
Abstract
Background. There is little research on how affective reactions (e.g., stress) to perceptions of nutritious food accessibility contribute to dietary behaviors. Aims. This study explores whether stress associated with limited access to nutritious foods—termed nutrition resource stress (NRS)—contributes to diet outcomes, and whether these associations are mediated by health-related self-efficacy. Method. Using data from the cross-sectional National Cancer Institute’s Health Information National Trends Survey, analyses were conducted to examine whether reported NRS was associated with specific dietary behaviors (i.e., fewer servings of fruit/vegetables; more servings of sugar-sweetened soda; N = 3,112). Results. Analyses revealed a main association such that NRS was negatively associated with fruit/vegetable consumption (β = −0.08, p = .016). There was a negative association between NRS and self-efficacy (β = −0.11, p < .001). There was no significant association between NRS and soda consumption. Mediation analyses revealed a significant indirect association between NRS and fruit/vegetable consumption, mediated by perceived health-related self-efficacy (β = −0.03, 95% confidence interval [−.04, −.01], p < .0001). Given that self-efficacy (the mediator) was not significantly associated with soda consumption (β = 0.01, p = .912), mediation analyses were not conducted for this outcome. Conclusion. This study suggests that stress associated with perceptions of inability to access nutritious foods may influence dietary behaviors, and points to a psychological mechanism (i.e., self-efficacy) that may explain the association. In addition to improving objective barriers of access to healthy foods, future interventions might address ways of improving nutritious food–related self-efficacy or perceived stress related to obtaining healthy foods.
Limited access to nutritionally adequate food, often arising from time or financial constraint, is a burden affecting the overall health of many individuals living in poverty (Coleman-Jensen, Rabbitt, Gregory, & Singh, 2015; Franklin et al., 2012; Gucciardi, Vahabi, Norris, Del Monte, & Farnum, 2014; Gunderson, Kreider, & Pepper, 2011; Stuff et al., 2004). Survey results from the U.S. Department of Agriculture (2016) show that approximately 14% of all households had limited access to nutritious foods (defined as reduced quality, variety, or desirability of diet and/or disrupted eating patterns or reduced food intake), at some point during the year 2014 (Coleman-Jensen et al., 2015). Individuals with limited access to such foods often eat fewer daily servings of vegetables, fruits, and dairy and higher amounts of heavily processed, energy-dense foods (Fleischhacker, Evenson, Rodriguez, & Ammerman, 2010; Kant & Graubard, 2005; Leung, Epel, Ritchie, Crawford, & Laraia, 2014). Given that poor nutrition is related to many of the leading causes of death (including coronary heart disease, stroke, and many types of cancer; Bergstrom, Pisani, Tenet, Wolk, & Adami, 2001, Donaldson, 2004; Eilat-Adar, Sinai, Yosefy, & Henkin, 2013), independently and via its contributions to risk for obesity, limited access to nutritionally adequate foods has serious health consequences (Wang & Chen, 2011).
Simply being exposed to cues associated with perceived resource scarcity (e.g., news about job loss or an economic crisis), even when those cues do not relate to one’s own circumstances, can facilitate eating patterns that reflect scarcity (i.e., eating less nutritious but high-calorie foods; Laran & Salerno, 2013). Moreover, emerging evidence suggests that improving objective access to nutritious foods (e.g., by making it easier to afford nutritious foods, by reducing geographic barriers to nutritious foods) may improve dietary behaviors through perceptions rather than the improved objective access per se. Dubowitz et al. (2015) found overall net positive changes in dietary quality in a neighborhood where a new supermarket opened (via lower kilocalorie consumption from solid fats, added sugars, and alcohol). However, the only positive diet outcome that was directly associated with regular use of the new supermarket was improved perceived access to healthy food. This research suggests that the simple perception of limited access to nutritious foods may be an important predictor of dietary behaviors. The emotional component of this perception may also be important, given that perceived limited access to nutritious foods is associated with increased stress and anxiety (Whitaker, Phillips, & Orzol, 2006).
While previous research has identified a clear relationship between access to nutritious food and diet outcomes (Fleischhacker et al., 2010; Kant & Graubard, 2005; Tarasuk & Beaton, 1999), there is little research on how perceptions of nutritious food accessibility, and affective reactions to those perceptions (e.g., worry or stress), can contribute to healthy food consumption. The present study examines this specific perceived stressor—here, termed nutrition resource stress (NRS)—as a potential contributor to unhealthful dietary behaviors.
