
Abstract
Background. India’s National AIDS Control Programme calls for, among other things, targeted behavioral interventions that address determinants contributing to new infections among men who have sex with men (MSM) and hijras (transgender women). Aim. To determine if the information–motivation–behavioral skills model was transferable to an Indian context. Methods. We recruited 442 MSM and 7 hijras into an online cross-sectional study that asked questions about condom use knowledge, motivation, self-efficacy, and sexual behavior. Structural equation modeling was used to test the overall information–motivation–behavioral skills structure. Results. Condom use and HIV risk knowledge did not significantly predict condom use self-efficacy or having condomless anal sex with more than one male partner in the past 3 months, and knowledge was not significantly correlated with attitudes toward barebacking. Despite this, the final structural model explained 14.4% of the variance in condom use self-efficacy and 20.0% of the variance in risky sexual behavior. Overall fit of the model was good: χ2(201, N = 447) = 445.002, p < .0001, root mean square error of approximation = .052, 90% CI [.046, .059], comparative fit index = .989, Tucker–Lewis Index = .987. Conclusion. The public health response to India’s HIV epidemic is currently different than in the West due to differences in medication access and public health infrastructure. As Indian MSM and hijras learn more about the effectiveness of viral suppression and hopefully have greater access to preexposure prophylaxis, researchers should monitor for changing attitudes toward condoms and be prepared to collaborate with the public health infrastructure in order to develop interventions that reinforce positive attitudes toward condom use.
Since the introduction of treatment as prevention and preexposure prophylaxis (PrEP), much of the Western HIV-prevention has focused on early identification, antiretroviral treatment (ART), retention in care, and PrEP-uptake among persons at greatest risk for HIV (Hankins & Dybul, 2013; Young & McDaid, 2014). U.S. men who have sex with men (MSM) living in urban centers or a large gay male community have greater access to ART, PrEP, and support of behavioral interventions (Raymond, Chen, & McFarland, 2016; Raymond et al., 2013). However, Indian MSM have less access to ART, PrEP, and behavioral risk reduction interventions (National AIDS Control Organisation, 2007). Additionally, a weaker health care infrastructure makes it difficult for MSM to access prevention services (Li et al., 2016). Consequently, prevention efforts have focused on increasing condom use, linkage to care, and retention in care when viral load reaches 350 cells/mm3(National AIDS Control Organisation, 2007). To address these gaps, Phase IV (2012-2017) of India’s National AIDS Control Programme calls for the strengthening of the health care infrastructure and the implementation of targeted interventions that focus on determinants of HIV transmission (National AIDS Control Organisation, 2007).
This focus creates an opportunity to develop new theoretically based behavioral interventions that address the determinants driving the infection, such as stigmatizing attitudes toward homosexuality and persons living with HIV (Chakrapani, Newman, Shunmugam, Kurian, & Dubrow, 2009; Chakrapani, Newman, Shunmugam, McLuckie, & Melwin, 2007; Ekstrand, Bharat, Ramakrishna, & Heylen, 2012; Li et al., 2016). Salient determinants include inconsistent condom use, sexual concurrency, substance use, depression and anxiety disorders, a lack of knowledge about safer sexual practices, and less condom use self-efficacy (Brahmam et al., 2008; Chakrapani et al., 2009; Mimiaga et al., 2013; Newman, Chakrapani, Cook, Shunmugam, & Kakinami, 2006; Phillips et al., 2010; Thomas et al., 2009; Thomas et al., 2011).
The information–motivation–behavioral skills (IMB) model (Fisher & Fisher, 1992) attempts to address individual-level determinants by increasing knowledge about a risk reduction behavior and increasing motivation and skills to enact the behavior. Behavioral skills can be measured directly via observation or through measures of self-efficacy (confidence in ability) to perform a skill. Developed to inform HIV-/STI-prevention interventions targeting MSM, interventions theoretically based in IMB have been used to decrease substance use (Avants, Margolin, Usubiaga, & Doebrick, 2004; Avants, Warburton, Hawkins, & Margolin, 2000; Margolin, Avants, Warburton, Hawkins, & Shi, 2003) and increase condom use (Bryan, Fisher, Fisher, & Murray, 2000; Crosby et al., 2008; Nostlinger et al., 2011; Scott-Sheldon et al., 2010) in the United States and Europe.
