
Abstract
Young African American and Latina women aged 15 to 24 are more likely to adopt short-acting forms of contraception over long-acting reversible contraception. Mobile applications and other forms of digital media may be useful for providing adolescents with information about sexual and reproductive health both inside and outside of the health care setting. The miPlan app was designed in accordance with principles of user experience design, and its content was informed by the theory of planned behavior and the transtheoretical model of behavior change. A university-based design team engaged young African American and Latina women to inform app development and provide input on app design, conducting multiple rounds of usability testing. Researchers then evaluated the acceptability of the miPlan app in family planning clinics among African American and Latina women aged 15 to 24. Participants rated the app highly acceptable, finding it both easy to use and highly informative. We demonstrate that mobile applications designed in conjunction with user populations may be effective at providing health information due to users’ ability to identify with them and their accessibility.
Despite data on the efficacy and safety of long-acting reversible contraception (LARC) for adolescents, many African American and Latino adolescents and young adults still do not adopt LARC methods (McNicholas & Peipert, 2012; Ott & Sucato, 2014). Among adolescents ages 15 to 24 who use contraception, coital-dependent methods (condoms) and short-acting methods (oral contraceptive pills [OCPs]) remain the most commonly used (J. Jones, 2012). Among African American adolescents, 38% use condoms and 24% use OCPs. Among Latina adolescents, 29% use condoms and 36% use OCPs. African American and Latina adolescents, use of LARC methods such as the intrauterine device (IUD) ranges between 5% and 8%, respectively, with implant use being even lower. These rates are similar to rates of use by adolescents overall, IUD (8%) and implant (3%; Daniels, Daugherty, Jones, & Mosher, 2015).
A variety of factors may contribute to African American and Latina adolescents’ preference for short acting methods of contraception. Factors may include access to health care (Dehlendorf, Rodriguez, Levy, Borrero, & Steinauer, 2010; Haider, Stoffel, Donenberg, & Geller, 2013; Rew, 1998), health literacy, and misinformation, and cultural norms related to childbearing and fertility (Biermann, Dunlop, Brady, Dubin, & Brann, 2006; Geronimus, 2003). Some researchers have posited the patient–provider relationship as another barrier to LARC uptake, citing mistrust by patients associated with clinicians’ historical overuse of sterilization and injectable and implantable contraceptives (Bogart & Thorburn, 2006; Higgins, 2014; Killien et al., 2000). Others have shown that misinformation is a barrier for adolescents of color, especially for contraceptive methods that require the involvement of a health care provider (Shelton, Goldman, Emmons, Sorensen, & Allen, 2011; Thorburn & Bogart, 2005). Mistrust of providers related to provider bias in overprescribing LARC methods to women of color and poor women, minimization of side effects, and provider control and hesitancy in removing LARC methods on request have all been reported by young women (Higgins, Kramer, & Ryder, 2016). Adolescents have also expressed concerns about the potential for LARC having long-term effects on fertility and discomfort with having a foreign object in one’s body for an extended period of time (Murphy, Burke, & Haider, 2017). While adolescents should only use methods they desire, removing barriers may ensure they are aware of all available methods.
