campaign, and campaign exposure was associated with increased likelihood of disposing of prescription drugs at a drug collection day event (adjusted odds ratio = 4) and of talking to a child about the risks associated with prescription drug abuse (adjusted odds ratio = 2). The causal mediation analysis demonstrated that the campaign influenced audiences by reinforcing their efficacy to safely dispose of prescription drugs, but also potentially by stimulating conversations among community members about this topic. Drug take-back campaigns can be an effective mechanism to decrease the availability of prescription drugs in communities.
Keywords
The misuse and abuse of prescription drugs continue to pose a serious public health problem in the United States (Nielsen & Weiss, 2015). Although most people take prescription medications responsibly, the most recent estimates indicate that about 15 million people aged 12 years or older used prescription drugs nonmedically in the past year (Substance Abuse and Mental Health Services Administration, 2015). Major health risks associated with prescription drug abuse include fatal and nonfatal overdosing and drug addiction (Nielsen & Weiss, 2015). Prescription drug abuse is also increasingly burdening the health care system, with treatment admissions for misuse or abuse of prescription opioids alone increasing more than fivefold since 2000 (Calcaterra, Glanz, & Binswanger, 2013).
Easy access to prescription drugs is a major factor contributing to this epidemic (Johnston, O’Malley, Miech, Bachman, & Schulenberg, 2015; McCabe, Boyd, Cranford, & Teter, 2009; Office of National Drug Control Policy [ONDCP], 2014), and public health response to it draws on the combination of four primary strategies: educating patients and health care providers about the risks of misusing prescription drugs, supporting the expansion of state-based prescription drug monitoring programs, reducing prescription drug diversion to unauthorized users through targeted enforcement efforts, and developing more convenient and environmentally responsible disposal methods to remove unused medications from the home (ONDCP, 2014). Within this prevention framework, prescription drug take-back programs are seen as potentially effective and safe means of decreasing the availability of expired, unwanted, or unused (EUU) prescription medicine in communities nationwide (ONDCP, 2014; Stergachis, 2014). However, with very few exceptions (e.g., Gray, Hagemeier, Brooks, & Alamian, 2015; Stewart et al., 2015), public participation in such programs and events has not been systematically assessed, and what is known is limited to the types and quantities of drugs collected in a single collection event. This study assessed and analyzed public response to a campaign promoting a drug take-back and disposal program, the American Medicine Chest Challenge (AMCC), in a single state (New Jersey) over the first 3 years of implementation (2010-2012).
The American Medicine Chest Challenge
The AMCC is an ongoing community-based public health initiative designed to raise awareness about the dangers of prescription drug abuse and host a drug collection day event held in November each year in many communities. Nationwide, AMCC currently has more than 2,000 official collection sites set up by more than 1,000 community and law enforcement partners. The AMCC public campaign invites adults and families to participate in AMCC’s Five-Step Challenge: (a) taking inventory of the medicine stored at home, (b) locking their medicine cabinet, (c) safely disposing of EUU medicine in their home or at an authorized drug collection site, (d) taking their medicine(s) exactly as prescribed, and (e) talking to their children about the dangers posed by prescription drugs. AMCC’s prevention strategy can be generally described as community-based prevention marketing (Bryant et al., 2007) and is focused on building a coalition of law enforcement, government, nonprofit, media, and corporate partners in each of the communities they serve, with each partner providing specialized knowledge or resources that can be leveraged to support the community effort. The AMCC communication campaign aims to increase public awareness to the prescription drug abuse problem and to promote the safe disposal of EUU prescription medicine stored at home.
Since its inception in 2010, AMCC was able to collect several tons of prescription drugs nationwide (Partnership for Drug-Free New Jersey, 2013), but the scope and nature of the influence the campaign had on audiences beyond participation in drug take-back events is largely unknown. In theory, the campaign may have encouraged individuals and families to dispose of EUU prescription medicine stored in their home in several different ways: (a) by influencing their perceived severity of the risk posed by storing EUU medicine and their perceived susceptibility to that risk (Janz & Becker, 1984); (b) by instilling a sense of personal agency—whether self-efficacy (Bandura, 1986) or response efficacy (the belief that a particular action is effective; Witte, 1992, 1994)—regarding the actions recommended to the public; or (c) by leading individuals to believe that disposal of prescription drugs is the norm in their community (Fishbein & Ajzen, 2010; Rimal & Real, 2005). It may also be that the campaign influenced actions indirectly, by stimulating conversations among members on this topic, which in turn caused them to reflect on their own behavior (Southwell & Yzer, 2009).
