
Abstract
Background. Substance use, particularly injection drug use, continues to fuel the HIV/HCV (hepatitis C virus) epidemics in San Juan, Puerto Rico (PR). Aim. This article examines individual and sociostructural factors that affect HIV/HCV risk among people who use drugs (PWUD) living with or at risk for HIV/HCV in San Juan, PR. Findings were used to inform a community-level intervention to enhance HIV care access and retention for this population. Method. A rapid ethnographic assessment in collaboration with a community-based organization was conducted. Data collection took place between June and December 2013 and included field observations, 49 unstructured interviews with PWUD, and 19 key informant interviews with community stakeholders. Fieldnotes, photographs, and interview transcripts were analyzed for recurrent themes and to address the intervention-planning needs. Study results are presented as fieldnote excerpts, direct quotes from interviews, and photographs. Results. Findings suggest that PWUD in PR face myriad challenges that affect HIV/HCV risk and hinder linkage to and retention in care. Results describe a layered risk environment where PWUD encounter many barriers to prevention, care, and treatment such as transience, social isolation, stigma, limited housing options, and inadequate medical and substance use disorder treatment services. Discussion. These observed circumstances provide an empirical basis for the development and evaluation of comprehensive interventions that may serve to reduce barriers to care and link individuals to other supportive services. Conclusion. New approaches and comprehensive interventions are needed to break the structures that perpetuate risk and lack of engagement and retention in HIV care and substance use disorder treatment in San Juan.
For the past three decades, injection drug use (IDU) has been deemed a “public health emergency,” and the principal driver of the HIV epidemic in Puerto Rico (PR; Centers for Disease Control and Prevention, 2009; Mino, Deren, & Colón, 2011; Puerto Rico Department of Health [PRDH], 2017). Since the beginning of the epidemic, PR, and particularly the San Juan Metropolitan Statistical Area (MSA), has historically been the only U.S. state/territory where IDU is the main route of transmission for most HIV cases (43%), followed by heterosexual transmission (29%) and men who have sex with men transmission (20%; PRDH, 2017). In 2014, PR ranked sixth in HIV prevalence and ninth in its AIDS diagnosis rate among adults and adolescents ≥13 years, compared with other U.S. states (Centers for Disease Control and Prevention, 2016). Recent unpublished data showed that of 548 people who inject drugs sampled, 11.7% (n = 64) tested positive for HIV where almost half (48.4%, n = 31) were unaware of their diagnosis (PRDH, 2015). The recent economic crisis on the island has only served to deepen the despair and associated health risks for people who use drugs (PWUD; Leff et al., 2017; Roman, 2015).
The Alliance for Research in El Barrio and Bayamón study, the most comprehensive study of HIV risk behaviors among Puerto Rican PWUD in New York City (NYC) and in San Juan, found that substance users in PR seroconverted at a rate of four times that of NYC-based PWUD (Colón et al., 2001; Mino et al., 2011; Oliver-Velez et al., 2003). HIV-infected individuals in PR were more likely to contend with mental health problems including depression (Asencio Toro, Burns, Pimentel, Sánchez Peraza, & Rivera Lugo, 2006) and were less likely to access health services and adhere to HIV treatment regimens (Finlinson et al., 1999) leading to a threefold higher death rate from HIV (Colón et al., 2006; Robles, Matos, Colón, Sahai, et al., 2003). Many Puerto Ricans have migrated to NYC and other U.S. cities to access substance use disorder (SUD) treatment and other health care services; consequently, this “air-bridge” has raised questions about the accuracy of SUD and HIV prevalence rates (Deren et al., 2003; Deren et al., 2007; Deren et al., 2014; Finlinson et al., 1999; Robles, Matos, Colón, Deren, et al., 2003). Nevertheless, the San Juan MSA undoubtedly remains a critical target for increasing access to HIV and SUD treatment services.
Given the myriad of high HIV risk behavior, substance use, and inadequate health care services prominent in San Juan, a randomized controlled trial (RCT) was initiated in 2012 titled Proyecto Proveyendo Acceso a Cuidado y Tratamiento [Providing Access to Care and Treatment Project; PACTo] (U.S. National Library of Medicine, 2013). The trial employed a community-based approach to (a) identify HIV-infected PWUD who were either unaware of their HIV status or not engaged in HIV care; (b) provide direct health services through a mobile care clinic; and (c) employ patient navigators to enhance participants’ ability to engage in SUD treatment and HIV care, initiate antiretroviral therapy, and adhere to their treatment regimens. Prior to PACTo’s implementation, a rapid ethnographic assessment was conducted to inform key aspects of the intervention and participant recruitment strategy. The role of ethnography in community-based interventions is to document pertinent aspects of the target population and contextualize the local environment to inform the design, implementation, and evaluation of interventions, particularly with vulnerable populations (Garcia et al., 2015; Maher et al., 2010; Messac, Ciccarone, Draine, & Bourgois, 2013; Needle et al., 2003; Schensul et al., 2009; Trickett & Pequegnat, 2005). The ethnographic observations and in-depth interviews conducted prior to the start of the RCT served to better understand individual and sociostructural factors that affect HIV risk behavior, prevention practices, and treatment (non)adherence in the study population (Carlson, Wang, Siegal, Falck, & Guo, 1994; Semaan, Lauby, & Liebman, 2002).
