
Abstract
Background. Parental communication about the importance of reporting concussion symptoms can influence a child’s attitudes about such reporting, and is likely related to perceived threat of concussion. However, parental investment in child sport achievement might impede this communication. Purpose. To examine the relationship between perceived threat of concussion and parent–child communication regarding concussion symptom reporting, and the potential interaction with parental pressure regarding child sport achievement. Method. A total of 236 parents of youth soccer players completed an anonymous online survey. Results. There were greater odds of encouraging concussion reporting among parents who perceived that their child had a greater likelihood of sustaining a concussion (OR = 1.03, 95% CI [1.01, 1.04]) and lower odds among parents who exhibited greater parental sport pressure (OR = 0.88, 95% CI [0.78, 0.99]). Parents whose child had a prior concussion were much more likely to communicate with their child about concussion reporting (OR = 7.86, 95% CI [3.00, 20.55]). Conclusion. Initiatives are needed to support healthy sport parenting, particularly focusing on parental encouragement of concussion reporting. Possible directions for concussion education for parents based on the results of this study include providing parents with concrete guidance about the important role they can play in encouraging their child to report symptoms of a concussion, communicating the athletic consequences of continued sport involvement while experiencing symptoms of a concussion, and using narrative messaging with exemplars to personalize the information for parents of youth who have not previously sustained a concussion.
More than nine million U.S. children and adolescents annually play organized soccer (Malina, 2010; U.S. Soccer, 2015), and soccer involvement is increasingly recognized as having concussion risk. Among high school soccer players, approximately two concussions are diagnosed for every 1,000 exposures to a game or practice (Marar, McIlvain, Fields, & Comstock, 2012; Marshall, Guskiewicz, Shankar, McCrea, & Cantu, 2015), an underestimate of the true incidence as many concussions are not reported or diagnosed (Kerr et al., 2014). While most athletes who sustain a concussion will clinically recover within 2 weeks, during the symptomatic period postconcussion the brain is in a vulnerable state where an additional impact may cause more severe injury (Prins, Alexander, Giza, & Hovda, 2013). Continuing to play while symptomatic has also been associated with prolonged recovery (Asken et al., 2016; Elbin et al., 2016). Thus, ensuring that youth athletes with concussion symptoms are removed from game or practice and do not return until they have been medically cleared is an important risk-reducing strategy (Harmon et al., 2013).
Parents have the potential to play an important role in encouraging youth athletes to seek care for suspected concussion. Education about general health and safety starts at home, through verbal instruction and reinforcement of safety-related behaviors such as wearing helmets and using car seats (Tinsley, 1992; White, Kavussanu, Tank, & Wingate, 2004). For concussion, such informal parent-led education may include talking with the child about concussion symptoms and care seeking, as well as providing positive reinforcement for the child’s care-seeking behaviors. Perceived norms have been identified as a key determinant of whether athletes seek care for symptoms of suspected concussions, and parents are an important referent population whose opinions about concussion reporting matter to athletes (Chrisman, Quitiquit, & Rivara, 2013; Kroshus, Baugh, Daneshvar, & Viswanath, 2014; Kroshus, Garnett, Hawrilenko, Baugh, & Calzo, 2015; Register-Mihalik et al., 2013). One in 10 college athletes report parental pressure to continue playing their sport while experiencing symptoms of a concussion, and this was associated with being less likely to seek care for a suspected concussion (Kroshus et al., 2015). However, no published research to date has explored communication about concussion care seeking from the perspective of parents and no concussion education for parents has targeted parent communication about concussion safety.
