
Abstract
Serogroup C invasive meningococcal disease (IMD) outbreaks in men who have sex with men (MSM) have been occurring with greater frequency in urban areas across the United States. An effective vaccine for IMD is available and is recommended for MSM in outbreak settings. Particular subgroups of MSM have been disproportionately represented in outbreaks, specifically young, Black, and HIV-positive MSM. As little is known about the knowledge, awareness, and vaccination status of young MSM, we sought to describe this and explore racial/ethnic differences. Data were collected from an established cohort study—RADAR—of 16- to 29-year-old MSM recruited through previous cohort studies and/or by being a partner or peer of a current study member. A total of 486 young MSM (YMSM) responded to 13 IMD-related questions. Approximately half of the sample correctly identified how IMD is spread and 58.6% accurately responded that vaccination was the best prevention method; however, more than 60% of participants felt they were at no risk of getting meningitis and only 49% self-reported vaccination. Additionally, White YMSM were significantly more likely to be vaccinated and to have accurate knowledge and risk perception of IMD compared with Black YMSM. Findings have important implications for disease control, outbreak management, and intervention development.
Meningitis is an inflammation of the meninges covering the brain and spinal cord that can be caused by a variety of pathogens—fungi, parasites, amoeba, cancer, viruses, and bacteria. There are 14 serogroups of meningococcus, among which A, B, C, W, and Y are the most invasive. The distribution of meningococcal disease varies by geography, serogroup, and age (Nelson & Williams, 2013). The bacterial form of meningitis is highly contagious and is spread through close contact with infected individuals; it most commonly affects individuals with compromised immune systems, including people living with HIV/AIDS (PLWHA; Centers for Disease Control and Prevention [CDC], 2017). Symptoms resemble influenza and include headache, fever, and stiff neck. While some cases of meningitis improve over a few weeks without treatment, experts recommend immediate treatment, as many cases can be fatal within days. Physicians immediately treat bacterial meningitis with an array of antibiotics, and prehospital treatment is recommended, due to the rapidity with which the disease causes permanent damage (Hoffman & Weber, 2009).
Over the past decade, there has been frequent community outbreaks of serogroup C invasive meningococcal disease (IMD), caused by Neisseria meningitidis, in urban areas across North America (Thigpen et al., 2011), including Toronto (Zhou et al., 2012), Chicago (Schmink et al., 2007), New York City (Kratz et al., 2015), and Los Angeles (Nanduri et al., 2016). These outbreaks have disproportionately affected men who have sex with men (MSM), as well as PLWHA. Largely, these recent outbreaks have been isolated to communities within urban areas (Kratz et al., 2015; Nanduri et al., 2016; Schmink et al., 2007; Thigpen et al., 2011; Zhou et al., 2012).
In the United States, there are two types of vaccines available: (1) meningococcal polysaccharide and (2) meningococcal conjugate. The conjugate, in which the polysaccharide is bonded to a protein to elicit immune response, has been found to be more effective in young children than the polysaccharide vaccine (Nelson & Williams, 2013). A vaccine for IMD was first licensed and recommended for adolescents in 2005, with approximately 70% to 90% effectiveness (Cohn et al., 2013). In 2006, it was recommended that all individuals entering middle school, high school, or college receive a dose of the quadrivalent conjugate vaccine, as well as anyone aged 11 to 15 years who was at increased risk for acquiring the disease (American Academy of Pediatrics Committee on Infectious Disease, 2006). In 2009, the CDC recommended booster doses for high-risk individuals every 5 years after initial vaccination. While HIV-negative individuals only need one dose of the vaccine to be protected from IMD, CDC recommended in 2010 that HIV-infected individuals should receive 2 doses, separated by 8 weeks. In 2016, the Advisory Committee on Immunization Practices recommended routine use of the IMD conjugate vaccine (MenACWY-D or MenACWY-CRM) for PLWHA aged >2 months (MacNeil, Rubin, Patton, Ortega-Sanchez, & Martin, 2016). At the onset of the IMD outbreak in Chicago, vaccination recommendations for PLWHA were only in place during periods of active outbreaks.
