
Abstract
African American women have the highest colorectal cancer incidence and mortality rates among women of any race/ethnicity in the United States. Colonoscopy screening is an efficacious procedure for the prevention and early detection of colorectal cancer, making it a promising tool in the effort to eliminate colorectal cancer disparities. Toward that end, the present qualitative study sought to assess acceptability of and preferences for a beauty salon–based intervention to promote colonoscopy screening among African American women. A total of 11 focus groups were conducted: 6 with staff from African American–serving salons (n = 3 with salon owners, n = 3 with salon stylists) and 5 with African American salon clients. Theory-guided focus group questions were used to explore participants’ beliefs, interests, and preferences associated with the proposed intervention. Results indicated that, across all subgroups, participants were highly supportive of the idea of a salon-based intervention to promote colonoscopy screening among African American women, citing reasons such as the commonplace nature of health discussions in salons and the belief that, with proper training, stylists could effectively deliver colorectal cancer-related health information to their clients. The greatest differences between salon staff and clients were found with respect to the specifics of the intervention. Staff focused more heavily on content-related issues, such as the specific information that should be stressed in the intervention, whereas clients focused largely on process-related issues, such as the preferred intervention formats and how stylists should present themselves to clients. The findings from this study offer both encouragement and important groundwork for the development of a salon-based, stylist-delivered intervention to promote colonoscopy screening among African American women.
Keywords
African American women have the highest colorectal cancer (CRC) incidence and mortality rates among women of all racial/ethnic groups in the United States (American Cancer Society, 2017). The incidence of CRC among African American women is 47.6 per 100,000 compared with 38.6 per 100,000 among non-Hispanic White women, while their CRC death rate among African American women is 41% higher than that of their White counterparts (American Cancer Society, 2016). Although colonoscopy screening (CS) is efficacious for both the prevention and early detection of CRC (Jacob, Moineddin, Sutradhar, Baxter, & Urbach, 2012), only about 60% of African American women report having undergone recent CS (Adams-Campbell, Makambi, Mouton, Palmer, & Rosenberg, 2010)—a rate that is particularly unfortunate given the excess burden of CRC within this population and the utility of CS in reducing CRC morbidity and mortality. Increasing rates of CS among African American women might therefore represent a promising strategy to reduce—and ultimately eliminate—the burden of CRC among African American women. Differences in screening have been found to account for up to 42% of the disparity in CRC incidence and 19% of the disparity in CRC mortality between African Americans and non-Hispanic Whites (Lansdorp-Vogelaar et al., 2012).
Beauty salons and barbershops have been increasingly highlighted as culturally appropriate venues for health promotion among African Americans. Both have played an historic role in African American communities as sources of news and information, are routinely frequented by African American clients (Wilson et al., 2008), and represent trusted environments where frank discussions surrounding a variety of topics—including health—are already commonplace (Solomon et al., 2004). Barbers and stylists have been identified as “natural helpers” who are interested in discussing health topics with their clients (Browne, 2006; Hart et al., 2008; Linnan et al., 2001; Linnan et al., 2011; Solomon et al., 2004) and, importantly, would feel comfortable doing so (Linnan et al., 2011; Linnan, D’Angelo, & Harrington, 2014; Luque et al., 2015). The bond often reported to exist between African American barbers/stylists and their clients also suggests that barbers and stylists may be uniquely effectual as lay providers of—and/or liaisons to—health information and services (Linnan et al., 2014; Luque, Ross, & Gwede, 2014).
These strong foundations have already translated into several barbershop interventions to address health topics such as prostate cancer (Frencher et al., 2016; Luque et al., 2011) and hypertension (Hess et al., 2007; Ravenell et al., 2013; Releford, Frencher, Yancey, & Norris, 2010; Victor et al., 2011) among African American men, while salon-based interventions targeting African American women have focused primarily on the topic breast cancer (e.g., Howze, Broyden, & Impara, 1992; Linnan et al., 2001; Linnan et al., 2005; Linnan et al., 2007; Linnan & Ferguson, 2007). Notably, they have also established the feasibility and efficacy of stylist-delivered interventions. Wilson et al. (2008) trained stylists to educate women of African descent about breast cancer screening and found that self-reported exposure to stylist-delivered messages was associated with improved breast self-examination rates and greater intentions to have a clinical breast exam. Sadler et al. (2011) reported that a stylist-delivered breast cancer education program significantly improved mammography screening rates among African American women: Women in the experimental condition were twice as likely to have become adherent to mammography screening during the 6-month follow-up period compared with women in the control condition.
In their recent review of health promotion research in beauty salons and barbershops, Linnan et al. (2014) reported that, although 47.6% of the studies were cancer-related, their focus was on either prostate, breast, or general cancer prevention topics (Linnan et al., 2014). The authors suggest that more research is needed to fully understand which topics and types of interventions are more or less suited for the beauty salons/barbershop setting. Such investigation is clearly warranted with respect to CRC and CS. Only handful of barbershop interventions addressing CRC screening among African American men have been described in the literature (e.g., Holt et al., 2009; Ravenell et al., 2013), with evaluation of intervention effects yet to be reported. What is more, to our knowledge, there are currently no salon-based interventions specifically aimed at promoting CS among African American women.