Understanding what makes parents likely to communicate with their child in support of concussion safety is important for determining how to most effectively encourage this behavior. One important factor may be their concussion-related threat perceptions. Consistent with the health belief model (Rosenstock, 1974), parents who perceive a greater threat from concussions may be more likely to engage in concussion safety-related practices (i.e., encouraging concussion symptom reporting) compared with parents who perceive less threat. We operationalize “perceived threat” as the perceived likelihood that a concussion will be sustained in addition to the perceived harm if it were sustained (Brewer et al., 2007; Rosenstock, 1974). Such threat perceptions may be a product of experience: Having a child previously sustain an injury or having sustained a similar injury oneself tends to increase perceived susceptibility (Glik, Kronenfeld, & Jackson, 1991).
Attitudes about their child’s sport achievement may also influence parent communication. Parents play an important socializing role in their child’s sport participation (O’Rourke, Smith, Smoll, & Cumming, 2013; Sánchez-Miguel, Leo, Sánchez-Oliva, Amado, & García-Calvo, 2013; Wheeler & Green, 2014) but their actions are not always in the best interest of their child’s long-term health and development (DiFiori et al., 2014). For example, youth athletes are increasingly specializing at an early age in a single sport, training and competing year-round without adequate periods of recovery (DiFiori et al., 2014), and engaging in developmentally inappropriate supplementary training (Faigenbaum et al., 2009). These parent-initiated decisions can have physical, mental, and behavioral consequences for young athletes (DiFiori et al., 2014). It is possible that the importance parents place on their children’s sport achievement manifests in their concussion safety-related beliefs and behaviors; however, this has not been explored empirically. Consistent with Eccles’s expectancy-value theory (Eccles, 1993; Eccles et al., 1983; Fredricks & Eccles, 2004), parents who strongly value their child’s sport involvement may view concussion care seeking as interfering with athletic achievement, and may thus be less likely to encourage concussion care seeking.
Parent gender may also play a role in the extent of pressure put on sport achievement and likelihood of concussion safety communication. In general, fathers have a different approach toward risk taking and safety than mothers, with fathers more strongly valuing developmentally appropriate opportunities for their children’s risk taking, even if these opportunities include the potential for minor injuries (Brussoni, Creighton, Olsen, & Oliffe, 2013; Brussoni & Olsen, 2011, 2013). Striking a balance between risk taking and protection is seen as being part of a “fathering identity” (Creighton, Brussoni, Oliffe, & Olsen, 2017). In the sport domain, Gottzén and Kremer-Sadlik (2012) have described that fathers who are increasingly conforming to a more inclusive and nurturing form of masculinity face a tension with conforming to the traditional form of masculinity characteristic of sport when parenting in the sport context.
The present study tested three hypotheses. First, that greater perceived threat of concussion would be associated with greater parent–child communication about the importance of seeking care for a suspected concussion. Second, that parents who put more pressure on their child related to sport achievement would be less likely to encourage care seeking. Third, parental attitudes regarding sport achievement would modify the association between perceived threat of concussion and communication. We also sought to assess how these variables differed by parent gender, testing the hypothesis that mothers would place less pressure on their child related to sport achievement, and be more likely to encourage concussion reporting than fathers.
Method
Sample and Procedure
Parents of competitive youth club soccer players (8-18 years old) in a city located in the Pacific Northwest region of the US league were contacted by e-mail and invited to complete an anonymous online survey using Qualtrics™. Parents reviewed an information sheet and provided informed consent before viewing survey questions. Only one parent per athlete was included in the sample. Survey questions are provided as electronic supplemental material (available with the online article). Research activities were approved by the Seattle Children’s Research Institute Institutional Review Board.
Measures
Demographic Information
Parents reported the age of their child. Those with multiple children participating in the study soccer club were asked to respond with reference to their oldest child. Parents were asked to indicate their own gender.
Child Concussion History
Parents reported whether their child had ever been diagnosed with a concussion (yes, no).
Concussion Knowledge
Parents completed an 11-item adapted version of the general concussion knowledge assessment used in Glang, Koester, Beaver, Clay, and McLaughlin’s (2010) study of youth sport coaches. Items were included about the mechanism of injury (e.g., “You have to be hit on the head to have a concussion”), signs and symptoms (e.g., “Concussions often result in loss of consciousness”), and postconcussion management (e.g., “Any item requires removal from the game or practice”). Response options were “true,” “false,” and “I don’t know.” Correct responses were scored as one point each and summed to create an index with a maximum score of 11.