Similar to many other communicable diseases, there are demonstrated racial/ethnic differences in meningitis awareness and infection. For instance, in an analysis of 3,188 patients diagnosed with bacterial meningitis between 1998 and 2007, incidence among Black individuals ranged between 2 and 3 times greater than among White individuals (Thigpen et al., 2011). Similar disparities have been seen in the recent urban outbreaks; nearly twice as many cases in the New York City outbreak were among Black than among White individuals (Kratz et al., 2015).
In Chicago, the first IMD outbreak occurred in 2003; this outbreak was exclusively among MSM and resulted in five confirmed cases and one death (Schmink et al., 2007). More recently, a sustained outbreak of IMD from 2015 to 2016 resulted in seven cases and one death in 2015, and three cases in 2016 (Fricchione, Kemble, & Black, 2016). In response to this outbreak, the Chicago Department of Public Health (CDPH) expanded its vaccination efforts across the city in order to distribute 18,000 vaccinations to various clinics and community-based organizations serving populations most affected by the outbreak in Chicago—Black MSM, transgender women, and PLWHA (CDPH, 2016). CDPH worked to engage providers across the city through webinars and stakeholder meetings that provided information related to the outbreak, its disproportionate effect on MSM and PLWHA, how to order additional vaccines from the city, and challenges and successes in achieving higher vaccination coverage (Chicago Health Alert Network, 2016). CDPH (2015) also launched a media campaign targeted at affected populations that consisted of press releases, paper canvassing, billboards, Action Alerts to community partners, social media outreach, push notifications on dating apps, and digital ads on Facebook, Twitter, and Google. CDPH’s outreach efforts were evaluated via a web-based survey sent to community partners—96% of community partners who responded rated CDPH’s outreach efforts as “Very Good” or “Good,” and 87% of community partners rated CDPH’s communication efforts as “Very Good” or “Good” (CDPH, 2015). These efforts, however, have not seemed to have reached the populations most at-risk in Chicago; according to CDPH, two thirds of MSM have not been vaccinated against meningitis, and 90% of HIV-positive MSM have not received both doses of the vaccine (CDPH, 2015).
As young MSM (YMSM), particularly Black YMSM, are at the greatest risk of HIV infection (CDC, 2016), it is of utmost importance that they are vaccinated against meningitis infection. While historically it has been shown that Black individuals are at higher risk for meningitis compared with White individuals, information regarding vaccination coverage, or even awareness of meningitis, within the YMSM population is inconclusive (Folaranmi et al., 2017). Therefore, this study sought to describe the knowledge and awareness of, and vaccination for, meningitis within a racially/ethnically diverse sample of YMSM in Chicago, and to explore any racial differences that might explain disparities seen in the broader MSM community.
Material and Method
Data for this study were collected within RADAR, a longitudinal cohort study of YMSM in Chicago focused on understanding the individual, dyadic, network, social, and biological factors that are associated with HIV infection. Study participants complete an initial assessment that includes a network survey, an individual-level psychosocial survey, and collection of biological samples for HIV and STI testing. Subsequent visits occur every 6 months for the duration of the cohort study. Data for this report came from study participants who attended a visit between August 16, 2016 and November 22, 2016 who were administered the self-report meningitis items, regardless of visit number, and included in the analytic sample (n = 486). The meningitis items were only administered to each study participant once.
