
Abstract
Mobile applications (“apps”) designed for sexual health education have the potential to reach teens and young adults that are hard to reach through traditional platforms; however, little is known about availability of these apps and their adherence to existing guidelines. Following a search on the two major app stores, data from 2,693 apps were analyzed. Only 697 (25%) addressed sexual health, and only 15 (1%) of apps met inclusion criteria for comprehensive programs and their content was further analyzed. The content of most of these apps narrowly focused on sexually transmitted infections and pregnancy prevention and lacked information on puberty, sexual identity, and personal safety. Theoretically grounded strategies including self-efficacy and modeling behavior to strengthen behavior change efforts were largely absent. Last, we identified significant shortcomings in the literate design of these apps, including limited use of interactive features, such as videos, quizzes, or games. These findings indicate that the potential of apps as sexual health promotion tools has not yet been fully realized. We outline recommendations for developing theory- and evidence-based sexual education apps and provide suggestions for health educators on how to select relevant apps when working for youth.
The increase in sexual education programs and resources has contributed to the decline in teen pregnancy rates in the United States (Boonstra, 2014; Santelli, Duberstein Lindberg, Finer, & Singh, 2007). Despite this progress, this rate is higher than in most developed countries (United Nations Statistics Division, 2015), and risky sexual behavior remains a major cause of mortality and morbidity among teenagers, including a recent rise in sexually transmitted infection (STI) rates (Centers for Disease Control and Prevention [CDC], 2014). Research strongly supports use of comprehensive programs, which are grounded in behavior change theories and include medically accurate information on a variety of topics, approach sexuality from a positive perspective, and aim at enhancing teens’ abilities, values, and skills to internalize and implement healthy behavior (Future of Sex Education Initiative [FoSE], 2012; Kirby, 2007). Despite the extensive evidence on the effectiveness of comprehensive approaches, the format of sexual education programs available in the United States varies, and many teens lack information and skills to make healthy sexual decisions.
In addition to traditional face-to-face education, advances in communication technologies provide emergent modalities to engage adolescents in comprehensive sexual education programs. Internet-based sexual health interventions have shown success in reducing sexual risk behavior and increasing sexual health knowledge in teens by utilizing interactive and engaging functionalities, such as online games, social networking sites, and virtual environments (Bull, Pratte, Whitesell, Rietmeijer, & McFarlane, 2009; Moreno et al., 2009; Read et al., 2006). In view of the potential for reaching underserved populations, the World Health Organization stated in 2011 that mHealth, defined as use of mobile technology for health purposes, has the potential to extend Internet-based health promotion efforts (World Health Organization, 2011). Using similar interface and content principles as websites, mHealth enhances interactivity, adaptability, and accessibility in the delivery of health care services and information (Bull, 2012). In particular, mobile phone applications (apps) provide a unique platform to reach teenagers from diverse ethnic groups (Anderson, 2015). Most (73%) teenagers in the United States own a smartphone and use it to download health-related apps, with 36% of teenagers aged 13 to 18 reporting changing health behavior because of an app (Wartella, Rideout, Zupancic, Beaudoin-Ryan, & Lauricella, 2015). Similarly, three out of four college students have downloaded health and medical apps to their smartphones (Richman, Webb, Brinkley, & Martin, 2014). mHealth allows health educators to reach a broad audience, standardize material, and tailor messages to individuals (Levine, 2011).
To date, research on the use of mHealth in sexual health contexts has been limited to studies examining either pregnancy or HIV prevention apps (Chen & Mangone, 2016; Mangone, Lebrun, & Muessig, 2016; Muessig, Pike, LeGrand, & Hightow-Weidman, 2013), thus overlooking the importance of comprehensive sexual education. Research on sexuality education websites for adolescents showed a dearth of evidence-based content (Marques et al., 2015). Availability of sexual education apps (SEA) and the degree to which they feature comprehensive sexual education approaches is unknown. In view of the potential of mHealth in meeting adolescents’ need for comprehensive, evidence-based sexual health information, this study focused on analyzing the availability, design, and content of comprehensive sexual education apps (CSEA). Different standards are available to guide sexual education app developers in content creation and design. First, seven core content components of effective sexual education curricula were developed based on research evidence provided by the CDC (2012) and Kirby (2007). The National Sexuality Education Standards include (a) anatomy and physiology, (b) puberty and adolescent development, (c) identity, (d) pregnancy and reproduction, (e) STIs and human immunodeficiency virus (HIV), (f) healthy relationships, and (g) personal safety (FoSE, 2012). Additionally, the International Planned Parenthood Federation (2010) has added sexual pleasure to the list of effective sexual education components. Second, incorporating behavior change theories is pivotal in securing behavior change. Specifically, Bandura’s (1977, 1986) social learning and social cognitive theories and the theories of reasoned action and planned behavior (Ajzen & Madden, 1986; Fishbein & Ajzen, 1975) have been shown to increase health behavior change efforts in Internet-based interventions (Webb, Joseph, Yardley, & Michie, 2010), including sexual health promotion (Bailey et al., 2010). However, the degree to which app developers are adhering to these guidelines is unknown. Moreover, to reach target populations, including those experiencing health disparities, it is essential to provide information in an appropriate literacy level. Consequently, the roundtable of the Institute of Medicine (Broderick et al., 2014) produced guidelines for the design of literate mHealth including specific standards for content, organization and navigability, and interactivity.