This ethnography was informed by the “risk environment” (RE) framework, which seeks to examine the types of environment (physical, social, economic, and political), levels (micro, macro), and mechanisms (susceptibility and vulnerability) of environmental influence that increase the chances of drug-related harm (Rhodes, 2002). Using RE as a heuristic analytical framework, we sought to understand the broad range of factors in San Juan that might shape risk for HIV-infected PWUD in targeted areas. The results portray a uniquely layered RE and explain how and why access to prevention, care, and treatment remain significant challenges for PWUD in San Juan. We discuss the ethnographic findings within the context of the RE framework and its applications to the intervention component of the larger study with policy and programmatic implications.
Method
The ethnographic team was composed of two Latina, bilingual researchers: An experienced qualitative researcher of Puerto Rican heritage with a doctorate degree in sociology (DH) and a junior researcher of Dominican descent with a master’s degree in social work and 5 years of experience working with vulnerable populations (YF). The team collaborated with the study’s community partner, Iniciativa Comunitaria de Investigación, Inc. (ICI), a local community-based organization recognized for providing comprehensive services to underserved populations living with or at risk for HIV. With 25 years of experience, ICI has served thousands of Puerto Ricans through (a) counseling and HIV testing, (b) primary care services, (c) preventive case management, (d) detox and SUD treatment, and (e) syringe exchange (the first in PR). ICI served as a key gatekeeper by facilitating access to relevant field sites and community members during the ethnographic assessment.
Field Observations
Between June and August 2013, the ethnographic team logged over 120 collective hours of field observations. They accompanied ICI staff members on syringe exchange routes to shooting galleries and attended overnight community outreach activities that involved providing food, clothing, and wound care to homeless PWUD. The ICI staff person assigned to this project (FT-C) provided key insights as a practitioner with academic training in anthropology. Acting as a broker between the ethnographers and the target populations, he helped make linkages to eligible participants, provided entry into venues that would otherwise be out-of-reach to the study team, and helped translate and interpret experiences in the field. During site visits, DH and YF observed social interactions and contextual facets of life for PWUD living with or at-risk for HIV/HCV (hepatitis C virus). Field observations were captured in descriptive fieldnotes written within 24 hours of site visits with regular jottings captured in transit while en route to other sites. While in the field, the ethnographers obtained verbal consent to take photographs of the surroundings (e.g., shooting galleries) and of individuals’ physical features related to substance use and other health issues (e.g., abscesses and wounds). Identifiable features (e.g., tattoos) were not captured.
Interviews With PWUD
Between June and August 2013, the ethnographic team had over 150 encounters and conducted 49 unstructured interviews with members of the target population—PWUD living with or at risk for HIV/HCV located in the study’s designated catchment areas (see Figure 1). They had repeated encounters with many participants as the syringe exchange and community outreach routes frequented the same venues. In some cases, the community partner introduced the ethnographers to particular participants, while natural conversations in the field occurred with others. The ethnographers asked participants about facilitators and barriers to obtaining health care services, their substance use and HIV risk behaviors, and individual-level and social factors that contribute to lack of treatment adherence for themselves and other PWUD. These informal interviews lasted approximately 15 to 20 minutes and were summarized in the fieldnotes (Creswell, 2012; Emerson, Fretz, & Shaw, 2011; Schensul, Schensul, LeCompte, 1999). The majority of participants were males between 24 and 55 years of age.