In addition to face-to-face provider–patient communication, health information can also be delivered via websites and new digital media (shareable digital media such as apps and text messages; M. Gilliam, Chor, & Hill, 2014), though increasingly these distinctions are growing less important given the advent of mobile websites. In addition to general health information, adolescents use, and perhaps prefer, the Internet for sexual health information. Among adolescents in one study, African Americans were more likely to be willing to communicate about sexual health through technology (Divecha, Divney, Ickovics, & Kershaw, 2012). Adolescents can access digital health information via a number of platforms. Mobile phones are near ubiquitous among adolescents, with 88% of young people, ages 13 to 17, in the United States possessing or having access to a mobile phone and 73% having a “smartphone” (i.e., containing a computer interface, access to apps, and/or the Internet; Lenhart, 2015). African American adolescents are more likely to have access to a smartphone (85%), compared with their White (71%) and Hispanic (71%) counterparts (Lenhart, 2015). Ninety-one percent of adolescents access the Internet through a mobile device at least occasionally, and African American adolescents are more likely to use a mobile device to access the Internet compared with White and Latino adolescents (Lenhart, 2015). While there is a lack of data for clinic-based, behavioral interventions delivered by apps as in the current study, research shows that apps are popular among adolescents and young adults. Almost 15% of adolescents and young adults ages 19 to 29 report using mobile apps for health information (Divecha et al., 2012). Among 18 to 24 year olds, 62% of time spent on digital platforms is spent on smartphone apps, with an additional 8% spent on tablet apps (comScore, 2017), with this age group spending more time with apps than any other age group. Furthermore, 18 to 34 year olds are the most likely to download five or more apps per month, compared with individuals in other age groups (comScore, 2017). Contraceptive information in particular can be effectively delivered digitally. Bedsider, developed specifically for adolescents and young adults, 18 to 29 years, has been studied in a range of demographic groups (Gressel et al., 2014) and found to be accessible for patient information and contraceptive choice.
User experience design offers a strategic approach for ensuring that the end user is engaged in intervention development. User experience design has been used extensively throughout the health field for a variety of interventions, including to develop a culturally tailored online program to prevent HIV among African American youth (Veinot, Campbell, Kruger, & Grodzinski, 2013), to develop an app seeking to improve healthy behaviors among WIC recipients (Biediger-Friedman et al., 2016), and to inform an app seeking to support weight management among overweight and obese youth (Knoblock-Hahn, Wray, & LeRouge, 2016), among many others.
This article describes the development and testing of a contraceptive counseling app called “miPlan” for use in the clinical setting with African American and Latina adolescents.
Method
This study used a multiple stage design, including app development and user testing, and evaluation of the resulting app via a randomized controlled trial.
miPlan App Development
The miPlan app was developed by refining an existing prototype app called “PreCounselor.” Modifying or “modding” is a common design approach for adapting an existing product. PreCounselor was developed by our team in the context of a quality-improvement study. In that study, young, female African American and Latina patients were engaged as part of a systematic study of potential gaps in high-quality health care for adolescents seeking contraception in Title X family planning clinics (M. L. Gilliam, Martins, Bartlett, Mistretta, & Holl, 2014). That study concluded that waiting room down time represented a missed opportunity for patient education about contraception. In response the waiting room contraceptive counseling app PreCounselor was developed. To ensure the app was patient-centered, the design team used user experience design in which African American and Latina patients collaborated with app developers/designers throughout the development process. In user experience design, the designer and end-user collaborate to create solutions in an iterative process of rapid prototyping with key stakeholder participation (Brown, 2008). The final PreCounselor app included information about all methods of contraception. A screen titled “Compare your methods” allowed patients to compare their contraceptive options with graphic depictions of all methods. Tapping on an image of a specific method enabled navigation to pages with information on side effects and contraceptive failure rates of the method. Patients also requested information regarding how men perceive and/or experience the method. In addition, PreCounselor included two videos featuring African American and Latina patients describing their experience (both positive and negative) with LARC methods. Graphics and photos also featured young women from these populations.
Theoretical Framework
The content of the miPlan app was informed by the transtheoretical model of behavior change (TTM) and the theory of planned behavior (TPB). The TTM provides a framework for understanding how individuals adopt new behaviors by progressing through a series of stages: precontemplation, contemplation, preparation, action, and maintenance (Prochaska & Diclemente, 1983). Specific processes facilitate the progression across these stages. The TPB posits that the best single predictor of behavior is the individual’s intention to perform the behavior (Ajzen, 1991). Behavioral intention is informed by the attitude toward the behavior and beliefs about outcomes associated with performing it; subjective norms and beliefs about those norms; and perceived behavioral control or self-efficacy, or the perception that one has the requisite skills and resources for performing the behavior. The TPB helps to explain how individuals move from the precontemplation, contemplation, and preparation stages into action. Together, these models establish a comprehensive view of the various influences and motivations by which individuals adopt a new behavior.