This study provided a deeper understanding of the availability and quality of SEA available to adolescents through an in-depth analysis of evidence-based components, including behavior change theories, and health literacy principles used in CSEA. To identify the availability of SEA in general, the first research question was posed:
In view of the evidence in support of comprehensive sexual education information, the second research question aimed to identify the availability of such information.
To learn about implementation of evidence-based design of CSEA, the third and fourth research questions were posed:
As a literate design of CSEA has the potential to disseminate content to broad audiences, the fifth research question was posed:
Method
Study Design
This study provided an overview of SEA through a rigorous screening and content analysis of apps available to iOS and Android users using procedures outlined in related analyses (Chen & Mangone, 2016; Cowan et al., 2013; Mangone et al., 2016). The process resulted in identifying SEA in general and analyzing the content and design of available CSEA.
Screening Process and Final Sample Identification
To answer the first two research questions, both the Apple ITunes store and the Android Playstore were screened for relevant apps in March of 2016. Search key words included sex, reproductive, and contraceptive (Mangone et al., 2016) as well as sexuality, sexual health, sexual education, safe sex, sex and relationships, and STIs. The search resulted in a total of 2,693 suggested apps. Mangone et al. (2016) noted a limitation in app stores’ search engines that do not allow researchers to copy or extract information. To address this problem, we utilized a data scraping software (Import.io, 2015). This innovative tool allowed for a systematic screening by extracting the app title, the targeted age group, and the description