The purpose of this analysis was to determine if the IMB was transferable to an Indian context. Therefore, we have operationalized the IMB constructs of information as knowledge about condoms effectiveness at preventing HIV. We defined motivation by assessing attitudes toward barebacking, which assesses the individual’s personal motivation to perform a preventive behavior. Finally, we operationalized behavioral skills as condom self-efficacy. Condom self-efficacy assesses the individual’s confidence in his ability to perform the behavior. Based on the model, well-informed and highly motivated individuals will engage in preventive behaviors. Therefore, we hypothesized that among an Indian sample of MSM, having information about HIV would positively predict condom use self-efficacy (confidence in condom use skills), while being motivated toward risky sexual behavior would negatively predict condom use self-efficacy. Conversely, HIV information and condom use self-efficacy would negatively predict risky sexual behavior, and motivation would positively predict the outcome. In line with the IMB model, we hypothesized that self-efficacy would be the strongest predictor of risky sexual behavior.
Method
Study Design
Between September 2013 and May 2014, we recruited 449 MSM and hijras through banner advertisements on gay websites, social media advertisements and posts, and the distribution of print materials at outreach events hosted by LGBT and HIV services organizations in the State of Maharashtra, India. The banner advertisements, social media advertisements and posts, and print materials directed participants to the study website where they could complete the eligibility screen. Eligible participants self-identified as MSM or hijras/transgender women living in the State of Maharashtra, being at least 18 years of age, having regular Internet access, and having at least one male sex partner in the previous 90 days. Once eligibility was determined, participants were provided with an overview of the study. It took approximately 30 minutes to complete the eligibility screener, consent process, and survey in Hindi, Marathi, or English. We translated and back-translated all study materials. For completion of the survey, participants were compensated ₹300 (approximately US$7) in the form of a gift card to an online retailor that supports India’s sexual and gender minority community. The institutional review boards of the authors’ institutions approved the study procedures.
Measures
Participants were asked questions about IMB constructs, online and offline sexual behavior, and demographic characteristics. All data were self-report. Items relevant to this analysis are described below.
Knowledge
To assess the information construct, participants answered four true/false items about condom use and HIV risk (see Table 2 for specific items). We developed knowledge items in collaboration with our community advisory board. We computed a knowledge sum score of all correct responses, which was treated as an observed variable in subsequent structural equation model (SEM) analyses. Higher values indicate more correct knowledge about condom use and HIV risk.
Attitudes Toward Barebacking
The attitudes toward barebacking scale (Halkitis, Parsons, & Wilton, 2003) was used as a proxy for the motivation construct. Participants rated their agreement with nine statements about condomless sex (see Table 2) on a 7-point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree). Higher values indicate more favorable attitudes toward barebacking. Internal consistency was high (α = .94).
Condom Use Self-Efficacy
Confidence in ability to use condoms was indicated by 11 items measuring the condom use self-efficacy construct. Participants were asked how sure they were that they could use a condom in various situations (see Table 2). Items were scored on a 5-point ordinal scale from 1 (not at all sure) to 5 (completely sure), and higher values indicated greater self-efficacy. The items were adapted from items from the Men’s Internet Study (Marin, Gomez, Tschann, & Gregorich, 1997; Rosser et al., 2010). To assess validity of the self-efficacy measure, we conducted an exploratory factor analysis with oblique rotation and a confirmatory factor analysis (CFA) on a 20–80 randomized split of the sample, respectively (Table 1). Although a two-factor solution appeared to have better fit than a one-factor solution, the correlation between the two factors was very high, greater than .95 in the CFA and full samples. Thus, the one-factor solution, which had adequate fit and internal consistency (α = 0.90), was selected.
Model Fit Statistics of Selected Exploratory and Confirmatory Factor Analyses for Condom Use Self-Efficacy.
