
Abstract
An in-depth understanding of the citizen’s perception and behavior is needed for the development of targeted public policies and interventions that can successfully encourage people to shift their dietary patterns and contribute to the prevention of non-communicable diseases. The present work aimed to identify barriers and facilitators for the adoption of the new Uruguayan dietary guidelines from a citizen perspective. Twelve semistructured focus groups were conducted with a total of 91 people (81% female, age 18-64 years) from 3 Uruguayan cities. Findings identified several multifaceted barriers, including lack of value given to food, meals and cooking, taste preferences for unhealthy foods, the unsupportive social context in terms of household preferences, customs and social norms, and lack of control of the situation through insufficient food capabilities, time scarcity, and an adverse food market environment. The potential facilitators discussed in the focus groups were mainly related to policies and regulations to discourage consumption of unhealthful products and the provision of more education and information. In addition, respondents acknowledged the need for own actions in terms of seeking greater cooking skills and enjoyment, incorporating changes in their daily routines and promoting a more supportive social environment. Results suggest that supportive actions are needed to support citizen’s adoption of the new Uruguayan dietary guidelines.
Noncommunicable diseases (NCDs), such as cancer, diabetes, hypertension, and heart diseases, have major negative human, social, and economic consequences on societies (World Health Organization, 2014). According to the global NCD action plan, countries should implement high-impact, affordable interventions to cope with the increasing burden of these diseases (World Health Organization, 2013). Considering that dietary patterns are one of the causes of NCD, public policies and communication campaigns aimed at promoting healthy eating habits have been extensively recommended (World Health Organization & Food and Agriculture Organization, 2003).
One of the first steps in the design of strategies to promote healthy eating habits is the development of dietary guidelines, which are intended to establish the basics for nutrition education programs and public policies to promote healthy eating habits, as well as to provide citizens with simple information to guide their food choices toward achieving nutritional goals (Smitasiri & Uauy, 2007). Dietary guidelines translate nutrient goals into a short list of easily understandable messages, often conveyed using simple graphical representations such as a pyramid or plate image, and tailored to meet the specific needs of the population of each country (Food and Agriculture Organization of the United Nations, 2017).
Dietary guidelines should ideally consider the relationship between eating habits and the cultural, economic, and social environment (Montagnese et al., 2015). However, the impact of the food environment on people’s eating patterns as well as the importance of the way in which foods are prepared, combined and consumed, has traditionally been underestimated in the phrasing of dietary guidelines (Monteiro et al., 2015). For this reason, the new dietary guidelines of some countries point differences in the nutritional composition of fresh and industrialized products and acknowledge the importance of the way in which foods are prepared, combined, and consumed (Montagnese et al., 2015). For example, the 2014 Brazilian dietary guidelines consider the influence of foods on both physical health and emotional and psychological well-being by recognizing the biological, behavioral, cultural, socioeconomic, and environmental factors that influence dietary patterns (Ministry of Health of Brazil, 2014; Monteiro et al., 2015).
Although dietary guidelines have the potential to bring health and economic benefits to society, they have not been as effective as expected at fostering changes in eating patterns and reducing the prevalence of NCDs (Montagnese et al., 2015). A potential problem with dietary guidelines is that multiple barriers impede their implementation in citizens’ everyday life, as for example, lack of knowledge, lack of interest or lack of ability to follow the recommendations because of external factors (Brown et al., 2008).
For this reason, changing people’s eating patterns has proven to be a difficult task. Considering that food choice is a complex process influenced by several physiological, psychological, social, and environmental factors (Barker & Swift, 2009), efforts aimed at promoting the adoption of dietary guidelines should be preceded by the identification of the barriers to the adoption of the recommendations. In addition, dietary guidelines should be accompanied by and facilitated through citizen-accepted policies and actions that can support dietary behavior change (Brown et al., 2008; Zoellner, Bounds, Connell, Yadrick, & Crook, 2010). An in-depth understanding of the citizen’s perspective and behavior can provide relevant information to policy makers when deciding on the priorities to the development of public policies and interventions to encourage citizens to shift their dietary patterns and contribute to the prevention of NCDs (Worsley, 2002).
Behavior change theories acknowledge the importance of individual’s beliefs and attitudes, as well as the influence of the social and contextual variables surrounding food- and health-related behavior (Barley & Lawson, 2016). In this sense, the theory of planned behavior (Ajzen, 2002) has been identified as particularly suited for understanding consumer decisions regarding their eating patterns (Armitage & Conner, 2001). This theory encompasses three determinants of intention, which are related to the individual citizen, the social surrounding, and the environmental context the person lives in. These determinants can influence intentions and, in consequence, the behavior in either a negative or positive direction (Ajzen, 2002). The theory of planned behavior has been successfully applied to a wide range of health-related behaviors (Malek, Umberger, Makrides, & Shaojia, 2017; McEachan, Conner, Taylor, & Lawton, 2011), among others in the area of nutrition (for recent reviews, see McDermott et al., 2015; Riebl et al., 2015). Although the theory of planned behavior has not been previously used in the context of compliance with the dietary guidelines, it has been used to identify factors that hinder and facilitate the adoption of recommendations for healthy dietary habits. Examples include studying mothers’ decisions on toddler’s food intake (Spinks & Hamilton, 2016), sodium intake of heart patients (Wu, Lennie, Dunbar, Pressler & Moser, 2016), or adoption of low-fat diet (Nguyen, Otis, & Potvin, 1996) and fruit and vegetable intake (Cox et al., 1998). The theory of planned behavior provides a comprehensive model that considers the multiple factors that might hinder or facilitate the adoption of dietary guidelines in daily life. For this reason, this theory was used as a guidance framework in this study in exploring citizen perception of the dietary guidelines and identifying perceived barriers for their adoption.