of each app. Subsequently, the results for each keyword were transferred to a spreadsheet and inclusion criteria were established. Apps were included if (a) their content focused on at least one specific component of sexuality or sexual health, such as sexual pleasure or pregnancy prevention; or addressed sexuality through interactive features (games, quizzes, etc.); (b) they were in English; (c) free; (d) not developed for a specific event, such as a conference (Mangone et al., 2016); and (e) not exclusively developed for individuals outside the United States.
A total of 257 apps were identified on the ITunes store and 577 apps on the Android app store. Duplicates were eliminated, leading to a sample of 679 apps (see Figure 1). Subsequently, the 679 apps were reviewed and screened for CSEA. Inclusion criteria for this stage were (a) apps provided sexual health information on more than one topic and (b) targeted teenagers and young adults (i.e., not parents, health care providers, as described on the webpage for each app). Twenty-six apps were identified as CSEA and downloaded. Two rounds of intercoder reliability checks were conducted for 19% (n = 20) of the CSEA at both screening stages, resulting in Krippendorff’s α values of .87 (95% agreement) for identifying free apps that were in English and addressed at least one component of sexual health, and .86 (95% agreement) for identifying CSEA, representing very high reliability (Taylor & Watkinson, 2007; see Figure 2). After the download, 7 apps were excluded because their content was inconsistent with their app store description and 4 did not function, resulting in 15 apps identified as CSEA that were further analyzed.
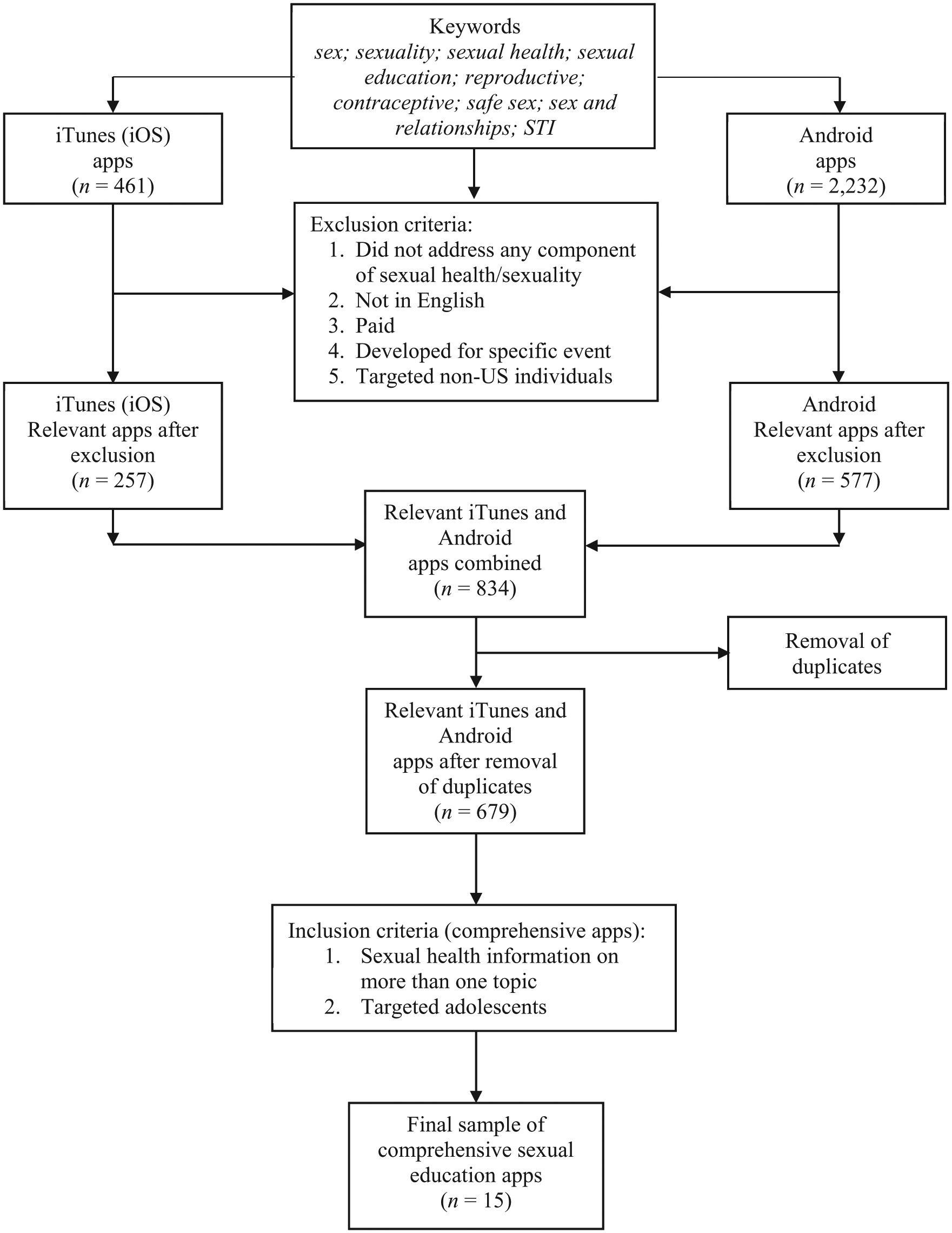
Screening process of eligible apps.
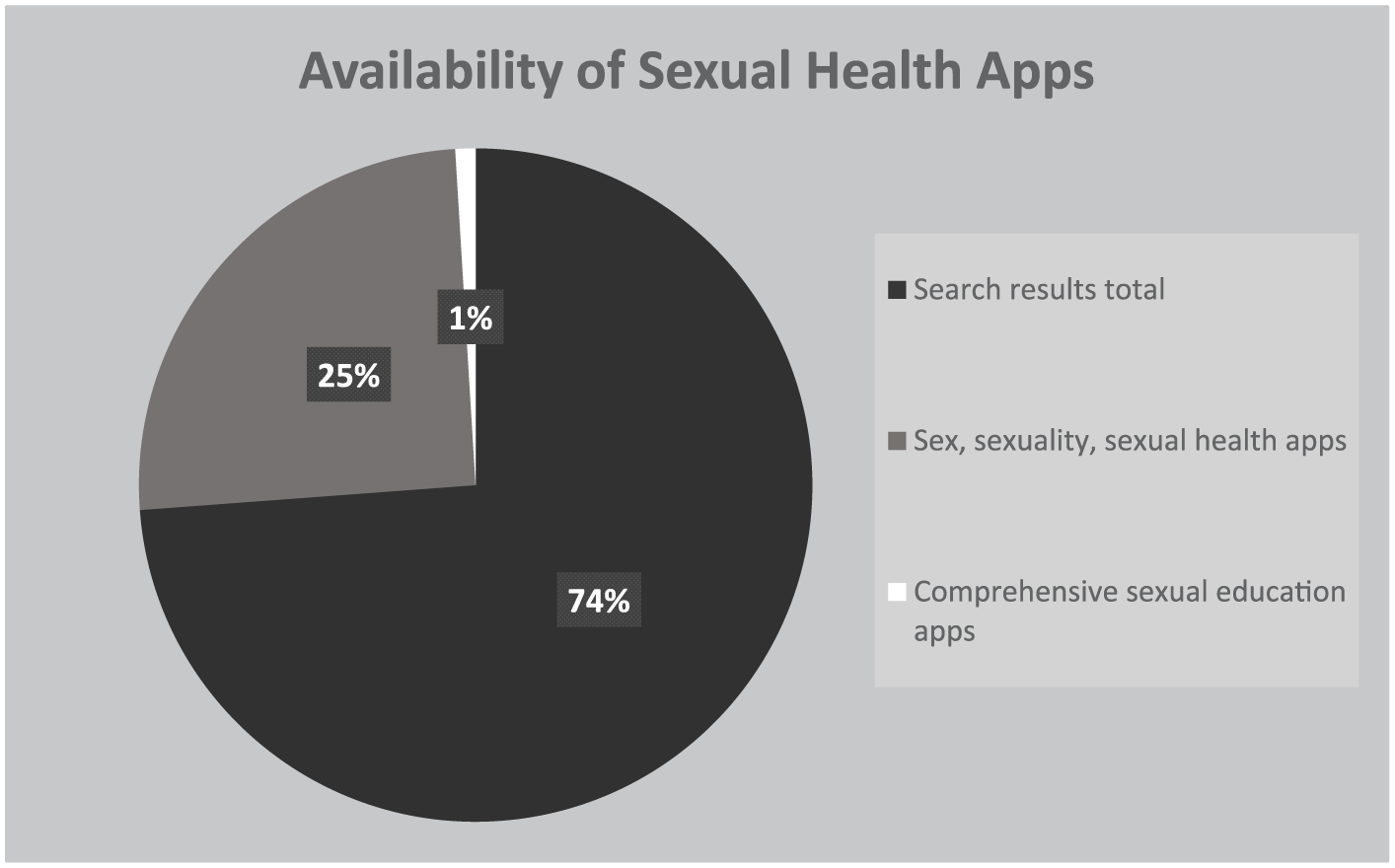
Availability of sexual education apps and comprehensive sexual education apps.