Although salon-based interventions to promote breast health among African American women have met with success, there is reason to question the extent to which an intervention focused on CRC and CS would yield similar results. Women might be comfortable discussing breast cancer in salons given that the topic is already common in the public discourse, whereas CRC and CS are appreciably less so. Details of the colonoscopy procedure (e.g., laxative preparation, insertion of the colonoscope) may also be viewed as too personal and/or embarrassing to discuss in public or with one’s stylist, and may even meet with objection among women in the salon who are not the targets of the intervention (i.e., those younger than 50 years of age) but who are nonetheless in the position to overhear its content. If the broader salon clientele is averse to a CS-promotion intervention, then salon owners might take pause in adopting such a program for fear of it negatively affecting their business—particularly given that women younger than 50 years of age likely comprise a significant proportion of their clientele. Each of these factors can lead to low levels of acceptability for a salon-based, CS-promotion intervention.
Differences in personal knowledge about breast cancer/mammography screening compared with CRC/CS may also have implications for the stylists serving as lay health educators. Compared with a breast health intervention, stylists delivering a CS-promotion intervention may need to bridge a larger knowledge gap—both for themselves and their salon clients—thus resulting in different (e.g., more intensive) levels of stylist training and client intervention required to affect change. Stylist may also find it more challenging to develop self-efficacy with respect to helping clients overcome fear of the colonoscopy procedure, which continues to be a major barrier to screening (Jandorf et al., 2013; Sly, Edwards, Shelton, & Jandorf, 2012). Combined, these factors may represent the need for more effort than stylists are either able or willing to undertake in order to serve as lay health educators in a CS-promotion program.
A salon-based, stylist-delivered intervention to promote CS among African American women has the potential to be a powerful and highly disseminable tool in the effort to reduce CRC disparities. However, given the unique aspects CRC and CS, it is necessary to first determine the acceptability of such an intervention among the primary stakeholders; namely, salon owners, stylists, and the female African American salon clients. Toward that end, the goal of the present focus group study was to determine acceptability of and preferences for a salon-based, stylist-delivered intervention to promote CS among African American women aged 50 years and older. Focus groups were the chosen approach given their noted utility when designing interventions targeting specific populations (Larkey & Gonzalez, 2007), and in keeping with recent recommendations to use community-based participatory approaches in designing barbershop and salon-based health promotion interventions (Linnan et al., 2014).
Method
Recruitment
Recruitment for the focus group interviews was localized to Central Harlem, a predominantly African American section of New York City, and was conducted sequentially for salon owners, stylists, and last, salon clients. Prospective participants were informed that the project was a focus group study to assess interest in beauty salons serving as a source of health education for African American women, and that they would receive $50.00 for their participation in a 2-hour group discussion with fellow Central Harlem beauty salon owners/stylists/clients. The study received full review and approval from the institutional review board of the City University of New York. The inclusion criteria for all participants was being at least 18 years of age and able to write and speak in English. In addition, beauty salon clients had to identify as female and African American. It is of note that, although screening for CRC is recommended to begin at age 50 for person at average risk, the age-related inclusion criterion for salon clients was the same as that for the other focus group discussions; namely, being at least 18 years of age. In keeping with the spirit of community-based participatory research, we did not want to exclude a sizeable and important part of the salon community. In addition, including younger clientele supports the ecological validity of our findings by addressing the extent to which all elements that exist within the salon system—not just those most proximally affected or targeted by the proposed intervention—are accepting of the potential changes to their shared salon environment.
Recruitment of Beauty Salon Owners and Stylists
Beauty salons were first identified through a combination of Internet searches, neighborhood canvassing, and “snowballing” procedures, with individual salons identifying other salons in the area. A brief introductory letter was then mailed care of the owners of all identified salons explaining the purpose of the study, and informing them that either a follow-up phone call or in-person visit to the salon would be made within approximately 1 week in order to provide more details. The letter included the contact information for the lead study research assistant, whom they could contact in advance if they did not wish to participate in the study.
Salon stylists were identified through referral from salon owners (including those who did not participate in an owner focus group) and during in-person visits to salons. Salon owners who referred staff to the study were asked to provide the prospective participating stylists with the project’s contact information, thus enabling the stylist to initiate contact if interested. Stylists who were directly engaged while at their salon were given a brief verbal introduction to the study and asked to provide their contact information so that further details could be discussed.
Recruitment of Beauty Salon Clients
Postcards were created to recruit beauty salon clients for the focus group discussions. The postcards stated that adult African American women were being sought to participate in a 2-hour focus group with other salon-going African American women regarding bringing health education to neighborhood beauty salons. Contact information was provided on the postcard so that interested salon clients could call the lead study research assistant if interested. Project staff visited Central Harlem beauty salons and requested permission from the salon owners/managers to leave the postcards in prominent areas for the clients to take. Owners/managers were also asked for permission to speak with any clients currently in the salon for the purpose of recruitment.
Participants
A total of 11 focus groups were conducted: 3 with beauty salon owners, 3 with salon stylists, and 5 with salon clients. Salon owners (N = 17; 94.1% female, 70.6% non-Hispanic Black; mean age = 48.9 years) reported that their salon serviced an average of 31.5 clients per day, approximately 39.6% of whom are aged 50 years or above. Stylists (N = 13; 92.3% female, 84.6% non-Hispanic Black; mean age = 39.7 years) reported a similar percentage of salon clients aged 50 years or above (35.8%) and a similar volume of salon clientele, indicating an average of 33.7 clients per day. All participating salon clients (N = 43) identified as Black/African American and female (0.5% Hispanic/Latina, mean age = 46.8 years) and reported an average salon visit of 3 hours. The majority of salon clients reported going to the salon either once every 2 weeks (44.2%) or once per week (32.5%).