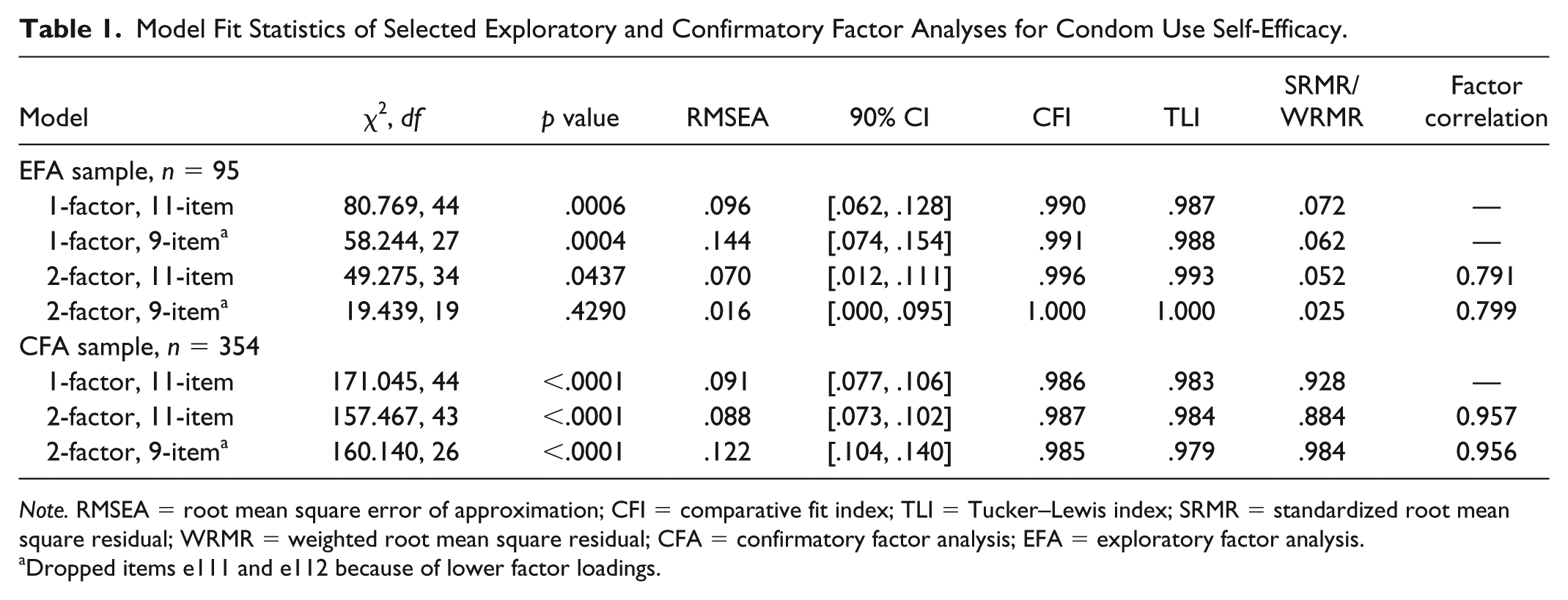
Note. RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker–Lewis index; SRMR = standardized root mean square residual; WRMR = weighted root mean square residual; CFA = confirmatory factor analysis; EFA = exploratory factor analysis.
Dropped items e111 and e112 because of lower factor loadings.
Risky Sexual Behavior
Participants were asked about the number of male and hijra partners they met online or off-line with whom they had insertive or receptive anal sex without a condom in the past 3 months. The four variables were summed to get a total number of condomless anal sex acts (CAS) with male partners and then dichotomized between having one or fewer versus having two or more male partners with whom they engaged in CAS in the past 3 months.
Data Analysis
A CFA was first conducted on the full sample for the latent variable measurement models (i.e., attitude toward barebacking, condom use self-efficacy) to examine data fit. Then, the measurement model was added to the SEM to test the overall IMB structure. Several model fit indices are reported, but model fit was chiefly evaluated using the comparative fit index (CFI) (Bentler, 1990) and Tucker–Lewis index (TLI) (Tucker & Lewis, 1973) because χ2 is affected by sample size and correlations, whereas small degrees of freedom inflates the root mean square error of approximation (RMSEA) (Kenny, Kaniskan, & McCoach, 2014). Values of >.95 for CFI, >.90 for TLI, and <.06 for RMSEA are generally considered an indication of adequate fit (Hu & Bentler, 1999). Descriptive analyses were conducted using STATA 13 (StataCorp LP, 2012), and the exploratory factor analysis, CFA, and SEM were conducted using Mplus 7 (Muthén & Muthén, 2012).