Stress associated with limited access to nutritionally adequate foods has been linked to perceived inability to take steps that would prevent disease or promote health (i.e., health-related self-efficacy; Mercille, Receveur, & Potvin, 2012; Vijayaraghavan, Jacobs, Seligman, & Fernandez, 2011). Thus, one pathway through which NRS may influence dietary consumption is through self-efficacy, given that self-efficacy is a robust predictor of health behavior change generally (Sheeran et al., 2016) and dietary consumption specifically (Guillaumie, Godin, Manderscheid, Spitz, & Muller, 2012; Kreausukon, Gellert, Lippke, & Schwarzer, 2012; Richert et al., 2010).
Here, we examined the associations of NRS with unhealthy dietary behaviors, including inadequate fruit/vegetable consumption and increased sugar-sweetened soda consumption, both of which may serve as proxies of diet behavior given that both are associated with an overall unhealthy eating pattern (Guenther et al., 2014; Vartanian, Schwartz, & Brownell, 2007). We operationalized NRS as worry or stress about the ability to purchase nutritious foods. In addition, we statistically controlled for general worry and socioeconomic status (income, education) to capture variance uniquely associated with perceptions of, and stress associated with, inaccessibility. Because an individual’s objective level of access to nutritious foods was not measured in the survey used here, it should be noted that income and education served as proxy indicators of actual access to nutritious foods, given the association between socioeconomic status and physical access and ability to afford healthy foods (Smoyer-Tomic et al., 2008). We predicted that NRS would be associated with consuming fewer servings of fruits/vegetables, as well as with consuming more servings of soda, predicting unique variance in self-reported dietary behaviors, above and beyond more objective predictors of limited access to nutritious foods (i.e., income, education), general worry, and sociodemographic predictors. We also examined health-related self-efficacy as a potential mediating factor that could explain an association between NRS and unhealthy dietary behaviors. We predicted that self-efficacy would significantly mediate the association between NRS and less healthy dietary behaviors (i.e., lower fruit/vegetable consumption, greater soda consumption), consistent with the hypothesis that self-efficacy is one psychological mechanism by which perceptions of food accessibility could influence dietary outcomes.
Method
Data Source
Data were obtained from the National Cancer Institute’s Health Information National Trends Survey 4 (HINTS 4, Cycle 1). HINTS is a nationally representative, cross-sectional survey of civilian, noninstitutionalized adults in the United States. Available in both English and Spanish, the survey was designed to monitor changes in cancer-related health communication, knowledge, and behavior. HINTS was reviewed and approved by the National Cancer Institute’s Special Studies Institutional Review Board, Westat’s Institutional Review Board, and the U.S. Government’s Office of Management and Budget.
Details regarding survey development, design and methodology are summarized in the HINTS 4: Cycle 1 Methodology Report (Westat, 2012).
In brief, the sampling frame was a database of nonvacant residential addresses in the United States. To ensure adequate representation, high–racial/ethnic minority areas were oversampled. Subsequently, a sample of adults within the selected households was asked to complete the survey. Self-administered questionnaires were distributed between October 2011 and February 2012. The protocol for mailing questionnaires involved the initial survey mailing, followed by a reminder card mailing and up to three additional survey mailings if necessary. The survey had a response rate of 36.7%, which resulted in a total of 3,959 survey respondents (Rutten et al., 2012). However, among all variables included in the present analyses (including sociodemographic and control variables), responses of “refuse” or “don’t know” as well as data entries that were clearly reporting errors were removed. The resulting sample size for the current study was 3,112 participants, although analyses had varying sizes due to differential patterns of missing data on the outcome variables.
Measures
HINTS items, including those employed in these analyses, have been adapted from various existing national health surveys (e.g., the National Health Interview Survey–Cancer Supplement and the Behavioral Risk Factor Surveillance System) and have been fielded over multiple iterations of HINTS since 2003. All HINTS items undergo extensive cognitive testing prior to being included in the HINTS surveys.
Nutrition Resource Stress
The main predictor variable in all analyses was NRS, which was measured with a single item: “How often in the past 12 months would you say you were worried or stressed about having enough money to buy nutritious meals?” Response options were 1 (always), 2 (usually), 3 (sometimes), 4 (rarely), and 5 (never). Responses were reverse coded so that higher scores indicated greater NRS.