Focus Group Design and Topics
Focus group questions were guided by constructs of social cognitive theory (e.g., self-efficacy; Bandura, 1986), theory of planned behavior (e.g., social norms; Ajzen, & Fishbein, 1980), and the health belief model (e.g., cues to action; Rosenstock, 1974), each of which has demonstrated efficacy in predicting cancer-related health behavior. Table 1 lists the specific content areas covered by the focus group and sample questions from each area. Groups were stratified based on primary relationship to the salon (i.e., owner, stylist, or client) given the need to pose several questions unique to each subgroup (e.g., for salon stylists, “If the appropriate training were made available, how interested or disinterested would you be in talking to your clients about colorectal cancer screening?”) and the distinct possibility that different themes and priorities would emerge across each subgroup. For example, salon owners might view offering a CS-promotion program as a good opportunity to raise their salon’s profile within the community and, as a result, be very receptive to the idea. Salon stylists, however, might view it as something that requires considerable time and effort on their part but that yields little direct benefit to them personally, thus leading to less overall interest and motivation.
Focus Group Content Areas and Sample-Specific Questions.

Accordingly, separate focus group guides were created for each participant group and included questions specific to their group membership, as well a general questions that were relevant and thus posed to three all participant groups (e.g., “How appropriate do you think beauty salons are for sharing information about colorectal cancer screening?”). Owners who were also salon stylists participated in the salon owner focus groups. All focus groups took place in a private room at a community-based venue (either at a public library or community center) and were facilitated by the trained project staff following the guidelines of conducting focus group methodology (Morgan & Kreuger, 1997).
Prior to initiating the focus group discussions, a 15-minute PowerPoint presentation was delivered to ensure that all participants had the same minimum level of understanding regarding CRC and CS. The presentation defined CRC as cancer that develops in the colon and/or rectum, covered the behavioral risk factors for CRC, the disproportionate burden of CRC among African Americans, the various forms of CRC screening, and a description of CS and why it is considered the “gold standard” in CRC screening.
Session Proceedings
Each focus group began with the study’s institutional review board–approved consent document being read to the participants, each of whom then signed a form acknowledging that the document was read to them and that they agreed to participate in the focus group discussion. Participants were given a copy of the informed consent summary. Participants then completed a brief sociodemographics and salon characteristics questionnaire. Each person then introduced himself or herself to the group and stated the name and location of the salon that they owned/worked at/patronized. Depending on the time of day, either a continental breakfast or a light lunch was provided. All sessions were digitally audiotaped, and a designated note-taker was also present to summarize content and document contextual elements (e.g., nonverbal behaviors, signs of discomfort among the participants). All focus groups were moderated by the study principal investigator (lead facilitator) and an assistant facilitator; an African American and multiracial woman, respectively. Each session concluded with the lead facilitator offering a summary of the comments and conclusions from the day, and inviting participants to add to, modify, or correct the summarized findings.
Analysis
All audiotapes were professionally transcribed and the transcripts then analyzed by a three-person analysis team, including an initial two-person coding team (the assistant facilitator and a master of arts–level graduate student not present during the focus groups), and an outside qualitative methods specialist. The analytic process described below was conducted in three waves, following the order of recruitment. Specifically, the first wave of analysis was conducted with transcripts of salon owner focus groups, followed by those with salon stylists, and last, those with salon clients.
The two-person team was trained to generate initial codes, define codes, and identify themes for the first transcript. After independently coding the first transcript, they then met to discuss and refine their codes and generate an initial codebook. The same process was then used in an iterative fashion for coding all subsequent transcripts. Specifically, the two-person team met to discuss their codes, refine existing codes, and revise the codes applied to previous transcripts as needed based on new data/newly developed codes and themes. Initial consensus documents were generated for each transcript; one for each of the study focus groups. The documents were later utilized by the qualitative methods specialist in conjunction with the original focus group transcripts to generate the final consensus document for each focus group. The qualitative methods specialist utilized existing codes from the two-person team and also identified additional codes and themes that could be applied to the data. The codes and themes selected for the present article represent those from the final consensus documents, which reflect input from all three members of the data analysis team. The themes most relevant to the study’s research objectives are reported herein.