Perceived Likelihood of Concussion
Parents indicated how likely they thought it was that their child would sustain a concussion during the next year. Responses ranged from 0 (will not sustain a concussion) to 100 (will definitely sustain a concussion). The measurement approach was modeled on Diefenbach, Weinstein, and O’Reilly’s (1993) percentage scale for measuring health hazard susceptibility. Parents with multiple children participating in soccer were asked to respond with reference to their oldest child.
Perceived Harm of Concussion
Parents indicated how much harm they thought a concussion, if sustained, would cause their child in two time ranges: (a) during the next year and (b) when their child is an adult. The format of this question—asking about specific time frames and the harm their child would experience during these time frames, as opposed to the harm associated with concussion in general—is consistent with best practice approaches for measuring the perceived severity of a health threat (Brewer et al., 2007). As with the concussion susceptibility measure, responses were elicited on a scale ranging from 0 (no harm) to 100 (extreme amount of harm).
Parental Sport Pressure
Parents completed the “pressure” subscale of Babkes and Weiss’s (1999) parental influence on youth soccer players’ performance measure. The pressure subscale included five items that examined “parents’ self-reported desire that their child’s performance demonstrates high level of competence.” An example item was, “I put pressure on my child to play soccer well.” Responses were on a 5-point Likert-type scale, ranging from almost never (1) to almost always (5). Higher summed scores indicated greater pressure. In the present sample, the scale had adequate internal consistency reliability (Cronbach’s α = .70).
Parent–Child Communication
Parents were asked to indicate whether they had previously talked to their child about “the importance of immediately reporting symptoms of a possible concussion.” Ordered response options were “yes,” “somewhat,” and “no.”
Data Analysis
Means for all variables were compared between males and females using two-group t tests for continuous variables and χ2 tests of independence for categorical variables. Next, we tested whether the three-category parent communication variable met the proportional odds assumption and could thus be used as an ordered categorical dependent variable in logistic regression analyses. To do so, we first conducted a likelihood ratio test for a model in which harm and likelihood were independent variables and the three-category parent communication item was the dependent variable, testing the null hypothesis that the proportional odds between levels of the outcome variable were the same. A nonsignificant p value on this test was used as indication that parent communication could be treated as an ordered categorical dependent variable in the logistic regression analysis. Next, ordered logistic regression analyses were conducted. First, we ran bivariate models separately including each independent variable. Next, we constructed a series of models, beginning with perceived threat variables (Model 1), then adding parent pressure (Model 2), and potential confounding variables of child characteristics (age and history of concussion diagnosis) and parent characteristics (gender and concussion knowledge; Model 3). Subsequently, interactions between mean-centered parent pressure and each of the mean-centered threat perception variables (perceived likelihood, harm [year], and harm [adulthood]) were separately examined. Analyses were conducted using STATA 12.1 (College Station, TX) and threshold for significance was set at α = .05.
Results
Two hundred and thirty-six parents completed the survey. Most parents (95.53%) had an undergraduate or graduate degree. Additional descriptive statistics for the sample are presented in Table 1. Across the full sample, just over two thirds of parents (68.38%) indicated that they communicated with their child about the importance of reporting suspected concussions. The remainder of parents indicated that they had “somewhat” talked about this topic with their child (16.24%) or had not talked about this topic with their child (15.38%). On average, mothers rated the magnitude of harm over the next year as 40.72 (SD = 25.41) and during their child’s adult life as 19.49 (SD = 19.33), while fathers rated the magnitude of harm over the next year as 27.18 (SD = 20.46) and during adulthood as 11.57 (SD = 19.33). These differences between mothers and fathers were statistically significant and of moderate effect size (p = .001, Cohen’s d = .59, and p = .025, Cohen’s d = .61). Pressure related to sport achievement also differed by parent gender, with mean pressure among mothers of 12.80 (SD = 2.54) and among fathers of 13.81 (SD = 2.65). This difference was statistically significant and of moderate effect size (p = .025, Cohen’s d = .39).
