
Abstract
Background. The U.S. uninsured rate has dropped significantly since the passage of the Affordable Care Act (ACA), yet insurance coverage remains lower in historically marginalized communities than in the overall population. New consumer engagement approaches that involve these populations are needed. The purpose of this study was to evaluate the effectiveness of the Insuring Good Health Intervention, a website and video series designed to improve engagement with health insurance and ACA reforms. The study was designed and implemented using a community-based participatory research approach. Method. We conducted a lagged-control cluster randomized controlled trial to evaluate Insuring Good Health with racially and ethnically diverse adults seeking services in medically underserved areas within the Detroit, Michigan metropolitan area. Outcomes were assessed at baseline and at 6 and 9 months postintervention, and including self-efficacy, knowledge, beliefs, and intention to seek help with insurance navigation and care. Results. Among 243 participants, mean age was 43.4 (SD = 13) years, and all participants met federal guidelines for poverty. The study had an 86% response rate at 9-month follow-up (n = 209). Compared with the lagged-control group, intervention participants had more positive beliefs concerning preventive care (estimate 0.51, standard error 0.16; p < .01), and intention to seek help with insurance navigation and care (estimate 0.43, standard error 0.17; p < .001) at 9-month follow-up. Hispanic participants benefitted the most from the intervention, including improved knowledge of health insurance eligibility over 9 months compared with other racial/ethnic groups (estimate −0.97, standard error 0.40, p < .01). Discussion. Insuring Good Health was associated with increased intention to seek help with insurance navigation and care, and improved beliefs around preventive care. Conclusions. Insuring Good Health has the potential to be an important consumer engagement tool to reduce disparities in health insurance coverage and care seeking.
Keywords
The uninsured rate has dropped significantly in the United States as a result of health insurance expansions under the Affordable Care Act (ACA; Centers for Disease Control and Prevention [CDC], 2018). However, despite extensive outreach efforts, nearly 28 million people continue to remain uninsured (CDC, 2018), and challenges navigating the U.S. health insurance infrastructure persist. Even 5 years after the passage of the ACA, there were high reports of knowing nothing or very little about the ACA, and lacking basic knowledge with health insurance plan terminology, differences in features across plans, and maintaining health insurance. These trends are particularly heightened among racial/ethnic communities (Ali, Combs, Muvuka, & Ayangeakaa, 2018; Ghaddar, Byun, & Krishnaswami, 2018; Loewenstein et al., 2013; Patel, Jensen, et al., 2018; Politi et al., 2014).
Health insurance enrollment and retention is critical to gains in health status in racial/ethnic communities, where large disparities persist (Artiga, Foutz, Cornachione, & Garfield, 2016). Recent efforts to increase skills in health insurance navigation using in-person workshops and adult learning techniques have shown reduced confusion and increased confidence and health insurance literacy among consumers (Brown, 2018; Brown et al., 2016). A plain-language website to increase capacity to access reproductive health care was appealing to young women, but difficult for them to navigate (Janiak, Rhodes, & Foster, 2013). A limitation to existing approaches is the predominant emphasis on increasing individual knowledge of complex information and a navigation infrastructure that may not be stable over time. The extent to which existing approaches specifically meet the needs of racial/ethnic communities is also unclear. Difficulties with the launch of insurance marketplaces and administrative challenges with Medicaid experienced by consumers (Vargas, 2016) reinforces the importance of consumer assistance with health insurance navigation and enrollment.
Enrollment assisters (also known as patient navigators or certified application counselors) are a new occupational group created by the ACA to provide no cost assistance to consumers exploring health insurance options and applying for coverage. Their primary duties include performing public education and outreach activities, distributing fair and impartial enrollment information on health plans and the availability of federal subsidies, facilitating enrollment in qualified health plans, provide referrals to appropriate agencies for grievances or complaints, and provide all information in a manner that is linguistically and culturally appropriate for the consumer (Goodell, 2013). They are trained and undergo recertification annually. The use of enrollment assisters has been attributed to increase gains in health insurance enrollment rates and less confusion around health insurance in low-income communities (Tolbert, Perry, Dryden, & Perry, 2014). Nationwide, many organizations are involved in enrollment and outreach efforts with the use of assisters. However, consumers are not always aware that these resources are available in their community (Pollitz, Tolbert, & Diaz, 2017).
Issues related to health insurance enrollment and retention are particularly salient to Detroit in Wayne County, Michigan, one of the country’s most segregated and economically disadvantaged major city, where nearly the entire city is designated as medically underserved (Michigan Department of Health and Human Services, 2018). In 2014, Michigan expanded Medicaid. However, in 2015, there were still high rates of uninsurance in areas of Detroit where enrollment assisters were available (Families USA, n.d.).
Detroit has unique strengths, including the expertise of community organizations and residents and their deep knowledge of the history and social and political context of Detroit (Mehdipanah et al., 2018). Drawing on these strengths, the present study built on the long-standing history of the Detroit Community–Academic Urban Research Center (Detroit URC) aimed at fostering and supporting community-based participatory research (CBPR) efforts to increase understanding of and address health inequities in the city. Several community–academic partnerships are evident in Detroit, working together to understand and address complex health inequities in cardiovascular health, increase physical activity, and improve activity-friendliness of neighborhoods (Harvey et al., 2009; Schulz et al., 2001; Schulz et al., 2011). Translating similar approaches of CBPR to the issue of health insurance navigation with, we developed Insuring Good Health—a novel, multimedia intervention to address health insurance literacy challenges, and connect consumers to enrollment assisters—especially in diverse racial/ethnic economically disadvantaged urban communities.