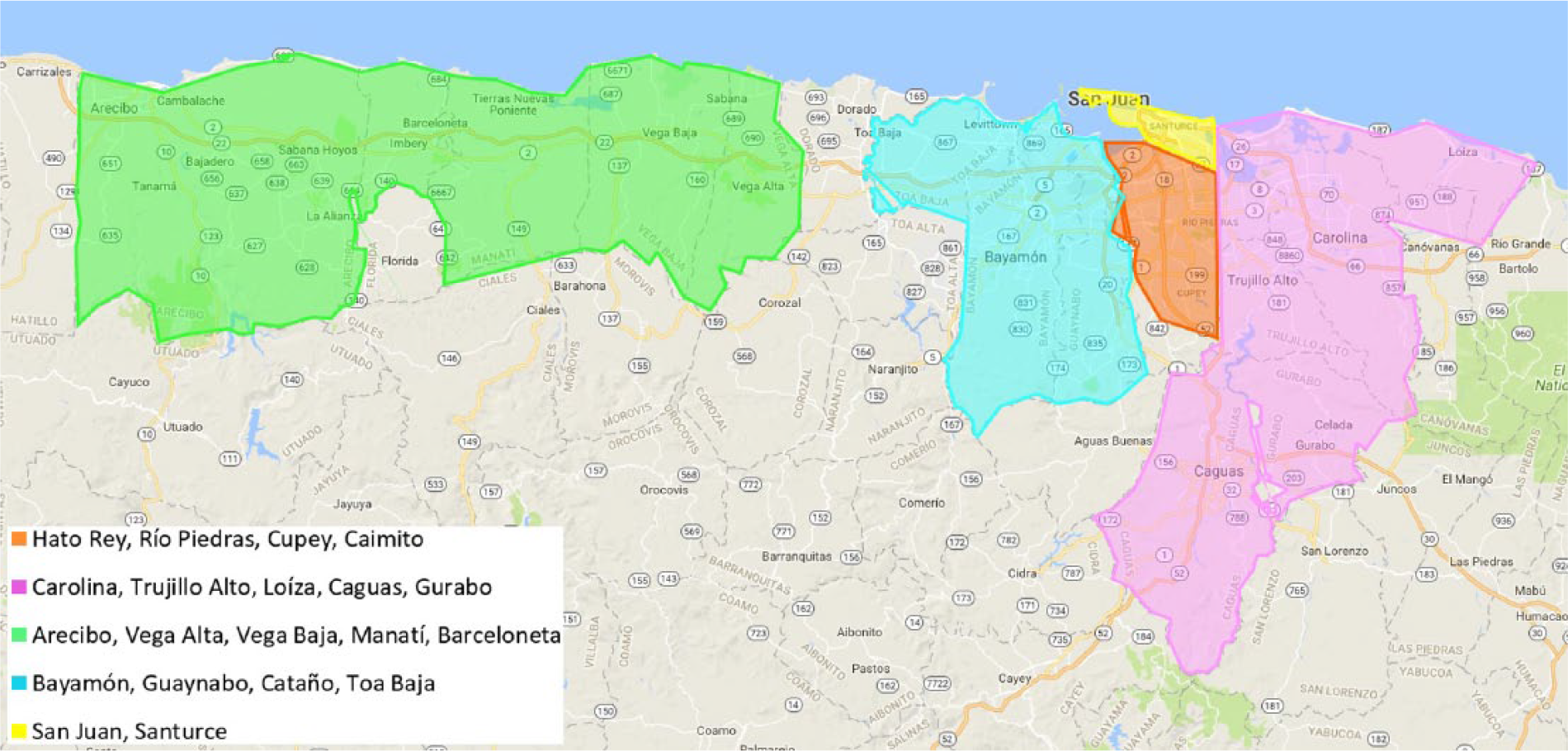
Map of designated study areas in the San Juan metropolitan statistical area.
Key Informant Interviews
Between July and December 2013, the ethnographic team also conducted 19 key informant interviews with HIV/substance use researchers (n = 4), community-based health and social service providers (n = 7), and health department personnel and policy makers (n = 8) knowledgeable about the target population. Participants were identified by study team members and through Internet searches of relevant agencies. The research staff invited them by e-mail and followed-up by telephone to schedule the in-person interview at the participant’s office or a quiet public space. Interviews were conducted in Spanish or English based on the informant’s preference. The interview guide consisted of questions covering health issues affecting the target population, HIV, the health care system, types of substance use, SUD treatment, and other pertinent issues. The respondents were actively probed for clarity and asked to expand on ideas beyond planned questions. Interviews lasted approximately 60 minutes, were audio-recorded, and professionally transcribed.
Ethics and Informed Consent
Institutional review boards at Columbia University, Weill Cornell Medicine, University of Miami, and the University of Puerto Rico approved this study. Verbal consent was obtained during interviews and field encounters. Pseudonyms are used in this article to protect the anonymity of participants.
Data Analysis
Fieldnotes, photographs, interview summary notes, and transcripts were compiled in ATLAS.ti (Version 6.0) and systematically coded and analyzed to assess thematic patterns and contextual dynamics in the data. During the initial coding phase, ethnographic team members (DH and YF) and an undergraduate research assistant (DG) reviewed the data, derived codes based on emergent themes, and applied these codes to pertinent data segments. A second round of coding by the team focused on identifying recurring themes and addressing the RCT planning needs. In this phase, two domains surfaced: (a) the social ecology of substance use and HIV/HCV risk and (b) key barriers to HIV/HCV prevention, care, and treatment. Study findings are organized by these two primary areas with relevant subsections and presented in the form of illustrative excerpts from ethnographic fieldnotes, direct quotes from interviews and photographs from the field.
Results
San Juan: A Layered Risk Environment for Substance Use and HIV/HCV
The firm grip of substance use in the San Juan MSA is hard to escape as its facets are ubiquitously interwoven into elements of everyday life on the island. La Cura [The Cure] is a commonly used term among residents that refers to copping drugs. As we learned, the characteristics of drugs used in PR are unique and their health and social consequences are often complex and dire.
La Cura: When the Risk Is the Cure
Sitting at his desk in the shooting gallery, Gelo prepared a hit of xylazine, a horse sedative and/or heroin substitute unique to the island, for his next “patient” (Reyes et al., 2012; Torruella, 2011). The informal interview began by DH and Gelo talking about their mutual love of salsa. Then, as if on cue, they sang the chorus to a 1980s salsa classic:
Amargura, señores que a veces me da, la cura resulta más mala que la enfermedad. [Bitterness, gentlemen that sometimes I feel, the cure is worse than the disease.]
Legendary salsa singer Frankie Ruiz’s song titled La Cura put a rhythmic beat to a social and cultural phenomenon that continues to fuel the HIV epidemic in PR today: injection drug use. The icon’s fate? Substance use followed by HIV-related death. For many Puerto Rican people who inject drugs, curándose [curing oneself] still comes at a grave cost.
Gelo, a longtime substance user and shooting gallery administrator in his 50s, explained why Puerto Ricans call copping drugs, La Cura:
It’s because the body craves the drugs and when people start feeling the symptoms of withdrawal they start to feel sick and the drugs cure that feeling.