Sample Characteristics.
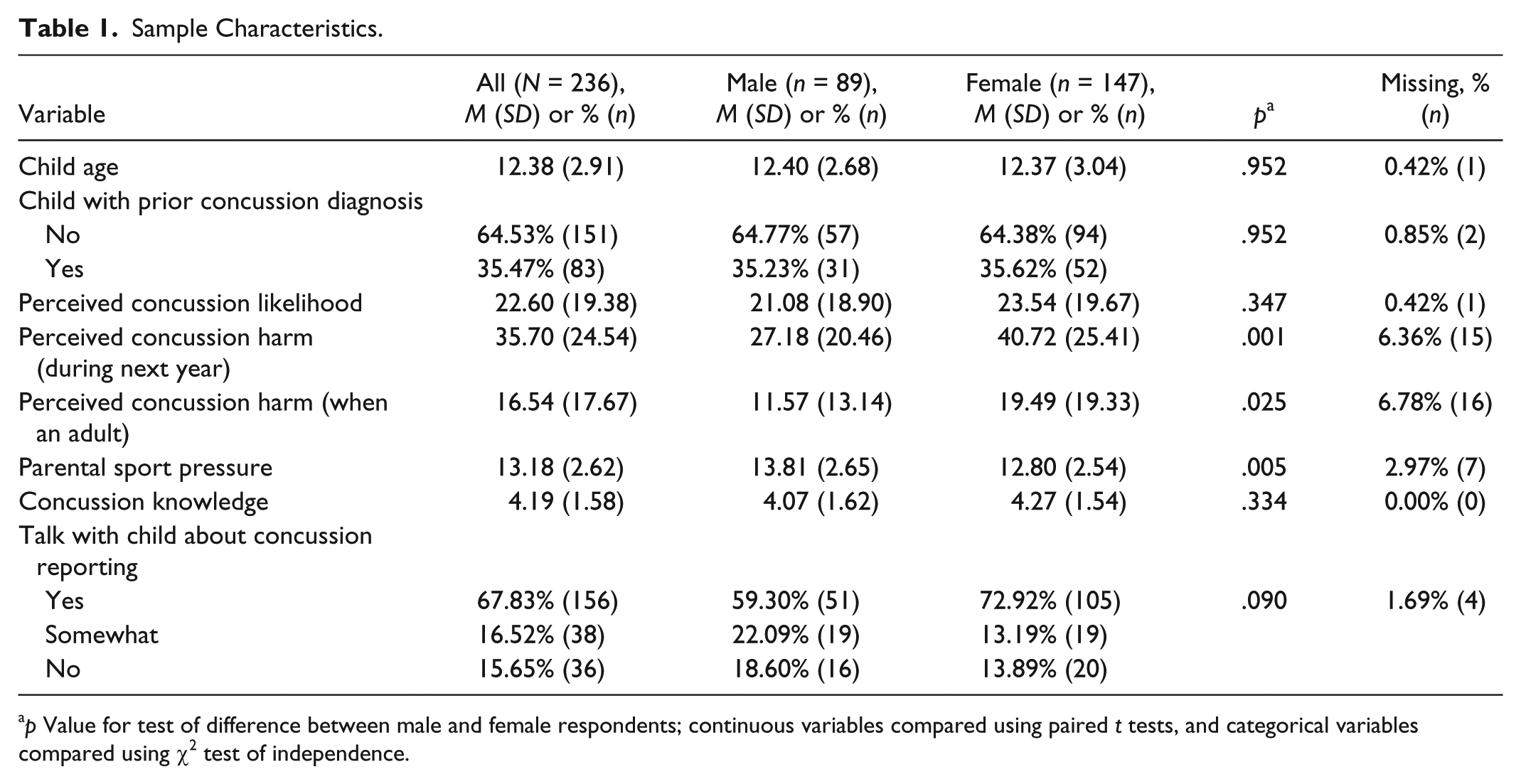
p Value for test of difference between male and female respondents; continuous variables compared using paired t tests, and categorical variables compared using χ2 test of independence.