Study Context
The objective of this study was to identify barriers and facilitators for the adoption of the new Uruguayan dietary guidelines from a citizen perspective and to develop suggestions for policy action.
Uruguay is located in the southeastern part of South America and shows one of the highest rates of overweight and obesity (64.9%) in Latin America (Ministerio de Salud Pública, 2015). Although accurate empirical food consumption data is not available, several studies have shown that Uruguay has undergone a rapid nutrition transition, characterized by a rapid increase in the consumption of processed foods with high sugar, fat, and salt content and a low consumption of fresh fruit and vegetables (Girona, Puyares, Saravia, Ares, & Rosano, 2016). Given that the first edition of the Uruguayan dietary guidelines, published in 2005, did not consider the contribution of processed foods to NCD (Monteiro, 2009), an update was deemed necessary to adapt their recommendations to changes in scientific knowledge on the relationship between eating habits and health (Montagnese et al., 2015). The update of the Uruguayan dietary guidelines started in 2015 and was coordinated by the Ministry of Health following the methodology proposed by Albert et al. (2007). A multisectorial committee was formed, composed of representatives of the public sector (health, social development, education, agriculture), academia, consumer groups, nongovernmental organizations, professional organizations, and international agencies (Ministerio de Salud Pública, 2016b).
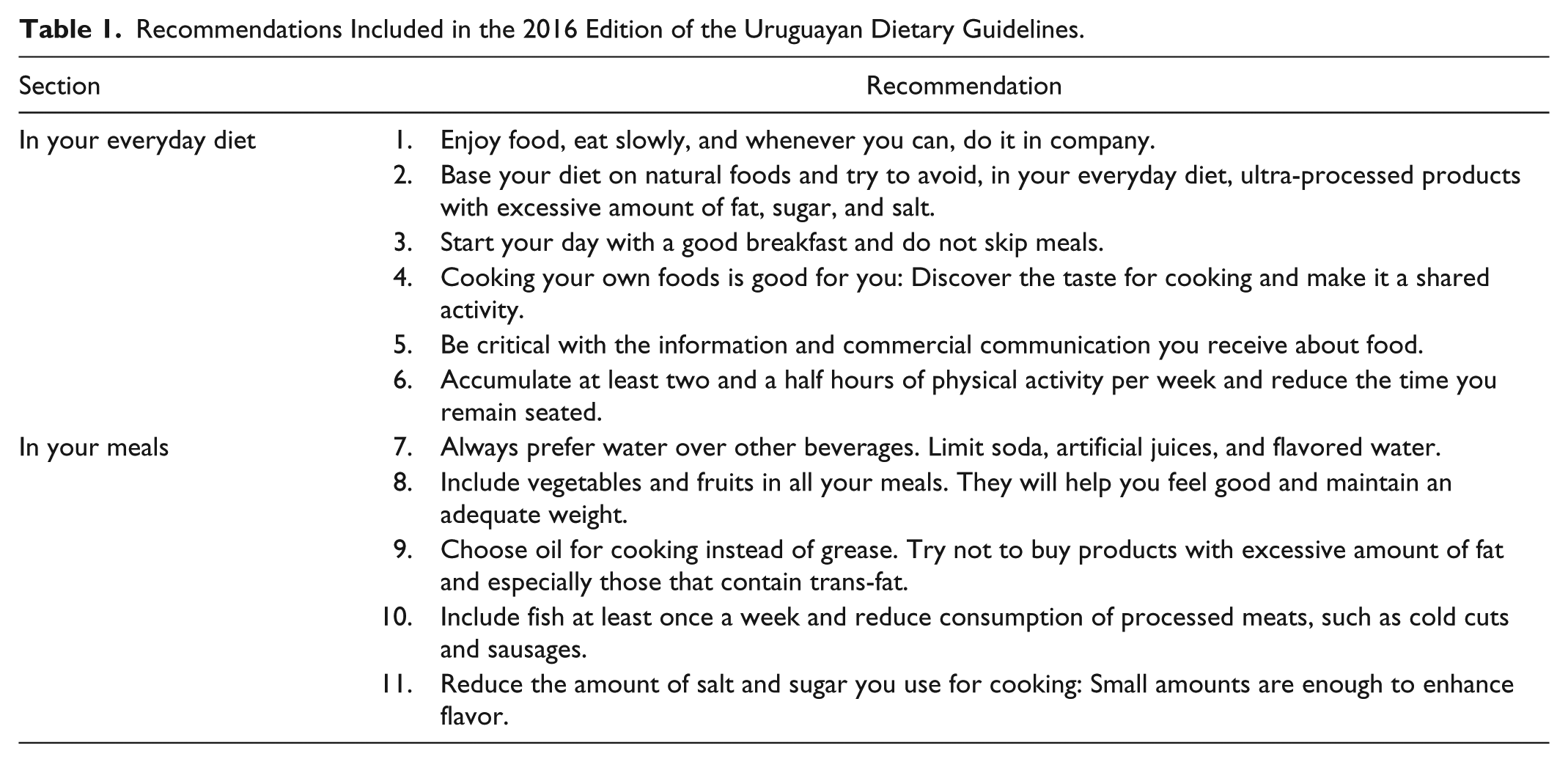
The innovative approach of the Brazilian dietary guidelines inspired the update of the Uruguayan dietary guidelines (Ministerio de Salud Pública, 2016b). The 2016 edition of the Uruguayan dietary guidelines is based on seven principles that acknowledge the importance of lifestyle and the food environment on food choice, and they emphasize the importance of consuming traditional home-made foods based on natural or minimally processed foods (Ministerio de Salud Pública, 2016a). The dietary guidelines include 11 recommendations related to food choice, ways of eating, as well as to barriers to healthy eating and physical activity (Table 1). The recommendations are sorted into two main groups: general recommendations about lifestyle and ways of eating (recommendations for “your everyday diet”) and recommendations related to the choice of specific foods (recommendations for “your meal”).