The TTM and TPB can be applied to conceptualizing how someone decides to use a contraceptive method. For example, adolescents who do not seek contraception are likely to be in the precontemplation stage, while those who seek contraception but are undecided as to which method to use are most likely in the contemplation stage and may be ambivalent about adopting a particular method. In order to move beyond precontemplation, individuals need to become aware of the availability of contraception. Similarly, to move beyond contemplation, individuals need to resolve ambivalence through a consideration of the relative benefits and costs of different contraceptive methods. Thus, patients need information about the contraceptive method to form an attitude, and useful information might include side effects, health risks, and non-contraceptive benefits of the method.
User Testing
For the development of miPlan, adolescents were asked to user-test an optimized version of PreCounselor, which used updated versions of text and graphics, still featuring African American and Latina young women, and omitted the videos used in PreCounselor. For all sessions, eligible use testers were ages 18 and older, African American or Latina, and English speaking. Researchers approached young women appearing to fit the study demographic in a university-based, clinic waiting room. Use testers were encouraged to use the app while researchers observed, interviewed, and took field notes. Researchers documented the tester’s experience, probing about expectations versus actual experience of using the app. Use testers were asked their opinion of the app and ways to improve the app. Sessions focused on different aspects of the app. One addressed text and graphical information, another viewed the videos, and a third assessed the full app.
In addition to navigating the app, the young women testers were also asked to evaluate videos for the app. Rather than creating videos of real patients, as in the PreCounselor app, five videos were made with different young female actors performing first-person monologues addressing the pros and cons of the implant and IUDs. Though not featuring real users, the content for these videos drew from the PreCounselor video interviews conducted with real patients. While videos of all methods would have been desirable, a decision was made to focus on these less familiar methods given the time constraints for use of an app in the waiting room. The videos were intended to be brief (each video lasted between 52 and 67 seconds), concise, and comprehensive. All videos featured African American and Latina young women. Testers were asked to rate the videos on believability and likeability. All user testing of the app used facility-based convenience samples and included the number of participants needed to obtain necessary information for the stage of app development (n = 27).
miPlan App Evaluation
The acceptability of miPlan was then studied as part of the intervention arm of a larger parent study, a randomized controlled trial of the app to determine its effects on contraceptive intentions and selection. Recruitment took place at four urban, community-based family planning clinics primarily serving African American and Latino women. Eligible women were between 15 and 29 years old, sexually active with a male partner within the past 6 months, self-identifying as African American or Latina, English speaking, presenting for contraception, and not already highly intending to use a LARC method (i.e., in precontemplation). Eligible participants completed informed consent procedures and were randomized (1:1) to the app plus clinic visit (intervention) versus clinic visit alone (control). A total sample size of 220 (intervention and control) was chosen in order to detect an increase from 25.8% (baseline) to 45% (intervention) in the proportion of patients interested in discussing LARC during their clinical visit based on a power (1 − β) = .80, with alpha set at .05. This study presents findings from the intervention arm only, comprising a total of 110 participants. Women randomized to the intervention arm were given a tablet computer programmed with miPlan and instructions to use the app for up to 20 minutes, with a minimum of 10 minutes. Participants were surveyed at baseline, immediately post app use, and at 3 months.
Measures
A baseline survey collected demographic information; sexual and reproductive health history (sexual experience and pregnancy history); and contraception-related variables (awareness of methods, knowledge of effectiveness, past and current method use, contraceptive self-efficacy, method interest and decisional balance for contraception). Contraceptive self-efficacy was measured using a five-item scale developed and validated by Galavotti (α = .84; Galavotti et al., 1995). Participants responded using a 5-point Likert-type scale with anchors of “not at all confident” and “extremely confident.” Decisional balance for contraception was assessed using a different scale developed by Galavotti, measuring both positive (five items, α = .86) and negative (five items, α = .81) perceptions of contraceptive use. For each item, participants rated how important each item was in their decision to use contraception, according to a 5-point scale anchored by “not at all important” to “very important.” To assess the acceptability of the app, participants indicated their agreement with seven statements regarding satisfaction (e.g., “The app was easy to use,” “I would recommend it to a friend”) using 5-point Likert-type scales (anchors were “strongly disagree” and “strongly agree”).