Results of the bivariate ordered logistic regression analyses and multivariate ordered logistic regression analyses are presented in Table 2. As presented in Model 1, parents were more likely to encourage their child to report concussion symptoms when they believed that their child had a high likelihood of sustaining a concussion (odds ratio [OR] = 1.03, 95% confidence interval [CI 1.01, 1.04]), and when they believed that sustaining a concussion would be more harmful in the next year (OR = 1.01, 95% CI [1.00, 1.03]). Parents were less likely to encourage concussion symptom reporting the more harm they believed their child would experience from concussion as an adult (OR = 0.98, 95% CI [0.96, 1.00]). Parental pressure was independently associated with communication (Table 2; OR = 0.88, 95% CI [0.78, 0.99]) with parents who placed more pressure on their child being less likely to encourage concussion symptom reporting, controlling for the perceived threat of concussion. When child age, child’s history of prior concussion diagnosis, parent gender, and parent concussion knowledge were added to the model, the associations between perceived likelihood and communication and between pressure and communication were no longer statistically significant (Table 2). Parents of children with a prior concussion diagnosis were much more likely than those whose children had not had a prior concussion to have communicated about concussion reporting (OR = 7.86, 95% CI [3.00, 20.55]). As child age increased so too did parent odds of communicating about concussion reporting (OR = 1.36, 95% CI [1.19, 1.55]). A similar association was seen between increasing parent concussion knowledge scores and communication (OR = 1.36, 95% CI [1.09, 1.70]). Next, interactions between parental pressure and concussion threat variables were assessed. The interaction between parental pressure and perceived severity was significant both when the reference period was the next year (OR = 0.99, 95% CI [0.99, 1.00]) and adulthood (OR = 0.99, 95% CI [0.98, 1.00]). The interaction between parent pressure and concussion likelihood was not statistically significant. Interactions between gender and threat variables were also not statistically significant.
Ordered Logistic Regression for Parent–Child Communication About Reporting Symptoms of Concussion.
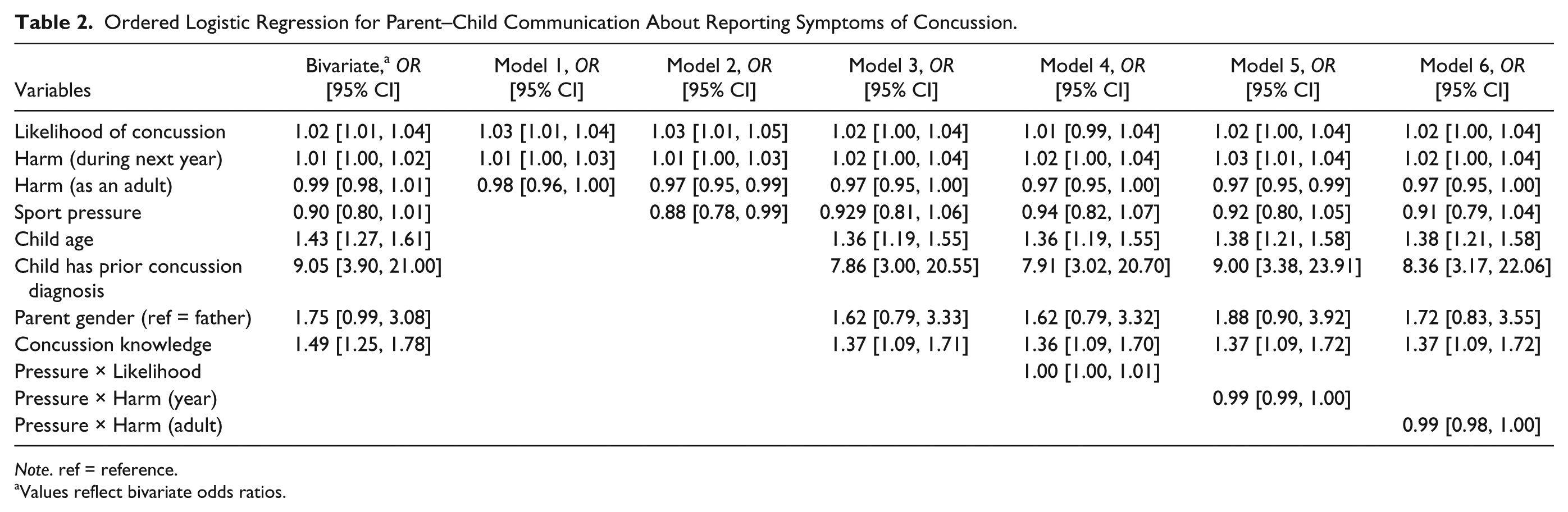
Note. ref = reference.
Values reflect bivariate odds ratios.
We conducted further post hoc analyses to explore the strong positive association between child concussion history and parental communication about concussion. First, we stratified communication behaviors by history of prior child concussion diagnosis. When a child had previously been diagnosed with at least one concussion, 90.48% of parents talked with them about the importance of immediately reporting symptoms of a future concussion, as compared with 56% of parents of a child who had never been diagnosed with a concussion (Pearson χ2 = 30.44, p < .001). Next, we explored whether there were differences in perceived likelihood of concussion by the child’s history of concussion diagnosis. Parents of a child who had previously sustained a concussion believed that their child was significantly more likely to sustain a concussion in the future as compared with parents of children who had not previously sustained a concussion (M = 27.17, SD = 22.17 vs. M = 20.78, SD = 17.36, t = 2.38, p = .018). Parent pressure scores were not significantly different by child’s history of concussion diagnosis (p = .571).