Participants
In order to be enrolled in the RADAR cohort, participants had to meet the following criteria: between 16 and 29 years of age, assigned a male sex at birth, English-speaking, and reported a sexual encounter with a man in the previous year or identified as gay or bisexual. Participants were recruited in three ways: (1) involvement in a cohort of YMSM and/or sexual and gender minority youth (Project Q2; Mustanski, Garofalo, & Emerson, 2010), Crew 450 (Mustanski, Johnson, Garofalo, Ryan, & Birkett, 2013), and a new 2015 cohort, all of which enrolled individuals when they were between 16 and 20 years old; (2) through being a serious partner of an existing RADAR cohort member (i.e., being in a current serious relationship with a RADAR cohort member); or (3) through peer recruitment by an existing RADAR cohort member. Study participants were enrolled into Project Q2 and Crew 450 through modified respondent-driven sampling; additional details can be found elsewhere (Mustanski et al., 2010; Mustanski et al., 2013). The new 2015 cohort was recruited using venue-based, peer-referral, and online recruitment methods. Although all serious partners were eligible for a one-time visit, they were required to meet the above criteria for enrollment in the cohort. Similarly, peer recruits needed to meet the same criteria, plus they needed to be between 16 and 20 years old. Age was restricted for peer recruits to match the recruitment design of the previous cohorts (i.e., Project Q2 and Crew 450), which at the time of the current study also had older participants (i.e., ages 20-29 years) and the overall RADAR sample needed to represent a full range of ages to achieve the multiple cohort, accelerated longitudinal design (Miyazaki & Raudenbush, 2000).
Measures
Demographics
At baseline, participants were asked to report their racial identity, and whether they identified as Hispanic or Latino. Following the 2007 U.S. Department of Education guidelines for combining ethnicity and race data, anyone who identified as Hispanic/Latino regardless of race was classified as Hispanic/Latino (U.S. Department of Education, 2007). All non-Hispanic/Latino individuals who identify as a single race were classified as that race; anyone who identified as two or more races were classified as multiracial. All other demographic information was collected during the interview at which the meningitis items were assessed. These measures include age, gender identity, educational attainment, student status, employment, and sexual identity.
Meningitis
A series of 13 questions were asked to measure participants’ level of knowledge about meningitis, the ongoing outbreak in Chicago (“Recently, there has been an increase in the number of meningitis cases in Chicago. Before today, were you aware of this recent increase in new meningitis cases in Chicago?”), and the vaccination campaign directed by CDPH (“Were you aware of the meningitis vaccination campaign being led by the local health department in Chicago?”). In addition, items related to reasons for and against vaccination and experiences with side effects were assessed (see the appendix).
The responses to the question “What is the primary way that meningitis is spread from person to person?” was collapsed into “Correct (Saliva or Spit)” and “Incorrect (All others).” Similarly, the responses to the question “What is the best way to reduce your risk of getting meningitis?” was collapsed into “Correct (Getting vaccinated against meningitis)” and “Incorrect (All others).”
HIV Status
All study participants were tested for HIV at each visit. HIV point of care testing was conducted on all self-reported HIV negative participants using the Alere™ Determine™ HIV 1/2 Ab/Ag Combo test. If a participant tested reactive or self-reported as HIV-positive, then a 5-mL SST (Serum Separator Tube) was drawn and sent for confirmatory testing. Once results are confirmed, no further HIV tests are conducted for that participant for the duration of the study.
Statistical Analysis
All analyses were conducted using SAS Version 9.4 (SAS Institute, Cary, NC). Univariable statistics were used to describe measures of meningitis knowledge, awareness, and vaccination. Then, odds ratios (ORs) were used to assess the association between categorical demographic variables and each of our three main outcome variables: (1) awareness of the ongoing meningitis outbreak in Chicago, (2) awareness of the vaccination campaign in Chicago, and (3) having been vaccinated against meningitis. As age was not normally distributed, Kruskal–Wallis tests were used to measure significant associations between age and each of the outcomes. Additional exploratory analyses were conducted to assess differences between White and Black YMSM across a number of meningitis items.