Results
Sample Description
Participant characteristics are summarized in Table 2. Participants ranged in age from 18 to 64 years, with an average age of 29.47 years (SD = 8.28). Almost 56% of the participants were middle or upper class, based on an income of ₹25,001 or more per month, and 85% indicated that they had completed postsecondary education. Approximately 56% reported being open or out about their sexuality to few or half of the people they knew, whereas almost 20% were out to most or all the people they knew; a quarter of the men said that they were not out to anyone at all.
ISHKonnect Participant Characteristics (N = 449).
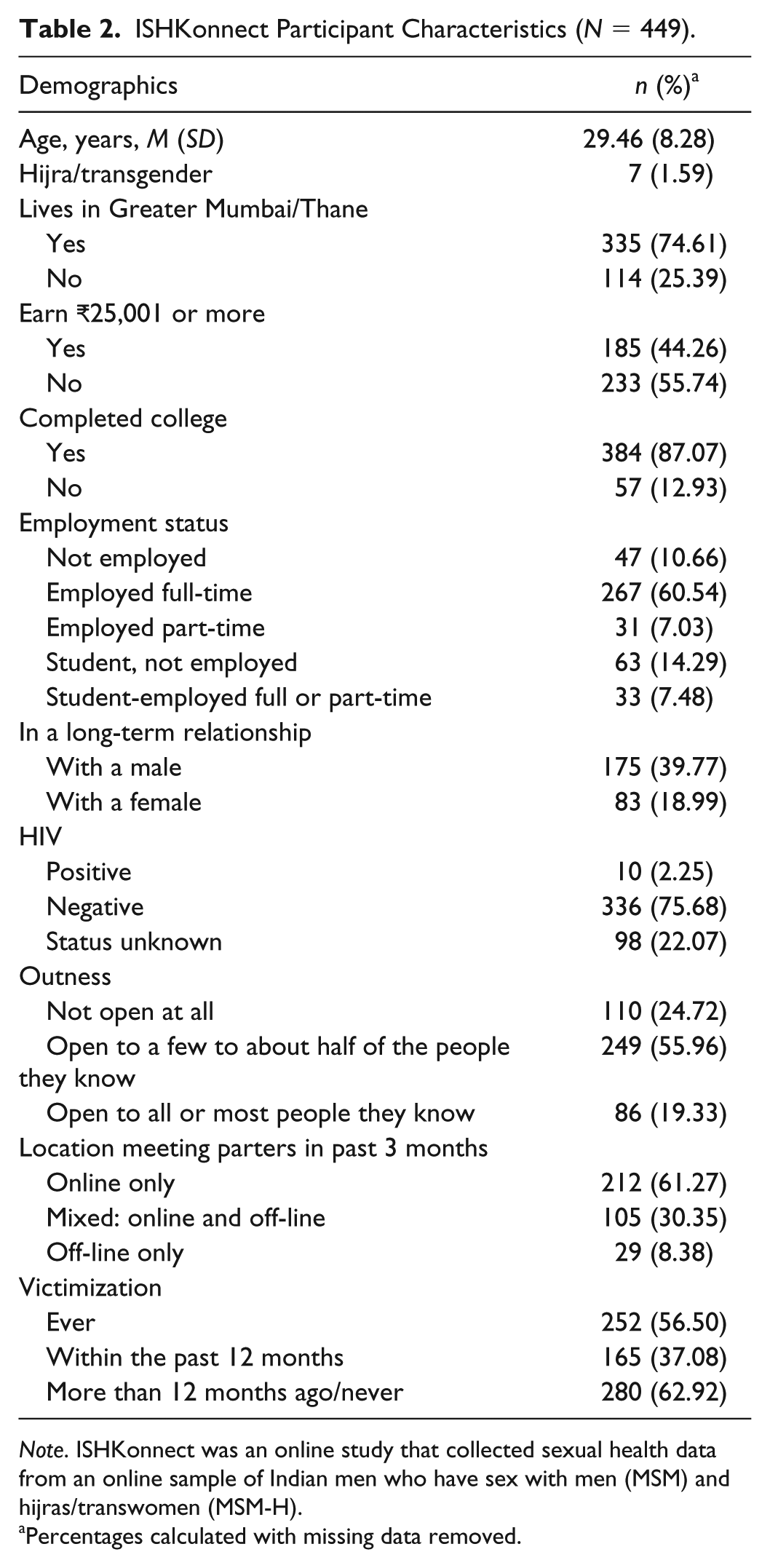
Note. ISHKonnect was an online study that collected sexual health data from an online sample of Indian men who have sex with men (MSM) and hijras/transwomen (MSM-H).