The purpose of this study was to evaluate the effectiveness of Insuring Good Health among predominantly African American, Arab American or Middle Eastern, and Latino/Hispanic residents of urban communities. These three racial/ethnic groups represent a sizable population of Detroit and its surrounding suburbs (80% African American; 8% Latino/Hispanic; and one of the largest concentrations of Arab American or Middle Eastern populations in the U.S.; U.S. Census, 2018). Although each of these groups has different sociopolitical histories, they have commonalities in terms of mistrust with government and medical institutions (Abuelezam, El-Sayed, & Galea, 2018; López-Cevallos, Harvey, & Warren, 2014; Mays, 2012), thus providing further justification for connections to enrollment assisters who can build legitimacy through one-on-one interactions and make clear their distance from government and private entities (Vargas, 2016).
We tested the following hypotheses:
Method
CBPR Partnership
Description of the CBPR partnership is available elsewhere (Patel, TerHaar, et al., 2018). In 2015, researchers at the University of Michigan (MRP, RL) reached out to eight organizations to form the Insure Detroit Steering Committee (SC). These organizations are involved in ACA-related outreach, and/or directly providing care or social services to our populations of interest. Each organization delegated one stakeholder to join the SC. The Insure Detroit SC met once a month to guide the creation, development, and evaluation of the Insuring Good Health intervention. At the first SC meeting, the group adopted a set of CBPR principles (Becker, Israel, & Allen, 2005) and generated operating norms to guide the work of the partnership. Adopted principles included co-learning and capacity building among all partners, shared power and decision making, and balance of research and action for the mutual benefit of all partners. A more detailed description of the CBPR partnership is available elsewhere (Patel, TerHaar, et al., 2018).
Insuring Good Health
The content and focus of Insuring Good Health were informed by focus groups conducted with key racial/ethnic populations in Detroit: African American, Latino/Hispanic, and Arab American or Middle Eastern groups (Patel, Jensen, et al., 2018). Key themes concluded that although health insurance is perceived as important, confusion and frustration persist around health plan benefits and coverage, eligibility requirements and key provisions of the ACA, and enrollment.
The main premise of Insuring Good Health is to effectively link individuals to enrollment assisters—a group that has demonstrated positive impacts on enrollment rates in low-income, diverse racial/ethnic communities (Tolbert et al., 2014). The Insuring Good Health intervention is a website that comprises key messaging around ACA provisions, health insurance eligibility, enrollment and navigation, and elements of coverage to care (Figure 1). It includes eight, high-quality, animated videos of superhero characters who navigate a health insurance/health care issue. The SC liked the theme of superheroes as a familiar concept across cultures, and a way of providing collective identity to the characters (Patel, TerHaar, et al., 2018). In collaboration with the SC, surface structure tailoring was used to foster connections to the website with different racial/ethnic groups of interest, including physical appearance of the characters and offering multiple language modalities for engaging with the website. The website and videos also provided information on both government-sponsored and private insurance options.

Insuring Good Health intervention.
Enrollment assisters appear in all the videos and help the superheroes solve their issues. An “Introduction” video foreshadows the story and enrollment assisters’ role in helping the superheroes navigate their dilemma. A “Conclusion” video brings together the individual stories into a collective message that strongly endorses the use of enrollment assisters for help with health insurance navigation. All videos present the choice of English, Spanish, or Arabic narration and subtitles. Images from the videos are also embedded throughout the website, which provides content that expands what is covered in the videos. A media production and consulting firm was hired to develop a creative concept and story to communicate learning objectives through a series of short videos. Description of the development of Insuring Good Health is available elsewhere (Patel, TerHaar, et al., 2018).
Storytelling techniques and Social Cognitive Theory provide the basis of behavior change for Insuring Good Health. Storytelling is a method of communicating information that can resonate across cultures and literacy levels. It is an effective method for inspiring behavior change that can simplify complex ideas while making them actionable (Hinyard & Kreuter, 2007; Hodge, Pasqua, Marquez, & Geishirt-Cantrell, 2002; Williams-Brown, Baldwin, & Bakos, 2002). Storytelling also lends itself to the application of behavior change constructs from social cognitive theory (Bandura, 1989). Behavioral capability, a construct from social cognitive theory, maintains that if people are to perform a particular behavior, they must know the behavior’s significance and components (knowledge), know how to perform the behavior (skills), and have the confidence to do so (self-efficacy) (Bandura, 1989). A reciprocal dynamic between the person and the social environment leads to behavior change (Bandura, 1989). Insuring Good Health aims to develop individuals’ behavioral capability to seek out assistance in order to reduce barriers to getting, maintaining, and effectively using health insurance. In order to raise self-efficacy around one’s ability to navigate health insurance and health care systems, storytelling methods were used to communicate mastery experience, social modeling via characters, and verbal persuasion. Past experiences that portrayed unsuccessful attempts with navigating health insurance were illustrated in the videos by each character to demonstrate how they overcame barriers, thus highlighting social modeling. Beyond individual factors, environmental factors such as legal status, may preclude individuals from considering their insurance options. Insuring Good Health addresses contextual factors through linking individuals to an enrollment assister to explore options.