A 3-month follow-up survey reassessed measures of contraceptive self-efficacy and decisional balance for contraception, contraceptive satisfaction, and intention to continue method use. The follow-up survey also included questions related to technology use, including use of mobile phone, apps, text messaging, and social media. All participants were asked whether they would use a sexual and reproductive health app outside of a clinic setting, used the Internet for information about contraception before and after their most recent clinic visit, and would have liked to have access to miPlan during or following their clinic visit.
The study was approved by the University of Chicago Institutional Review Board, which also provided a waiver of parental consent for minors.
Results
User Testing and App Development
Three women participated in user testing of the text-based content. User testing was conducted between October 24 and 27, 2014, in the waiting room of a university-based family planning clinic. Most testers reported that they liked being able to see all contraceptive options. However, this session revealed that the gestures needed for swiping through the app were not intuitive for users. Furthermore, testers comprehended contraceptive effectiveness better than contraceptive failure rates. Testers were not able to identify all methods of contraception, based on the graphic images alone.
Usability testing resulted in two major changes: (a) listing the name of each of the contraceptive methods below each image and (b) replacing contraceptive failure rates with contraceptive effectiveness rates.
Twenty testers rated the five LARC-focused videos; the three highest rated videos were then selected for the miPlan app. These addressed the implant, copper IUD, and hormonal IUD.
Four testers participated in assessing the final miPlan app, on November 11, 2014, in the same location as initial user-testing. Negative comments regarding the app included the following: lack of tailoring based on individual women’s behaviors, lack of videos for all contraceptive methods, lack of information about sexually transmitted infections, and statement that condoms are least effective for pregnancy prevention. Positive statements about the app included very informative; effectiveness page and videos were considered particularly useful. Other highly rated features included the app design, tapping on images of each method for additional information about side effects, and hearing about men’s experiences (see Figure 1).
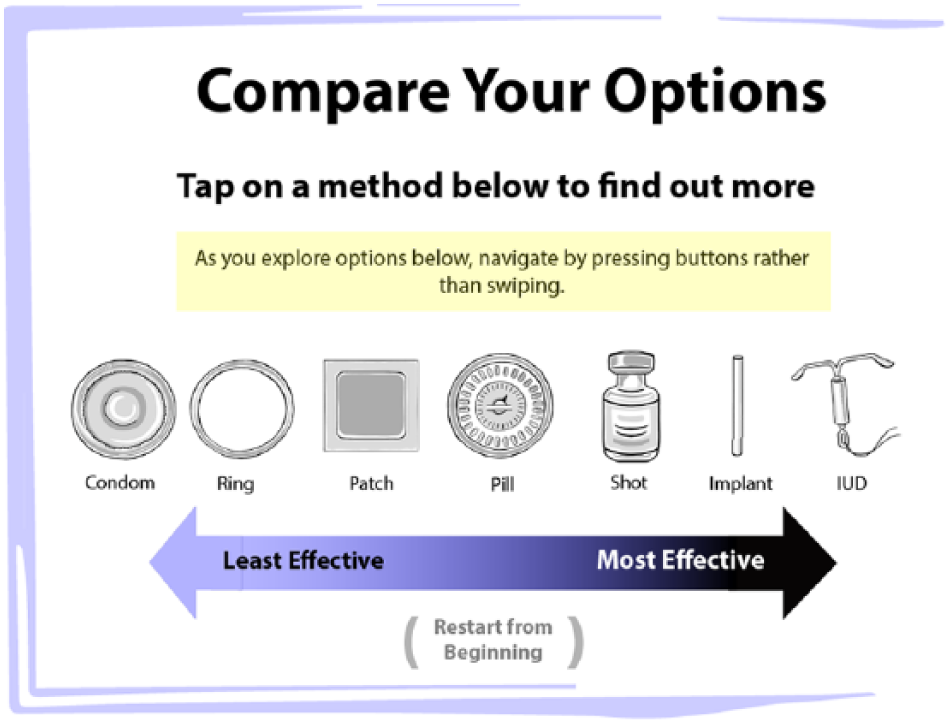
Screen shot from app.