Results
The 486 individuals included in this sample were a median age of 21.5 years (interquartile range = 5.1 years); most identified their current gender identity as male (92.0%) and their sexual orientation as either gay (71.0%) or bisexual (18.1%). Nearly equal proportions identified as Black (30.9%), Latino (30.2%), and White (25.2%), and one fifth were HIV-positive (19.6%).
Meningitis Awareness and Knowledge
Generally, accurate knowledge about meningitis within this sample of YMSM was moderately high. However, fewer than half of participants (42.8%) correctly identified the primary way that meningitis is spread as via saliva or spit (Table 1), and 58.6% accurately responded that vaccination is the best way to reduce their risk for acquiring meningitis. Despite inconsistent knowledge (or perhaps because of it), more than 60% of participants felt they were at no risk of getting meningitis.
Knowledge and Awareness of and Vaccination for Meningitis Among YMSM in Chicago (n = 486).

Note. YMSM = young men who have sex with men; CDPH = Chicago Department of Public Health.
Although there has been an active citywide campaign in Chicago to invigorate meningitis vaccination rates among MSM, it has not effectively caught the attention of YMSM in this sample. Only 31.7% of participants knew there was an ongoing meningitis outbreak in Chicago, and fewer than one quarter were aware of the meningitis vaccination campaign overseen by CDPH (23.5%). Of those who heard of the campaign, most learned about it from their health care provider (44.7%) or from the Internet (37.7%); venues which were targeted by CDPH, such as pride events and bars/clubs, were much less likely to be reported.
Meningitis Vaccination
Nearly one half of participants (49.0%) reported ever receiving a meningitis vaccination, most on the recommendation of their doctor (83.2%). Very few individuals reported experiencing side effects from the vaccine (3.4%). Of the 51% of YMSM who had not been vaccinated, the majority were unaware that a vaccine existed (51.2%), followed by 29.2% who did not think they were at risk. Unsurprisingly, having been vaccinated was significantly associated with awareness of the ongoing meningitis outbreak (OR = 2.31; 95% confidence interval [CI] [1.56, 3.42]), awareness of the local vaccination campaign (OR = 2.03; 95% CI [1.32, 3.12]), and knowing that receiving the vaccine was the best way to prevent meningitis infection (OR = 4.23; 95% CI [2.87, 6.23]).