Coding Process
Two independent coders who were graduate students with previous experience of coding mHealth apps’ content including adherence to literate design were trained by the first author in two sessions of 2 hours to ensure mutual understanding of the conceptualizations of each coding item. Subsequently, the 15 CSEA were downloaded onto smartphones and coded for absence (0) and presence (1) of each coding item.
Measurement
To facilitate the coding process, a code sheet and a code book were developed (see Supplemental Appendix A). The following nine topic areas were included: (a) anatomy and physiology, (b) puberty and adolescent development, (c) identity, (d) pregnancy and reproduction, (e) STIs and HIV, (f) healthy relationships, (g) personal safety (FoSE, 2012), (h) sexual pleasure (International Planned Parenthood Federation, 2010), and (i) communication and interpersonal skills (FoSE, 2012; Kirby, 2007).
Identification of behavior change theories followed Abraham and Michie’s (2008) taxonomy of behavior change techniques (BCTs), which has frequently been used as coding scheme for the identification of behavior theories in online and mobile health interventions, including sexual health (Carswell, McCarthy, Murray, & Bailey, 2012). The six BCTs in the coding scheme included health–behavior link, health consequences, intention formation, barrier identification, modeling behavior, and self-efficacy.
Last, the Institute of Medicine guidelines (Broderick et al., 2014) were applied to assess the use of health literacy strategies following established procedures (Caburnay et al., 2015; Ginossar et al., 2017). In total, 23 health literacy strategies were included in the coding instrument, eight of which referred to the display of content, nine to the organization and navigability of the app, and six to the level of interactivity and user-engagement. The final coding instrument consisted of 38 coding items (see Supplemental Appendix A).
Interrater Reliability
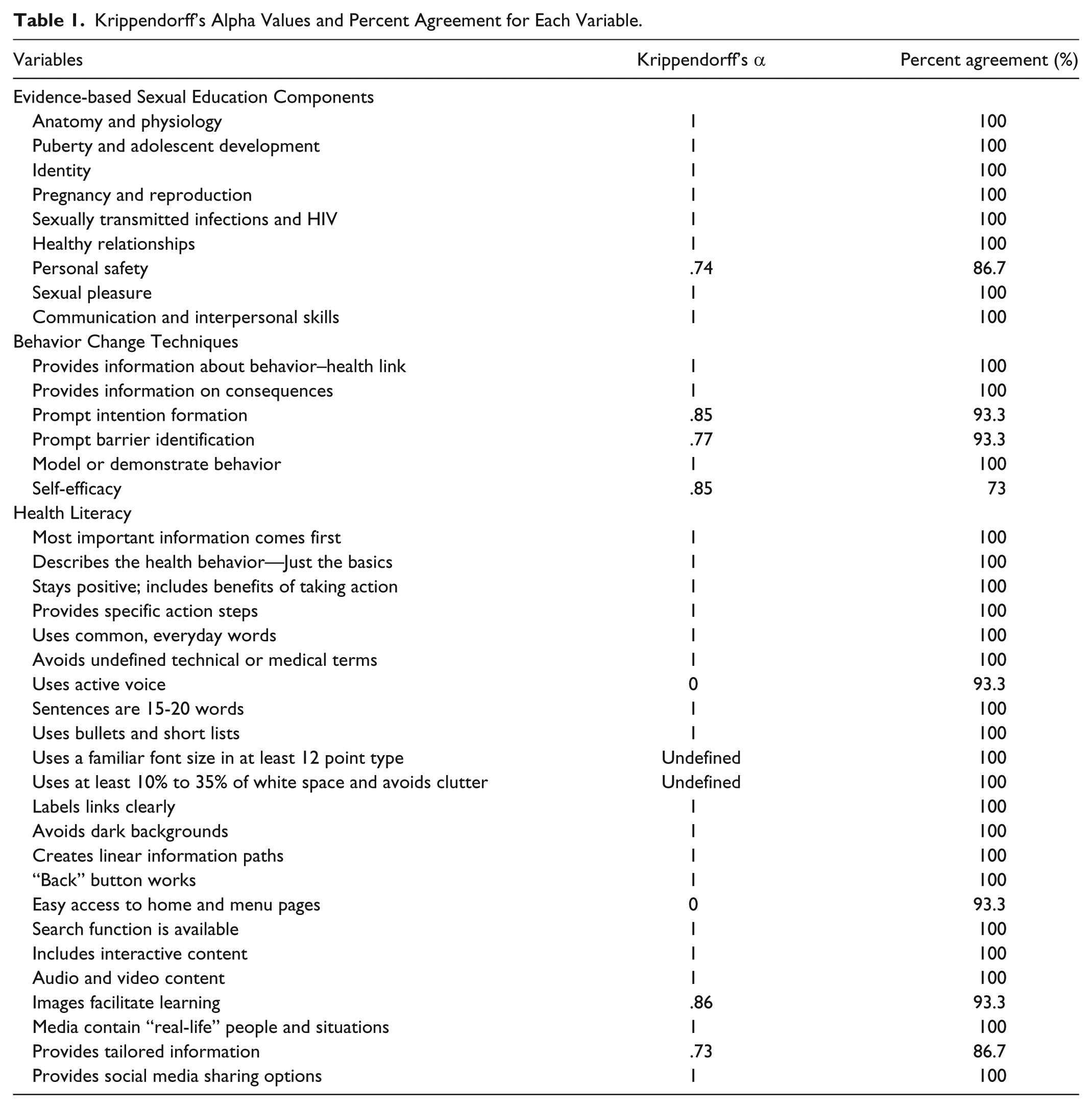