Percentages calculated with missing data removed.
Measurement Models
Table 3 details the mean scores for each item in each of the IMB variables as well as the standardized factor loadings for the attitudes toward barebacking and the condom use self-efficacy scales. For both latent variables, almost all items loaded highly and significantly onto their respective factors. The initial measurement model for attitudes toward barebacking showed no large residuals or outliers, no item correlations greater than .90, and adequate fit according to the CFI and TLI: χ2(27, N = 444) = 496.640, p < .0001, RMSEA = .198, 90% CI [.183, .213], CFI = .966, TLI = .955. Based on the results of the CFI, TLI, and CI fit indices and the hypothesized factor model, we made four modifications to the model to account for theoretical IMB connections between items. These modifications improved the model fit slightly: χ2(23, N = 444) = 288.363, p < .0001, RMSEA = .161, 90% CI [.145, .178], CFI = .981, TLI = .970. For condom use self-efficacy, the one-factor solution showed adequate fit: χ2(44, N = 438) = 192.338, p < .0001, RMSEA = .088, 90% CI [.075, .101], CFI = .988, TLI = .984. There were no large residuals or outliers, and only one item correlation was greater than .90. The condom use self-efficacy model showed evidence of good convergent validity (average variance extracted [AVE] = 0.71) and good composite reliability (CR = 0.96). The attitudes toward barebacking scale showed evidence of good convergent validly (AVE = 0.76) and good composite reliability (CR = 0.97).
Measurement Models and Items for the IMB Variables (N = 449).
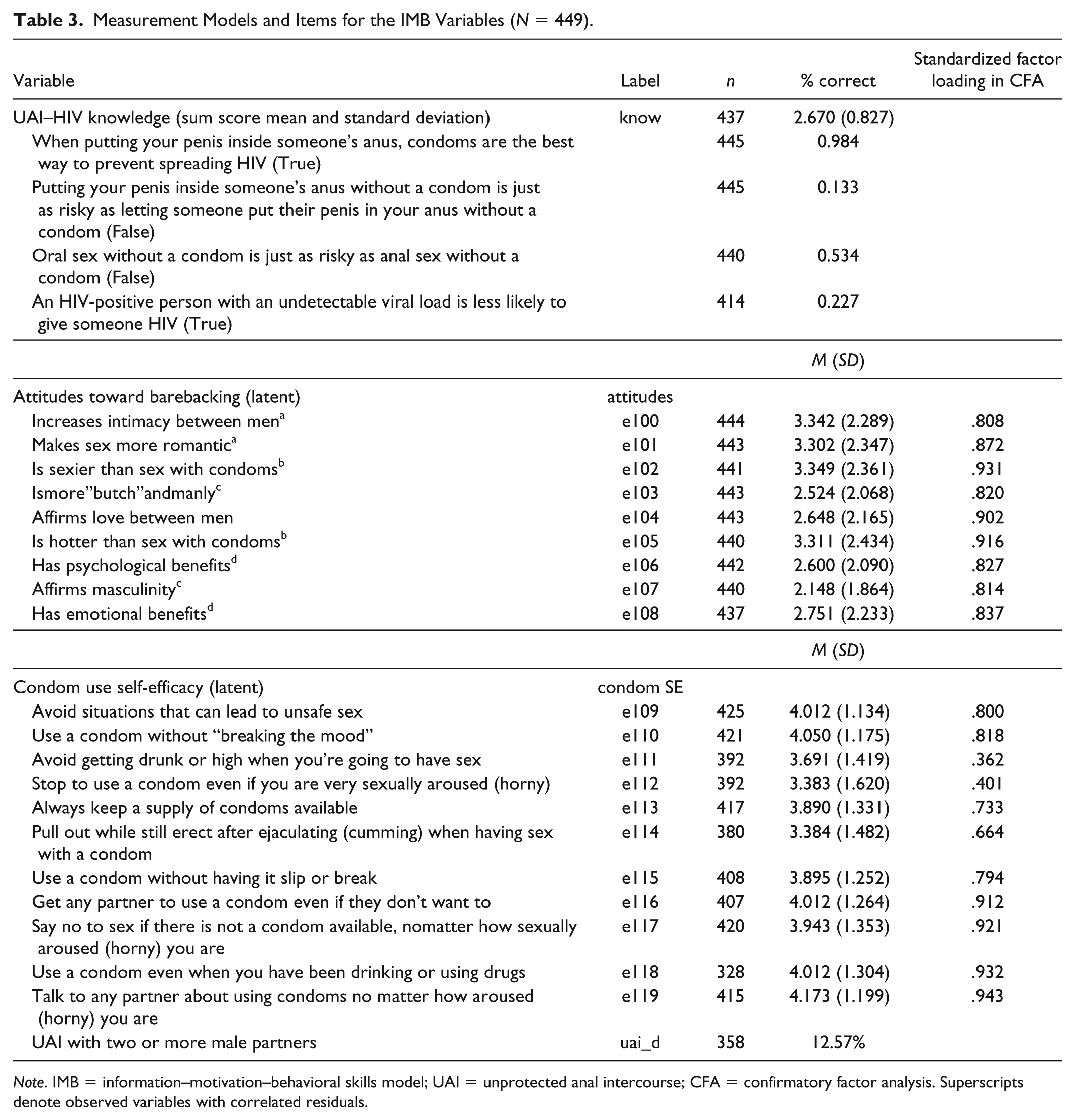
Note. IMB = information–motivation–behavioral skills model; UAI = unprotected anal intercourse; CFA = confirmatory factor analysis. Superscripts denote observed variables with correlated residuals.