Study Design and Sample
A two-arm, cluster randomized controlled design with a lagged intervention scheme for the control group was used to evaluate the effectiveness of Insuring Good Health with racially and ethnically diverse adults in urban communities in Detroit and its surrounding areas in Wayne County, Michigan. Evaluation follow-up for all participants was 6 and 9 months postbaseline. All study procedures were reviewed and approved by the university institutional review board.
Recruitment and Randomization
Inclusion criteria included (a) residents 18 to 64 years of age, (b) self-identified as non-White race, (c) had access to a telephone. Participants were screened and recruited from four local CHCs by research and agency staff. By appointment at the location where they seek services, participants completed informed consent and an interviewer administered baseline questionnaire. Interviews were conducted in either English, Spanish, or Arabic, based on the preference of the interviewee. Interviewers were volunteers at the organizations, who received training in conducting computer-assisted and telephone interviews and intervention delivery. Each participant interview was audited by research staff for duration of intervention delivery and completeness of procedures via checklists to ensure that the intervention was delivered with fidelity.
We conducted blocked-randomization by site to minimize sampling bias. Two CHCs were randomized to the intervention arm, and two were randomized to the lagged-control arm. Participants were assigned to study arms based on where they sought services. Participants randomized to the intervention arm viewed the videos and navigated the Insuring Good Health website during the first appointment, following baseline survey completion. The lagged-control group completed their baseline survey in-person. They also completed an acceptability survey. At 6 months postbaseline, the intervention group completed an interviewer-assisted survey over the phone. The lagged-control group completed their 6-month follow-up survey in person, followed by receipt of the Insuring Good Health Intervention, and acceptability assessment. At 9 months postbaseline, both the intervention and lagged-control group completed interviewer-assisted survey data collection over the phone. Once participants received initial exposure to the intervention (30 minutes with trained research staff), they were asked via survey to identify characters and videos that they found most helpful in order to receive tailored boosters with the website link between follow-ups. Boosters included a picture of their preferred character, a one-sentence learning point associated with that character, and a link to the website. Boosters were sent to participants once a month through their preferred choice of text, e-mail, or postal mail.
Over the 6-month recruitment period (September 2016-February 2017) a total of 822 individuals were identified and assessed for eligibility. Individuals were excluded due to not meeting inclusion criteria (n = 79), declining to participate (n = 359) (common reasons: time, transportation, declined to state reason), and unreachable to complete consent (n = 141). As a result, 243 individuals were successfully contacted, consented to participate, and provided baseline data. To enhance recruitment and retention of participants, a number of strategies were employed including utilizing staff and volunteers at recruitment sites for contact, providing modest monetary incentives, and sending follow-up contact via boosters over the 9-month period. At completion of data collection at 9-month follow-up, a sample size of 209 participants (corresponding to an 86% retention rate), who completed all data collection sessions, was available for analysis. No differences in demographic characteristics were observed between participations who completed the study and those lost to follow-up.
Acceptability of Insuring Good Health
The Intervention Evaluation Form and the Client Satisfaction Questionnaire (CSQ-8) were both adapted to assess acceptability of Insuring Good Health among study participants (Harper, Contreras, Bangi, & Pedraza, 2003; Larsen, Attkisson, Hargreaves, & Nguyen, 1979). Example items included “website made me more interested in the topic,” “I will be able to use the information from the website,” and “I learned a lot from the videos.” Measures of acceptability were dichotomized as yes/no responses.
Outcome Assessments
Self-reported data of the measures below were collected from participants. Our primary outcome was self-efficacy with health insurance navigation, and our secondary outcomes were knowledge on enrollment, eligibility and insurance terms, beliefs with health insurance, care seeking and preventive care, and intention to seek help with insurance navigation and care. Items were adapted from the validated Health Insurance Literacy Measure (Paez et al., 2014).
Self-Efficacy With Health Insurance Navigation
We measured three dimensions of self-efficacy: navigating provision of insurance (Cronbach α = .80), understanding insurance plan (α = .85), and navigating coverage (α = .72). We asked participants to rate their confidence on a 4-point Likert-type scale (1 = not confident to 4 = very confident) in his or her ability to navigate provision of insurance (four items), understand insurance plan (seven items), and navigate coverage (three items). Items comprising each dimension were summed to create a score, with higher scores indicating higher levels of self-efficacy.
Knowledge: Enrollment, Eligibility, Insurance Terms
Participants were asked about their knowledge of the enrollment process for health insurance (seven items) (α = .1), eligibility requirements specific to ACA reforms (five items) (α = .38), and insurance terms such as co-insurance, premium, and deductible (five items) (α = .32), all assessed through true or false responses. Items were summed for each knowledge domain, with higher scores indicating more knowledge.
Beliefs: Health Insurance, Care Seeking, Preventive Care
Participants were asked about their beliefs, specifically the importance they placed on having health insurance (seven items; Likert-type scale response: 1 = strongly disagree to 5 = strongly agree) (α = .61), their care-seeking behaviors (four items; Likert-type scale response: 1 = strongly disagree to 5 = strongly agree) (α = .60), and the importance of preventive care (two items; Likert-type scale response: 1 = not at all important to 10 = extremely important) (α = .50). Items were summed for each belief domain, with higher scores indicating stronger beliefs.
Intention to Seek Help With Insurance Navigation And Care
Participants were asked about their likelihood of engaging in health insurance or care navigation behaviors such as seeking out an enrollment assister for help and finding out what their insurance plan covers (six items) (α = .80). Items were assessed on a 5-point Likert-type scale (1 = extremely unlikely to 5 = extremely likely). Items were summed, with higher scores indicating higher intention to seek help with insurance navigation and care.