Self-Efficacy
A single item assessed health-related self-efficacy by asking participants, “Overall, how confident are you about your ability to take good care of your health?” Possible answers were 1 (completely confident), 2 (very confident), 3 (somewhat confident), 4 (a little confident), and 5 (not confident at all). This item was reverse coded for analyses so that higher scores indicated greater self-efficacy. Consistent with previous HINTS work (Cha et al., 2014; Chen & Feeley, 2014; Kershaw et al., 2015; Ritter & Lorig, 2014; Rutten et al., 2016) and other research on self-efficacy (McCusker et al., 2016; Nesoff, Dunkle, & Lang, 2016), we treated this item as a continuous variable.
Fruit/Vegetable Consumption
Two survey items were combined to measure fruit/vegetable consumption. Participants were asked, “About how many cups of fruit [or vegetables] do you eat or drink each day?” Possible responses included 0 (none), 1 (≤½ cup), 2 (½-1 cup), 3 (1 cup-2 cups), 4 (2-3 cups), 5 (3-4 cups), and 6 (≥4 cups). The HINTS survey provided standard estimations of cup size for participants by indicating that “1 cup of fruit could be 1 small apple, 1 large banana, 1 large orange, 8 large strawberries, 1 medium pear, 2 large plums, 32 seedless grapes, 1 cup (8 oz.) fruit juice, ½ cup dried fruit, 1 inch-thick wedge of watermelon.” Examples were also provided for vegetables. Adding fruit and vegetable responses resulted in one variable with a score ranging from 0 to 12.
Soda Consumption
One survey item asked participants, “How much sugar-sweetened soda or pop do you usually drink each day?” Possible responses included: 0 (none), 1 (≤12 ounces [1 can]), 2 (13-24 ounces [2 cans]), 3 (25-36 ounces [3 cans]), 4 (37-48 ounces [4 cans]), and 5 (>48 ounces).
Sociodemographic and Participant Background Characteristics
Self-reported covariates included age (continuous), sex, race/ethnicity, U.S. nativity (i.e., “Were you born in the United States?”), and seeing a regular health care provider (i.e., “Not including psychiatrists and other mental health professionals, is there a particular doctor, nurse, or other health professional that you see most often?”). Using respondents’ self-reported height and weight, body mass index was calculated as weight/height (kg/m2) and also included as a covariate. Education (coded into three categories, consistent with recommendations capturing socioeconomic disadvantage by educational benchmarks that effectively delineate occupation and earnings; Almeida, Neupert, Banks, & Serido, 2005; Marks & Shinberg, 1998; Marmot, Bosma, Hemingway, Brunner, & Stansfeld, 1997) and combined household income 1 were included as proximal predictors of limited access to nutritious foods. Finally, analyses controlled for general worry, which was examined with a single item taken from a distress scale that has been fielded in all iterations of HINTS: “Over the past 2 weeks, how often have you been bothered by any of the following problems: Not being able to stop or control worrying.” Response options were 1 (nearly every day) to 4 (not at all) and were reverse coded, with higher scores indicating greater general worry.
Analyses
All analyses incorporated jackknife replicate weights to account for the complex sampling design and to yield nationally representative statistical estimates (Korn & Graubard, 1999). Analyses controlled for general worry and socioeconomic status (income, education) to capture variance uniquely associated with perceptions of, and stress associated with, inaccessibility. Analyses were also adjusted for other sociodemographic covariates, described above. 2
We first performed a series of regression analyses in SAS-callable SUDAAN 11.0 to examine the association of NRS and fruit/vegetable consumption, soda consumption, and self-efficacy. We then assessed indirect associations of NRS and fruit/vegetable consumption, 3 mediated by self-efficacy, using Stata Version 14. As indirect effects were calculated as the product of two regression coefficients, they are not normally distributed, and the resulting statistical estimations can be biased (Mallinckrodt, Abraham, Wei, & Russell, 2006). Therefore, we used a Monte Carlo simulation to generate bias-corrected confidence intervals based on the asymptotic sampling distribution of the indirect effect, using the indirect effects calculated in Stata as input (Preacher & Selig, 2012; Selig & Preacher, 2008).
