
Abstract
Smoking and obesity are chief causes of mortality, morbidity, and medical expenditure. However, few studies have investigated the linkage between subjective obesity status and smoking behavior. This study examines whether females in a normal body mass index range who perceive themselves as obese are more likely to smoke than those who do not perceive themselves as obese. Stratifying by age-group, I employed the propensity score matching analysis to control for selection bias. Although body mass index is lower for younger females aged 20 to 39, they are more likely than elder females to consider themselves as obese. Based on a logistic regression, my findings show that younger females who perceive themselves as obese are 21.2% more likely to smoke than females who do not perceive themselves as obese. The positive relationship between perceived obesity status and smoking behavior is also found in the propensity score matching analysis. However, the disparity in smoking prevalence is not detected between elder females who perceive themselves as obese and those who do not. Public education that fosters accurate perception of body shape is imperative in inducing healthy lifestyles and improving social welfare.
As lifestyles have visibly changed in the Organisation for Economic Co-operation and Development (OECD) countries during recent decades, the obesity epidemic has become a common phenomenon in not only Western countries but also most OECD countries, including those in Asia (Sassi, Devaux, Cecchini, & Rusticelli, 2009). Although the obesity rate in Asia is quite low compared to developed countries such as the United States, the prevalence of obesity has increased in recent years (Yoon et al., 2006). The increase in the obesity rate has coincided with rapid economic growth in the past few decades in Korea and other Asian countries. In Korea, the prevalence of obesity has grown from 26.0% in 1998 to 31.1% in 2007-2009 (Rhee, Park, Kim, & Woo, 2013).
Obesity has emerged as a cause of many chronic diseases such as heart disease, musculoskeletal disorders, high blood pressure, type 2 diabetes, and cancers (Bray, 2004; Wyatt, Winters, & Dubbert, 2006). The stigmatization of obesity has led to mental health problems (Abbas, Salameh, Nasser, Nasser, & Godin, 2015; Schmalz & Colistra, 2016; Xiang & An, 2015). Obese individuals are highly stigmatized and suffer from multiple prejudices because of their weight (Brownell, Puhl, Schwartz, & Rudd, 2005; Puhl & Brownell, 2001). The mass media have produced a widespread debilitating stigma against obesity and contributed to the admiration of thinness (Heuer, McClure, & Puhl, 2011). The mass media characterize obese individuals as being lazy, physically unattractive (Chambliss, Finley, & Blair, 2004), weak-willed, unreliable, and foolish (Melo, Farias, Kovacs, & Damascena, 2014). The stigma harms females more than males (Brady, 2016).
The consequences of the stigma against obese individuals might affect smoking behaviors. Prior research suggests that some smokers, particularly women, make no attempt to stop smoking because they fear weight gain (Caan et al., 1996). Meta-analyses by the Surgeon General’s 1990 report concluded that smoking appears to contribute to reducing body weight because smoking burns calories and because nicotine is an appetite suppressant. Several studies report that smoking is used as a means of reducing weight, especially among females (Chou, Grossman, & Saffer, 2004; Sanchez-Johnsen, Spring, Sommerfeld, & Fitzgibbon, 2005; Ward, Klesges, & Vander Weg, 2001).
Since smoking and obesity are chief causes of mortality and morbidity (Leigh & Schembri, 2004; Mokdad, Marks, Stroup, & Gerberding, 2004) as well as medical expenditures (Sturm, 2002), it is beneficial to investigate the linkage between obesity and smoking. However, few studies have examined the linkage between subjective obesity status and smoking behavior. Females who are not actually obese may be more likely to smoke if they perceive themselves as obese. Therefore, I investigated the smoking behavior of Korean females in the normal body mass index (BMI) range by separating them into two groups: those who think they are of normal weight and those who perceive themselves as obese. In addition, I tested if the linkage between subjective obesity status and smoking behavior differs by age-group. It is known that the multiple forms of the stigma regarding obesity are more common in younger age-groups (Puhl & Heuer, 2009).