Structural Model
Figure 1 shows the final structural model for the IMB SEM among a sample of Indian MSM with standardized path coefficients. We chose WLSMV (mean- and variance-adjusted weighted least squares) estimator because of our ordinal data. Overall fit of the model was good: χ2(201, N = 447) = 445.002, p < .0001, RMSEA = .052, 90% CI [.046, .059], CFI = .989, TLI = .987. No post hoc modifications were made because the data fit the model well. All paths were statistically significant except for those associated with knowledge. Condom use and HIV risk knowledge did not significantly predict condom use self-efficacy or having more than one CAS male partner in the past 3 months. In addition, contrary to the IMB model, knowledge was also not significantly correlated with attitudes toward barebacking. Despite this, the final structural model explained 14.4% of the variance in condom use self-efficacy and 20.0% of the variance in risky sexual behavior.

Final structural model for IMB in a sample of Indian MSM (N = 449) with standardized path coefficients.
Discussion
The IMB model did not fully perform as predicted in an Indian sample of MSM and hijras. CAS with two or more partners in the past 3 months was associated with proxies for motivation and self-efficacy as hypothesized. Per the IMB model (Fisher & Fisher, 1992), we also hypothesized a negative correlation between knowledge of safer sex strategies and attitudes toward barebacking and positive associations between knowledge and self-efficacy and CAS. Contrary to our hypothesis, there was not a statistically significant association between knowledge and motivation, self-efficacy, and behavior.