Discussion
Despite the theorized importance of parental communication about concussion safety, only two third of parents engage in such communication with their youth athlete. There is clear room for improvement and a need to identify factors that make parents more likely to engage in concussion safety communication. While we did find significant bivariate associations between perceived threat variables and communication, the magnitudes of these associations were very small. Perhaps most notable was the finding of differences in communication by the child’s history of concussion. This appears to be, at least in part, driven by greater perceived likelihood of a future concussion by parents of previously concussed youth. It is possible this reflects a true difference in risk, for example, if a child has a genetic makeup that makes them more susceptible to injury, or if a child plays in a style that makes them more susceptible to injury. It is also possible that when a child is diagnosed with a concussion, parents learn more about the signs and symptoms of a concussion and thus have experiential knowledge that allows them to talk about concussion more easily. Parents of previously injured youth may also become more aware of the importance of reporting symptoms of future concussion as a result of the time it took their child to recover.
Further study is needed to understand what it is about exposure to a prior injury that leads parents to be more likely to encourage future care seeking. Such work can be used to design improved educational programming to support all parents in encouraging care-seeking communication. For example, to increase perceived likelihood among parents of youth who have not previously sustained a concussion, it may be useful to use narrative communication strategies with exemplars to make information about the injury feel more personally resonant (Dahlstrom, 2014). Should concussion education for parents seek to increase perceived susceptibility, it is critical that this messaging be accompanied by concrete steps that parents can take as well as credible information about the efficacy of engaging in these steps. When a health outcome is viewed as highly threatening, but there are no apparent risk-reducing strategies, this can lead to anxiety and behavioral paralysis (Witte & Allen, 2000). Providing information to parents about how talking to their child about concussion reporting can decrease their child’s potential for harm by increasing early care seeking may help increase perceptions of the efficacy of this behavior. Programming that provides modeling or that helps parents practice this conversation may also be beneficial for supporting parent action.