Results
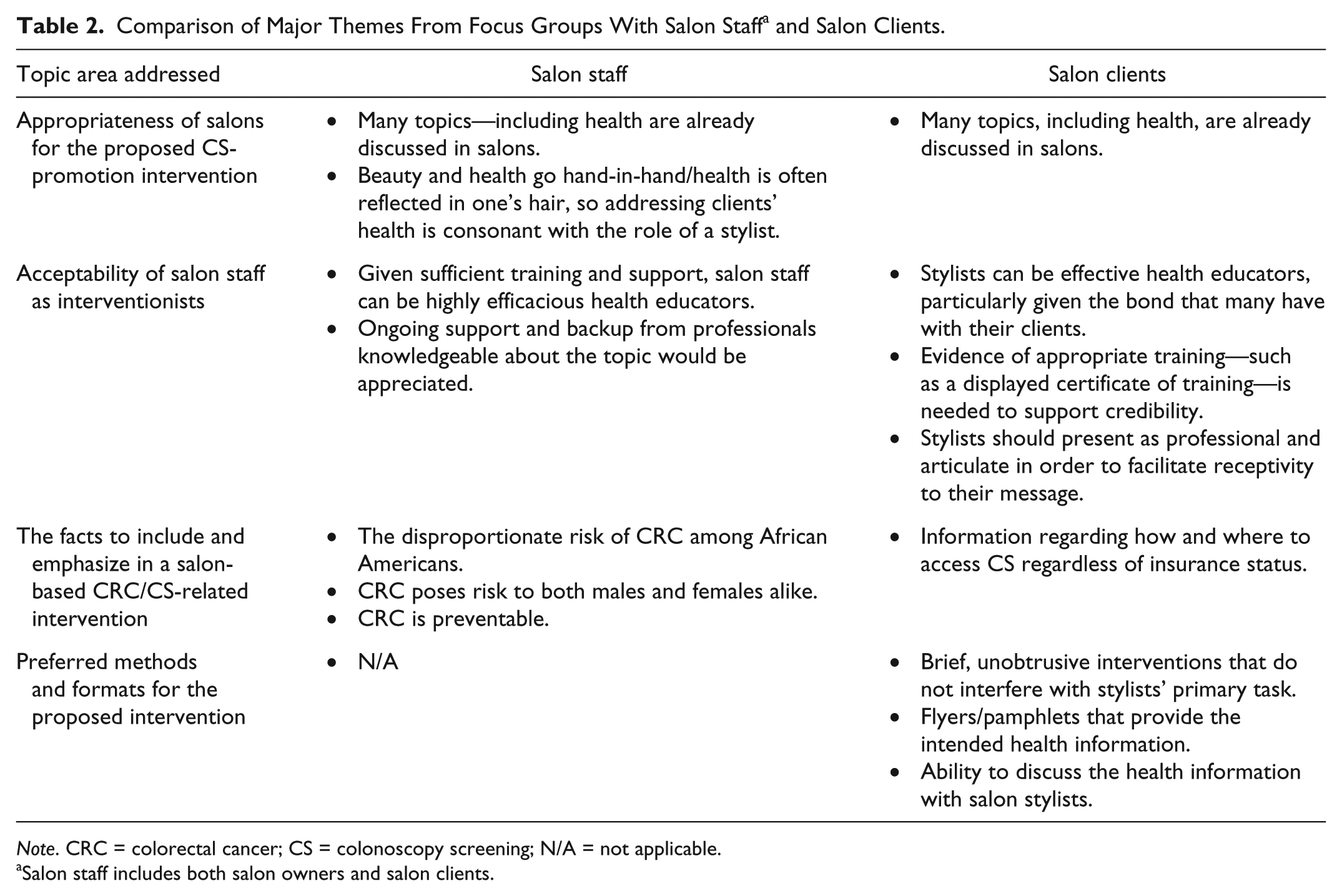
Although conducted and analyzed separately, the themes that emerged from focus groups with salon owners and were markedly consistent with those that emerged from salon stylists. As such, and in order to facilitate in interpretation, the themes from salon owners and staff are represented collectively as themes from “salon staff” (i.e., owners and stylists), which are compared and contrasted with those that emerged from focus groups with salon clients (see Table 2).
Comparison of Major Themes From Focus Groups With Salon Staff a and Salon Clients.
Note. CRC = colorectal cancer; CS = colonoscopy screening; N/A = not applicable.
Salon staff includes both salon owners and salon clients.
Core Themes From Beauty Salon Staff (Salon Owners and Stylists)
Analysis of transcripts from beauty salon staff revealed several themes that supported extant knowledge regarding the relevance of health education within the salon setting. They also lent encouragement for the development of a salon-based CRC/CS-promotion intervention and the possible role of stylists in delivering such an intervention.
Acceptability and Appropriateness of a Salon-Based CRC/CS-Promotion Intervention
Salon staff expressed strong support for a salon-based CRC/CS-promotion intervention. Two core themes emerged that from salon staff in response to questions regarding acceptability of a salon-based, CRC/CS-promotion intervention. Table 3 provides additional sample supporting quotes for each of the themes summarized below.
Acceptability of a Salon-Based Colonoscopy Screening-Promotion Intervention for African American Women: The Perspective of Salon Staff.

Many topics, including health, are already discussed with salon clients
Salon staff emphasized the fact that salons are a place where a multitude of topics are openly and routinely discussed, including health.
The clients, they’re really interested in their health. . . . And they have a positive attitude, you know, about talking about it. (Salon owner) They do talk a lot about their health. I mean, secretly, I find women sit in the chair and they have a health problem, and they really want to say something about it, you know. (Salon stylist)
As a result, they saw no reason why CRC and CS could not be among the many topics that are shared and explored. One stylist even indicated that it is already a prevalent topic:
We talk about everything. I mean, there’s nothing off the table, whether I bring it up or they bring it up. If it’s something current, no matter what it is, it’s in the shop that day. And colon cancer been in the shop so much lately. Because a lot of the clients are being diagnosed as having colon cancer.
Beauty and health go hand-in-hand/health is often reflected in one’s hair
Salon staff also indicated that one’s hair is often an indicator of their health, so they are also concerned about the health of their clients and view advocating for health as consonant with their roles as hair professionals. As one stylist described,
And I’m not just concerned about your outside hair, because it also delves from within. So we also, as hairstylists, we love to deal with your hair but we also worry about overall health.
Another expressed a similar viewpoint:
You know, change in the skin color, change in the hair texture . . . there’s so many different ways to tell, that [is why] we are the perfect advocates to help people.
Acceptability of Salon Staff as Interventionists
Salon staff also expressed confidence in their ability to deliver a CRC/CS-promotion intervention to their clients, but also pointed out that they would need sufficient training and access to continued support for the role, as described in the following themes (see also Table 4 for additional supporting quotes):
Acceptability of Stylists as Interventionists: The Perspective of Salon Staff.