Method
Procedure and Sample
The goal of this study was to estimate the population-level reach and influence of the AMCC campaign in the state of New Jersey by analyzing survey data collected from a representative sample of adults in the state in December of each of the first 3 years of AMCC (2010-2012), approximately a month post the annual drug take-back event. The telephone interviews were conducted by landline or cellphone with a scientifically selected random sample of adults in the state by the Eagleton Center for Public Interest Polling under protocols approved by Rutgers University’s institutional review board. For eligible respondents with which contact was established, response rates for all three surveys ranged from 20% to 22%, and the refusal rate ranged from 31% to 33%, yielding the final sample of respondents for the purposes of analysis (N = 906 in 2010, N = 907 in 2011, and N = 906 in 2012). Sampling weights were used in all analyses to minimize potential bias in estimates of variables and associations of interest.
Variables and Measures
Campaign Exposure
The degree to which respondents previously saw or heard information in the media concerning the prescription drug abuse problem was assessed with a single Likert-type scale item (ranging from never to at least daily), and a similar additional item assessed the frequency in which they recalled seeing or hearing AMCC-sponsored messages in the past 30 days. Respondents were also asked about the number of conversations, if any, they had with other adults in the past month about EUU medicine disposal. To assess audience processing of the information provided by the campaign, only respondents who reported being exposed to information about the AMCC were asked to assess (on a 5-point scale ranging from none to a great deal) the degree to which they (a) learned about how to safely dispose of EUU medicine in their home from this information and (b) were influenced by this information to take action.
Cognitive Mediators
All respondents (exposed and unexposed) were asked a set of five Likert-type scale items (ranging from strongly disagree to strongly agree) measuring cognitions that would be theoretically expected to change in response to the campaign. Two measured respondents’ perceived severity (“using or sharing prescription medicine that was prescribed to someone else is dangerous”) and perceived susceptibility (“I am concerned about other members of my household using and sharing prescription and over-the-counter medicine that was not prescribed to them”) regarding the risks posed to self or family from EUU prescription medicine stored at home, and a perceived threat score was calculated for each respondent by multiplying the responses to these two items. It is worth noting that whereas perceived susceptibility is typically measured by asking about one’s probability of experiencing a certain risk or adverse outcome (Rosenstock, Strecher, & Becker, 1994), the measurement of the construct in this study was based on assessing degree of concern or anxiety regarding the risk (see Champion, 1984) because the likelihood of action in this case is greater when the subjective evaluation of risk is affect-based (e.g., experiencing fear) rather than based on logical (and often, overly optimistic) evaluation of odds (Witte, 1992, 1994). The third item assessed respondents’ self-efficacy to safely dispose of EUU medicine (“I am confident that I know how to safely dispose of unused, unwanted, and expired medicine I have in home”), and the fourth their degree of response efficacy (“I believe that my personally disposing of unused, unwanted, and expired medicine in my household can prevent the misuse and abuse of these medications by someone else”). The fifth item measured respondents’ perception that most people important to them expect them to dispose of EUU drugs stored in their home.
EUU Drug–Related Behaviors
All respondents were also asked about the following actions they may or may not have taken in the past 30 days: (a) taking inventory of medicine stored at home, (b) locking medicine cabinet, (c) disposing of medicine in household trash, (d) participating in the AMCC-sponsored disposal day event, and (e) flushing medicine down a drain. One additional item asked them to report the number of conversations, if any, they had in the past 30 days with their or someone else’s child about the danger of prescription drug abuse.
Confounders
Confounders controlled in all analyses included age, sex, race/ethnicity, level of education, household income, employment status, religiosity, number of children in the household who are below the age of 18 years, having any EUU medicine stored at home (yes/no), and personal knowledge of a person who misused or abused prescription drugs—all of which can potentially account for the self-selection of respondents into the exposure or nonexposure groups as well as influence their drug disposal behaviors. General exposure to information about the prescription drug abuse problem in the media was also included as potential confounder; however, the number of conversations a respondent had with other adults about disposal of EUU medicine was excluded from the confounder pool since this variable may have mediated the effect of campaign exposure on outcomes.