We often heard PWUD describe La Cura as a priority, an urgent matter—“me tengo que curar” [I have to cure myself]. At $3 to $5 per hit, they cured themselves an average of seven times per day—a figure reported by most of the syringe exchange clients we encountered in the field and consistent with the literature (Finlinson et al., 2006; Reyes et al., 2012). As consumers of adulterated narcotics, many Puerto Rican PWUD use xylazinein addition to or in lieu of heroin (Reyes et al., 2012; Torruella, 2011). The xylazine “cure” results in physical deterioration when the syringe injecting the drug ruptures the skin to penetrate the veins resulting in bodily lesions and subsequent scars (see Figure 2).

Lesions on the skin, the physical evidence of injection drug use with xylazine.
Beyond the physical, La Cura was also associated with other harms such as homelessness, HIV and HCV infection, fractured social and institutional ties, and stigma. A homeless substance user panhandling at a busy intersection in Condado (an affluent and touristic neighborhood in San Juan) summarized this reality with a telling sign (see Figure 3). The seemingly disparate lives of Frankie Ruiz (the singer) and Gelo (the shooting gallery “administrator”) suggest that substance use affects Puerto Ricans of all socioeconomic backgrounds. This was evident in the shooting galleries and puntos [drug-dealing spots] and throughout our fieldwork where los usuarios [substance users] became known to us as the sisters, fathers, coworkers, and church parishioners at the shooting gallery in “El Guano” or outside the local bakery in Trujillo Alto. During the day, they washed windshields at the traffic light and slept under the highway at night. Helping DH make sense of this, Gelo explained,
Drugs do not discriminate. . . . I service doctors and lawyers in the upper echelons of society and “el guardia” [the police officer/security guard] that comes in to get their fix.
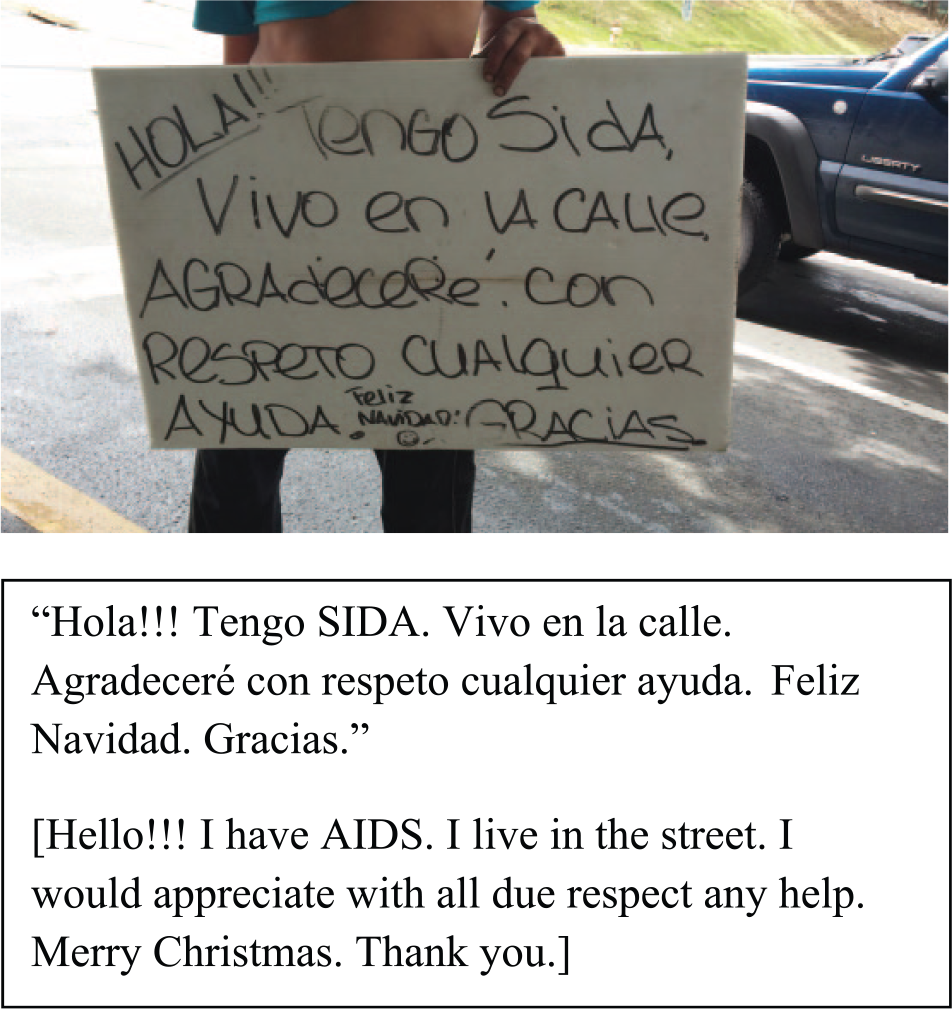
“A cry for help” through many “signs”—The message and the physical manifestations of his addiction in the form of track marks and abscesses.