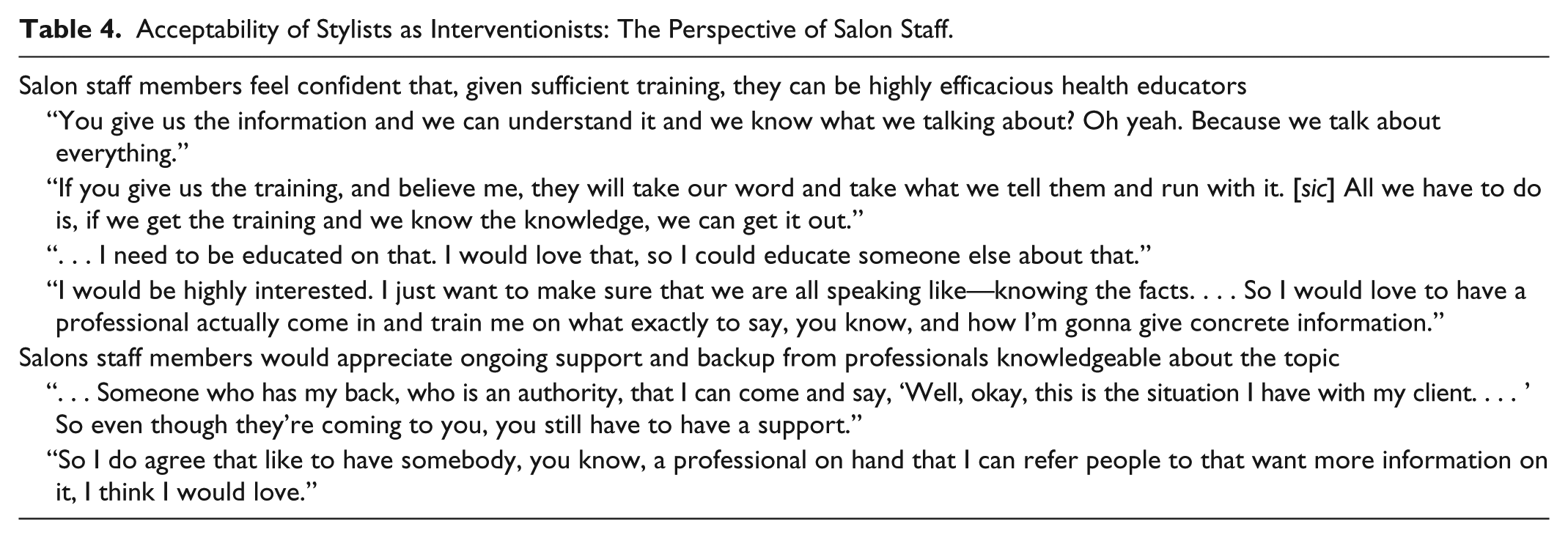
Salon staff members feel confident that, given sufficient training and support, they can be highly efficacious health educators
The prediscussion PowerPoint presentation allowed salon staff to be aware of the type of information that might be shared in a salon-based, CRC/CS-promotion intervention. In response, many seemed eager for the opportunity to educate their clients on these topics and shared that, with the proper training, they would be able to successfully engage their clients. As one stylist shared,
If you give us the training, and believe me, they will take our word and take what we tell them and run with it. . . . All we have to do is, if we get the training and we know the knowledge, we can get it out.
Salons staff members would appreciate ongoing support and backup from professionals knowledgeable about the topic
Despite confidence in their ability to deliver health information to their clients, salon staff also acknowledged a need for continued support following the proposed training. Such resources were desired both for themselves
. . . someone who has by back, who is an authority, that I can come and say, “Well, okay, this is the situation I have with my clients . . . ” So even though they’re coming to you [the stylist], you still have to have a support. (Salon owner)
as well as for their clients:
So I do agree that like to have somebody, you know, a professional on hand that I can refer people to that want more information on it, I think I would love. (Salon stylist)
Key Points That Should Be Emphasized and Included in a Salon-Based CRC/CS-Related Intervention
Several facts presented during the prediscussion PowerPoint presentation were of particular interest to salon staff, largely given lack of knowledge regarding the information prior to viewing the presentation. Specifically, staff underscored the importance of three core facts/content areas:
The disproportionate risk of CRC among African Americans should be more well-known
Many participating salon staff members were not aware that African Americans are more likely to be diagnosed with and die from CRC than members of other racial/ethnic groups in the United States. One participant noted,
I should say, like bringing more awareness to colon cancer. Because for me, most of us here, we know about it, but not really consider it maybe to be like one of the leading [cancer] death sentences [for African Americans]. (Salon stylist)
Another echoed a similar sentiment, suggesting that African Americans need to be aware of the fact that they need to get checked for CRC:
Just like she asked before, does it hit a lot of African American cultures? About 99% of my customers are African American. So I would probably say that because we have a tendency of not being—you know, having physicals. So I would probably kind of use that a little bit, like, “You need to be checked out.” (Salon owner)
CRC poses risk to both males and females alike
Several participating salon staff expressed surprise at the fact that females could also be diagnosed with CRC. Comments included the following:
I didn’t even know that women get it at all. I keep saying that because I just thought only men get it. (Salon stylist)
I was going to say, I believe there’s a myth. I’m not going to necessarily say amongst our people, but in general, I really thought more men suffered from it. (Salon owner)
The fact the CRC can be prevented is highly important and should be emphasized
Several participants were struck by the fact that CRC could be prevented and suggested that it was an important fact to include in any intervention regarding CRC. As one stylist stressed,
. . . how to prevent it from happening—I think that’s the number one thing, is educating them on how they can prevent it from happening. (Salon stylist)
For some, the issue of prevention was so crucial as to be considered a topic of the highest priority:
I think with awareness, giving people information on how to prevent it from happening, because you did mention, okay, if it’s as big in our community, well how do we prevent it, you know? [sic] Like that’s the thing that should be put out there first . . . (Salon stylist)
Core Themes From Beauty Salon Clients
Ideas shared by salon clients also pointed to the promise of a salon-based, CS-promotion intervention for African American women. Several major themes emerged, along with multiple subthemes that highlighted the intervention features that clients would find most acceptable. Each of the major themes are listed and summarized below. The subthemes and sample supportive quotes for each are provided in Table 5.