Interrater reliability was calculated using Krippendorff’s alpha (Hayes & Krippendorff, 2007). Thirty-four variables had alphas between .74 and 1, indicating excellent reliability (Taylor & Watkinson, 2007). The alpha for two variables was not calculated because there was no variance in the data. The value of alpha was 0 for two other variables despite coders’ agreement on 93.3% of cases. The lack of variance in the data could be the reason for this value. Any disagreements between the coders were resolved in consultation with the first author (see Table 1).
Krippendorff’s Alpha Values and Percent Agreement for Each Variable.
Results
The first research question sought to identify the availability of apps related to sexuality, sexual health, and sexual education in the iOS and Android app markets. The screening of the app descriptions led to the identification of 679 apps addressing various topics related to sexuality and sexual health from the originally 2,693 search results. To answer the second research question, the 679 apps were screened for apps containing detailed and extensive information on a variety of sexual health topics with the clear purpose of providing informational resources to adolescents. Fifteen apps (1%) were identified (see Figure 2).
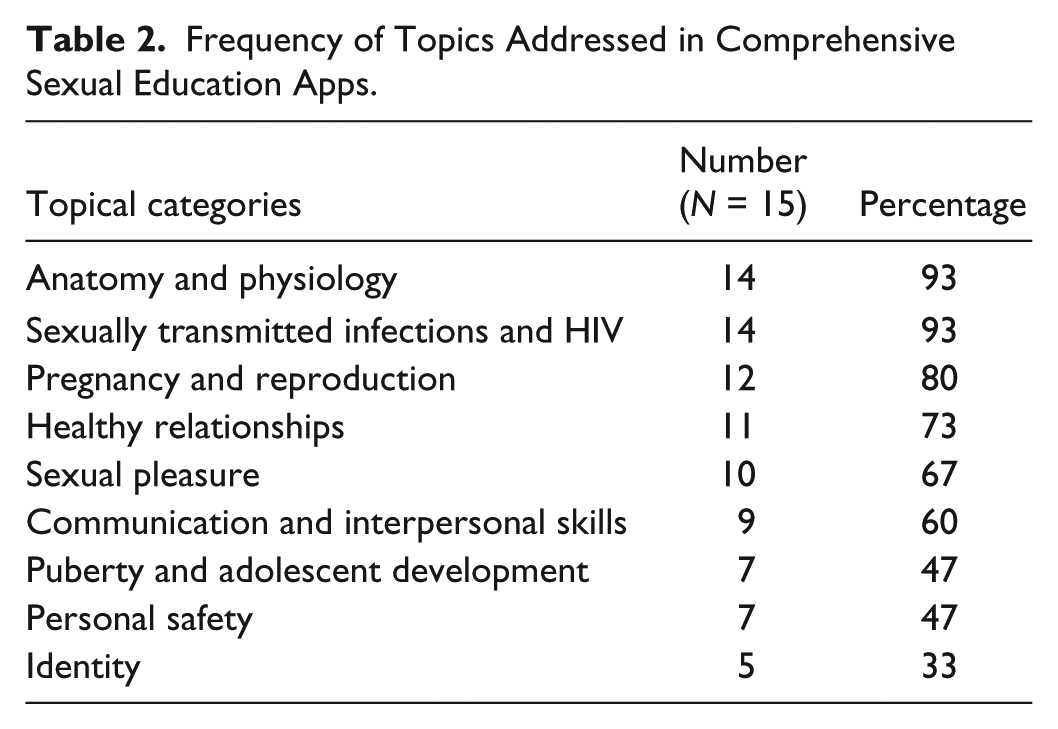
The third research question related to the integration of evidence-based sexual education components of CSEA identified in the previous stage (n = 15) and are presented in Table 2. The analysis revealed that the most frequent content areas included anatomy and physiology as well as STIs and HIV, appearing in 93% of all apps (n = 14), followed by pregnancy and reproduction with 80% (n = 12) and healthy relationships (73%; n = 11). Sexual pleasure and communication skills were mentioned in more than two thirds of apps with 67% and 60%, respectively. Less than half of the 15 apps addressed puberty and adolescent development (47%) and personal safety (47%). Identity was discussed in only one third of all apps (33%; n = 5).