Data Analysis Strategy
Associations between campaign exposure and outcomes were initially assessed separately for each year of the study by comparing the treatment (exposure) and control (nonexposure) groups on cognitive and behavioral outcomes while controlling for confounders. Confounder-adjusted estimates of campaign effects were then generated by means of logistic regression analysis. The final step of the analysis estimated direct and mediated associations between campaign exposure and each outcome of interest by means of causal mediation analysis (Hicks & Tingley, 2011; Wang, Nelson, & Albert, 2013), using the mediation package in Stata version 13 (Hicks & Tingley, 2011; StataCorp, 2013), which estimates the average causal mediation effect (ACME), the average direct effect (ADE), and the average total effect (ATE) with their corresponding 95% bootstrap bias-corrected confidence interval.
Results
Campaign Exposure and Message Evaluation
Table 1 compares the weighted sample characteristics of respondents exposed and unexposed to the AMCC campaign across the 3 years of the study (2010-2012). The percentage of respondents reporting any exposure to the campaign was 60% in 2010, 50% in 2011, and 52% in 2012, with about even distribution of exposed and unexposed respondents across major demographic and other grouping variables in each year. There was however modest positive correlation between campaign exposure and general exposure to information about the prescription drug abuse problem in the media across all three cross-sectional samples (gamma = .29, p < .001).
Weighted Sample Characteristics of Respondents Exposed and Unexposed to the American Medicine Chest Challenge Campaign in New Jersey, 2010 to 2012.

Note. The sampling error for each sample is ±3.3% at a 95% confidence interval. The superscripts a, b, and c indicate a statistically significant (p < .01) test of between-group differences on a particular attribute in 2010, 2011, and 2012, respectively.
In each year (2010-2012), about half of all respondents exposed to the campaign (49%, 46%, and 48%, respectively) indicated that they learned some or a lot about how to safely dispose of EUU medicine from the information provided, but only about one third (29%, 34%, and 31%, respectively) said this information influenced them to safely dispose of medicine. There were no statistically significant differences in the distribution of responses given to these two questions on any of the variables listed in Table 1. Still greater percentages of respondents exposed to the campaign in each year (28.5%, 19%, and 21%, respectively) compared to those of unexposed (13%, 11%, and 11.5%, respectively) reported having at least one conversation in the past month with another person about disposing of EUU medicine, and this difference was statistically significant in all cases (χ2 > 11, df = 1, p < .01). Interpersonal talk may have served as means of further disseminating the messages of the campaign or the exchange of additional relevant information (e.g., advice) that may have motivated action; however, the available data provide no information about the content of conversations respondents had.
Association Between Campaign Exposure and Prescription Drug Disposal Behaviors
In general, between 36% and 42% of all respondents (exposed and unexposed) in each year of the study reported taking inventory of the EUU medicine stored in their home, between 11% and 18% locked their medicine cabinet, between 24% and 30% disposed of EUU medicine in household trash, between 13% and 19% flushed medicine down a drain, and between 10% and 16% utilized the drug collection sites that were set up during the AMCC national collection day event. About 20% of all respondents in each year also reported having one or more conversations with a child in the past month about the dangers of prescription drug abuse. The median number of different recommended actions respondents reported taking in each year ranged from 1.3 to 1.6 actions, with about 40% of respondents reporting taking no actions to dispose of EUU medicine. However, about half of these respondents in each year also reported having no EUU medicine stored at their home. Thus, it appears that the majority (about 80%) of individuals in each year who had EUU medicine stored in their home took at least one action to safeguard or dispose of it.
Table 2 compares the percentage of AMCC-exposed and AMCC-unexposed respondents that performed each recommended action in each year of the study. Overall, there was little change across years in the percentage of respondents within each group of respondents that enacted each recommended preventive action. However, campaign exposure had a statistically significant association only with a respondent’s likelihood of disposing of EUU medicine in an AMCC-sponsored drug collection site and talking to kids about the dangers of prescription drug misuse.