Participants’ knowledge of safer sex practices was mixed. The variations in the proportion of correct responses could explain the lack of association between knowledge and the other constructs. While the majority (98%) knew that condoms were the best way to prevent the spreading of HIV when putting their penis inside someone’s anus, only half (53%) could differentiate the risk associated with oral and anal sex. Few knew that more risk was associated with being a receptive anal sex partner than the insertive partner (13%) or that a person living with HIV whose viral load is undetectable is less likely to transmit the virus to someone else (23%). The responses to these items suggest that Indian MSM and hijras have varying levels of information about safer sex practices, but that information is not associated with preventive behavior. Our results support prior findings by Fisher and Fisher (1992, 2000) which found that information does not always translate to motivation. While we cannot fully state that lack of motivation was the predictor of low condom use, we can question the conceptualization the role information has in predicting behavior. More study is required to understand how we can translate a HIV prevention model based on Western data into an Indian MSM context.
As India is not able to provide ART to all persons living with the virus regardless of viral load and PrEP to persons at greatest risk, the information Indian MSM will need to make protective sexual health choices will need to expand beyond the items assessed in this survey. To aid the public health infrastructure in preparing for increased access to medications, future research should begin exploring how to educate Indian MSM and hijras about medication adherence and PrEP.
Overall, the men in our sample tended to disagree with the statements that are positively associated with bareback sex (Halkitis et al., 2003), and the men had fairly high condom use self-efficacy, suggesting that cognitive barriers to condom use when engaging in anal sex are low. As Indian MSM and hijras learn more about the effectiveness of viral suppression and hopefully have access to PrEP, researchers should monitor for changing attitudes toward condoms and be prepared to collaborate with the public health infrastructure in order to develop interventions that reinforce positive attitudes toward condom use.
Limitations and Strengths
There are a few limitations to this study. The knowledge scale was not piloted tested or pretested. In future projects, the knowledge scale should be piloted tested and validated. Self-reported data were from a cross-sectional study, and the sampling frame included only MSM and hijras with access to technology. Longitudinal data would strengthen study findings. The sample included mostly men from Mumbai; many were educated and middle-class. Because the study participants did not differ greatly on personal characteristics, we believe that this could be a threat to internal validity. Findings might not be generalizable to all Indian MSM and Hijras. Although access to the Internet and smartphones is growing in India, disparities to access exist by income and proximity to an urban area (Internet Live Stats, 2016). Despite these limitations, study findings can inform public health practitioners working to implement Phase IV and develop and implement Phase V.
Implication for Practice
Phase IV of the National AIDS Control Programme outlines the nation’s strategy to prevent HIV transmission in India. Relative to MSM and hijras, the program calls for improved access to treatment for persons living with HIV; the reduction of stigma experienced by persons living with HIV and marginalized communities most affected by the virus, including MSM and hijras; and targeted behavioral interventions that address determinants most contributing to new infections (Government of India Ministry of Health and Family Welfare, 2012). Findings from the current study will inform future development of prevention messages. We believe that our findings suggest that prevention messages should expand beyond increasing knowledge toward safe sex. Consistent with our findings, HIV prevention messages should increase self-efficacy to use condoms under difficult circumstances (e.g., while using drugs or alcohol).
The public health response to India’s HIV epidemic is currently different than in the West due to differences in medication access and public health infrastructure. Future phases of the National AIDS Control Programme will likely build on the achievements experienced in Phase IV. In time, it is likely that India will be able to adapt successful viral suppression and PrEP strategies being implemented in the West, so it is prudent to begin planning for how to adapt strategies found successful in Western contexts. While it is also prudent to focus on improving behavioral interventions that increase condom use knowledge, motivation, and self-efficacy, there is a need to identify and understand barriers to condom use not included in the IMB model. It is likely that cultural and structural barriers specific to the Indian context need to be considered. Based on findings from this study, public health practitioners should increase MSM and hijras’s knowledge of condom use and reaffirm positive attitudes and self-efficacy to use condoms when engaging in anal sex with more than one partner. Researchers should explore how to adapt the IMB model for the Indian context.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study Internet-Based HIV Prevention for Indian MSM (ISHKonnect) was funded by the Indian Council of Medical Research, Division of Epidemiology and Communicable Diseases, grant number INDO-US/84/2010-ECD-II and the National Institutes of Health, National Institute of Allergy and Infectious Diseases, grant number 1R21AI094676-01.