Participants were also asked about their demographic and health-related characteristics, and health insurance status.
Data Analysis
All analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC). Descriptive and bivariate analyses were conducted to examine the baseline data of participants by treatment arms to understand the effect of blocked-randomization. Multiple linear regression models with inverse normal transformations on the outcome were used to compare the intervention effects on changes of the following longitudinal outcomes from baseline to both 6- and 9-month follow-up: confidence in understanding insurance plan, confidence in navigating provision of insurance, intention to seek help with health insurance navigation and care, and beliefs on health insurance, care seeking, and preventive care. Inverse normal transformation was used to ensure the normality for the outcomes, a step of variable transformation for the validity of applying classical parametric hypothesis testing or regression methods. Proportional odds logistic regression models were used for the modeling of ordinal categorical outcomes where intervention effects were compared on the changes of the following longitudinal ordinal outcomes from baseline to both 6- and 9-month follow-up: confidence in navigating coverage; and knowledge of enrollment process, eligibility, and insurance terms. Models were adjusted for age, marital status, head of household, educational attainment, household income, residency status, and presence of a chronic disease. We found that these potential person-level confounders were not randomly distributed across intervention arms due to the site-based, instead of person-based randomization we used. The blocked-randomization helped us to balance many site-level factors which, otherwise, were hard to be measured and dealt with in our analyses.
Subgroup analyses through the similar regression models examined outcomes between racial/ethnic groups at 9-month follow-up, specifically between Arab American or Middle Eastern and Latino/Hispanic participants, and African American and Latino/Hispanic participants. Lack of balanced groups at 9-month follow-up precluded a direct comparison between Arab American or Middle Eastern and African American participants. Alpha values less than .05 were considered significant.
Results
Sample Characteristics
Table 1 presents the descriptive statistics for the sample (n = 243). Mean age of participants was 43.4 (SD = 13.0) years, 74% were female, 51% reported being married, and 57% reported that they were the head of their household. Thirty-four percent were African American, 39% were Latino/Hispanic, and 25% were Arab American or Middle Eastern, and 2% reported other race. Thirteen percent of the sample reported an educational attainment of college or above, 58% were not in the work force, and 65% reported an annual household income of less than $20,000. Sixty-eight percent of participants reported having Medicaid insurance, and 17% had no insurance. Sixty-three percent reported being a U.S. citizen, and 73% reported a diagnosed chronic condition.
Demographic Characteristics of Participants by Intervention Groups.
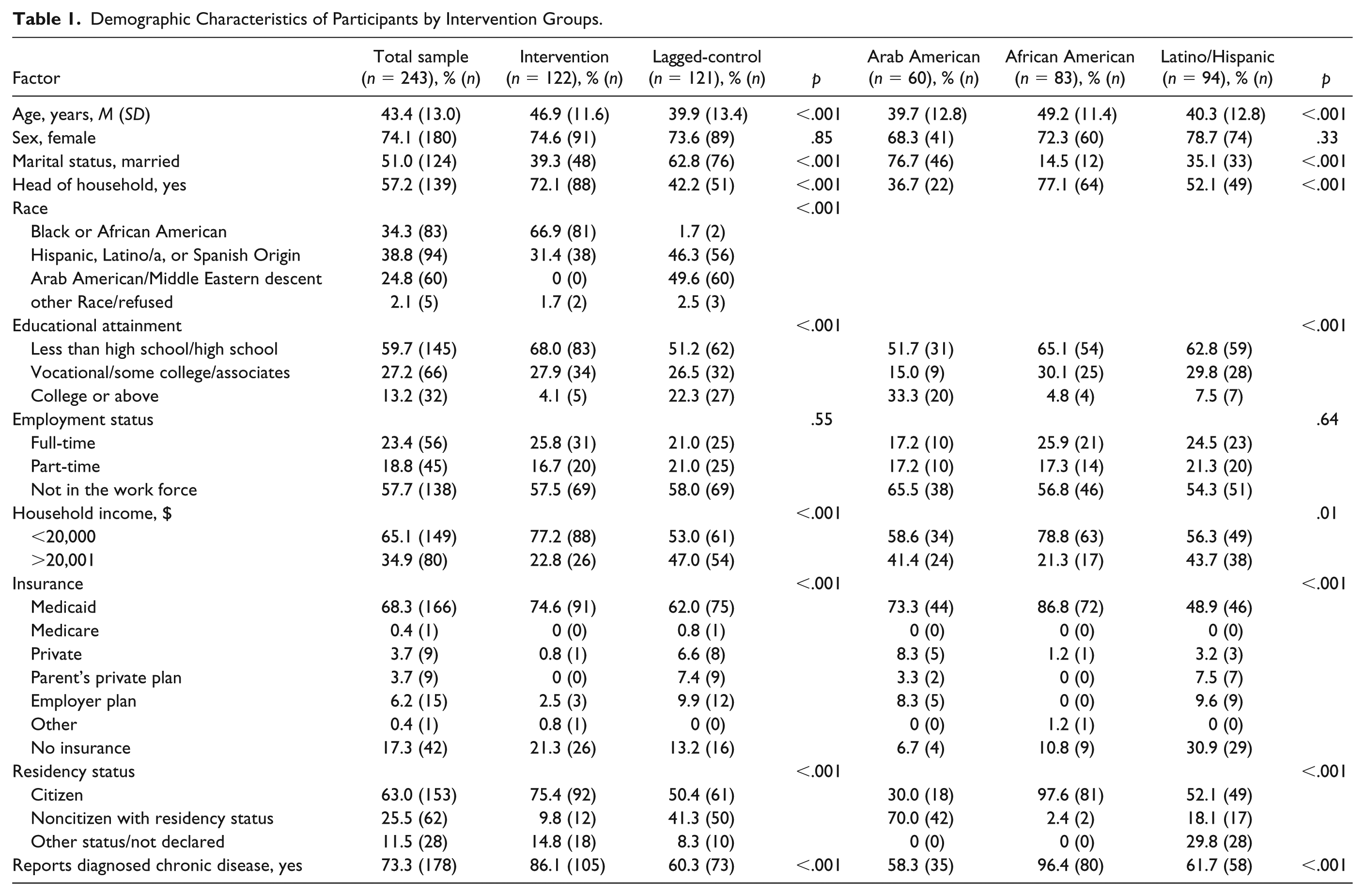
Our recruitment sites were in racially/ethnically segregated communities in Wayne County, Michigan, therefore demographic differences were evident between the intervention and lagged-control group, and between African American, Latino/Hispanic, and Arab American or Middle Eastern descent participants on all indicators except sex and employment status (see Table 1). These differences were anticipated, which were dealt with via the site-based randomization strategy to achieve maximal balance of treatment allocation within each site. Person-level confounders were adjusted for in all subsequent analyses.