Bivariable Associations
Several demographics were associated with awareness of the meningitis outbreak in Chicago. YMSM who were aware of the outbreak were, on average, almost 3 years older than those unaware (median: 23.6 vs. 20.8 years, respectively; p < .0001). Participants who knew about the ongoing outbreak were more likely to be HIV-positive and less likely to be a current student or unemployed (Table 2). There were no differences based on race/ethnicity.
Demographic Associations With Meningitis Awareness and Vaccination (n = 486).
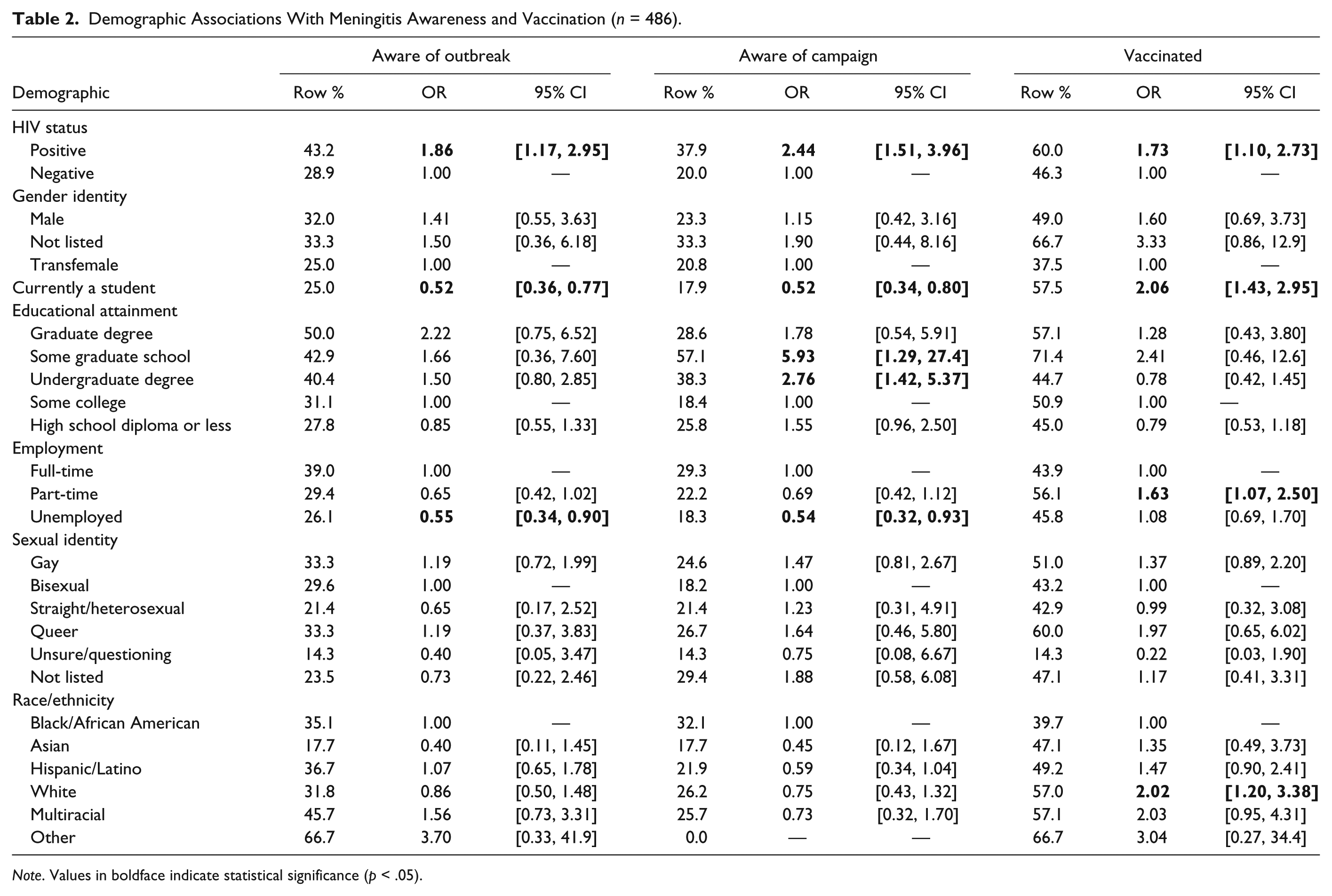
Note. Values in boldface indicate statistical significance (p < .05).
There were similar findings for awareness of CDPH’s vaccination campaign. Specifically, those who were aware were older (median: 23.9 vs. 20.8 years, respectively; p < .0001), more likely to be HIV-positive, and less likely to be a current student or unemployed (Table 2). Education differences were also identified: Compared with YMSM with some college education, individuals with an undergraduate degree were almost 3 times as likely to know of the campaign, those with some graduate education were almost 6 times as likely to have heard about the campaign. Additionally, there were a few demographic differences for reported source of information about the vaccination campaign: White YMSM were 9 times as likely to have seen advertising at bars or clubs as Black YMSM (OR = 9.10, 95% CI [1.10, 75.1]), and HIV-positive YMSM were more than 4 times as likely to have heard about the campaign from a health care provider as HIV-negative YMSM (OR = 4.56, 95% CI [2.49, 8.35]).
With regard to receipt of the meningitis vaccination, the direction of some associations reverses from the awareness metrics. YMSM who had been vaccinated were younger (median: 20.9 vs. 22.3 years, respectively; p = .008) and twice as likely to be a current student (Table 2). Similar to awareness assessments, vaccinated YMSM were nearly twice as likely to be HIV-positive. Those who received the vaccine were also significantly more likely to have part-time employment (vs. full-time) and identify as White (vs. Black/African American). Of note, the odds of White YMSM receiving the vaccine compared to Black/African American YMSM increased after controlling for both age and HIV status (adjusted OR = 2.63, 95% CI [1.49, 4.64]).