Recommendations Included in the 2016 Edition of the Uruguayan Dietary Guidelines.
To identify the citizen perspective on the new dietary guidelines, a qualitative research approach was chosen as most adequate for uncovering the “why and how” of their behavior and practices. The study was conducted between February and April 2016, before the release of the new Uruguayan dietary guidelines in September 2016. A qualitative approach was used to explore the diverse views of Uruguayan citizens. Qualitative research has been previously used for identifying barriers and potential facilitators for healthy eating (for examples, see Gough & Conner, 2006; Reyes, Klotz, & Herring, 2013; Lea, Worsley, & Crawford, 2005; Marcinow, Randall Simpson, Whiting, Jung, & Buchholz, 2017). Focus groups were selected in the present work as they allow respondents to freely express their opinions and jointly discuss their views about a specific topic, which cannot yet be observed in real life (Flick, 2009).
Method
Sample
Twelve focus groups were conducted with a total of 91 participants in three cities of Uruguay: Montevideo (the capital city), Artigas (494 km from the capital, northward), and Treinta y Tres (249 km from the capital, eastward). In each city, a total of 4 focus groups, each consisting of 5 to 10 participants, were conducted: 2 with participants with middle or high socioeconomic level and 2 with participants with low or medium socioeconomic level. Participants were recruited from databases in each city, purposively sampling an age and gender distribution adequate for the Uruguayan population. The number of focus groups was selected a priori to assure that each of the recommendations of the dietary guidelines was discussed in one group in each city