Acceptability of Insuring Good Health
Figure 2 shows that Insuring Good Health was highly acceptable across multiple indicators specific to the website, videos, and language-specific features. Specifically, the majority of participants learned a lot, found the topics relevant, and the information provided useful, and would recommend it to a friend.
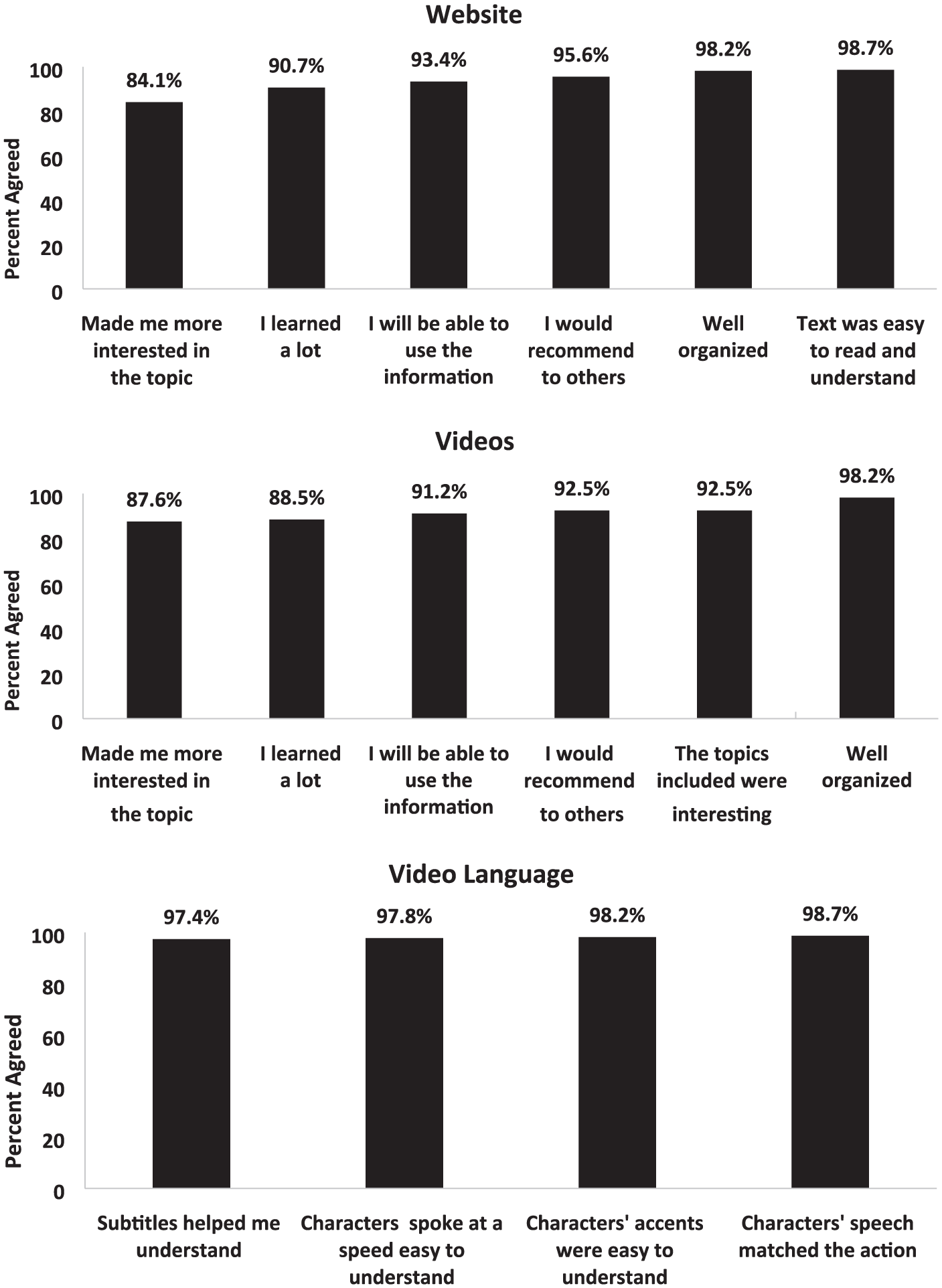
Acceptability of insuring good health.