Nevertheless, some distinctions were made between casual users and addicts:
I met a man in his mid-30s who smiled generously and spoke to me in English. He said he worked at [a luxury hotel]. He admitted to casual drug use but made a distinction between his habit and that of “addicts.” He wasn’t homeless, nor jobless; he was physically in shape and seemingly in control. Many others had passed that threshold and were deeply ingrained in the drug subculture. (YF fieldnote)
We learned that people take on various roles in the drug market economy. Some people sold, while others used; and at times, it was just a matter of time before a seller became a user:
Carlos bleakly described the options for people growing up in Vega Baja. He said some sell drugs or engage in drug-related crimes and others succumb to use. He pointed out a former schoolmate who was also 26 years-old and making his way up the hill to the shooting gallery. In an interesting parallel, he described his former engagement with firearms, crime and selling drugs and said that he stopped 3 years ago once his child was born. Carlos is fortunate to have found steady employment as a driver and he also runs a small trucking business. He noted that some people relapse into the drug lifestyle if they find themselves “broke.” (DH fieldnote)
Involvement in the drug market economy was only one driver of substance use. Other structural drivers were related to poverty, education, employment and housing, as well as a broader political history of colonialism and PR’s commonwealth status vis-à-vis the United Status.
Homelessness and Social Dislocation Among PWUD
Homelessness and social dislocation were regularly intertwined with substance use. Some participants described homelessness as a main driver of substance use, while others noted how the downward spiral caused by using led to homelessness. The transience caused by the loss of contact with service organizations and distance from sources of social support also had significant implications. In the field, ICI staff pointed out discreet places that homeless PWUD occupied:
The trained eyes and experience of ICI’s staff helped illuminate the area’s otherwise invisible population; those that found shelter under the sky. Their makeshift abodes were made from cardboard, meticulously stacked milk crates, the front gate of a pink doll house; mattresses set in the underpass of a highway, and donated blankets ironically stacked alongside storefronts selling paint and expensive home décor in strip malls. (YF fieldnote)
Homelessness was a common experience among the PWUD we encountered:
Miguel is homeless and said that drugs are sometimes a function of homelessness; that is, it’s not necessarily the case that drug users are homeless but that those without homes become drug users by virtue of being on the street. He explained that there are very few shelter options and no middle ground between being housed and being on the street. (DH fieldnote)
One public health professional described the virtues of “harm reduction housing”:
“People start using drugs many times here because they’re homeless. You need to address the broader issues of housing, and not just supportive housing or transitional housing, permanent housing right off the bat, which means harm reduction housing. . . . If you take an individual who is injecting chronically in the street, and has HIV, hepatitis C, and a lot of risk behaviors—you put him in housing, a permanent housing with a lot of support, a lot will stabilize, and a lot of the risk starts coming out of not only the network but that individual and the community.”
Lack of stable housing and economic hardship also produced challenges for PWUD in maintaining steady ties to people, places, and services. A community-based service provider described how transience among the target population affected loss to follow-up:
“You would go visit someone and the individual; they don’t live there anymore. It seems like people change their cell phones and numbers every three months . . . [Eventually] there’s no way of reaching that individual.”
Local mobility on the island was partly attributable to shifts in the drug market where PWUD traveled to different neighborhoods in search of available and/or higher quality drugs:
Izzy, a fellow Nuyorican, explained to me that the two “puntos” in the area were shut down because there was a shipment of heroin that was seized by authorities. He said that the only drug available on the island was horse tranquilizer [xylazine]. (DH fieldnote) Jorgie explained that he travels to where the drugs are good. He usually finds out by word of mouth and will sometimes “cop” in nearby neighborhoods if the supply is not as good near where he typically stays. (YF fieldnotes)
Participants also described mobility between PR and other major cities in the mainland United States via the Puerto Rican “air-bridge” in order to access SUD treatment, procure educational and work opportunities, and maintain familial ties (Deren et al., 2007; Robles, Matos, Colón, Deren, et al., 2003):
I had a brief conversation with a friendly gentleman in his 50s who said that he had spent time in Chicago in a drug treatment facility where he successfully quit for over two years. Tonight, he was back in the shooting gallery and said he started up again shortly after returning to PR. (DH fieldnote)
Family strife, trauma, and violence were common facets of life for our participants; many encountering significant barriers to accessing institutional and social support. Familial support and communication were often described as limited or nonexistent. Many severed ties with family members because of the shame of being seen “this way,” referring to various stigmatized identities such as being a substance user, homeless, and/or HIV-positive:
The man adjusted the shirt he had just gotten from our van, buttoning the shirt, adjusting the collar and clearing his face as if to be decent for his brother on the [phone] line. [An ICI employee] passed the phone and they said hello for the first time in 9 years. They caught up asking about loved ones and their whereabouts. The brother must’ve asked him how he was doing and when he said, “fine, just running the streets.” Then the brother asked why he had not been back to Isabela (where their family is from) and he said he didn’t want them to see him with his llagas (the lesions on his skin). He adjusted his shirt some more as if to maintain his presentability and then asked for $30 via Western Union. (DH fieldnote)
HIV/HCV Risk by Drug Site, Stigma, and Shortage of Services
The conditions of exclusion, invisibility, and isolation among PWUD posed direct and indirect risks for HIV/HCV transmission and for those already infected. They also amplified challenges in seeking and maintaining care. Key sources of risk pertained to particular sites, the experience of stigma, and a shortage of health care and SUD treatment services.