and for each socioeconomic level. In addition, conducting this number of focus groups enabled to reach a point of saturation (Carlsen & Glenton, 2011). The characteristics of the participants are summarized in Table 2. Participants signed an informed consent form and received a book as a small gift for their participation. The study was approved by the Ethics Committee of Facultad de Química (Universidad de la República).
Sociodemographic Characteristics of the Participants of the Focus Groups (n = 91).
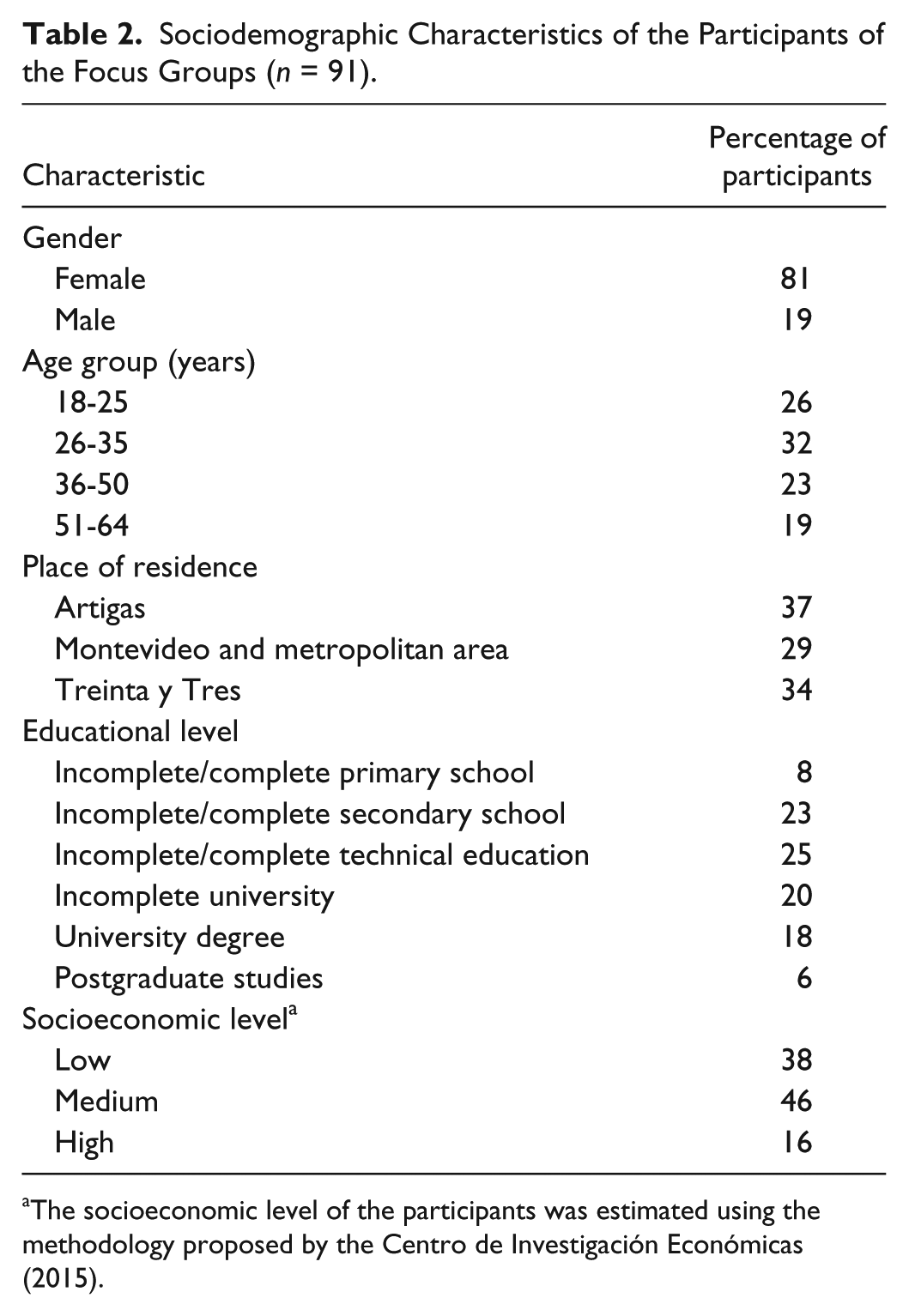
The socioeconomic level of the participants was estimated using the methodology proposed by the Centro de Investigación Económicas (2015).
Data Collection
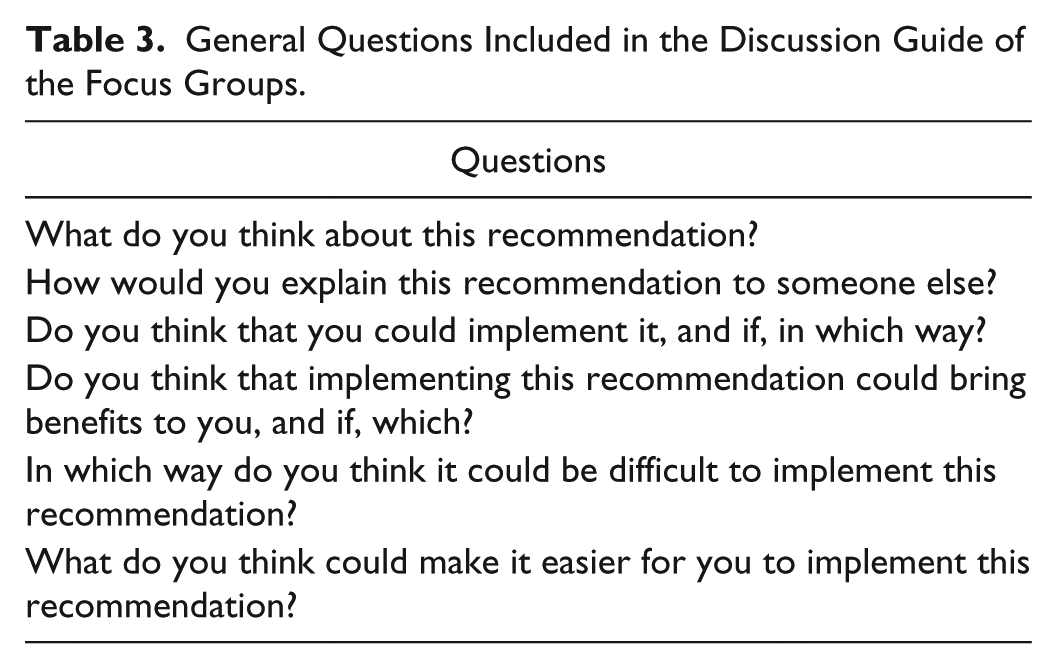
Focus groups lasted 60 to 90 minutes and were conducted by the same experienced moderator. In each city and for each socioeconomic level, the 11 messages of the dietary guidelines (Table 1) were divided into 2 groups (5 and 6 messages) and assigned to each of the 2 focus groups. This was done to allow a more in-depth discussion of each recommendation, given the overall length of the dietary guidelines. During the focus group discussion, no references to the two sections of the dietary guidelines (i.e., in your everyday diet and in your meals) were provided. The semistructured interview guide included questions related to participants’ understanding, acceptance, perceived benefits, as well as facilitators and barriers for the implementation of the recommendations. The general questions included in the discussion guide are included in Table 3. Focus group sessions were audio-recorded with participants’ consent and then transcribed.
General Questions Included in the Discussion Guide of the Focus Groups.