Differences in Behavioral Outcomes Between Intervention Groups at Baseline
Table 2 shows differences between the intervention and lagged-control group on behavioral outcomes at baseline data collection. Differences between groups was evident for knowledge of insurance terms, with the lagged-control group demonstrating higher baseline knowledge compared with the intervention group (mean 3.46 vs. 3.05, p < .01).
Differences in Outcomes From All Participating Sites Between Intervention Groups at Baseline.

Table 2 also shows differences in behavioral outcomes between racial/ethnic groups at baseline. Latino/Hispanics participants reported lower baseline knowledge on eligibility (p < .01), confidence in both understanding their insurance plan (p < .03) and navigating coverage (p < .01), and intention to seek help with insurance navigation and care (p < .01) compared with African American and Arab American or Middle Eastern participants. Arab American or Middle Eastern participants had much lower beliefs on care seeking compared with African American and Latino/Hispanic participants (p < .001).
Effectiveness of Insuring Good Health
Table 3 shows changes in behavioral outcomes at 6- and 9-month follow-up postbaseline between the intervention and lagged-control groups. At 6-month follow-up post-baseline, no differences in behavioral outcomes were observed between those in the intervention group who engaged with the Insuring Good Health intervention, and the lagged-control group who did not receive the intervention during that time period.
Intervention Effects on Behavioral Outcomes at 6- and 9-Month Follow-up Postbaseline.
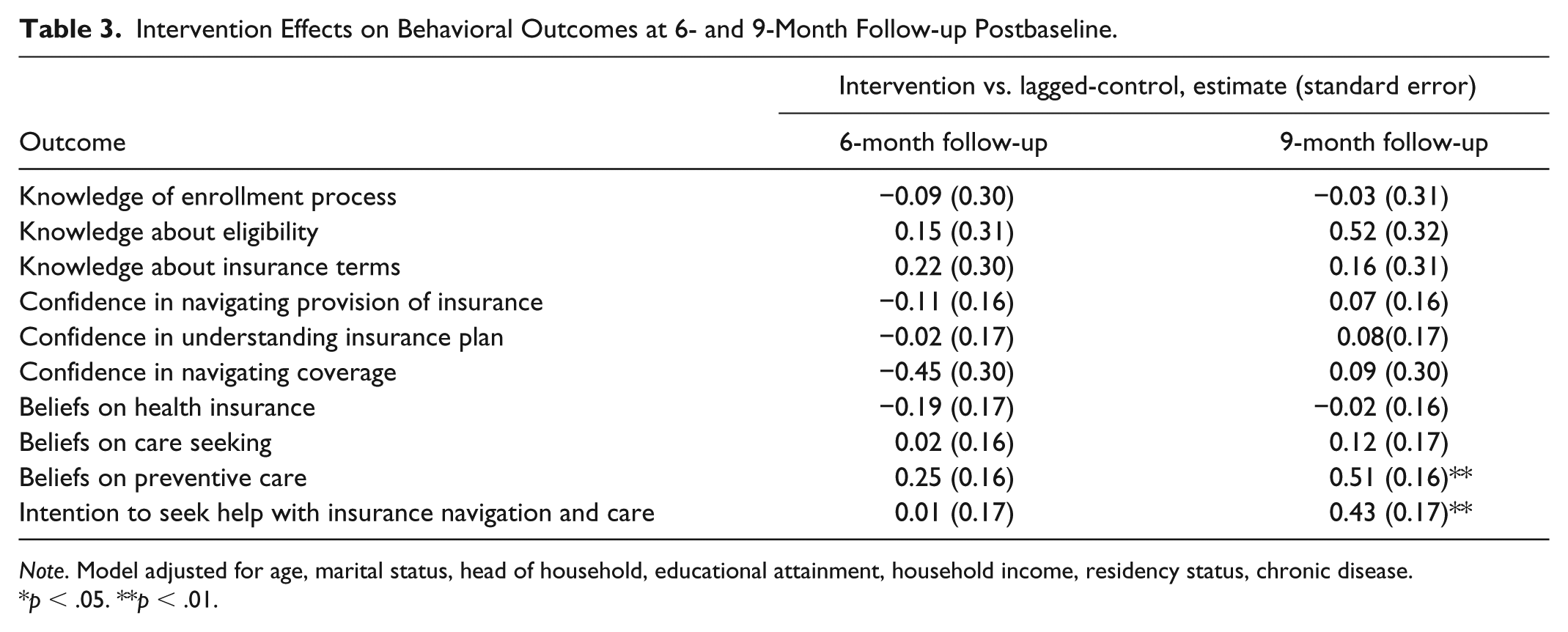
Note. Model adjusted for age, marital status, head of household, educational attainment, household income, residency status, chronic disease.
p < .05. **p < .01.
At 9-month follow-up, participants in the intervention group demonstrated stronger beliefs about preventive care (estimate 0.51, standard error 0.16; p < .001), and greater intention to seek help with health insurance navigation and care (estimate 0.43, standard error 0.17; p < .01), compared with the lagged-control group.