Frequency of Topics Addressed in Comprehensive Sexual Education Apps.
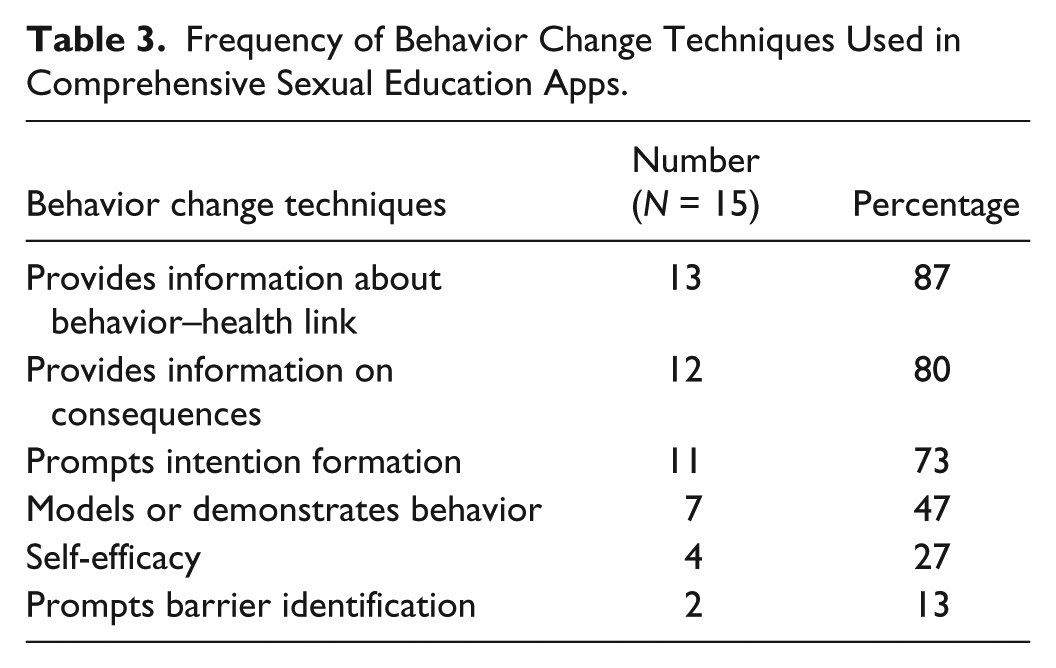
The fourth research question examined to what extent apps integrated health behavior techniques. A majority of apps provided information on sexual health that showed a clear link between sexual behavior and health outcomes (n = 13; 87%). Eighty percent of apps (n = 12) addressed the consequences of sexual behavior and 73% (n = 11) prompted intention formation. Less than half of apps modeled or demonstrated sexual health behavior (n = 7; 47%) and only 27% (n = 4) tried to increase the level of self-efficacy in their users. Last, only two apps (13%) addressed potential barriers to healthy sexual behavior (see Table 3).
Frequency of Behavior Change Techniques Used in Comprehensive Sexual Education Apps.
To answer the fifth research question, we analyzed the adherence to health literacy principles in the design of CSEA (see Table 4). The analysis revealed that the most common content-related design feature consisted of active voice (n = 14; 93%). Most apps (73%; n = 11) put the most important information first and included the benefits of taking action. Furthermore, more than two thirds of apps used common words and short sentences (n = 10; 67%), avoided medical or technical terms (n = 9; 60%), and provided specific action steps (n = 9; 60%). Half of all apps (n = 8; 53%) described only the basics of health behavior.
Frequency of Health Literacy Principles in Comprehensive Sexual Education Apps.