Results
Descriptive Statistics
Table 1 contains the sociodemographic characteristics of the sample and descriptive statistics for predictors and outcomes, 4 weighted to yield nationally representative estimates. NRS was positively correlated with general worry (r = .39, p < .001), soda consumption (r = .13, p < .001), and body mass index (r = .09, p < .001) and negatively correlated with fruit/vegetable consumption (r = −.18, p < .001) and age (r = −.18, p < .001). A series of independent univariate weighted regressions indicated that NRS was higher among those of race/ethnicities other than non-Hispanic White (β = 0.48, p < .001) and those without a regular health care provider (β = 0.29, p < .001), lower among those with college education (β = −0.59, p < .001) and those born in the United States (β = −0.37, p = .006), and unassociated with gender (β = 0.15, p = .069). Compared to those with a household income of more than $75,000 per year, NRS was higher among those with a household income of $50,000 to $75,000 (β = 0.36, p < .001), $35,000 to $50,000 (β = 0.81, p < .001), $20,000 to $35,000 (β = 1.13, p < .001), and less than $20k (β = 1.33, p < .001) per year.
Sociodemographic Characteristics and Descriptive Statistics (N = 3112).

Note. Percentages and means were weighted to generate nationally representative estimates.
Fruit/vegetable consumption survey item responses included 0 (none), 1 (≤½1/2 cup), 2 (½-1 cup), 3 (1 cup-2 cups), 4 (2-3 cups), 5 (3-4 cups), and 6 (≥4 cups).
Main Associations
Main associations among NRS and each outcome are found in Table 2. Analyses revealed a main association such that NRS was negatively associated with fruit/vegetable consumption (β = −0.08, p = .016), after adjustment for all other sociodemographic variables in the model. There was no significant association between NRS and soda consumption (β = −0.01, p = .801). There was a negative association between NRS and self-efficacy (β = −0.11, p < .001).
Results From Multivariable Linear Regressions Modeling the Effects of Nutrition Resource Stress on Fruit/Vegetable Consumption, Soda Consumption, and Health-Related Self-Efficacy, Adjusting for Sociodemographic Covariates.
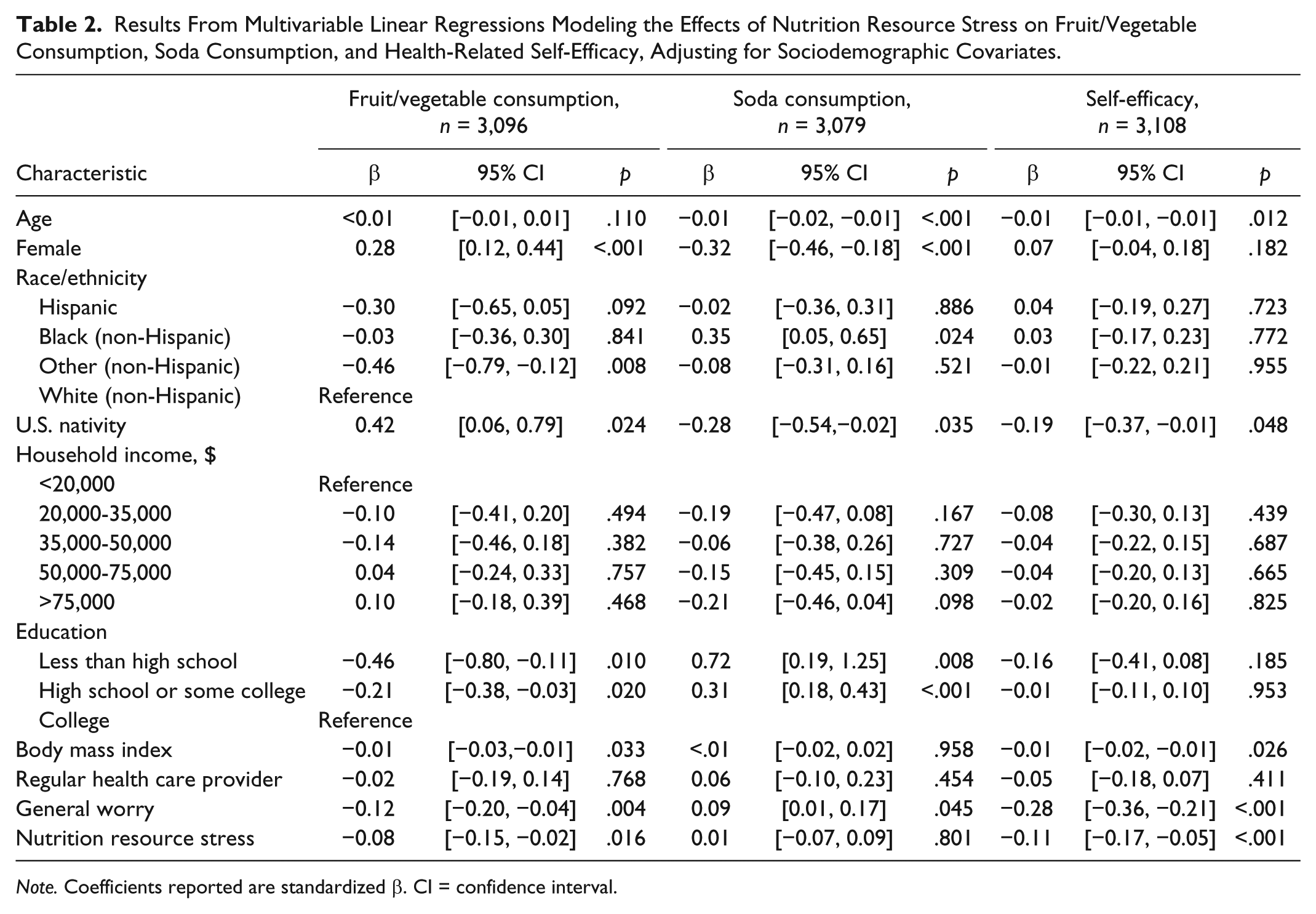
Note. Coefficients reported are standardized β. CI = confidence interval.
Mediation Analyses
There was a significant indirect association between NRS and fruit/vegetable consumption, mediated by perceived health-related self-efficacy (β = −0.03, 95% confidence interval [−0.04, −0.01], p < .0001).Given that self-efficacy (the mediator) was not significantly associated with soda consumption (β = 0.01, p = 0.912), mediation analyses were not examined for this outcome.
Discussion