miPlan App Evaluation
Participant Characteristics
Women were enrolled between February 2014 and January 2015. The 110 young women randomized to the intervention arm evaluated the app (Table 1). The median age of participants was 22 years. The majority were African American (73.1%) and the remainder Hispanic 26.9%. Almost all (99.1%) had had sexual intercourse. Most (53.4%) had completed some college. In addition, almost all owned mobile phones and used mobile applications. There was variation in relationship status, with 20.2% living with a partner or spouse, 33.7% being in a relationship without cohabiting, 21.4% having casual partners, and 26.0% being single. Regarding LARC awareness 59.4% and 58.5% had heard of the IUD and the Implant, respectively.
Characteristics of Participants (N = 110) Who Received MiPlan App.
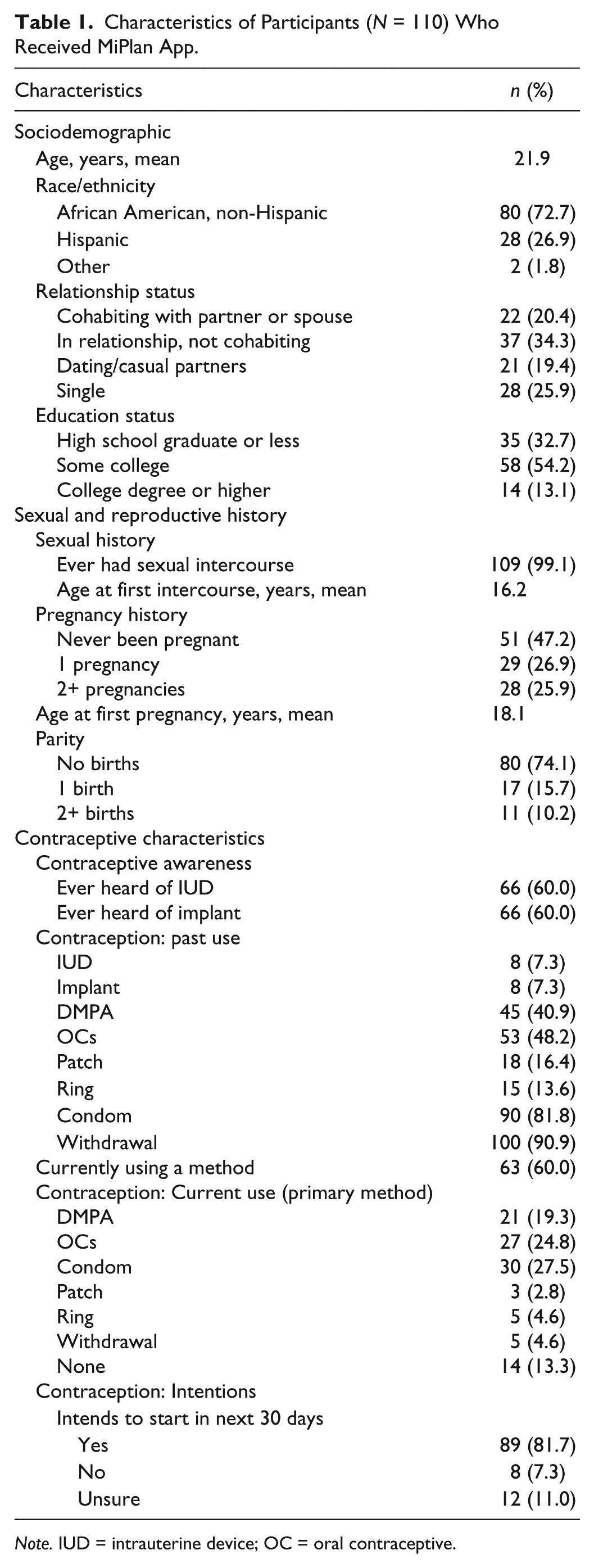
Note. IUD = intrauterine device; OC = oral contraceptive.