Acceptability of and Preferences for a Salon-Based Colonoscopy Screening-Promotion Intervention: The Perspective of Salon Clients.

Acceptability and Appropriateness of a Salon-Based CRC/CS-Promotion Intervention
Salon clients expressed that salons are places where they commonly discuss a wide range of health topics with their stylists, with whom they tend to share a notable bond. Given that health is one of the most prevalent topics discussed in the salons, clients felt that discussion of CRC/CS would be acceptable. As one mentioned,
We talk about anything in there, but mainly it’s about our health that we talk about in there, so I know it wouldn’t be a problem . . .
Acceptability of Salon Staff as Interventionists
Salon clients believed that salon staff appropriate could be effective lay health educators, but also pointed to several factors that would influence their receptivity to stylist-delivered health messages.
Stylists can be effective health educators given the bond that many have with their clients
Many salon clients emphasized the bond that they share with their stylists, which can lead the former to be particularly receptive to stylist-delivered messages.
And you feel comfortable talking to your hairstylist, because you build that kind of relationship with them. And you could talk to ‘em about anything, you know.
Importantly, this receptivity extends to health-related topics. As expressed by one client,
So if my stylist, the person that you trust the most with your hair, you know, a physical thing, is also able to tell you something about your health, I think that’d be very good.
Although many clients acknowledged a strong bond with their stylist and intrinsic confidence in his or her potential as a health educator, others express the need for more than just the “stylist” identity to make them feel confident in his or her abilities as a health educator. Specifically:
Clear evidence of stylists’ training would bolster confidence in the accuracy of the information
Observable evidence of the education and training that stylists received to deliver the health information would be appreciated. For example,
[They should have a] certificate showing me that they went through some kind of training that they can really talk to me about it.
Clients will be most receptive to stylists who present as articulate and professional
Salon clients reported that some stylists are notably less articulate and refined than others. As such, they would prefer to receive health information from a stylist who presents as professional and has good communication skills. As one woman put it,
It’s the way they greet you, you’ll know if they that person to have that intellectual kind of conversation with you and stuff like that. Because they might know about it but they can’t, you know—deliver it.
The Intervention Should Address How and Where to Access CS Regardless of Insurance Status
For salon clients, the primary fact that they felt should be included in the proposed intervention was information about where and how to access CS. In short, they wanted some guidance on how to act on the health information provided, particularly in light of potential insurance-related barriers. As one client suggested,
And at the end you can direct people where to go to have the procedure done. You know, because some people don’t have insurance. Insurance is a major issue.
Preferred Modes and Formats for the Intervention Include Print Material and Casual Discussion
A brief and unobtrusive intervention is preferred in the salon setting
Clients expressed a clear preference for brief information-delivery formats that would not interfere with the stylists’ ability to continue to style their hair. As one woman described, anything that would require stylists to deviate from their primary task would be undesirable:
But if talking about it, you know, then she gotta stop and pull out pamphlets and, “Girl, let me give you this . . . ” or, “Hold on, let me write down a website.” If you doing all of that, then, no, I don’t want it. Because that’s too much.
Flyers/brochures/pamphlets are good ways to deliver health information
Consistent with their preference for a brief, unobtrusive intervention, salon clients suggested that brochures and flyers would be a highly acceptable way to receive health information. One participant even cast it as a useful way to pass the time:
No, I agree about the brochures and that. I spend a lot of time under the hairdryer, so I’m always searching for something else to read.
For some, the ability to discuss the information is crucial to their ability to engage the materials
Some salon clients expressly indicated that they would like or even prefer the opportunity to actively discuss the topic with another person. They pointed to the fact that print material is not sufficiently dynamic or engaging and that having a conversation with someone and being able to ask questions would be the best way to get the message across. For example,
If I look at this paper, I’m looking at it, but then if I want to know something, I have to wait and either go on the internet, I ain’t into that either, but I want to be able to talk to somebody that can give me the information I want.
As outlined in Table 2, salon staff and salon clients were in agreement regarding the appropriateness of salons for health-promotion activities, but differed most notably with respect to the specific content that they considered to be important for a CRC/CS-related intervention.
Discussion
The present study sought to determine acceptability of and preferences for a salon-based intervention to promote CS among African American women. Several studies have already established the feasibility of barbershop and beauty salon–based interventions for health promotion, particularly within African American communities (see Linnan et al., 2014, for a review). Our findings not only provide continued support for this overall model—participants across all three subgroups expressed that salons are natural and appropriate venues for health promotion—but they also take the important step of establishing CS, specifically, as a suitable topic for the salon environment. The significance of this finding is manifold. To begin, it suggests that the salon model may represent a robust method for addressing a variety of health-related issues, not just those deemed to be of particular relevance and/or interest to women (e.g., breast cancer). Future studies should further explore the potential bounds of the model’s utility in addressing other health-related content areas, but it is encouraging to find that CS—a topic potentially considered too graphic or embarrassing to discuss in public—is something that our participants embraced. Indeed, this may simply underscore the desire of African Americans to receive health-related information, even if it is of an intimate nature, from settings and sources that feel more comfortable and trusted than those encountered in the mainstream health care system. Indeed, medical mistrust is still common among African Americans and has been linked to lower rates of CRC screening within this population (see Adams, Richmond, Corbie-Smith, & Powell, 2017, for a recent review).