Risk by Drug Site
Shooting galleries function as “hubs” that draw a wide range of actors. The venues varied in form and location from vacant houses to makeshift shacks behind parks and in open plots of land in residential communities, to tents set up in construction zones or repurposed infrastructure in utility plants. Shooting galleries are organized spaces with rules that govern conduct and roles among patrons and providers (Bourgois, 1998; Friedman et al., 2002; Robles et al., 1998). One shooting gallery “administrator,” Chela, posted her rules that emphasized cleanliness and order (see Figure 4) and made efforts to reduce harm by taking care of herself and her “clients”:
I asked Chela about her HIV status and she said that she was negative and tests regularly. She also makes sure that the conditions in her shooting gallery are sanitary to keep her clients safe. (YF fieldnote)
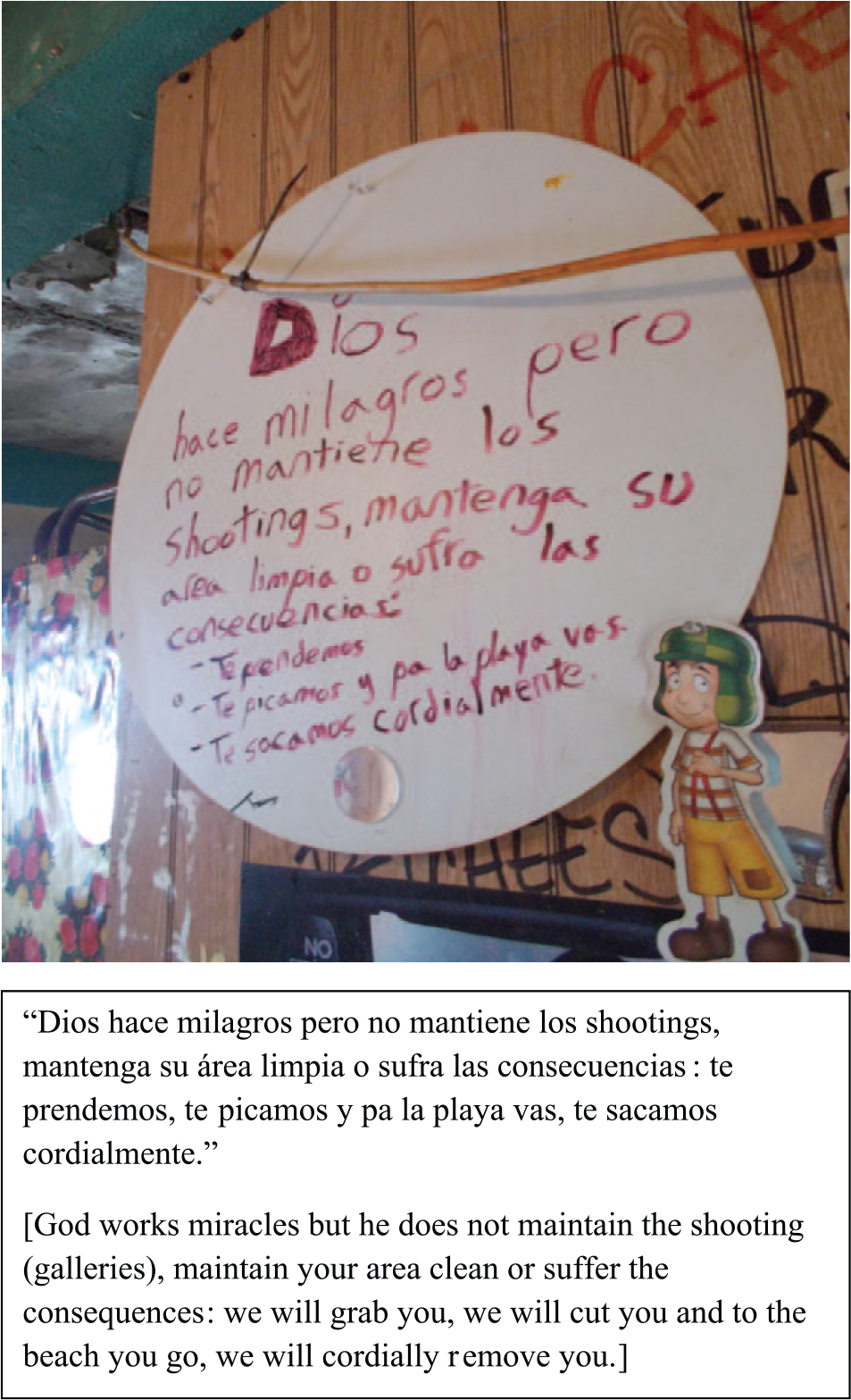
Rules posted in a shooting gallery.
Chela was afraid of needles and did not herself inject drugs. However, administrators like Gelo managed the space and provided other key services:
“I’m like a nurse or a doctor,” Gelo said, as he explained how he helps his clients prepare the drugs they will consume by “cooking” solid substances into liquid form and then he helps inject the users for a small fee—a portion of the drugs. He shares the drug paraphernalia including needles. I asked if he knows if people are sick [meaning are HIV- or HCV-positive] and he said that he usually judges by whether or not they “look healthy.” (DH fieldnote) Many of the people we encountered also admitted to sharing needles, but most did attempt to ensure that they got the first hit at the syringe. As Jesús said, “el que va después de mí, allá ellos” [whoever goes after me, that’s on them]. (YF fieldnote)
The common practice of sharing needles in shooting galleries thus increased risk of HIV/HCV transmission. Though the syringe exchange services were important in risk reduction, the risks were not completely eliminated by these efforts.
