
Abstract
Background. Highly processed foods are inexpensive and abundant in our food supply, nutritionally poor, and disproportionately marketed to minority youth. This study is part of a curriculum development project to develop, implement, and evaluate the In Defense of Food (IDOF) curriculum designed to increase intake of whole/minimally processed foods and decrease intake of highly processed foods in youth. Aims. This pilot outcome evaluation was undertaken to assess initial effectiveness and to provide an in-depth understanding of changes in behavioral outcomes and psychosocial mediators. Methods. We used an explanatory mixed method approach, including a single-arm pretest–posttest of intervention effect, followed by a food rules assessment and in-depth interviews to describe participant responses to the intervention in more detail. The study was conducted in three afterschool classrooms in urban low-income neighborhoods with 32 multiethnic middle-school youth, receiving 10 weekly 2-hour sessions. Results. Two weeks postintervention, there was a large positive significant increase in whole/minimally processed food intake (p < .01; d = 0.59) and a small decrease in consumption of highly-processed foods (p = ns; d = 0.06), compared with baseline. Significant increases in psychosocial mediators: Self-efficacy and positive outcomes expectations were seen; others were not significant but changed in the desired direction. Qualitative assessments suggest that the intervention promoted skill building, but environmental barriers made these difficult to use. Discussion. The IDOF curriculum may be most effective for promoting consumption of fruits and vegetables, rather than decreasing intake of highly processed foods. In addition, in this young age-group, short actionable food rules may support self-regulation and behavior change. Conclusion. Among adolescent students in low-income urban neighborhoods, the IDOF afterschool curriculum may help promote self-efficacy and positive outcome expectancies and increase fruit and vegetable intake. Focusing on food processing and using “Food Rules” may be promising to elicit behavior change in youth; however, greater supports are needed to overcome social and environmental barriers.
It is commonly accepted that the current “Western” lifestyle is contributing to the pandemic of chronic diet-related diseases in the United States (Amine et al., 2002; Gootman, McGinnis, & Kraak, 2006; World Cancer Research Fund & American Institute for Cancer Research, 2007). A shift in diet quality and increased rates of diet-related diseases correspond with the rapid increases in and availability of “fast” or “convenience” ready-to-eat and ready-to-heat highly processed foods (HPF) and drink products (Popkin, 2006; Poti, Mendez, Ng, & Popkin, 2015).
“Processed foods” are defined as foods (other than raw agricultural commodities) that are classified based on the extent to which they have been altered from their natural state (Dietary Guidelines Advisory Committee, 2015). All foods exist on a spectrum of processing from unprocessed or minimally processed, like fresh fruits or milk, to those that are highly processed (containing multi-ingredient, industrially formulated mixtures), as found in most fast foods and packaged convenience foods (Poti et al., 2015). On average, HPFs have a higher proportion of fat, sugar, and salt compared with less processed versions (Poti et al., 2015); they are substantially cheaper than more healthful options (Drewnowski & Darmon, 2005; Drewnowski & Specter, 2004); and tend to lead to a greater consumption of overall calories (Chandon & Wansink, 2012; Poti et al., 2015). Emerging research indicates that diets predominated by HPF tend to be nutritionally poor compared with those composed of mostly whole foods (Moubarac et al., 2013; Poti et al., 2015).
American youth can easily access and select HPF, which are cheap and abundant in the food supply and heavily marketed to them. Billions of dollars per year are spent by the food industry marketing highly processed junk food to young people—a vulnerable population who are unable to fully understand the persuasive intent of marketing strategies. Furthermore, Black and Hispanic youth are disproportionately targeted by the food industry, which has direct impacts on their selection and consumption of these foods (Cairns, Angus, Hastings, & Caraher, 2013; Harris et al., 2013; Harris et al., 2015).
Rather than pinpointing a particular nutrient or an individual food as the culprit of the health complications that adolescents are facing, it is becoming increasingly clear that a number of behaviors that define a dietary pattern, such as whether a person consumes a large amount of various processed foods (sugar-sweetened beverages, processed-packaged snacks, and fast food) compared with whole foods (fruits and vegetables [FV]), may influence whether a person can maintain energy balance and optimal health over the long term (Baranowski, Cerin, & Baranowski, 2009; Moreno et al., 2010; Popkin, 2006; Poti, Duffey, & Popkin, 2014).
Although processed foods have come to dominate the American diet, few nutrition initiatives aim to specifically and explicitly provide the message to eat less HPF. Among those who have brought to the attention of the American public the importance of healthy eating patterns, as opposed to a focus on individual nutrients, is Michael Pollan. His book, In Defense of Food (Pollan, 2008), highlights the dietary approach of eating less HPF and more whole/minimally processed plant-based foods.