Percentages of Respondents Exposed and Unexposed to the American Medicine Chest Challenge Campaign Reporting Taking Actions to Safeguard and Dispose of Prescription Medicine, New Jersey, 2010 to 2012.
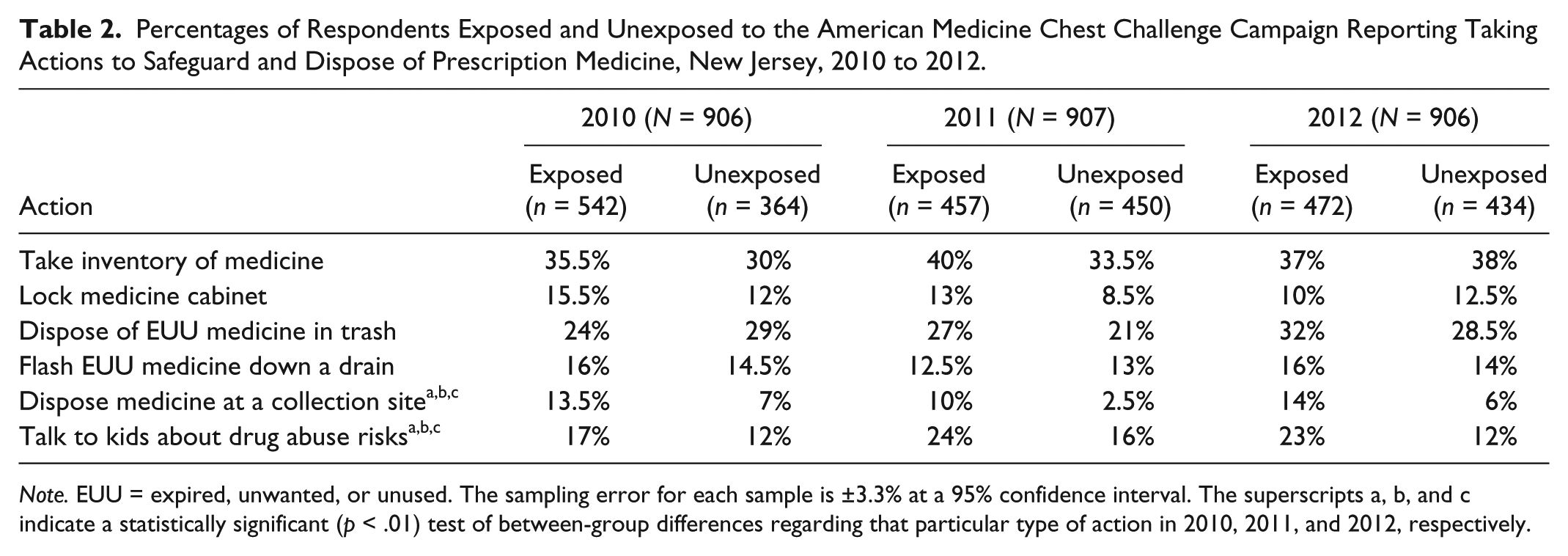
Note. EUU = expired, unwanted, or unused. The sampling error for each sample is ±3.3% at a 95% confidence interval. The superscripts a, b, and c indicate a statistically significant (p < .01) test of between-group differences regarding that particular type of action in 2010, 2011, and 2012, respectively.
Estimates and Pathways of AMCC Campaign Effects
The degree to which exposure to the AMCC campaign independently explained the differential likelihood of respondents to (a) dispose of EUU medicine in a drug collection site, (b) talk to a child about the dangers of prescription drug misuse, and (c) have one or more conversations with others about prescription drug disposal was initially assessed through a series of hierarchical logistic regression analyses. In each model estimated, all potential baseline confounders and all hypothesized cognitive mediators entered the model in Step 1, and AMCC campaign exposure in Step 2, such that estimates of campaign effects were adjusted for the effect of confounders and mediators (see adjusted odds ratios [AOR] in Table 3). Evidence of a statistically significant improvement in model fit (i.e., a significantly smaller 2 lower limit value) with the inclusion of campaign exposure as additional predictor was interpreted to suggest an independent effect of this variable on the outcome modeled. The results summarized in Table 3 show that those exposed to the campaign had more than twice the confounder-adjusted odds of the unexposed to have had one or more conversations with others about prescription drug abuse prevention in each year of the study. They were also more likely to have had at least one conversation with a child about the dangers of prescription drug misuse, and the contribution of campaign exposure to variations on this variable increased in each successive year, from AOR = 1.65 in 2010 to an AOR = 2.7 in 2012. Still the strongest potential effect of exposure to the AMCC campaign was observed regarding respondents’ likelihood of utilizing AMCC-sponsored drug collection site: The exposed had twice (in 2010), four times (in 2011), and three times (in 2012) the confounder-adjusted odds of the unexposed to report disposing of EUU medicine at a collection site.