Racial Associations
Based on statistics from the ongoing meningitis outbreak in Chicago, Black MSM have been substantially more affected than White MSM, so further exploration of the factors differentiating these groups was conducted. Compared with Black YMSM, White YMSM were significantly more likely to correctly identify the main way in which meningitis is spread (OR = 2.61, 95% CI [1.54, 4.42]) and to correctly identify vaccination as the optimal way to prevent meningitis infection (OR = 3.10, 95% CI [1.78, 5.40]). Black participants were also significantly more likely to believe they were at no risk for meningitis (69.5% vs. 41.1%; p < .0001).
Most barriers and facilitators to vaccination did not differ by race within this sample. However, White YMSM were 2.44 times as likely to have been vaccinated as a result of a health care provider recommendation than Black YMSM (95% CI [1.59, 3.74]). Additionally, compared with Black YMSM, White YMSM were substantially more likely to have been vaccinated due to a friend or family member’s recommendation (OR = 12.1, 95% CI [2.74, 53.6]).
Discussion
To our knowledge, this is the first study to investigate meningitis knowledge, awareness, and vaccination uptake among YMSM, a population highly susceptible to infection during community outbreaks. As YMSM, particularly Black YMSM, are the group most at risk for HIV (CDC, 2016), and a compromised immune system places one at substantially greater risk of acquiring meningitis (CDC, 2017), there is an urgent need for research on ways to minimize the burden of disease within this population. This need is highlighted by our findings, in which the majority of YMSM were unaware of the main transmission route of meningitis, and felt they were at no risk for becoming infected. Additionally, more than 40% of participants indicated a method other than vaccination as the primary way to prevent getting meningitis. Clearly, meningitis knowledge is suboptimal within this population, and new ways to disseminate health-related information are needed.
In Chicago, where these data were collected, in addition to distributing vaccines and educating providers on the active outbreak, there was also an active, city-wide social marketing campaign focused on meningitis vaccination led by the local health department throughout the meningitis outbreak. Less than one third of participants knew there was an active outbreak, and only 23.5% had seen or heard about the vaccination campaign. A substantial portion of the campaign was conducted at pride events and at bars and clubs in the city, yet very few participants learnt about the campaign at these venues—of note, White YMSM were more likely to have seen campaign materials at bars and clubs than Black YMSM, potentially indicating a dearth of advertising in primarily Black venues. Instead, the most common route was hearing about the campaign from their health care provider. Similar to a substantial body of research on other preventable diseases (Chi & Neuzil, 2004; Gerend, Madkins, Phillips, & Mustanski, 2016; Reiter, McRee, Katz, & Paskett, 2015; Samoff, Dunn, VanDevanter, Blank, & Weisfuse, 2004), we found that health care provider recommendations were the most significant predictor of vaccination uptake. As such, future control efforts that include marketing campaigns should continue to focus on health care providers to ensure awareness of outbreaks and to ensure optimal vaccine uptake among the at-risk population.
Unsurprisingly, similar demographics were associated with awareness of the outbreak and of the campaign. These YMSM were older, more likely to be HIV-positive, and less likely to be unemployed or current students. All these factors are common correlates with health care–seeking behaviors (Salomon et al., 2009; Siconolfi et al., 2013; Straub et al., 2011) and again serve to highlight the importance of including providers in marketing campaigns. Conversely, those who actually received the vaccine tended to be younger and were more likely to be current students; this likely reflects the general requirement for meningitis vaccination prior to entry into college (CDC, 2015). Additionally, HIV-positive YMSM were nearly twice as likely to have been vaccinated as HIV-negative YMSM; as HIV-positive YMSM are more likely to be connected to a health care provider, and presumably one with a focus on HIV treatment, they may be much more likely to be offered the vaccine due to the Advisory Committee on Immunization Practices vote recommending vaccination for PLWHA (MacNeil et al., 2016). Although this can be viewed as a vaccination campaign success, it also highlights the need for seeking alternate outreach routes for HIV-positive YMSM who are not engaged in care.