This study provides a pilot outcome evaluation for the In Defense of Food (IDOF) curriculum (Bhana, Koch, Uno, & Contento, 2016) for afterschool, based on Pollan’s book In Defense of Food and aimed at decreasing intake of HPF and increasing intake of whole/minimally processed foods (W/MPF) in youth. The aim of the study is to assess initial efficacy and to provide an in-depth understanding of the potential behavioral outcomes and psychosocial mediators of youth participating in the curriculum. This study is part of a larger curriculum development project, described elsewhere, composed of an initial curriculum development assessment (Luesse & Contento, in press), a detailed description of the development of the curriculum (Luesse, Koch, & Contento, in press), and its process evaluation (Bhana, 2017).
Method
Study Design
The outcome evaluation utilized an explanatory mixed-methods approach (Creswell & Plano Clark, 2007) in which pretest–posttest survey data were collected, followed by open-ended one-on-one assessments and semistructured in-depth interviews. The Program Evaluation Lifecycle conceptual framework was considered to ensure the alignment of the program lifecycle and evaluation lifecycle (Scheirer et al., 2012; Urban, Hargraves, & Trochim, 2014) by matching a mixed methods pretest–post approach to the early life stage of the program. This framework suggests that the evaluation of a program should match the stage of development of the program. Programs at their initial stages of development and implementation are undergoing rapid and often substantial changes and therefore should be accompanied by evaluation plans that emphasize internal consistency, measure implementation factors, and select outcomes within intervention groups, rather than between groups, to ensure more effective and efficient use of resources (Bowen et al., 2009; Urban et al., 2014; Zapka, Goins, Pbert, & Ockene, 2004). At the early stages of development and evaluation of a health promotion program, modifications and adjustments based on a new program’s application to a new setting and population may be apparent. Thus, a range of evaluation levels (e.g., process and outcome) are often suggested to strengthen the ability to accurately measure outcomes (Kozica, Lombard, Hider, Harrison, & Teede, 2015).
IDOF Curricular Components
Overview
IDOF is a health education curriculum for youth (Grades 6 to 8) designed for an afterschool setting. The principal author with the support of a curriculum development team at Teachers College, Columbia University, developed the IDOF curriculum (Bhana, 2017; Bhana et al., 2016). It consists of 10 sequential 2-hour educational lessons and is the companion guide to the Public Broadcasting Services documentary film In Defense of Food based on Pollan’s best-selling books In Defense of Food (Pollan, 2008) and Food Rules (Pollan, 2009).
The curriculum was designed to help youth become critical of the corporate food supply and familiar and confident to select and prepare W/MPF. In doing so, the curriculum aims to challenge students’ current perceptions of what “food” is by combining activities that have “shock appeal,” such as unveiling cunning marketing strategies, along with preparing and eating W/MP dishes with the objective of making these foods fun and cool.
The lessons are structured into three units, consisting of three lessons each, followed by a final celebration lesson, that highlight a particular concept related to Pollan’s seven-word axiom for healthy eating (Eat food. Not too much. Mostly plants). Table 1 provides a detailed outline of the curriculum and its components.
Description of In Defense of Food Curriculum Components.