An extensive body of literature has identified limited access to nutritious food as an important determinant of overall poor health (Franklin et al., 2012; Gucciardi et al., 2014; Gunderson et al., 2011; Stuff et al., 2004), via its influence on dietary consumption (Fleischhacker et al., 2010; Kant & Graubard, 2005; Leung et al., 2014). However, there is little research on how perceptions of limited access—as opposed to more objectively assessed access—are associated with dietary consumption. To that end, we examined whether an individual’s NRS—the stress associated with the perception of inaccessibility to healthy foods—contributed to unhealthy dietary behaviors, above and beyond socioeconomic status (as an indicator of financial capacity to access nutritious foods) and general worry. Moreover, we examined whether the link between NRS and dietary consumption was statistically mediated by health-related self-efficacy.
In support of our hypotheses, we found that NRS was significantly associated with fruit/vegetable consumption, even when controlling for socioeconomic factors including income and education, as well as general worry. We also found that perceived self-efficacy partially mediated the association between NRS and fruit/vegetable consumption—in line with our hypothesis that self-efficacy is one of the psychological mechanisms by which perceptions of food accessibility could influence dietary outcomes. It should be noted that although the magnitude of this indirect association is small (β = −0.03), even small effects can be clinically meaningful at the population level. Given the prevalence of individuals in the United States with limited access to nutritious foods (Coleman-Jensen et al., 2015), and the potential that perceptions may matter above and beyond actual access (Laran & Salerno, 2013), it is imperative to understand how such perceptions may predict dietary consumption. By contributing evidence in support of the hypothesis that NRS can affect behaviors that influence health outcomes, we highlighted one potential area of intervention for those individuals who feel they have limited access to healthful food. That is, in addition to enacting measures to reduce cost burden or increase availability of healthy food options (e.g., increasing availability of farmers markets or improving the quality of school lunch programming), future interventions might also target perceptions of food insecurity. For example, interventions might tackle NRS by equipping individuals with strategies to cope with the stresses associated with low socioeconomic status that might affect food affordability. Interventions targeting self-efficacy, for instance, those that increase individuals’ capacities to shop for and cook healthy meals, may also be a potential avenue for combating the potential deleterious effects of NRS, given that it statistically mediates the association between NRS and fruit/vegetable consumption. In fact, there is a great deal of evidence pointing to a lack of self-efficacy as a significant barrier to enacting healthy eating behaviors (Guillaumie et al., 2012; Kreausukon et al., 2012; Morin, Demers, Turcotte, & Mongeau, 2013; Richert et al., 2010; Sheeran et al., 2016; Woodruff & Kirby, 2013).