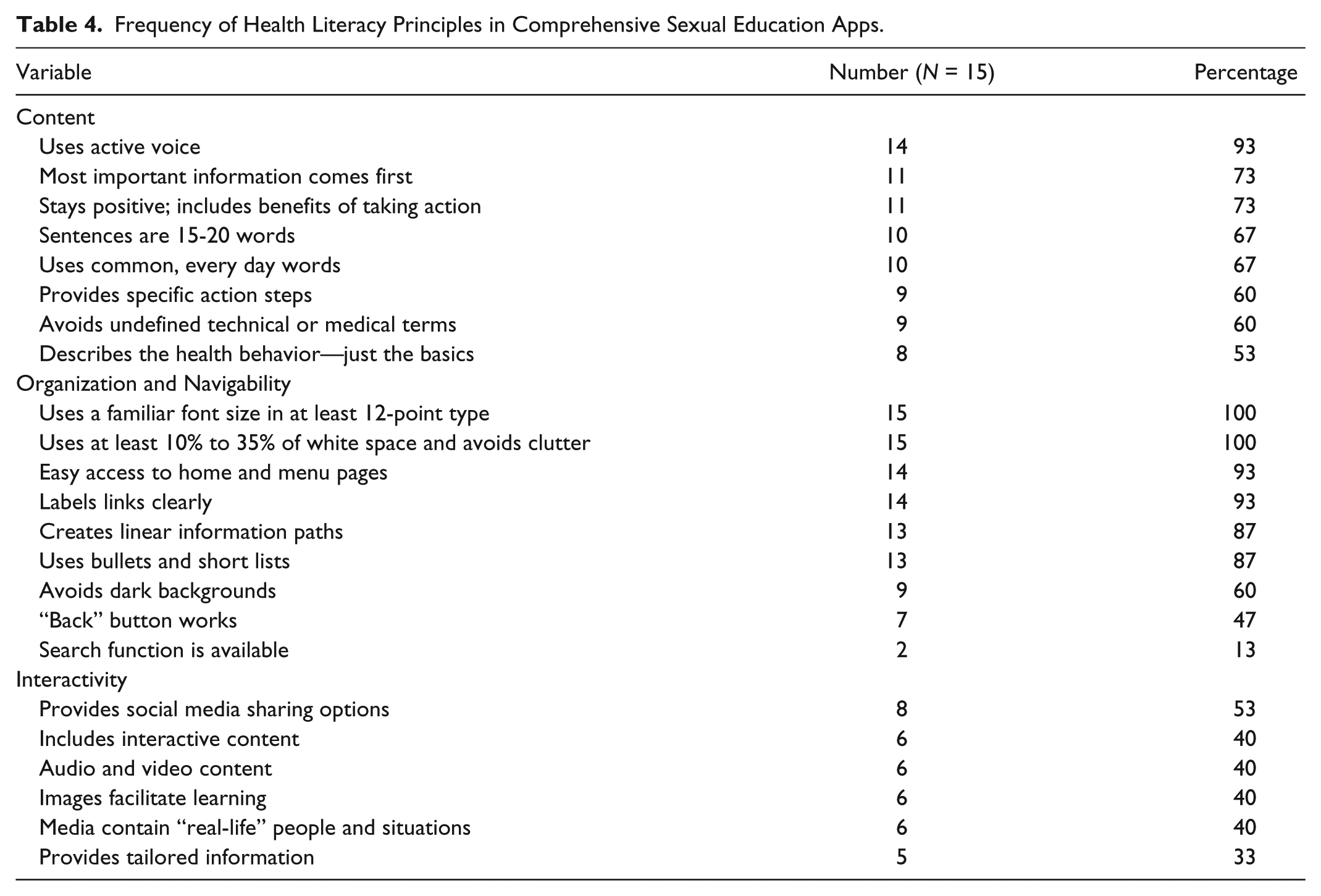
Similarly, the majority of apps adhered to health literacy principles in terms of organization and navigability. All apps used a familiar font size and avoided a cluttered interface (n = 15; 100%), while 93% (n = 14) provided clearly labeled links and easy access to the home menu. Eighty-seven percent of apps were organized linearly and used bullet points and short lists (n = 13). Only two thirds avoided dark backgrounds (n = 9; 60%) and less than half of all apps had a functioning back button (n = 7; 47%). Only two apps (13%) provided the recommended search function.
Finally, use of recommended interactivity principles was low. Fifty-three percent of apps allowed users to share content through social media (n = 8), while only 40% (n = 6) included interactive features such as quizzes and games. Audio and video content as well as images to facilitate learning appeared in only 40% (n = 6) of all apps. When media were provided, less than half of them contained “real-life” people or situations (n = 6; 40%). Last, only 33% (n = 5) of apps provided tailored information to users, such as gender- or age-specific functions.
Discussion
The current study utilized a content analysis to examine the scope of SEA available to Android and iOS users, with a focus on availability, content, and literate design of comprehensive sexual education components. The overarching finding was that despite an overwhelming number of SEA, only a dearth of literate, evidence- and theory-based SEA is in fact available to teenagers. This study advances the field in a few ways. First, whereas the effectiveness of comprehensive sexual education has been increasingly recognized in face-to-face educational settings, our study showed that they have not yet been widely implemented in mHealth. Moreover, analysis of the few CSEA available to users revealed that even app developers who integrate aspects of comprehensive programs do not apply the full range of the recommended components.
Despite the recognized need to promote a holistic, positive outlook on sexuality, we found that app developers mainly focused narrowly on pregnancy and STI prevention. This limited focus is concerning as it leaves out crucial topics such as puberty and emotional development and sexual identity. Although lesbian, gay, bisexual, transgender, or queer (LGTBQ) youths are particularly in need of sexual health information (CDC, n.d.) and thus providing essential resources to sexual minority youth is paramount, few apps addressed their needs. App developers should follow evidence-based guidelines that explain the physical and emotional changes during puberty and include information supporting LGTBQ youth forming an identity and navigating relationships. Being more inclusive in the presentation of content may help reduce health disparities and foster understanding and respect for LGTBQ adolescents. Furthermore, less than half of all apps provided information on personal safety. In view of the prevalence and impact of dating violence on adolescents (CDC, 2014), this result constitutes a missed opportunity to address this issue.