As with many other health conditions, we found disparities between Black and White individuals in our study. Black YMSM were significantly more likely to believe they were at no risk for meningitis and to incorrectly report the primary methods of transmission and prevention. Addressing racial/ethnic health disparities requires individual-, community-, and policy-level interventions strategically designed to reach those most at risk of disease acquisition. Results from our study demonstrate that current techniques (e.g., leveraging health care providers, vaccination requirements, social marketing) are differentially affecting Black YMSM compared to White YMSM; additional strategies are needed to increase knowledge, awareness, and vaccine uptake among Black YMSM. Use of techniques, such as diffusion through social networks (Rogers, 2003), has been shown to be effective at enacting behavior change within Black MSM samples (Jones et al., 2008; Maulsby et al., 2013). Therefore, diffusion of meningitis vaccination information within the social and sexual networks of Black YMSM may be an alternative intervention to existing community-wide campaigns.
The main reason our sample reported for not being vaccinated was being unaware of the existence of a meningitis vaccine, followed by not feeling they were at risk. Future studies should explore predictors of intention to receive vaccination and whether or not knowledge and risk perception are related to intention and ultimate uptake of vaccination; particularly as perceived benefits of vaccination have been found to be strongly related to intent and receipt of vaccination among YMSM. Identifying the causal pathway to vaccination uptake, and whether or not it varies by demographic characteristics, will ensure that future intervention strategies are tailored effectively for populations most at risk of exposure during outbreaks.
Implications for Practice
Health educators and other public health practitioners, particularly those who work with YMSM, should be aware of the importance of provider influence and vaccination guidelines/requirements on vaccination acceptance and uptake. Study findings indicate that meningitis knowledge was suboptimal in this population; therefore, future programming and health education efforts directed at this population should include information on meningitis risk and prevention. Finally, public health practitioners can work to reduce disparities in vaccine knowledge and coverage by designing and promoting interventions specifically for racial/ethnic minority individuals. Awareness that standard citywide campaigns may only reach the most visible individuals is important for developing alternative approaches such as network diffusion to improve access to more hidden populations.
Study findings should be interpreted with the following limitations in mind. First, the cross-sectional design of our study limits the ability to make causal inferences. Thus, it will be important for future research to explore whether or not exposure to awareness campaigns precede vaccination awareness and uptake. Second, while our sample was racially/ethnically diverse, the sample was nonrandom and therefore study findings may not apply to all YMSM. Third, variables of interest were assessed through self-report measures; however, use of self-interview technology was employed to minimize social desirability bias. Additionally, participants may not accurately recall their medical history of vaccination or may incorrectly conflate vaccination for prior diseases with meningitis vaccination, thus leading to over reporting of receipt of the meningitis vaccine. Finally, although provider recommendations played a key role in the decision to get vaccinated, we were unable to investigate how the CDPH campaign targeting health care providers may have increased these recommendations. It will be important for future research to examine meningitis awareness, knowledge, risk perception, vaccination intention, and barriers/facilitators to vaccination uptake in a national sample of YMSM.
Conclusion
Vaccination is the most effective strategy to prevent and control community outbreaks of meningitis. The results of this study suggest public health interventions need to strategically target Black YMSM and those who are not engaged in primary health care (e.g., nonstudents, older YMSM less likely to be on parents’ insurance).
Footnotes
Appendix
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by a grant from the NIH-funded Third Coast Center for AIDS Research (CFAR; P30 AI117943) and used data collected within the NIDA-funded RADAR study (U01 DA036939).