Data and Method
The Korean National Health and Nutrition Examination Survey (KNHANES) is a series of cross-sectional surveys with a stratified geographic cluster probability sampling design that selects representative samples of the noninstitutionalized Korean population. KNHANES is conducted to evaluate the health and nutritional status of Koreans according to Article 16 of the National Health Promotion Act. The prepared statistics are designed by the government based on Article 17 of the Statistics Act. In addition, KNHANES produces statistics regarding smoking, drinking, and obesity requested by the World Health Organization (WHO) and OECD.
In this study, I tested if one’s false self-perception of her obesity status is associated with actual smoking and if this phenomenon is different among age-groups. To investigate the hypotheses, I pooled the most recent data of KNHANES from the years 2009 to 2013. Following the WHO guidelines (Sturm, 2002), I calculated BMI as weight in kilograms divided by height in meters squared (kg/m2). Each individual’s height and weight, as well as other measurements, were checked by experts such as nurses and nutritionists for KNHANES.
Based on the BMI classification of the WHO guidelines (Sturm, 2002), the participants were limited to nonpregnant females aged 20 to 59 whose BMI is in the normal range from 18.5 to 24.9. After excluding observations with missing information, 8,040 participants were investigated. I used the statistical software STATA 13 for the empirical analysis.
I analyzed the effects of subjective obesity status on smoking behavior with the following equation:

where Smokingi is a dichotomous variable equal to 1 if the subject is currently smoking, and 0 otherwise.
The equation for testing the hypothesis could be investigated with logistic regression. However, the regression results may suffer from selection bias, which arises because a subjective belief about obesity status may not be randomly assigned for each female. For example, females who are pessimistic might be more likely to smoke as well as perceive themselves as obese.