Our findings also lend support to the importance of incorporating theory-based, positive approaches to SEA. Although most apps included a health–behavior link, the information they provided centered on adverse health outcomes of sexual behavior. Contrary to existing guidelines, apps rarely incorporated modeling behavior and increasing self-efficacy. Showing teenagers how to perform healthy sexual behaviors is essential for strengthening their self-efficacy and enabling them to adopt these behaviors (Bandura, 1977). Receiving this information leads to delays in sexual onset among teens (Tortolero et al., 2010) and reduced dating violence (Foshee et al., 2005). Furthermore, despite the influence of social determinants on teens’ sexual health behavior (Kirby & Lepore, 2007), only two apps addressed potential barriers to healthy sexual behavior, such as peer pressure or lack of financial means. Addressing these barriers and showing ways to overcome them can increase the effectiveness of mHealth interventions.
The study also revealed significant shortcomings in apps’ adherence to health literacy principles. While the use of literacy strategies regarding clear organization and easy navigability by most apps was encouraging, the results support the need for plain language. For instance, medical terms remained undefined in almost half of apps and content did not focus on the basics of sexual health information. Considering that teens prefer plain language and clear content, and in view of the relationship between low literacy rate and sexual health disparities (Champion, Harlin, & Collins, 2013), the design of current CSEA may hinder youths’ access to essential health information. It is thus evident that app developers have to pay more attention to literacy principles in order to strengthen app effectiveness and reduce disparities in access to sexual health information.
Although several studies have shown great success in promoting healthy sexual behavior by making use of these features (Levine, 2011; Lou, Zhao, Gao, & Shah, 2006; Nguyen et al., 2013), only a minority of CSEA included pictures, audios, videos, or other interactive features. Consistent with previous research that identified an even lower number of videos and audios in a sample of pregnancy prevention apps (Mangone et al., 2016), these findings are alarming considering that sharing information, communicating with like-minded people, or watching videos are some of the features that teenagers are particularly enthusiastic about (Levine, 2011; Wartella et al., 2015). Therefore, there is an identified need to incorporate such features in the design of apps.
Implications for Practice
Our findings have implications for the way health educators can use apps in the delivery of sexual health information when working for adolescents. First, in view of the difficulty in identifying appropriate apps, health educators should seek opportunities to identify evidence-based apps and recommend them to adolescents. CSEA identified and evaluated for this study may help health educators choosing appropriate apps (see Supplemental Appendix B). Overall, we recommend apps that take on a positive perspective on sexuality and include BCTs, such as increasing self-efficacy and demonstrating healthy behaviors. Moreover, health educators should examine the design and navigability of apps. Content should be presented clearly and concisely, without excessive medical jargon or undefined words. Selecting apps that contain interactive or user-engaging features, such as quizzes and videos, may increase the interest of adolescents in sexual health information. Notably, greater attention should be placed on selecting apps for populations who experience increased disparities. For instance, LGTBQ teens need additional information on gender-based violence, homophobia, and sexual orientation.
Strengths and Limitations
This study led to several important findings regarding mHealth use in sexual education. The screening process provided an overview of the availability of relevant apps. Using a scraping tool allowed us to address methodological barriers to conducting such an analysis that were identified by previous authors (Mangone et al., 2016). More important, this is the first study to explore the quality of CSEA. Furthermore, to our knowledge this is the first study that assessed use of literate design of SEA. Therefore, the study recommendations can advance future research as well as inform future mHealth interventions.
Nevertheless, there were limitations to this study. For instance, we based our analysis on the app descriptions provided in the app stores. As these descriptions might not always correspond to the actual content of the apps, it is possible that some apps were wrongly excluded. Another limitation relates to the search process. Although we followed past studies in identifying search terms, the search phrases chosen may differ from those that teens would use to look for health information. Therefore, future usability studies should be conducted to identify users’ search patterns and explore usability as judged by the target audience to gain insights and perspectives into their use patterns as well as to measure app effectiveness. Finally, as we examined apps in English only, and did not explore apps’ cultural adaptation, future studies should examine the availability and content of SEA in additional languages, and consider cultural factors, such as cultural sensitivity, that were beyond the scope of this investigation.
Conclusion
Our analysis revealed missed opportunities in fully capitalizing on the potential of mHealth as an innovative and engaging platform to promote sexual health among teens. We identified a pressing need to move away from the narrow focus on STI and pregnancy prevention and to approach sexuality from a comprehensive, holistic, and positive perspective. Stronger emphasis should be placed on currently overlooked aspects, which may help reduce health disparities and provide resources that resonate with minority youth. Health educators should work with app developers to strengthen self-efficacy and demonstrate theoretically based healthy behaviors by taking advantage of innovative and engaging features of apps and by using plain language principles to reach broader audiences.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.