Contrary to predictions, we found no association between NRS and soda consumption. One potential explanation for this finding is that soda consumption is not a compensatory purchase (i.e., a less expensive substitute for a more expensive, healthier food or beverage) when individuals perceive limited access to nutritionally adequate foods, and thus may not be affected by NRS. Future research should examine whether NRS predicts consumption of an unhealthful food product more representative of a substitute purchase for fruits and vegetables (i.e., something more regularly eaten as a part of a meal and not as a “filler” or snack, e.g., frozen foods or fast foods). Another potential explanation for the finding that NRS is unassociated with soda consumption is that the survey item captures only soda consumption, rather than assessing other sugary drinks (e.g., sugary sports drinks, or flavored beverages); this may have led to an underreporting of actual sugar-sweetened beverage consumption, thereby weakening any observed association. Moreover, in our sample, soda consumption was quite low overall (M = 0.76 twelve oz. cans/day, SD = 0.95; Table 1), limiting variance that could be predicted. Indeed, research on soda consumption tends to show associations with negative health status outcomes only when soda consumption is frequent (i.e., >1 twelve oz. cans/day; Rehm, Matte, Van Wye, Yound, & Frieden, 2008).
This study had several additional limitations. First, due to the cross-sectional nature of the study, it was not possible to draw conclusions about causality among study variables. NRS may be either an outcome or a cause of inadequate fruit/vegetable consumption. Thus, while results were consistent with our hypotheses, they also highlight the importance of future longitudinal or experimental research to determine temporality and infer causality. Furthermore, responses came from self-reported data, meaning they may be susceptible to recall bias or to other inaccuracies in recording. However, note that the survey items have been adapted from screeners that correlate strongly with more objective and intensive measures of dietary consumption (Nelson et al., 2010). Because of the breadth of HINTS, there were also several limitations regarding the level of detail available in the survey items used here. First, HINTS has a limited number of items on dietary intake, and because of this, we relied on the single-item measures of fruit and vegetable consumption and soda consumption as proxies of overall diet behavior. Moreover, the data did not allow us to explore objective inaccessibility to nutritious foods in relation to NRS, beyond controlling for socioeconomic status. It would be worthwhile to investigate whether individuals who experience objective limited access to healthful foods (i.e., are unable to afford healthful foods or, due to their physical location, cannot access healthful foods), but have lower levels of NRS, do in fact exhibit better fruit/vegetable consumption. An additional limitation is that there was limited variability observed in participants’ responses to the measures of both NRS and fruit/vegetable consumption. Although individual participant scores covered the full range of response options, the limited variability of these measures nonetheless limits the generalizability of these findings.
However, these limitations are offset by a number of strengths, including the use of a large, nationally representative sample. In addition, although we rely on HINTS single-item measures, these items have been carefully selected based on performance in larger validated scales, have undergone cognitive testing prior to administration, and have been shown to perform consistently across administrations. Moreover, nationally representative surveys often rely on and publish results using single-measure items (including not only HINTS but also the National Health and Nutrition Examination Survey: https://www.cdc.gov/nchs/nhanes/index.htm, and the National Health Interview Survey: https://www.cdc.gov/nchs/nhis/index.htm; Ferrer, Bergman, & Klein, 2013; Kobayashi & Smith, 2015), and previous research has validated the use of single-item measures for constructs such as self-efficacy in research and clinical practice (Hoeppner, Kelly, Urbanoski, & Slaymaker, 2011).
Because low socioeconomic status confers multiple types of stressors—beyond stress related to limited access to nutritious foods—it will be important for future work to explore more diverse areas of stress related to low socioeconomic status to determine whether they might similarly influence health behaviors. Although these results are exploratory in nature, they do suggest that health outcomes often attributed to lack of financial resources (diet being a very common one) can in part be accounted for by stress related to the socioeconomic situation. Ultimately, our work bolsters evidence that the difficulty of obtaining nutritious foods is an issue that must be addressed, and one that can be addressed through multiple and different avenues.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jada G. Hamilton was supported by National Cancer Institute P30 CA008748.