Differences in Effectiveness of Insuring Good Health by Racial/Ethnic Background
Table 4 shows comparisons in changes in outcomes between racial/ethnic background of participants at 9-month follow-up after engaging with the Insuring Good Health intervention. Compared with Latino/Hispanic participants, participants of Arab American/Middle Eastern descent reported lower knowledge of eligibility requirements (estimate −0.97, standard error 0.40; p < .01), confidence in navigating provision of insurance (estimate −0.59, standard error 0.20; p < .004), and confidence in understanding their insurance plan (estimate −0.93, standard error 0.19; p < .001). They also reported weaker beliefs on the importance of health insurance (estimate −0.55, standard error 0.20; p < .01), and preventive care (estimate −0.73, standard error 0.18; p < .001) compared with participants of Latino/Hispanic descent.
Differences in Outcomes by Racial/Ethnic Group at 9-Month Follow-Up.
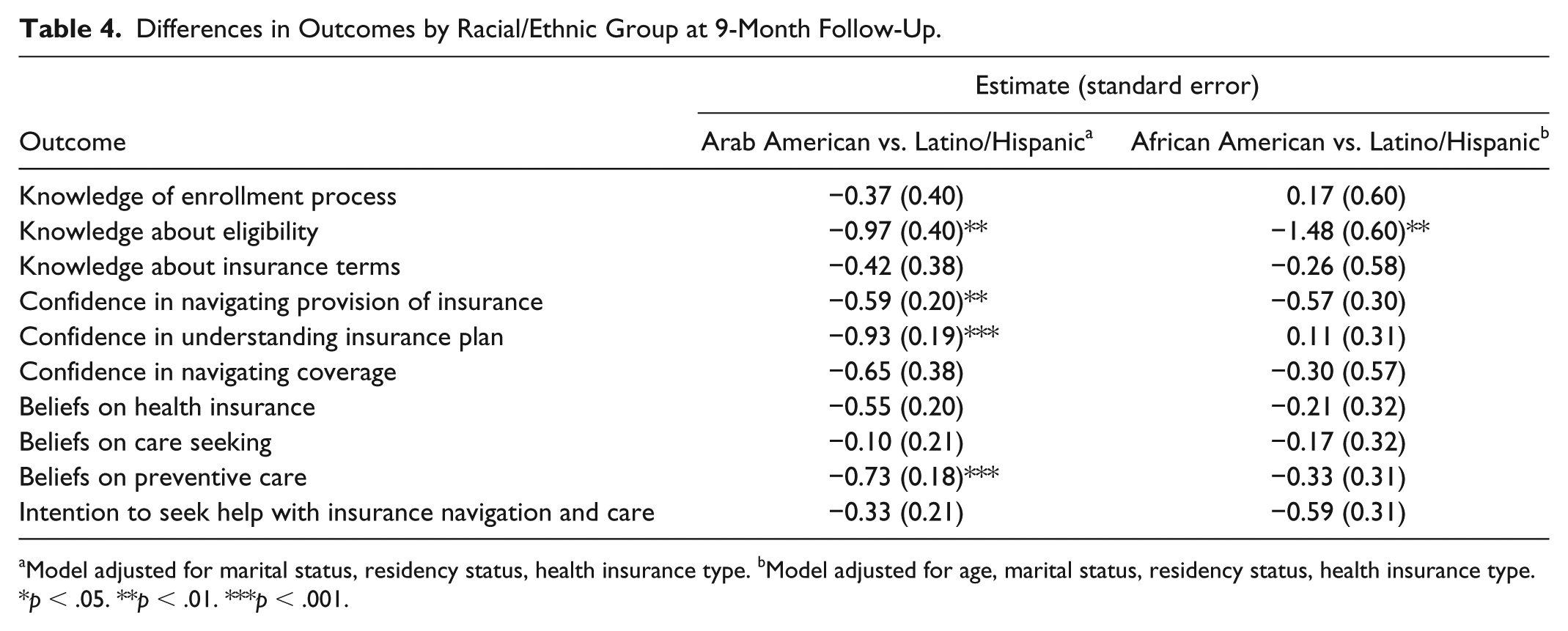
Model adjusted for marital status, residency status, health insurance type. bModel adjusted for age, marital status, residency status, health insurance type.
p < .05. **p < .01. ***p < .001.
Compared with Latino/Hispanic participants, African American participants demonstrated lower knowledge of eligibility requirements (estimate −1.48, standard error 0.60; p < .01). No other differences were observed between groups.
Discussion
This is the first study we are aware of that has used CBPR principles to develop and evaluate an intervention post-ACA to improve engagement with health insurance navigation, especially in a racially and ethnically diverse urban community. Although ACA coverage expansions have been successful in reducing long-standing disparities in access to care, barriers persist in optimizing enrollment and use of health insurance. We evaluated the acceptability and effectiveness of Insuring Good Health among racially and ethnically diverse residents of urban communities via a randomized-controlled lagged trial design with 6- and 9-month follow-up. Diverse racial/ethnic groups responded positively to Insuring Good Health, including the videos and website and language features. We found that long-term exposure to Insuring Good Health resulted in stronger beliefs around preventive care and stronger intention to seek help with health insurance navigation and care. We also found that racial/ethnic subgroups in our study showed differential benefit from Insuring Good Health.