To our knowledge, this is the first study to establish acceptability of a salon-based CS-promotion intervention for women; however, barbershop interventions to promote CRC screening have already been described in the literature (e.g., Ravenell et al., 2013). Although studies assessing the efficacy of these interventions have yet to be reported in the scientific literature, our preliminary findings converge substantially with the formative research of Holt et al. (2009), who described development of a barbershop intervention to address prostate and CRC. Men in their advisory board—a combination of barbers, shop patrons, and cancer survivors—suggested that statistics regarding the burden of CRC among African American men and the fact that a test for CRC can be lifesaving be among the central messages conveyed. This is consistent with the recommendation of salon staff in our sample, who indicated that the risk of CRC to African Americans and the fact that CRC is preventable be emphasized. They also wanted women to be aware that they, too, are at risk for CRC. In combination, these findings suggest that those who likely view themselves as responsible for the content of the intervention prioritize information regarding risk and prevention. That is, the emphasis is on ensuring that African Americans are aware of the extent of their risk and opportunities to reduce it. Much of this interest appears to stem from of prior lack of knowledge—participants expressed surprise at several of the facts associated with CRC and CRC screening. This lack of knowledge indicates that any CS-promotion intervention should be accompanied by key facts that clarify both relative risk and risk-reduction strategies.
Potential recipients of barbershop/salon-based CRC screening interventions appear to be expressly concerned with the practical elements associated with its delivery, such as the method by which the information is delivered, and by whom. Both the barbershop patrons in Holt et al.’s (2009) focus groups and the salon clients in the present study indicated that print material, such as pamphlets containing information that the barber/stylist can expound on, would be a good approach. Both also expressed interest in information that they can follow-up on, such as a telephone number to call for more information or for accessing services, as well as a firm belief that barbers/stylists need to be properly trained in order to be perceived as credible. In fact, in a quote strikingly similar to one highlighted in our results, one of Holt’s barbershop patrons is cited as having said,
If he’s going to educate us and you’re going to train him to educate us, give him some kind of credentials he can hang on his wall. I mean, give him some kind of credentials that he can display to say I’ve been through the UAB Program and I’m qualified to speak to you about colon cancer and that will add some credibility to it. (p. 220)
Clearly, patrons want explicit confirmation that the barber/stylist delivering the intervention has been properly vetted as a health educator. What the literature has yet to achieve consensus on, however, is how much education would be required, and for what level of intervention. Reports have ranged from 2.5 (Fraser et al., 2009) to 10 hours (Luque et al., 2011) to train barbers and 4 hours of initial training for salon stylists (Sadler et al., 2011; Wilson et al., 2008). More research is needed to determine the optimal amount of training required to produce efficacious results, as well as if and how that might vary based on intervention parameters. Clarifying the content of the training is also crucial, particularly in cases where there might be varying recommendations regarding the target health behavior. Such is the case with CRC screening among African Americans. Although CRC screening is generally recommended to begin at age 50, some recommend that African Americans start screening earlier, at age 45, due to increased risk (Rex et al., 2017). Barbers/stylists would need to be aware of these alternate recommendations and of how to best address clients’ related questions or concerns. It also points to the fact that barbers and stylists will need to be aware that their African American clients aged 45 to 49 years would also appropriate targets for the promotion of CRC screening.
In addition to relevant facts, the content of barber/stylist training might also need to include some guidance on the overall style of presentation. Salon clients in our study noted that some stylists do not communicate in a professional manner or exude characteristics that would encourage one to take heed to their message. As a result, even if armed with the requisite knowledge and proof of credentials, some stylists might lack efficacy due solely to their interpersonal communication style. Consistent with this perspective, Releford et al. (2010) advise that having staff that are engaged and understand the importance of being cordial and accommodating are essential to a successful barbershop-based health promotion intervention.
Aside from a professional demeanor, salon clients in our study mentioned no other stylist characteristics that would influence their receptivity to a stylist-delivered intervention. This was the case even though we specifically inquired about stylists’ age, sex, and race/ethnicity as potential moderators. Although these possibilities were not endorsed by salon clients, it is still possible that they would influence outcomes and should therefore be explored when implementing any barbershop- or salon-based intervention. Barbers’/stylists’ age might be especially relevant with screening-related health promotion efforts. Those who are younger than the recommended age for screening might hold less sway given that they would have no personal screening experience to draw on. That said, it is noteworthy that personal experience with CS was not mentioned as a stylist-related factor that would influence clients’ receptivity. One might expect that, among stylists who are of age for CS, clients would prefer that the stylist has “practiced what they preach” by having undergone CS himself or herself. Most previous barbershop- and salon-based health promotion interventions have not indicated if or how barbers’/stylists’ own relevant health behavior plays a role. Holt et al. (2009), however, did find that the men in their study said that if the barbers were also cancer survivors, it would increase their credibility. It would be wise for investigators evaluating barbershop- or salon-based health promotion interventions to assess potential barber/stylist-related moderators. This should include those specific to the health target, such as the barbers’/stylists’ own adherence to the recommended health behavior, as well as interpersonal factors such as the clients’ perception of the barbers’/stylists’ professionalism. Length of acquaintanceship between the barber/stylist and client would also be helpful in demonstrating proof-of-concept, as the trust between barbers/stylists and their clients is believed to be an important mechanism of effect in barbershop and salon health promotion efforts.