Contraceptive Self-Efficacy and Decisional Balance for Contraception
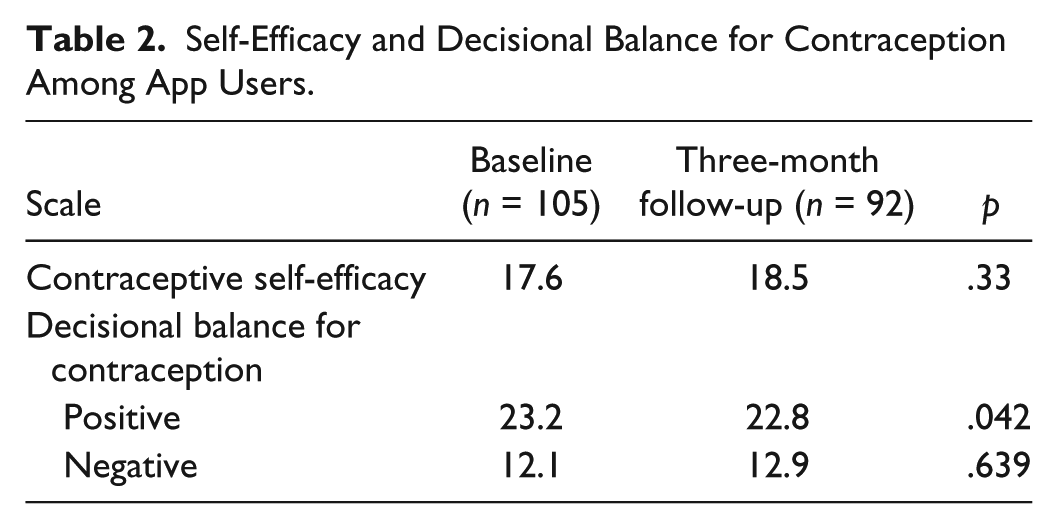
Following app use, contraceptive self-efficacy increased from a mean score of 17.6 to 18.5, though this change was not statistically significant (p = .33; Table 2). Positive decisional balance (i.e., perceived advantages of contraceptive use) decreased slightly over the study period (M = 23.2 to M = 22.8, p = .042). Negative decisional balance for contraception (i.e., perceived disadvantages) increased slightly from M = 12.1 to M = 12.9, though this was not statistically significant (p = .64).
Self-Efficacy and Decisional Balance for Contraception Among App Users.
miPlan App Acceptability
Almost all participants “strongly agreed” or “agreed” that they liked the app (95.4%) and that it was easy to use (97.3%; Figure 2). In addition, most strongly agreed or agreed that the app taught them new things about birth control, and that they would use the information in the future. A large majority of participants (96.4%) reported that miPlan was an appropriate use of the time spent waiting before their clinic visit.
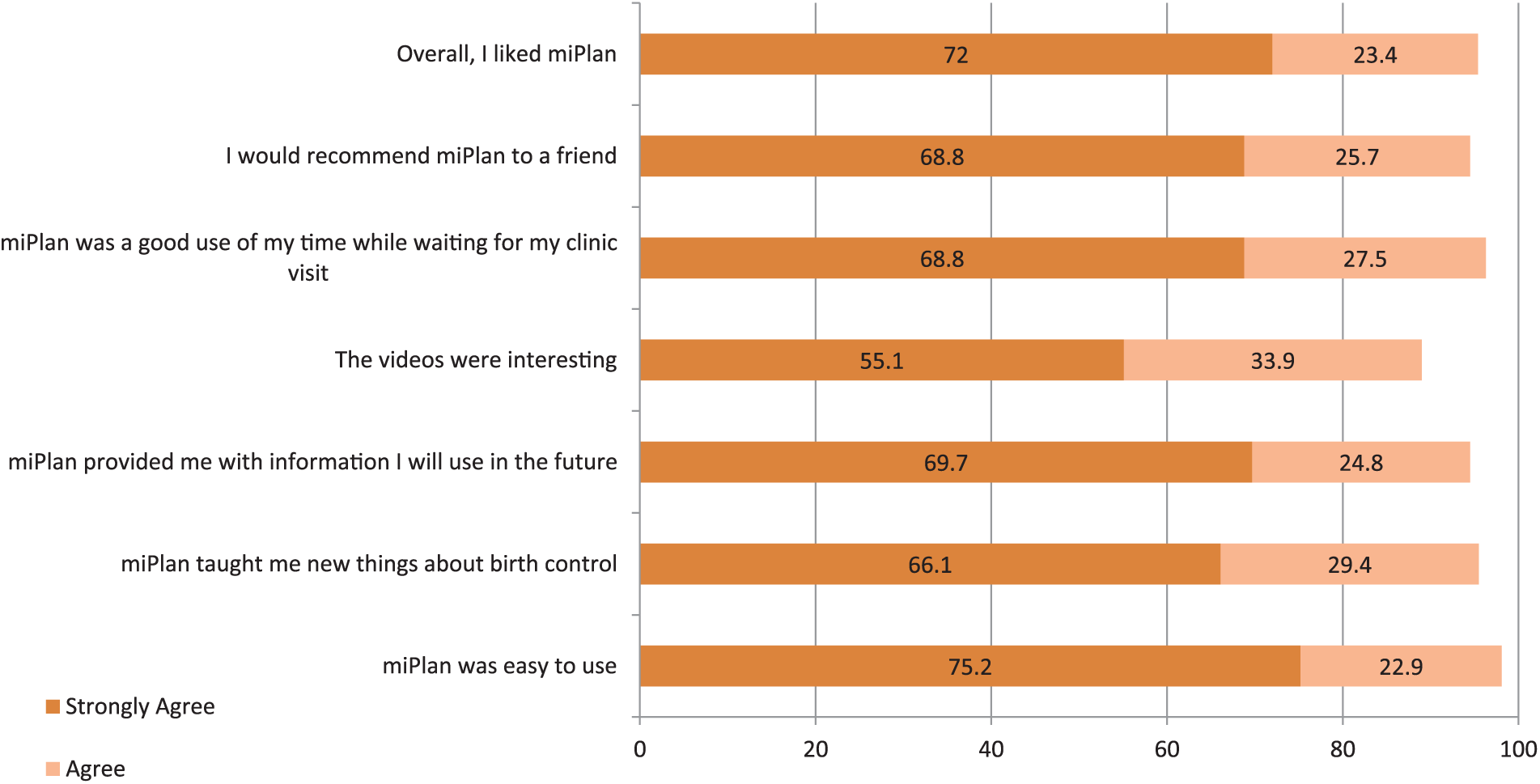
miPlan app acceptability (percentage of app users responding “agree” or “strongly agree”).
Technology Use
When asked 3 months later if they would use an app to learn about sexual and reproductive health outside of a clinic setting, 88.8% of participants responded that they would. Sixty-three percent of participants reported that they used the Internet to research contraceptive options before their clinic visit, and the majority of participants (66.3%) reported not having done so since. A slight majority of participants (57.5%) also responded that they wanted to refer back to the information in the app either during or after their clinic visit.
Discussion
This study describes a participatory approach to designing a contraceptive app with African American and Latino adolescents and young women. Given the multiple barriers to care for adolescents and young women of color, their inclusion in the development of an app featuring women with whom they might identify represents a potentially important advance in developing contraceptive counseling interventions. This study demonstrates that engaging young women in app development is feasible and results in a usable and highly acceptable app. Nearly 9 in 10 young women reported they would use an app outside of a clinic setting and over half of those who used the app reported wanting to refer to it during or after the visit. This study also highlights a key benefit of digital media interventions—ease of modification and refinement.
Despite finding the app highly acceptable and a majority expressing they would like to use it in the future, app users reported no change in regard to their self-efficacy for contraception over the study period, and mixed change in regard to their decisional balance for contraception. While we are unable to determine why there was no change in these dimensions, one possibility is that information and normative messaging via a digital app may be insufficient to shift self-efficacy and decisional balance. Though the app was designed to operationalize health behavior change theory, additional research is needed to explore how self-efficacy and decisional balance for contraception can be better supported and increased. For example, perhaps more engagement with the app, through either more time at intervention or via additional refresher sessions in the intervening period, could significantly support change in these beliefs.