Data Analysis
Transcripts of the focus group discussions were analyzed in Spanish using inductive coding (Krippendorff, 2004) by one of the researchers who authored the study and verified by two additional researchers (Hennink, Hutter, & Bailey, 2011). First, interview fragments discussing barriers and facilitators for the adoption of the guidelines were identified from the transcripts. Responses to the additional questions included in the discussion guide are not included in the present work.
For each of the two main topics of the discussion, interview fragments were arranged into themes and categories, which were created as they emerged from the data when examining and reexamining the transcripts. Disagreements among the researchers were resolved through discussion until agreement about the best code was reached. Exemplar quotes within each subcategory were selected and translated from Spanish to English.
The theory of planned behavior was used in the interpretation of the barriers for the adoption of the dietary guidelines. The identified themes and categories were grouped into the three determinants of individuals’ intention to perform the behaviors included in the recommendations: attitudes, social norms and perceived behavioral control of the situation.
Results
Overall, the content of the discussion was similar in all groups and no differences were found in their responses to the questions included in the discussion guide. No apparent differences emerged between the groups carried out in the different cities or with participants from different socioeconomic levels. This indicates homogeneity in the perception of barriers of and facilitators for implementation of the dietary guidelines. Participants showed an adequate understanding of the recommendations included in the guidelines, which allowed to discuss barriers and facilitators for their adoption. In addition, participants showed a positive attitude toward all the recommendations, recognized potential positive consequences and emphasized that they would be interested in adopting the recommendations in their everyday life.
The emerging themes identified in the focus group discussions about barriers and facilitators to the adoption of the dietary guidelines, as well as examples of quotes, are shown in Tables 4 and 5, respectively, and described in detail next. Figure 1 provides a visualization of the results related to the barriers and the potential facilitators, as well as which facilitators can potentially alleviate which barrier.
Emerging Themes and Examples of Quotes Related to the Barriers to Implementing the Dietary Guidelines of the 2016 Edition of the Uruguayan Dietary Guidelines, Grouped Into the Three Determinants of Intention According to the Theory of Planned Behavior.
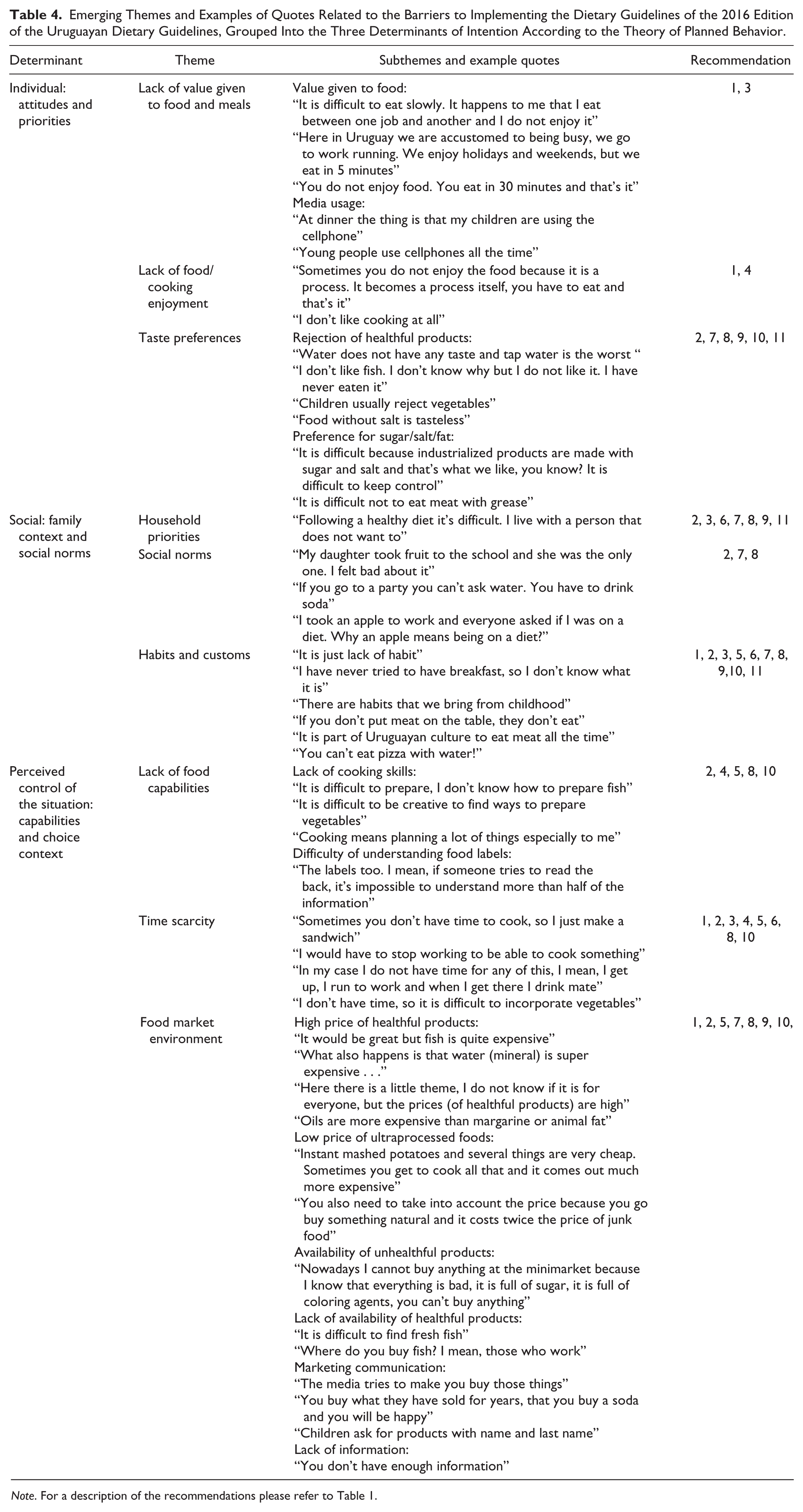
Note. For a description of the recommendations please refer to Table 1.