Risk by Stigma
Despite IDU being a known risk factor for HIV and HCV transmission, there was a palpable silence around the topic of HIV among those interviewed. As part of the syringe exchange outreach activities, we noted the majority of PWUD self-reporting as HCV-positive, but a mere fraction said they were HIV-positive or coinfected. Some were unaware of their status, while others were reluctant to disclose. During one field site visit, we observed a mobile unit offering free, rapid HIV tests along with educational pamphlets. Whereas on that day the harm reduction team processed several syringe exchange transactions in just over an hour, the testing team had not one patron. Though hard to generalize based on this brief observation, it was revealed in our interviews that HIV and HCV testing was infrequent among participants.
Moreover, the experience of living with HIV and HCV and not being engaged in medical care and treatment was common among participants:
In time [Gelo] disclosed that he has HIV and HCV, but has not seen a doctor in quite some time except to receive wound care at a local hospital. Shifting uncomfortably in his chair, Gelo asked me to lower my voice as I asked more questions about his HIV status and care. I did and asked if he had ever been on medication, he said “no” and explained that he did not want to be known as “sick” given his role in the shooting gallery. (DH fieldnote)
He was not alone in knowing his status and lacking care:
Bent over with a needle full of a brown liquid substance clenched by her front teeth, Anita searched diligently through mounds of litter for syringes to exchange. . . . I had a chance to speak to her and she told me she was HIV-positive, but that it had been a while since she’d been to a doctor. The daily grind of substance use had consumed her; tending to her health was not a priority by comparison. (YF fieldnote)
Substance-use–related stigma permeated medical care. One medical provider discussed his mistrust of patients based on their history of mishandling medications:
“I remember when this medication became available only to those who were sick or dying. People who had HIV that were not sick or at the end of the spectrum, they were not allowed to have the medication, so there was a big demand for black market. So the “junkies” would go out—and excuse me for using the word, sorry, it’s not derogatory, it’s just the way I was raised with that term—they used to go there, get the medication, and at the next corner, they would sell it for $10 or $20 to whoever, you know, that needed it or maybe they would sell it.”
This cynical sentiment was not lost on the PWUD we encountered, even those of known HIV-positive status. Many refused to receive regular medical attention and adhere to an HIV treatment regimen because they felt “discriminated against” and “marginalized” in clinic and hospital settings. However, there was at least one instance in which a participant described himself as virally suppressed:
Tito self-identified as HIV-positive. When I went over to inquire further, he was talking to [ICI’s resident physician] about having his numbers under control and taking meds. I eventually sat on the ground with them to ask a little more but he noted that he had had some lab work done recently and that he was all clean, “no HIV, no Hep C,” a completely clean bill of health, meaning that he was virally suppressed. (YF fieldnote)
Tito had initially been referred to services through the ICI team during their street outreach activities. Having built a rapport with ICI’s volunteer physicians, he followed up during their weekly night rounds.
Risk by Shortage of Services
The challenges with seeking and maintaining medical care as well as the lack of housing mark key service shortage areas. In addition, there were few accessible and effective SUD treatment programs available to those in need of them (Leff et al., 2017). Furthermore, the existing treatment options often lacked an evidence-based approach as explained by an upper level regional policy director:
“The faith-based or religious community who sort of lean towards providing services for the broad population of drug users do not place enough value on evidence-based practices, but rather follow a more non-scientific, spiritual [approach] that has no bearing on the outcome of care.”
Participants themselves expressed frustration with the limited SUD treatment options:
One after the next, when I asked about medical care and doctor’s visits, they instead geared the conversation to “detox narratives.” They talked about wanting to get clean and expressed a sincere frustration with the current options, often citing [religious organization’s], detox program as too short and their housing program as chaotic, making their transition difficult with the palpable presence of drugs in the environment. Costs and the difficulties completing Medicaid paperwork were also described as obstacles to enrollment. (DH fieldnote)
For PWUD, this equated to a vicious cycle of using, temporary cessation and relapse:
Pito was tired, his words and body language reflecting a sense of exhaustion. He felt trapped in this cycle—the drug dependence had taken over his life and he wanted to relinquish it. He’d tried and relapsed. He mentioned the few resources available on the island and the lack of homeless shelters and decent detox/drug treatment options. He was stuck. (DH fieldnote)
The reasons for the lack of services and loss of contact varied and were due to transience among PWUD (as previously described), the ineffectiveness of some treatment regimens, and loss of funding—especially with a worsening economy on the island.
Discussion
This ethnography of PWUD in PR describes a complex reality that serves to increase drug-related harm in this population. The present analysis provides detailed descriptions of individual and sociostructural risk factors that pose key barriers to HIV/HCV prevention and linkage to and retention in care. This article describes the embeddedness of substance use in everyday life in San Juan that has permeated cultural forms, including its music, and peppered communities with puntos, shooting galleries, and individuals in search of La Cura. Where the cure is ironically the very risk, substance use contributes to a social ecology of risk marked by homelessness, social dislocation, and the loss of familial ties while increasing risk of HIV and HCV transmission via particular sites such as shooting galleries, stigma, and the shortage of housing, medical, and SUD treatment services.
Drawing on the RE framework, this article accomplishes a main tenet of the approach, namely, to describe the nuances of risk that are situated on the social ecological basis of individual, community, and environmental contributors to harm for Puerto Rican PWUD. However, the framework is also intended to transition from REs to “enabling environments” by (a) leading to situational and structural interventions that reduce harm and (b) highlighting contextual factors that are non-drug and non-health specific that influence health and vulnerability in a broader sense. To that end, this work (a) helped inform the development of a community-level intervention and (b) points to policy and programmatic gaps.