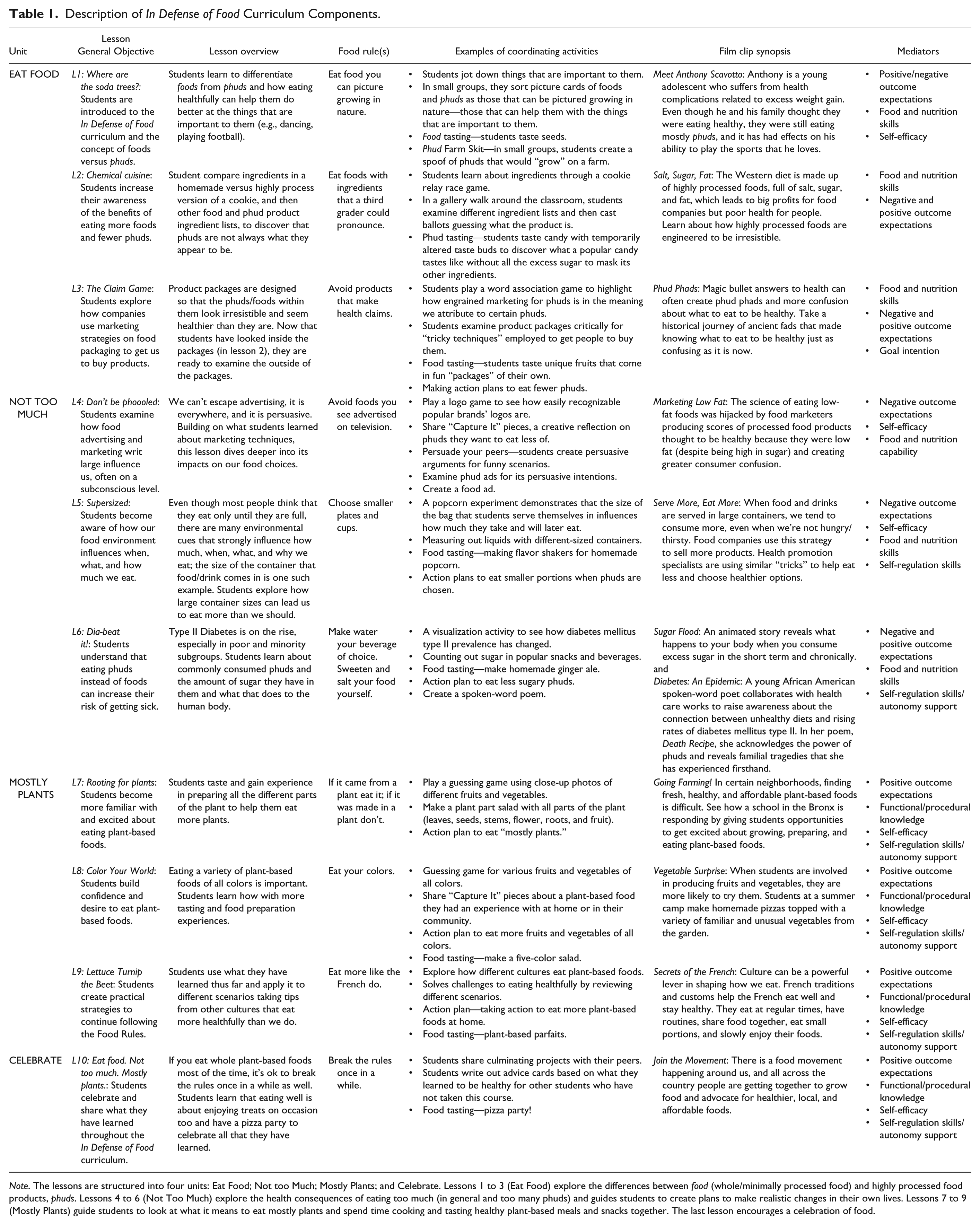
Note. The lessons are structured into four units: Eat Food; Not too Much; Mostly Plants; and Celebrate. Lessons 1 to 3 (Eat Food) explore the differences between food (whole/minimally processed food) and highly processed food products, phuds. Lessons 4 to 6 (Not Too Much) explore the health consequences of eating too much (in general and too many phuds) and guides students to create plans to make realistic changes in their own lives. Lessons 7 to 9 (Mostly Plants) guide students to look at what it means to eat mostly plants and spend time cooking and tasting healthy plant-based meals and snacks together. The last lesson encourages a celebration of food.
Food Rules
Each lesson provides a take away “Food Rule” to help youth put the lesson’s theme into action. For example, Lesson 5 presented the food rule “Choose smaller plates and cups,” helping youth eat smaller portions of HPF.
Film Clips
Each lesson also introduces a film clip from the documentary film to reinforce the themes and messages of the lesson and provides opportunities for thoughtful discussions.
Food Preparation/Tastings
Most lessons provide a food preparation/tasting component to introduce youth to tasty and healthful foods and provide them with the skills to select and prepare W/MPF.
Goal Setting
Most lessons provide youth with goal-setting and self-regulation skills by having them complete written action plans aimed at developing specific, actionable, and measurable goals to eat more W/MPF and eat fewer HPF.
The IDOF Theoretical Model
The curricular objectives are grounded in the social cognitive theory (Bandura, 1986) and the self-determination theory (Deci & Ryan, 1985) mediators (also referred to as determinants) of positive and negative outcome expectations, attitudes, goal intention, factual/procedural knowledge and skills, self-efficacy, autonomous motivation, and self-regulation skills. Self-efficacy, outcome expectations, and self-regulation skills have been cited in the literature as predictive of health behavior change as it relates to FV and decreasing sugar and fat intake in adolescents (Dewar, Lubans, Plotnikoff, & Morgan, 2012; Schnoll & Zimmerman, 2001).
The behavioral outcomes are to increase intake of W/MPF, operationalized as FV, and decrease intake of HPF, operationalized as sugar-sweetened beverages, fast foods, and processed-packaged snacks.