Emerging Themes and Examples of Quotes Related to the Facilitators for the Adoption of the Dietary Guidelines of the 2016 Edition of the Uruguayan Dietary Guidelines, Grouped According to the Respective Policy Measure.

Note. For a description of the recommendations please refer to Table 1.

Visualization of the barriers and facilitators for implementing the dietary guidelines from a citizen perspective.
Barriers to Implementing the Dietary Guidelines
Using the theoretical background of the theory of planned behavior, the barriers for the adoption of the recommendations of the dietary guidelines were sorted into three main determinants: an individual’s attitudes and priorities, the social context and norms, and perceived control of the situation in terms of capabilities and choice context. These determinants summarize various themes and subthemes that emerged from the analysis. Table 4 provides an overview of the main themes and subthemes identified in the focus group discussions, as well as a description of the recommendations for which each of the themes was mentioned.
Individual: Attitudes and Priorities
According to the respondents, a major barrier to the implementation of the recommendations of the Uruguayan dietary guidelines was related to individual attitudes and priorities with regard to food and eating habits within their lifestyle (Table 4). Respondents reported that they typically did not give value to food and meals in the way the first recommendation suggested (e.g., eating in company, switching off electronic devices). They repeatedly reported not to prioritize time for enjoying food, as they tend to invest only a few minutes for eating, or even ate while continuing to work, which prevented them from eating slowly (Recommendation 1), having breakfast and not skipping meals (Recommendation 3). Many participants stated that they did not enjoy food and cooking and that they tried to invest only limited time preparing their food, which was a major barrier for cooking from scratch (Recommendation 4).
A strong preference for products with high sugar, fat, and/or salt content or preference for flavorsome beverages over water was one of the main reasons not to follow several of the recommendations (Table 4). In addition, participants referred to their rejection for healthful foods, such as fish, as well as their dislike for products with low salt content, as barriers for changing their eating habits and following the recommendations included in the guidelines.
Social: Family Context and Social Norms
The social context was identified as another important barrier (Table 4). Some participants indicated that they found it difficult to follow a healthful diet because other people in the household prioritized certain foods and refused to eat healthful food. Family context was regarded as particularly relevant for the adoption of 7 of the 11 recommendations included in the dietary guidelines (Table 4). Participants recognized the unsupportive social norms in their social context when trying to eat healthfully in specific situations, in contrast to the norm. Social norms were regarded as a barrier to avoiding ultraprocessed foods, soda, artificial juices, and flavored water and including vegetables and fruit in all the meals. Participants also emphasized that many of their habits and customs were not in agreement with most of the recommendations of the dietary guidelines and that changing them would be a difficult task, given the culturally bound roots of the habits (Table 4). They explicitly referred to not having breakfast, frequently consuming meat, processed meat, and sweetened drinks (which, e.g., was regarded as the “must-have” company to pizza), as well as using salt while cooking.
Perceived Control of the Situation: Capabilities and Choice Context
Participants mentioned that although they enjoyed cooking at times, they felt overwhelmed by having to think about what to cook every day. The food capabilities needed for cooking seemed to lack among many participants as they recognized difficulties to plan their weekly meals as well as to cook specific products, first and foremost vegetables but also fish. Lack of cooking skills was regarded as a motivation for consuming ultraprocessed products (Table 4).
In addition, participants stated that they find it difficult to understand the information included on food labels and that, as a consequence, they did not use these labels to guide their food choices and in food handling. They explicitly referred to the difficulties in understanding nutritional information. Difficulty of understanding food labels was regarded as a major barrier to being critical with the information and commercial communications they received about food (Recommendation 5, Table 1).
Another aspect of modern lifestyle that seemed to largely influence dietary patterns was time scarcity, which was highlighted as a barrier for the majority of the recommendations (Table 4). Participants stated that they did not have time to cook or prepare healthful food, particularly vegetables, and that they thus preferred to eat ready-to-eat products, regardless of their nutritional profile. Several women emphasized that they were the main person responsible for cooking despite a part- or even full-time employment.
Several barriers related to the characteristics of the food market environment (meaning the country’s food market composition in terms of products offered, their nutritional characteristics, price levels and the information about and marketing of food) were also identified (Table 4). Participants emphasized that unhealthful products were widely available in the marketplace and that they tended to be cheaper than other more healthful options. Furthermore, marketing strategies of food companies were recognized to be a strong trigger for buying unhealthful products. Participants stated that they were unable to judge the veracity of many of the nutrient and health claims used in food marketing. Participants emphasized the role of marketing communication and advertising in the food preferences of children and recognized that children usually ask for specific brands rather than for the product itself.