Informing a Community-Level Intervention
The insights generated by this ethnography document common social and health care–related issues faced by the target population. Through the enhanced access and retention intervention of the RCT, we saturated the five areas of San Juan targeted by the intervention with HIV testing, linkage/reengagement, health services, and retention support services. There were two study components that were especially enriched by the ethnographic findings regarding the social and health care barriers in meeting the unique needs of PWUD in PR: Patient Navigation and the Mobile Care Clinic.
First, the Patient Navigator Linkage to HIV Care and Substance Use component used a strengths-based case management approach to provide support to HIV-infected PWUD, motivate them to attend HIV care visits, encourage their adherence to antiretroviral therapy, and assist them in overcoming any barriers to accessing social services and attendance at HIV care visits and SUD treatment. Examples of patient navigator responsibilities include linking and coordinating care with HIV care providers and SUD treatment programs, obtaining required documentation (e.g., identification cards) and completing applications/forms necessary to access health care and social services, arranging or providing transportation, and identifying sources of housing and food. Second, the Mobile Care Clinic provided basic health services (e.g., wound care and HIV rapid testing), consultations with the study nurse and physician, and referrals to social services, medical care, and SUD treatment. By focusing the efforts of the Patient Navigator and the Mobile Care Clinic on the specific barriers elucidated through our team’s ethnographic observations and interviews, the intervention was modeled to include strategies that have the most potential for securing relevant healthcare services, including HIV testing, and eventually achieving better health outcomes, for the target population.
Implications for Policy and Practice
The ethnographic findings point to several policy and programmatic measures that transcend the scope of the project, namely access to housing, SUD treatment, and primary care services in the context of worsening social, economic, and political times. Housing shortages were a key barrier to risk reduction. As noted above, homelessness is a driver of substance use, and substance use-related risk was exacerbated by lack of adequate housing options. Adoption of evidence-based approaches such as the “Housing First” model are consistent with the recommendation for “harm reduction housing” and might prove beneficial given the dearth of temporary housing options in the Puerto Rican context (Aidala et al., 2016; Padgett, Stanhope, Henwood, & Stefancic, 2011). Furthermore, detox narratives were common as participants described a desire to quell their addiction but described the lack of services as a formidable challenge. Expanding the availability of evidence-based SUD treatment can help address this gap.
Importantly, some respondents described shame and stigma as barriers to health care utilization and providers reinforced the sentiment with insensitive comments. Therefore, greater access to primary care services and HIV prevention, care, and treatment services necessitate the reduction of barriers to enrollment as well as cultural and structural competency training for providers to reduce stigma. Participants presented unaddressed medical needs ranging from skin abscesses to mental health and chronic illness. Most Puerto Rican residents qualify for state-based health insurance coverage, but lack of enrollment remains a critical issue for PWUD (Leff et al., 2017). Last, an unfortunate casualty of the economic crisis in PR has been the outmigration of professionals (i.e., medical and social service providers) and reduced support for services due to government cuts. The consequences of this crisis are still unfolding and may have grave implications for the problems highlighted herein.
Limitations
There are a number of methodological factors that could have influenced the quality of our results including, but not limited to, the abbreviated length of time in the field, the brevity of the interviews conducted with PWUD, and participants’ willingness and comfort in disclosing personal information to female researchers while in the field. Participants were encountered at outreach activities for homeless PWUD and on routes between syringe exchange programs and shooting galleries. Therefore, the findings may not be generalizable to all Puerto Rican PWUD. For example, housing may not have arisen as a major theme if the sampling approach did not target homeless PWUD. Moreover, policing/law enforcement issues and sexual risk behavior did not surface as major themes among our participants, in part because the interview guide focused primarily on substance use behavior and related risks. In general, the ICI partnership was advantageous in terms of facilitating trust and access to the population. However, being accompanied by ICI staff members could have influenced the content of the conversations with respondents. It is possible that the ethnographers missed or misinterpreted information in the field due to language and cultural barriers, despite being native Spanish-speakers of Latino Caribbean descent. We also acknowledge that the data were collected over 3 years ago and that changes on the island may affect their relevance now and in the future.
Conclusion
Despite the possible noted shortcomings, this article provides important ethnographic data to demonstrate that the multifaceted factors affecting PWUD living with or at risk for HIV/HCV in San Juan operate synergistically in a layered context of risk. The issues range from unmet needs at the individual level to social issues such as a shortage of supportive housing and a lack of evidence-based SUD treatment facilities. The insights gleaned herein were used to inform an intervention aimed at improving linkage to care for HIV-infected PWUD. As evidenced by the present findings, comprehensive approaches are needed to break the structures that perpetuate risk and lack of engagement and retention in care. If effective, the initiatives being tested should be implemented broadly in PR and beyond in order to achieve greater impact.
Footnotes
Acknowledgements
The authors gratefully acknowledge the respondents for their participation in the interviews and Greduvel Durán, MD, for his support of this study.
Authors’ Note
Data are not available for online access; however, readers who wish to gain access to the data can write to the corresponding author, Diana Hernandez, PhD, at
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Drug Abuse (R01DA035280) and the National Institute of Allergy and Infectious Diseases (P30AI073961). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies or the U.S. government.