I applied a propensity score matching (PSM) analysis as an alternative empirical approach, which widely applies for situations where one has a treatment, a group of treated individuals, and a group of untreated individuals when the treatment is not randomly assigned (Rosenbaum & Rubin, 1983). I applied three commonly used PSM algorithms—radius, kernel, and stratification—to contrast the outcome of treated individuals with that of the comparison group members (Cameron & Trivedi, 2005). Caliendo and Kopeinig (2008) reported more details about the PSM and algorithms.
The lists of the variables contained in Equation (1) are presented in Table 1. Using the subjective judgment for obesity status to the question “What do you think about your body shape?” I created a dichotomous variable,
Descriptive Statistics.
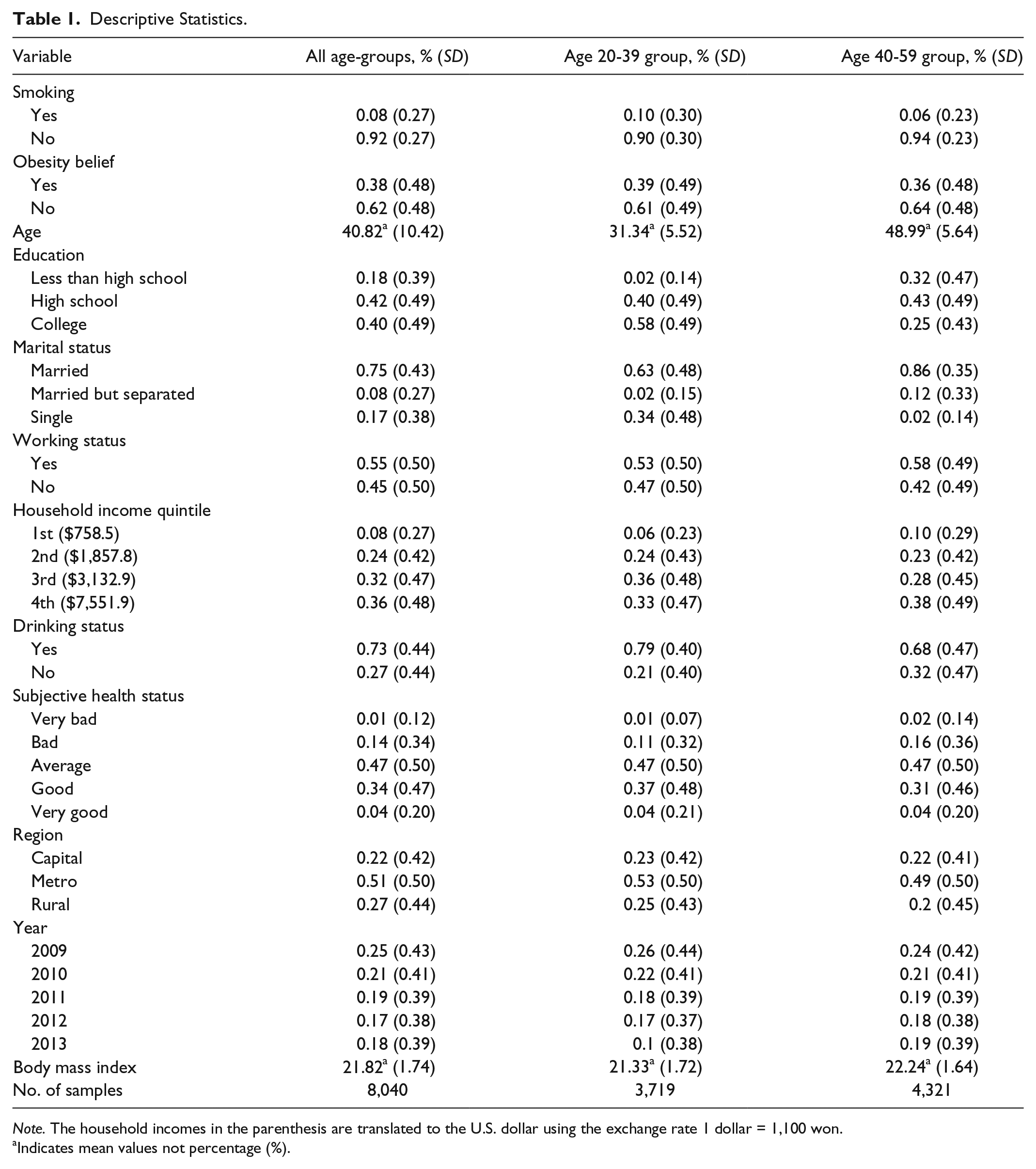
Note. The household incomes in the parenthesis are translated to the U.S. dollar using the exchange rate 1 dollar = 1,100 won.
Indicates mean values not percentage (%).
Following prior literatures on smoking behavior, the other variables contained in
For the consistent analysis approach between logistic and PSM models, I reported standard errors without adjusting for sample weights, clusters, and strata of the survey design because the PSM does not simultaneously allow for adjusting for them. Furthermore, there was no need to adjust for taxes because there is no regional variation, and any changes in taxes over time were captured by the year variables.
Results
Table 1 shows the descriptive statistics separately for younger females aged 20 to 39 and elder females aged 40 to 59, along with the entire female sample aged 20 to 59. According to the descriptive statistics, 37.7% of females of normal weight perceived themselves as obese. While the average BMI for the younger group was lower (21.33) than it was for the elder group (22.24), the proportion of false belief about their obesity status was higher among younger females (39.0%) compared to elder females (36.0%). Likewise, among normal-weight females, the proportions of smoking and drinking among younger females (10.1% and 79.4%, respectively) were higher than they were among elder females (5.6% and 68.0%, respectively).
Table 2 shows the logistic regression results. For convenience, the estimated coefficients from the logistic regression were converted into odds ratios (ORs) by exponentiating the estimated coefficients,
Association Between Subjective Obesity Status and Smoking Behavior by Age-Groups Using a Logit Model.