Teacher Training and Curriculum Implementation
The study was conducted over a 14-week period in the fall of 2015; lessons were taught by the regular afterschool program teachers, one lesson/week, over 10 weeks. Prior to implementing the curriculum, study investigators conducted a 2-hour professional development training for all the teachers from the participating sites. Teachers were given an additional hour of training 2 weeks into the curriculum and further support as needed throughout the curriculum delivery period.
Recruitment and Participation
We distributed recruitment flyers in person to afterschool program directors (n = 70); 15 expressed interest in participating in this study. Sites that included an afterschool program accommodating low-income, minority middle school–aged youth and could facilitate weekly 2-hour lessons were invited to participate in the study. Initially, four sites were eligible and expressed continued interest; however, two dropped out before the start of the intervention for scheduling and logistical reasons. The remaining two afterschool program sites in low-income neighborhoods in New York City were enrolled in the study to offer the curriculum across three classrooms (one classroom at Site 1 and two classrooms at Site 2). All procedures, surveys, and protocols were approved by the Teachers College, Columbia University review committee on the protection of human participants. Parents consented to student participation, and students provided informed assent. All enrolled youth at the two respective sites received the IDOF curriculum; however, only those with written parental consent were included in the evaluation. Participating youth and teachers received a gift valued at $20 for their time.
Description of the Outcome Evaluation
A flowchart is presented in Figure 1.
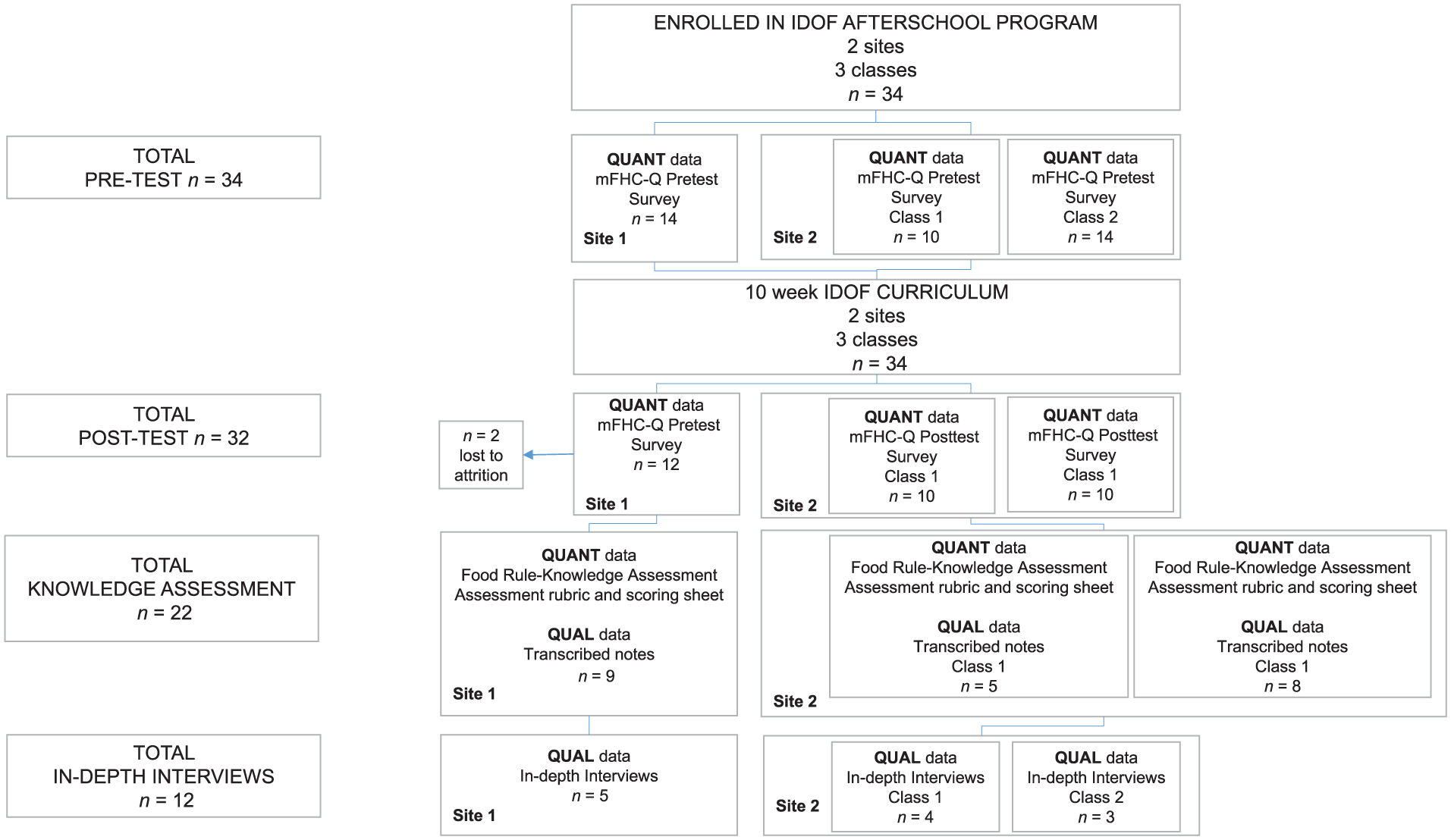
A mixed methods study flowchart.