Logistic Regression Estimates for the Effect of American Medicine Chest Challenge Campaign Exposure on Respondents’ Self-Reported Prescription Drug Abuse Preventive Actions, 2010 to 2012.

Note. AOR = odds ratio adjusted for the effects of sex, age, race/ethnicity, level of education, family income, employment status, religiosity, parental status, general exposure to news about drug abuse, and having expired, unwanted, or unused medicine stored at home; CI = confidence interval.
p < .05. **p < .01.
The results of the causal mediation analysis are summarized in Table 4. This analysis estimated the direct and mediated effects of campaign exposure on the two outcomes previously found to be associated with this variable (i.e., likelihood of disposing of EUU medicine at a drug collection site and likelihood of talking to a child about the dangers of prescription drug misuse). For the purposes of this analysis, data were pooled together across the three annual cross-sectional surveys (N = 2,719) to obtain the statistical power needed to generate unbiased estimates of average total, direct, and indirect campaign effects (Hicks & Tingley, 2011; Wang et al., 2013). First, however, bivariate correlation matrixes were estimated to ensure that suspected mediators were correlated with both campaign exposure and the behavior predicted. The results of this analysis demonstrated that, controlling for confounders, campaign exposure was positively associated with self-efficacy to safely dispose of EUU medicine stored at home (r = .22, p < .001), with response efficacy (r = .20, p < .001), and with having one or more conversations with others regarding the disposal of EUU medicine (r = .11, p < .01). The likelihood of disposing of EUU medicine at a drug collection site was positively associated with self-efficacy to safely dispose of EUU medicine (r = .14, p < .01), response efficacy (r = .18, p < .01), and having one or more conversations with others about EUU medicine disposal (r = .14, p < .01). The likelihood of talking to a child about the dangers of prescription drug abuse was positively associated with response efficacy (r = .10, p < .05) and having one or more conversations with others about EUU medicine disposal (r = .20, p < .01), but not with self-efficacy (as can be expected since the measure utilized was about self-efficacy to safely dispose of medicine and not self-efficacy to talk to a child). Perceived threat had no statistically significant association with campaign exposure and any of the outcomes modeled and this was also true when the same associations were estimated separately for perceived severity and perceived susceptibility. Therefore, the causal mediation models estimated included a direct path and all viable mediated paths from campaign exposure to each of the two behaviors modeled.
Estimated Direct and Indirect Causal Effects (and 95% Bootstrap Bias–Corrected CIs) of American Medicine Chest Challenge Campaign Exposure on the Pooled Sample of Respondents’ (N = 2,719) Self-Reported Prescription Drug Abuse Preventive Actions, 2010 to 2012.