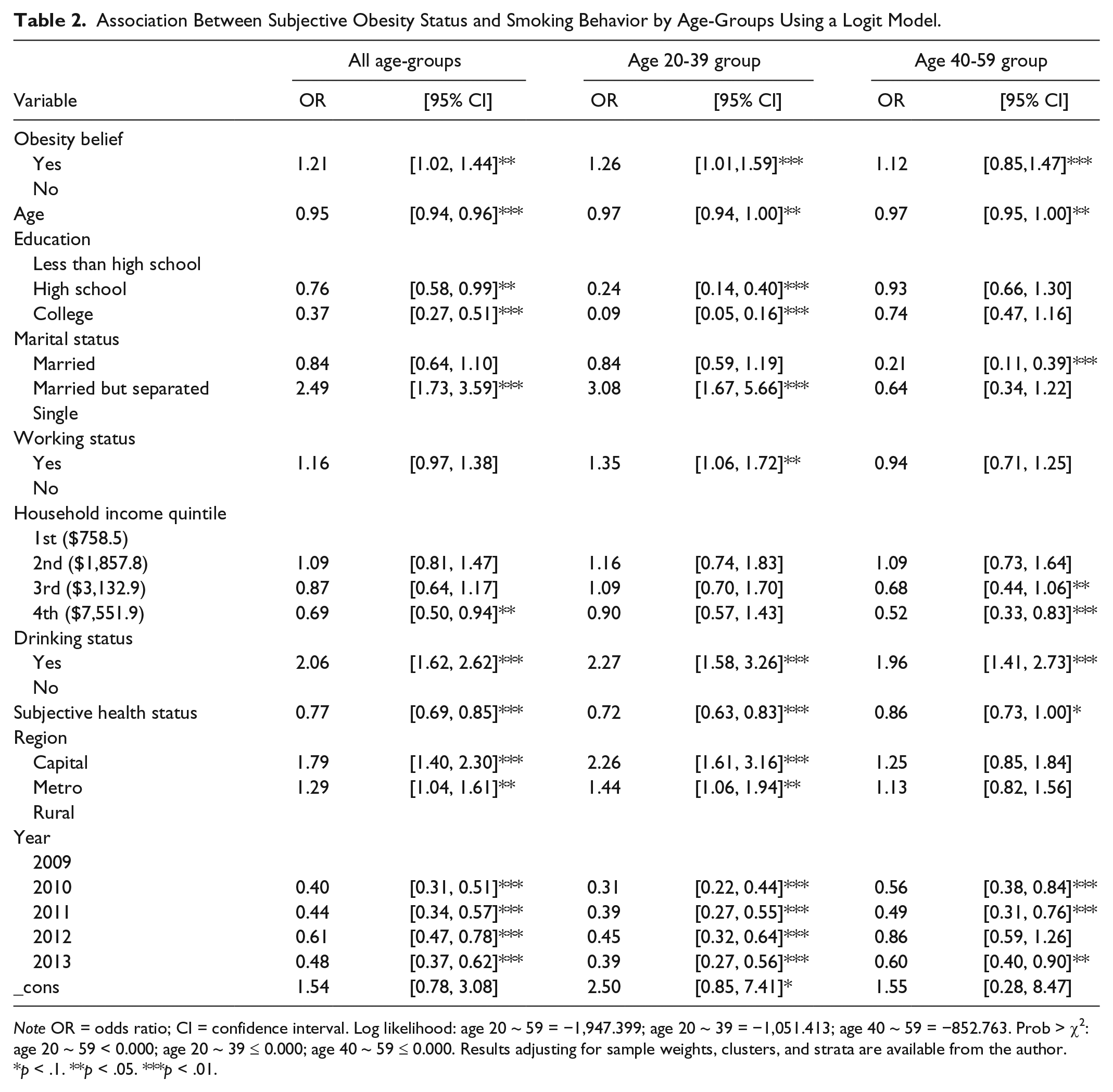
Note OR = odds ratio; CI = confidence interval. Log likelihood: age 20 ~ 59 = −1,947.399; age 20 ~ 39 = −1,051.413; age 40 ~ 59 = −852.763. Prob > χ2: age 20 ~ 59 < 0.000; age 20 ~ 39 ≤ 0.000; age 40 ~ 59 ≤ 0.000. Results adjusting for sample weights, clusters, and strata are available from the author.
p < .1. **p < .05. ***p < .01.