In addition, lack of information played a role in hindering the adoption of the recommendations of the dietary guidelines. Many participants indicated that they lacked the information necessary to identify products with high sugar, fat, and/or salt content, or were not aware of the potential negative effect of these nutrients on their health or that of their children.
Facilitators for the Adoption of the Dietary Guidelines
The different themes discussed as potential facilitators were categorized into seven groups that represent measures that can be taken by majorly the individual (cooking enjoyment and skills, changes in the daily routine, or changes in the social environment), or by public stakeholders (education and information, regulation, information, products, or the market). Table 5 provides an overview of the themes identified in the focus groups, the barriers they could potentially overcome, and for which recommendations they were mentioned.
Information, Product, and Market Regulation
Different types of regulations were mentioned as facilitators for the adoption of the recommendations of the dietary guidelines identified in the focus group discussions (Table 5). Participants emphasized that the government should implement policies and regulations to change the food market environment or provide information. They referred to the Uruguayan anti-tobacco campaign and stated that similar coercive regulations should be implemented for unhealthful products, as for example taxes to increase their price, regulation of advertising and the inclusion of warnings on the packages. These policies would make it easier for citizens to be critical about the information they receive about food and could potentially encourage the adoption of the recommendations related to consumption of unhealthful products, such as ultraprocessed foods and soda (Table 5). Participants also stated that the government should introduce subsidies on healthful products (fruits, vegetables, and fish) and encourage food companies to reduce the salt, sugar, and fat content of their products. Regarding facilitators for increasing consumption of healthful products, participants mentioned the need to increase their availability and explicitly referred to ensuring free availability of fruits, as well as having more places where they could buy vegetables and fish close to their home (Table 5).
Education and Information
Participants also emphasized the need to increase nutrition knowledge and awareness of the relationship between food and health. Education and information campaigns were regarded as facilitators for the adoption of most of the recommendations (Table 5). Different strategies were mentioned, including public awareness campaigns in mass media, public events, television programs, and social media. The importance of implementing nutrition education programs targeted at children was highlighted.
Cooking Enjoyment and Skills
The importance of food preparation at home was also recognized as a facilitator for the implementation of several of the recommendations (Table 5). Participants emphasized that people should develop an interest for cooking and learn how to cook in order to be able to prepare healthful products, such as vegetables and fish. In addition, they recognized that if they cooked more, they would be able to reduce their consumption of ultraprocessed products, as well as their salt and sugar intake.
Changes in Daily Routines
Small changes in daily routines were also suggested as necessary to comply with several of the recommendations of the dietary guidelines (Table 5). Participants stated that changing their eating habits required being motivated and finding ways to implement the recommendations. They acknowledged the need to have a more efficiently organized daily life and routines to be able to eat healthful food and avoid last minute decisions about their meals, as well as to find simple strategies at home that allow them to enjoy meals more.
Changes in the Social Context and Environment
Changes in the social environment were also recognized as facilitators for the implementation of the recommendations (Table 5). Some participants stated that having more time, as well as a comfortable room to have lunch at work, could encourage them to eat slowly and more healthfully, as well as help them to avoid skipping meals. In addition, the importance of other people’s support for changing habits and maintaining those changes over time was also recognized. Other people interested in following the recommendations of the dietary guidelines were regarded as a facilitator for eating slowly, reducing consumption of ultraprocessed products and soda, increasing consumption of fruit and vegetables and accumulating the recommended hours of physical activity.
Discussion
Barriers for the Adoption of the Recommendations of the Dietary Guidelines
Results confirmed the existence of multifaceted barriers that hinder the adoption of the recommendations (Figure 1), in agreement with previous studies that describe a wide range of barriers to healthy eating (e.g., Rose, Bodor, Hutchinson, & Swalm, 2010; Davison, Share, Hennessy, & Stewart Knox, 2015). Although the interviewed citizens seemed to be interested in following the recommendations included in the guidelines, they described how their own attitudes and priorities, their social context and the food market environment were factors that prevented them from doing so. These barriers have been recognized by the theory of planned behavior as the main determinants of individuals’ intention to comply with health-related behaviors (Ajzen, 2002; Armitage & Conner, 2001).
Factors such as lack of value given to food, meals, and cooking, aggravated by the perceived time scarcity, can be regarded as the main characteristics of modern life style that hinder healthful eating patterns and the adoption of the recommendations of the Uruguayan dietary guidelines in particular. The perception of time scarcity impeding to meet all goals and thus having to prioritize between different goals are increasingly common in industrialized societies. Time scarcity issues have been reported to affect the way in which people purchase, prepare, and consume foods (Jabs & Devine, 2006).
As the results showed, participants’ social context largely influenced compliance with dietary recommendations. Family members, friends, and coworkers and their food preferences or the social norms enacted by them have a relevant role in constraining or facilitating healthy food choices. In the present work, participants widely acknowledged that the habits and customs resulting from their lifestyle and social context might be in disfavor of the recommendations, and that the habits and customs are difficult to change.