Interestingly, participants in Holt et al.’s (2009) study mentioned barriers to screening such as fear, lack of symptoms (which leads to lower perceived need for screening), and the notion that CRC screening is violating, whereas participants in our study did not consistently mention any of these concerns. Although this could reflect gender-related differences in core concerns about screening—for example, the notion that CRC screening is violating might reflect a male homophobic response to colonoscopy—it might also be an artifact of our focus group procedure. Specifically, we did not explicitly ask participants about barriers to CS, and the lack of such a cue might explain why many of the barriers commonly noted in others studies—such as fear, bowel preparation protocols, and infrequent primary care visits/opportunities for referral (Bromley, May, Federer, Spiegel, & van Oijen, 2015)—were not mentioned. It is important to note, however, that the one barrier that did naturally emerge in our discussion was insurance, which was mentioned by salon clients. This not only underscores their emphasis on practical considerations but also the fact insurance remains a priority issue within the community. Barbershop and salon-based interventions should be sure to include resources for accessing the touted health behavior or service. Providing as many of the tools needed for individuals to actually engage in the recommended health behavior is a crucial component that should be considered a “best practice” for all health promotion interventions, particularly those focused on health behavior change and that target disparity populations for which access is a common barrier.
The present study yielded many instructive findings but is not without its limitations. It is not clear if the findings will generalize to other geographic areas. This includes other areas of New York City. Whereas much of the Black population residing in Central Harlem identifies as African American, many from other areas of the city are of Afro-Caribbean heritage. As a result, they might have different beliefs, concerns, and informational needs regarding CRC and CRC screening. Another potential limitation is that our sample of salon clients included women younger than the age of 50 years. This was a decision made in the inclusive spirit of community-based participatory research, but it also potentially skews interpretation of how acceptable a CS-promotion intervention will be among the actual intended targets. However, the fact that the mean age of salon clients in our sample was 46.8 years indicates that many were indeed close in age to be CS-eligible, particularly given that some recommend that African Americans begin screening at age 45 (e.g., Rex et al., 2017). Had we confined participation of salon clients to those either 45 or 50 years of age and older, then it would have enabled us to stratify clients based on whether they had already been referred for or undergone CS. This could understandably influence perceived acceptability of a salon-based CS promotion. Finally, there were several questions that were not asked in the focus groups that would have offered further insight regarding potential intervention content. For example, specific questions regarding barriers to screening and the role of primary care physicians in individuals’ screening decisions would have been particularly instructive.
Despite these limitations, the present study still represents an important addition to the literature regarding salon-based health promotion interventions. To our knowledge, it is the first to establish that CRC and CS are acceptable topics to discuss in the salon setting. Lessons learned from this focus group study suggest that a maximally acceptable intervention of this type would possess the following features:
Succinct print material could be used as the primary source of health education information, which can be discussed and elaborated on through discussion with the salon stylist.
Specific points to emphasize should include the disproportionate burden of CRC among African Americans, the fact that CRC affects women as well as men, and the fact that CRC can be prevented with routine CS.
Provided information should include resources detailing where and how individuals can obtain CS, regardless of their current insurance status.
Care should be taken in selecting and training salon staff members who deliver the intervention. In particular, staff persons who exude professionalism and knowledgeability should be priority selections, perhaps even over considerations regarding the stylist’s age and/or gender.
Stylists who complete training should receive some form of visible attestation to their qualifications, which would give clients a sense of confidence in the accuracy of the information that they share and greater context for why they are doing so.
Ongoing support and resources should be provided to stylists even after successful completion of training. Stylists recognize that there will be limits to what they know and will be able to provide to their clients. The resources should be available both the stylists themselves, such as access to persons who can guide them on how to handle emergent situations, as well as to clients, who might want to know where or how to obtain more information.
Implications for Theory, Policy, and/or Practice
The above guidelines provide fertile ground for the development of an efficacious, highly acceptable salon-based intervention to promote CS among African American women. Such an intervention has the potential to reach a sizeable number and cross-section of women, including those who either may or may not yet be connected to primary care. Ironically, among African Americans, both groups are at risk for not receiving information about and/or referral for CRC screening. Persons not connected to primary care are especially vulnerable given that physician referral is known to be a major determinant of CRC screening adherence among African Americans (Wong, Bloomfield, Crookes, & Jandorf, 2013); however, even among those connected to care, recent findings indicate that African Americans are less likely than Whites to get a recommendation for CRC screening (Coleman-Wallace, Baltrus, Wallace, Blumenthal, & Rust, 2013). Consequently, Coleman-Wallace et al. (2013) suggest that efforts to overcome racial disparities in screening extend beyond physicians to trusted members of the African American community. A salon-based intervention to promote CS among African American women would be highly responsive to this call. It reflects an opportunity to mobilize communities to promote CS among African American women, as well as a culturally informed approach to reaching a disparity population. If successful, an intervention of this nature could lead to the elimination of extant CRC disparities among women and lay the groundwork for future studies to explore other health topics that can effectively utilize the salon model.
Footnotes
Acknowledgements
The authors would like to thank the Central Harlem beauty salon owners, stylists, and patrons for their thoughtful and valuable input during the study focus group interviews.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a subaward from the National Cancer Institute (Grant Number U54 CA132378) and by NIH Cancer Center Support Grant P30 CA008748-48.