The PSM analysis in Table 3 reports the same results as the logistic analysis. The empirical result was consistent even for each matching method algorithm. The average treatment effect on the treated (ATT) of smoking status by subjective obesity belief was statistically significant for the entire sample as well as for the younger age-group 20 to 39 for all matching methods. The ATT values for smoking behavior among younger females differed by matching method (0.034 from radius, 0.031 from kernel, and 0.024 from stratification). Elder females who perceived themselves as obese were more likely to smoke than elder females who thought that they are nonobese, but the estimated ATT was relatively small and statistically insignificant in all the matching methods.
ATT Estimation by Age-Groups With Propensity Score Matching Methods (Nearest Neighbor, Radius, Kernel, and Stratification Matching Methods).
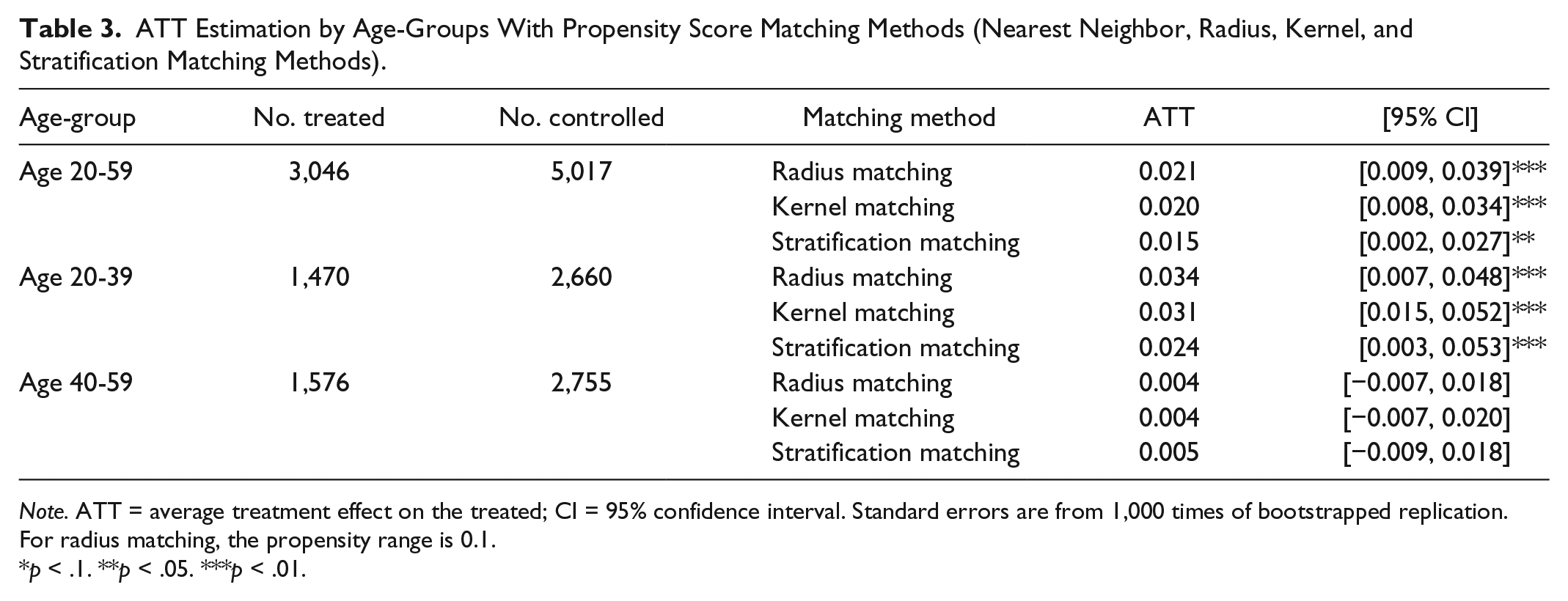
Note. ATT = average treatment effect on the treated; CI = 95% confidence interval. Standard errors are from 1,000 times of bootstrapped replication. For radius matching, the propensity range is 0.1.
p < .1. **p < .05. ***p < .01.