The lack of cooking enjoyment discussed as a barrier for reducing consumption of ultraprocessed products and increasing consumption of healthful products, such as fruit, vegetables, and fish, is closely linked to lack of cooking skills, which has been negatively associated with balanced food choices (Hartmann, Dohle, & Siegrist, 2013). Lack of food handling capabilities might be aggravated by the lack of knowledge and difficulty to interpret existing information. Overall, it also became apparent that the food market environment, an issue repeatedly discussed as a potential contributor to unhealthful choices (Glanz et al., 2016), plays a major role in hindering the adoption of the recommendations of the dietary guidelines and promoting unhealthful eating habits among Uruguayan citizens. Participants emphasized that marketing strategies, as well as the price and availability of unhealthful products, play a key role in promoting the consumption of unhealthful foods.
Facilitators for the Adoption of the Recommendations of the Dietary Guidelines
Results from the present work also identified facilitators for the adoption of the recommendations included in the dietary guidelines. The facilitating policies and actions discussed by participants are measures that can be taken by either the individual or by public stakeholders. Of the measures that respondents can implement themselves, changes in the in-home availability of fruit, vegetables, and fish, as well as working toward changes in the physical environment of work places are strategies that have previously been reported effective in modifying eating habits (Brug & Van Lenthe, 2005; Story, Neumark-Sztainer, & French, 2002).
However, other measures require the government to act to support changes in the individuals’ priorities or the social context. For example, strategies aimed at encouraging people to enjoy cooking and invest more time in preparing meals seem relevant for discouraging consumption of convenience products and improving eating habits. Overall, participants emphasized the importance of changes in the regulation of the food market environment, as for example, the need to regulate sales of unhealthful products, implement taxes on unhealthful products and subsidies on healthful products, as well as to regulate the marketing strategies of food products. The importance of these public policies to promote healthy eating has been previously recognized (Capacci et al., 2012). In particular, regulation of advertising received special attention from participants, who emphasized its importance in shifting their food choices and particularly the preferences of children.
Public awareness campaigns and the inclusion of front-of-pack nutrition information were recognized as facilitators. Such nutrition-related mass media campaigns create awareness and motivation to change attitude, which could increase likelihood to change behavior. These campaigns should not only provide nutrition knowledge, but also encourage citizens to engage in small changes in their daily routine toward more healthful habits, as highlighted by participants. Research indicates that public policies with such a social marketing aspect can be effective (Capacci et al. 2012; Aschemann-Witzel, Perez-Cueto, Niedzwiedzka, Verbeke, & Bech-Larsen, 2012). In the present study, participants did not refer to any specific campaign related to food, which can be explained considering that this type of public policy has not been common in Uruguay.
However, it should be considered that changes in lifestyle are difficult to achieve in the short term. For this reason, policies aimed at improving the nutritional profile of processed food products could contribute to an improvement in the health status of the population. Gradual reformulation strategies for decreasing the sodium and sugar content of products are already being successfully implemented in several countries (MacGregor & Hashem, 2014).
Limitations of the Study
As a limitation of the study, it has to be mentioned first that while the qualitative nature of the study provided a deep understanding of the barriers and facilitators for the adoption of the recommendations, further studies are necessary to estimate the relative importance of these barriers, or potential differences in perception between different sociodemographic segments of the population. This will allow to determine priorities for the development of a national action plan to promote the guidelines. Second, participants volunteered to participate in the study and only received a small gift for their participation, which suggests that they are more interested in food than the average Uruguayan citizen. Given that, it can be expected that the barriers might be even more pronounced in the general population, while the average Uruguayan citizen might have less ideas regarding measures that could contribute to their adoption of the recommendations, as well as less interest in the facilitators.
Implications
Strategies aimed at encouraging the adoption of the recommendations of dietary guidelines should take into account the habitual nature of eating behaviors and modify the situational cues that trigger those habits (Verplanken & Wood, 2006). The existence of several multifaceted barriers for the adoption of the recommendations of the Uruguayan dietary guidelines suggests that they are unlikely to achieve relevant changes in the eating patterns of the population unless a variety of measures of different nature is implemented (Trapp et al., 2015). The identified barriers as well as the desired facilitating actions suggest that both restrictive and informative policies are needed (Mazzocchi et al. 2015; Rothschild, 1999). Such broad and varied actions likely require a coordinated national plan and collaboration between stakeholders. The development and implementation of supportive policies, regulations and social measures are strongly needed to encourage people to change their eating habits and to create healthy environments that sustain those changes.
According to the results of the present work, the emphasis of these measures should be placed on supporting favorable attitudes and priorities, changing the social context, and modifying the food market environment. Meal and cooking enjoyment, value given to food, changes to the social norms and eating habits, lack of cooking capabilities and understanding of nutrition information despite the time scarcity are issues of particular importance, as is the reduction of availability, accessibility, and appeal of unhealthful food in favor of more healthful foods in the market environment.
Footnotes
Acknowledgements
The authors are indebted to the Food and Agriculture Organization of the United Nations for the technical assistance granted to Ministerio de Salud Pública (Uruguay) for updating the Uruguayan dietary guidelines.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.