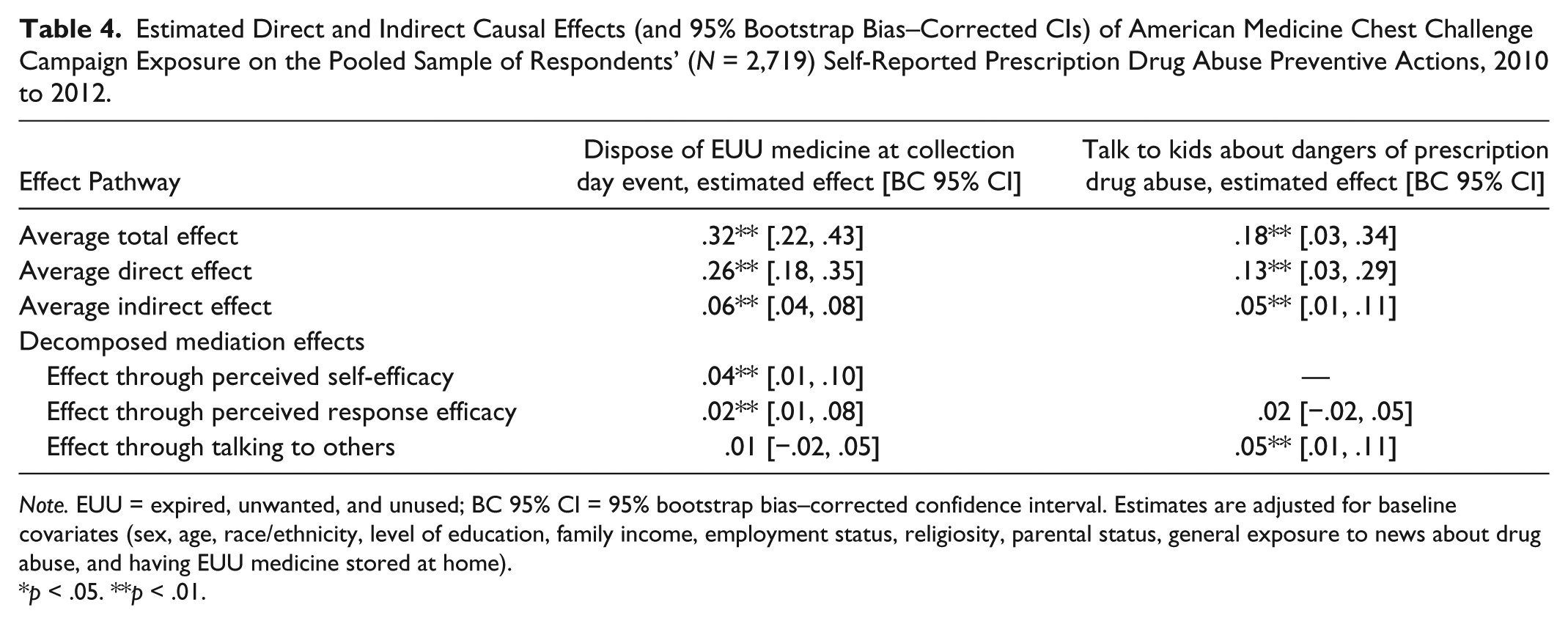
Note. EUU = expired, unwanted, and unused; BC 95% CI = 95% bootstrap bias–corrected confidence interval. Estimates are adjusted for baseline covariates (sex, age, race/ethnicity, level of education, family income, employment status, religiosity, parental status, general exposure to news about drug abuse, and having EUU medicine stored at home).
p < .05. **p < .01.
As shown in Table 4, the estimated ATE of campaign exposure on disposing of EUU medicine at AMCC-sponsored collection site was ATE = .32. This means that campaign exposure increased a person’s probability of enacting this behavior by .32 (or about one-third) on average. The ADE (.26) accounted for 81% of the ATE, and the average causal mediation (or indirect) effect (ACME = .06) accounted for the remaining 19%. The ACME was further decomposed into three plausible paths, and this analysis showed that two of these—the effect mediated through greater perceived self-efficacy to safely dispose of EUU medicine (ACME = .04) and the effect mediated through greater response efficacy (ACME = .02)—fully accounted for the indirect effect of campaign exposure on this variable. Next, the estimated ATE of campaign exposure on a respondent’s likelihood of talking to a child about the dangers of prescription drug misuse (ATE = .18) suggests that exposure to the campaign increased a person’s probability of talking to a child by 18% on average. The ADE (.13) accounted for 72% of the total average effect and the average causal mediation (or indirect) effect (ACME = .05) accounted for the rest. Here too the ACME was further decomposed into two plausible paths, and this analysis showed that only one of these—the effect mediated through having conversations with others about safely disposing of EUU medicine (ACME = .05)—fully accounted for the indirect effect of campaign exposure on this outcome.
Discussion
Prescription drug misuse continues to pose a serious public health problem in the United States, and promoting safe and environmentally responsible disposal of medicine stored at home is seen as an important component of the multipronged national strategy to decrease the availability of prescription drugs for unauthorized or medically unnecessary use (Stergachis, 2014). Many prescription medicines now include specific disposal instructions on their labeling or patient information leaflet that instruct patients on the proper disposal of medications at home—whether flushing them down the sink or toilet or mixing with household trash such as used coffee grounds, dirt, or kitty litter—but community-based drug take-back programs continue to be promoted to the general public as the best option (ONDCP, 2014). This study assessed and analyzed public response to a campaign promoting one such drug take-back and disposal program, the AMCC, in New Jersey between 2010 and 2012.