This study did not show the benefit of Insuring Good Health on outcomes of interest compared with usual practice at the 6-month follow-up. However, we did observe that individuals who engaged with Insuring Good Health and its messaging over the full 9-month follow-up period reported stronger beliefs around preventive care and stronger intention to seek help with health insurance navigation and care. One reason for this may be greater exposure by the intervention group to features of the narrative elements of Insuring Good Health, specifically characters overcoming common challenges and meeting their personal goals in relatable health situations. Over the follow-up period, we had routinely sent participants booster messages with a link to the website that reflected their preferred video character. Prior work has shown that narrative messages that illustrate their content with concrete and realistic characters produced greater engagement with message content and an indirect effect on intention through engagement (Kim, Bigman, Leader, Lerman, & Cappella, 2012). Although Insuring Good Health incorporates multiple behavior change elements including storytelling and vicarious experience, culturally compatible multicomponent strategies may be needed to demonstrate short-term and more immediate changes in behavioral outcomes such as goal setting, coaching, or peer-support. Prior studies also provide supportive evidence that interventions that use more behavior change techniques are more effective than those that use fewer behavior change techniques (Webb, Joseph, Yardley, & Michie, 2010).
We also found that Latino/Hispanic participants realized more benefit from Insuring Good Health than did African American participants and those of Arab American or Middle Eastern descent. The benefit was specifically seen with knowledge about eligibility, confidence in health insurance navigation and understanding their insurance plan, and beliefs around having health insurance and seeking preventing care. Other work suggests that as a whole, Latino/Hispanic communities especially required different outreach approaches related to health insurance enrollment and navigation. National surveys show that African American and Latino/Hispanic populations in the United States achieved significant gains in coverage from the ACA (Artiga, Foutz, & Damico, 2018). This was especially evident for Latinos, who were significantly more likely than any other racial/ethnic group to be uninsured (Doty & Collins, 2017). The literature also indicates that even 2 years after ACA implementation, Latinos’ awareness and knowledge regarding ACA and its various provisions and expanded eligibility requirements and options were low (Garcia Mosqueira, Hua, & Sommers, 2015). Thus, engaging with linguistically compatible outreach through Insuring Good Health appears to show benefit in improving critical behavioral outcomes for Latinos when it comes to health insurance navigation.
Baseline knowledge about the eligibility requirements and specific features of the ACA were already quite high for African American and Arab American/Middle Eastern participants in our study. However, care-seeking was found to be lower among Arab American/Middle Eastern participants at baseline and was not changed as a result of engaging with Insuring Good Health. Our preliminary work that informed the intervention did not show significant differences in health insurance-related needs among our racial/ethnic groups of interest. However, the social and political environment both related and unrelated to the ACA has affected each of these groups on a national scale since the inception of our study. As a result, these other factors may have impacted participant’s priorities, attitudinal factors, and confidence with health insurance navigation.
There are several limitations that should be noted. We were not able to collect demographic data on the pool of individuals who were approached about the study but declined to participate or were unreachable to complete consent. Although conceptually aligned, measures that comprised our knowledge scores had low reliability and should be interpreted with caution. We relied on self-report data to minimize burden to busy and underresourced community-based clinics and centers. Data may be subject to social desirability bias. We relied on interviews with our steering committee members to determine the dose of the intervention, which may not always translate to dose needed to achieve efficacy in the outcome of interest (Voils et al., 2014). This study aimed to measure key behavioral outcomes. We recommend that future studies explore objective outcomes such as care seeking, and follow-up with enrollment assisters. Although individuals may have shown stronger intention in our study to seek out assistance, barriers may still be evident such as the potential of a reduced navigator workforce as a result of funding cuts. However, through our steering committee who are well-connected to the local area, we know that organizations are investing in the retention of navigator services despite threats to federal funding. Asking about follow-up with an enrollment assister was a missed opportunity in our study. Lack of balanced groups at 9-month follow-up precluded a direct comparison between Arab American or Middle Eastern and African American participants in examining changes in outcomes between racial/ethnic groups. The lagged-control study design and clustering of racial/ethnic groups by site precluded examination of outcomes within each racial/ethnic group. Future studies should also consider mixed methods evaluation approaches to better understand the health insurance experiences of participants after involvement in the intervention. The sample consisted of individuals who seek services at low-income clinics and social service agencies in Metro Detroit and may not be representative of all individuals who are not connected to these services.
Notwithstanding these limitations, this study has important implications for research and practice. In late 2017, federal funding to support health insurance navigator programs under the ACA were cut by 41% on average and as high as 92% in some areas (Pollitz et al., 2017). These cuts disproportionately affected the Midwest and South. Insuring Good Health is a unique health insurance navigation tool because of its emphasis on utilizing enrollment assisters to overcome common challenges with health insurance. Insuring Good Health has the potential to be a useful tool for community-based organizations to support outreach efforts in the face of these funding cuts. The positive reception of Insuring Good Health from diverse community members and its ability to change several, important behavioral outcomes support this favorable outlook. The website can be promoted at minimal to zero cost to organizations. More trials are also needed to better establish the generalizability and impact of Insuring Good Health in diverse racial/ethnic communities. More trials should also test the specific features of the website and videos on improved outcomes and consider increasing the intervention dose with motivational interviewing or peer-support.
Footnotes
Acknowledgements
We would like to acknowledge the contributions of all the individuals at our partner sites who have contributed to this study: Latino Family Services, Community Health and Social Services (CHASS) Center, Arab Community Center for Economic and Social Services (ACCESS), Covenant Community Care, Mercy Primary Care Center, Enroll America, the Michigan Primary Care Association and the Health Disparities Reduction and Minority Health Section of the Michigan Department of Community Health. We appreciate the support provided by the Detroit Community-Academic Urban Research Center. We thank Honey Locust Health, study staff and participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This study was funded through the National Institute for Health Care Reform (UM#N019071)