Discussion
Several studies have covered topics of perceived weight status and shown that children and adolescents misperceived their weight status (Sarafrazi, Hughes, Borrud, Burt, & Paulose-Ram, 2014; Shirasawa et al., 2015), and people with distorted self-perceived weight status have inadequate knowledge on the health effects of obesity (Mogre, Abedandi, & Slifu, 2014; Mogre, Mwinlenna, & Oladele, 2013). This is the first study, to my knowledge, to address the relationship between perceived obesity status and smoking behavior among nationally representative female adults who are in the normal BMI range.
The results suggest that education about the right perception of obesity status and the risks of smoking would lead to health and welfare gains because educative programs improve people’s ability to identify obesity status correctly (Pakpour, Yekaninejad, & Chen, 2011) and reduce tobacco use (Centers for Disease Control and Prevention, 2012). Thus, such educative programs would be helpful not only for preventing smoking initiation but also for reducing smoking prevalence among normal-weight females who perceive themselves as obese. Furthermore, such programs could potentially improve mental health since false perceptions of obesity status have been found to cause depression (Mamun & Cramb, 2007; Sanchez-Villegas et al., 2013). It is recommended that the targets of education for perception of obesity status should be obese people who consider themselves as nonobese as well as nonobese people who consider themselves as obese. Because some obese individuals underestimate their weight categories (Moore, Harris, & Wimberly, 2010), they would undervalue the efforts such as healthy diet and physical activities for reducing weight.
Above all, policy makers need to be educated since less than half of them in various countries do not know the extent of the obesity problems and the BMI cutoff point for obesity according to the survey study by the European Association for the Study of Obesity (2014). It is also essential to challenge common societal assumptions that perpetuate the obesity stigma because it poses numerous consequences of psychological and physical health without reducing obesity (Puhl & Heuer, 2010).
In spite of the best efforts to minimize all limitations that might creep in the course of this research, there were certain constraints within the study. This study was unable to disentangle the mechanism between subjective judgment regarding obesity status and smoking behavior. One limitation was the use of cross-sectional data. Panel data can be superior to cross-sectional data in terms of addressing the selection bias because they allow tracing how individuals change their smoking behavior when their subjective judgment regarding obesity status changes. However, under the situation of lacking panel data and considering that addictive smoking behavior rarely changes over time, applying a PSM approach for cross-sectional data would be an appropriate alternative.
Another limitation was that the standard errors in the logistic and PSM models were not adjusted for sample weights, clusters, and strata of the survey design because the PSM did not simultaneously allow for adjusting for them. However, when adjusting for sample weights, clusters, and strata in the logistic model, the results remained similar to the results before the adjustment. Nevertheless, it is possible that results in the PSM would be different when making the adjustment.
Conclusion
By addressing the effect of subjective obesity status rather than actual obesity status on smoking behavior, this study shows that young females of normal weight who perceive themselves to be obese are more likely to smoke than young females of normal weight who do not perceive themselves to be obese.
While the welfare improvement attributable to reduced obesity resulting from smoking may offset the welfare costs of smoking, as suggested by Gruber and Frakes (2006) and Rashad and Grossman (2004), smoking induced by an inaccurate judgment of obesity status among females of normal weight may cause only the welfare costs. Thus, public programs encouraging accurate body shape perception are imperative to induce healthy lifestyles and improve social welfare. In addition, persistent attempts are required to reduce the stigma against obese individuals, especially obese females.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by Dong-A University.