Developing and testing a tailored contraceptive app fills an important research and clinical gap. A 2016 systematic review of 218 pregnancy prevention apps currently available through online stores found that the majority focused on fertility tracking and many lacked information on modern methods of contraception. The review identified 15 contraceptive information apps (Mangone, Lebrun, & Muessig, 2016). Having a wider variety of tailored apps is essential, as studies have shown that apps have promise for youth education (Chavez, Shearer, & Rosenthal, 2014; M. Gilliam, Chor, et al., 2014; Whiteley, Mello, Hunt, & Brown, 2012). Researchers have identified the lack of tailored apps for minority communities as an ongoing challenge in digital media interventions (Chavez et al., 2014). HCD may be an ideal way to create a tailored app through modification and refinement of existing apps. Resulting interventions are based on available technology, address true barriers, and are matched to a realistic understanding of behaviors, skills, and informational needs of the user. As mobile technology proliferates, there is a need to share patient-engaged research methodologies for intervention development. Thus, miPlan, in both its development and evaluation, offers a notable contribution to the current field of mHealth interventions.
Apps have additional benefits such as providing high-quality information with fidelity outside of the clinical setting. Researchers have documented adolescents’ wariness of information on sexual and reproductive health information found on the Internet, finding that young women prefer sources they deem to be reputable and trustworthy (R. K. Jones & Biddlecom, 2011; R. K. Jones, Biddlecom, Hebert, & Mellor, 2011). Apps provide intervention fidelity by ensuring that patients are given correct information that can be updated as new information becomes available. This particular intervention took advantage of the clinic setting to access family planning patients and also because participants could follow up with their provider for further counseling and questions. Future studies might consider how this app performs in the nonclinical setting.
In both content and features, miPlan used behavioral theory to inform app development. Behavioral theories are an important component of behavioral interventions and indeed are the cornerstone of many heath behavior changes (Noar, Benac, & Harris, 2007). Some have argued for the need to employ behavioral theory in contraceptive counseling (Jaccard, 2009). Yet, contraception is a preference-sensitive choice, raising the question of how to think of a behavior change model in the contraceptive counseling setting. On the one hand, the app features all contraceptive methods, engaged women in the app development process, and was intended to precede a routine contraceptive visit including further counseling. On the other hand, only some methods had dedicated videos. Thus, attention must be paid to issues of autonomous decision making (Higgins, 2014). Future studies might assess the feasibility, acceptability, and clinic burden of additional videos and adding information on sexually transmitted infections and condom use.
Study limitations must be noted. First, the app was tailored to African American and Latina women, and, thus designing and assessing the app with other demographic groups might result in different outcomes. Second, we did not measure sense of coercion. This omission was intentional as we deemed it difficult to assess coercion specifically for the app, as women also received counseling and a provider visit. Social desirability regarding the app may have contributed to the highly positive ratings of the app, though post-app surveys were administered via tablet computer in order to minimize such bias. Finally, the app was evaluated by women not already highly intending to use a LARC method. Reactions from women who are at different stages of change might be different.
Conclusion
This study demonstrates the potential value of using user experience design processes for designing an app with specific populations. Users requested and enjoyed the graphics, videos, and tailored information, including the male partner perspective. In a subsequent evaluation, with over one hundred women, the app was highly rated and almost all agreed it was a good use of their time in the waiting room. Apps are particularly promising because they can be digitally disseminated to reproduce information with fidelity. Additional research is needed to gain empiric evidence on scalability and whether young women would use it outside of a research setting associated with incentives, and outcomes when used with other populations.
Footnotes
Acknowledgements
The authors thank Edeliz Flores, Rayna Brown, and Erica Phillips for their assistance with recruitment and data collection.
Authors’ Note
Presented at the North American Forum on Family Planning, November 5-7, 2016, Denver, Colorado. Clinical Trial Registration (ClinicalTrials.gov): NCT02396602.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by a grant from the William and Flora Hewlett Foundation Global Development and Population Program.