The results of this study suggest that parent attitudes about their child’s sport achievement may be another consideration when designing concussion education. There was a significant direct effect between pressure and communication, with parents who place more pressure on their child less likely to encourage concussion reporting. Additionally, there were significant interactions between parent pressure and perceived harm, with the relationship between perceived harm and communication less strong among parents who placed more pressure on their child. Consistent with Eccles’s expectancy-value theory (Eccles, 1993; Eccles et al., 1983), it is possible that parents believe that if their child reports a minor concussion, they will be unnecessarily kept out of play and will subsequently lose competitive opportunities. Alternatively, or additionally, parents may believe that communicating to their child about concussion reporting will make them play more tentatively or may result in oversensitivity to symptoms that are not in fact the result of a concussion. Building on these findings, concussion education efforts for parents should include content about the athletic consequences of continued play while symptomatic—for example, slower reaction time (Eckner, Kutcher, Broglio, & Richardson, 2014). Taking a step back from a focus solely on concussion, it may be useful to educate parents about athletic development benefits of taking a less intense approach to youth sport participation overall (Fraser-Thomas, Côté, & Deakin, 2005). The present findings provide additional support for the benefits of shaping lower pressure parent attitudes toward sport achievement.
Interventions related to shaping healthier sport-parenting practices should consider tailoring by parent gender. We found notable gender differences in the perceived harm of concussion and in parental pressure related to sport achievement. Mothers tended to think that concussions would result in more harm in both the next year and in adulthood than did fathers. We cannot say on the basis of these results whether mothers or fathers were more accurate in their perceptions of harm. Prior research has suggested that threat perceptions are not necessarily accurate, and parents may be subject to an optimistic bias phenomenon, whereby they think that their child is less likely to get injured than other children (Gielen et al., 2004). It is possible that in valuing risk taking and sport achievement more strongly than mothers, fathers were subject to a self-protective cognitive bias in believing concussions would be less harmful. Understanding the root of these differences in perception can help develop educational interventions that resonate with both mothers and fathers. It may be useful to explore how educational messaging about concussion safety can be framed as consistent with sport achievement: for example, emphasizing how failing to report a concussion ultimately leads to more time away from the game and may put an athlete at risk for a career ending subsequent injury (Asken et al., 2016).
Limitations
Only 15% of parents on the e-mail list to whom the survey was distributed chose to participate, and it is likely that these parents are a highly engaged group with an interest in, or concern about, concussions. Additionally, the parents in the present sample were highly educated. Consequently, the mean values reported in this study for perceived likelihood and harm of concussion are likely not representative of all youth soccer parents and they may also not generalize to parents of youth participating in other sports. Additional research is needed to extend the present analysis to other sports, to include parents with less education, and to use a data collection modality (e.g., in person at a mandatory administrative meeting) that can result in a greater response rate. Another limitation of the present study was the approach to measuring perceived likelihood and harm. There are no existing validated measures of these constructs as they pertain to concussions. Our measurement approach was modeled on existing literature in other domains and we chose to use a single-item summary measure for each construct to limit participant response burden.
Conclusion
Parents can play an important role in shaping their child’s attitudes and behaviors toward seeking care for a suspected concussion. Possible directions for concussion education for parents based on the results of this study include providing parents with concrete guidance about the important role they can play in encouraging their child to report symptoms of a concussion, communicating the athletic consequences of continued sport involvement while experiencing symptoms of a concussion, and using narrative messaging with exemplars to personalize the information for parents of youth who have not previously sustained a concussion. Research is needed to understand how to most effectively and acceptably deliver such information to parents. More broadly, these findings underscore the importance of developing initiatives to support healthy, and developmentally appropriate, sport parenting as such efforts may have benefits that include greater parent encouragement of concussion safety.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.