Overall, the findings reported here demonstrate that the AMCC public communication campaign was able to influence members of the public in New Jersey to safely dispose of EUU medicine stored in their homes during the first 3 years in which the program was operating (2010-2012). During this time, the campaign was able to reach a sizable portion (50% to 60%) of the intended target audience with messages that promoted the safe disposal of prescription drugs stored in homes, and between 20% and 30% of individuals who were exposed to the campaign in each year also engaged in interpersonal conversations on this topic that may help further spread this message. The findings also demonstrate that, in each year, a majority of adults in the state (about 55%) reported taking at least one of the actions recommended by the campaign to safely dispose of EUU medicine stored in their homes, and that exposure to the campaign was a statistically significant predictor of a person’s likelihood of disposing of medicine at a collection day event, as well as the likelihood of talking to children about the risks of misusing prescriptions drugs, even after controlling for likely confounders. On average, individuals exposed to the campaign had more than twice the odds of talking to a child about the risks for prescription drug misuse and up to four times the odds of disposing of prescription drugs at the community drug collection day event.
Still it is not entirely clear how the campaign was able to stimulate this level of public response. The results of the casual mediation analysis hint at the possibility that the campaign contributed positively to increasing people’s sense of personal agency (i.e., self-efficacy and response efficacy) regarding simple actions they can take to protect themselves and their community from the dangers of prescription drug misuse, but the fact that the direct path of effect between campaign exposure and each behavior modeled accounted for much of the observed relationship between these variables suggests that other influence mechanisms, not directly observed in this study, may have been at play. In particular, it seems likely that community participation in efforts to decrease the availability of prescription drugs to potential abuse may be greater when strong social norms that support this practice are visible in the community (e.g., via the information circulating through community channels and events) and when communities organize to enable the behavior (e.g., having multiple collection boxes in the community that are easily accessible to residents year-long). At the individual level, motivation to dispose of medicine stored at home may be undermined by the belief that EUU medicine is good to have around in a case of a health emergency or recurrence of the original condition for which the medicine was prescribed, as well as by the lack of perceived economic incentive to dispose of otherwise costly medication. Future research may be able to generate additional insights regarding the contribution of these and other factors to drug disposal behavior.
It is also important to qualify any conclusions drawn from this study in light of the obvious limitations of the available data—that is, its cross-sectional nature, the limited measurement of key constructs, and the fact that estimates of campaign exposure and behavioral outcomes were limited to past 30 days—which greatly complicate the task of estimating the true effect of the campaign on audiences. At the same time, because data were collected from a representative sample of New Jersey adults at three different time points, and because important confounders were controlled for in all analyses, the general pattern of findings observed in this study is sufficiently robust to alleviate concerns about their potential spuriousness.
From a public health perspective, the results of this study confirm findings of previous studies (Glassmeyer et al., 2009; Gray et al., 2015; Stewart et al., 2015; Yang, Doshi, & Mason, 2015) that drug take-back events are a potentially effective instrument for decreasing the availability of prescription drugs to potential misuse in communities nationwide. At the same time, given that the data analyzed in this study involved self-reports on drug disposal behaviors collected from a representative sample of adults in an entire state, it is possible to begin estimating the nature and scope of drug disposal practices that people enact in their homes. Thus, whereas only 10% to 16% of respondents in each year of the study reported utilizing a drug collection site to dispose of EUU medicine, many others took inventory of medicine at home (36% to 42%), locked their medicine cabinet (11% to 18%), disposed of medicine in household trash (24% to 30%), or flushed medicine down a drain (13% to 19%). These findings underscore the importance of disseminating credible and concrete information to local and national audiences regarding safe prescription drug disposal practices as well as systematically monitoring disposal practices at homes. The results also suggest that successful programs such as AMCC, which integrates a public communication campaign with community-based organizing, could be potentially emulated in other contexts to improve health outcomes for individuals and communities, providing they are properly supported and funded.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.