Instruments and Data Collection and Analysis
Pretest–Posttest Survey
A self-report previously validated instrument, FHC-Q (Gray, Koch, Contento, Bandelli, & Di Noia, 2016), was modified for this study, mFHC-Q, (approximately 55 minutes), measuring frequency of W/MPF and HPF intake; six hypothesized theoretical mediators of W/MPF and HPF intake (described below); and demographic variables (age, ethnicity, and gender). The survey was administered with students a week prior to and 2 weeks after the delivery of the curriculum using an electronic audience response system.
The food and beverage behavioral outcome items in the FHC-Q were adopted from the Beverage and Snack Questionnaire (BSQ; Neuhouser, Lilley, Lund, & Johnson, 2009) previously validated in middle school–aged youth against 4-day food records. The psychosocial mediators in the FHC-Q, included in the mFHC-Q, underwent two cognitive testing sessions with elementary school-aged children to ensure student’s understanding of the survey questions as well as for test-retest reliability testing (Gray et al., 2016).
Each behavior or mediator was represented by a scale with three to nine items. Questions for behavioral outcomes were asked with the stem, “In the past week, I ate/drank . . .,” and response options included “0 times,” “about 1-2 times,” “about 3-4 times,” “almost every day,” and “2 or more times every day.”
Items measuring fruit and vegetable intake (e.g., apples, broccoli, carrots) and highly processed food intake (e.g., fast food, sweetened beverages, processed-packaged snacks) were presented with a picture of the foods or beverages being assessed.
For the psychosocial mediators, items used a 5-point Likert-type scale with scores ranging from 1 to 5 (with higher scores reflecting more of each construct). Specific mediators related to the target behaviors included positive and negative outcome expectations (e.g., Eating FV helps my body do what I want it to do; Drinking sweetened beverages contributes to my developing diabetes), self-efficacy (e.g., I am sure I can eat vegetables at dinner), attitudes (e.g., Eating FV is important to me), and goal intention (e.g., I would like to eat more FV). General mediators, those related to health behavior change overall, included self-regulation skills (e.g., I know how to keep track of my food intake) and autonomous motivation (Eating healthy is an important choice I really want to make).
Pretest and posttest data were analyzed using the Statistical Package for the Social Sciences (SPSS), v24 (2016). Mechanical errors with the audience response system in pretest and suboptimal Cronbach’s alpha coefficient values led to the removal of goal intention and attitudes from analysis. Cronbach’s alpha coefficient values for all remaining mediators ranged from 0.72 to 0.90 rendering a 46-item questionnaire for analysis. We calculated descriptive statistics and used paired t tests to evaluate baseline to postintervention changes in behavioral outcomes and psychosocial mediators. We used Cohen’s d to calculate effect size by taking the mean difference between pre and post values and dividing by the standard deviation for each behavioral outcome and psychosocial mediator.
Food-Rule Assessment
We applied an analytic rubric to assess the depth of comprehension that students need to demonstrate understanding (Allen & Tanner, 2006) of each of the 11 Food Rules when provided the assessment prompt “What does this Food Rule mean? How would you use this Food Rule?”
The lead investigator (female) conducted the Food-Rule assessments using the two aforementioned open-ended questions with a subsample of the cohort (represented from each classroom and selected based on high attendance throughout the program). All Food-Rule assessments were held in a private room at each site over a 2-week period after curriculum delivery, administered after the posttest assessment to reduce any potential bias, and lasted for approximately 15 minutes. Extensive paper-and-pencil notes and audio-recordings were used to capture student responses; audio-recordings were transcribed for pertinent information, and written notes were reviewed for accuracy against the audio-recordings.
The lead investigator and a trained research associate (male) reviewed three transcripts before coming to a consensus on the scoring rubric and achieving a chance-corrected (kappa) interrater reliability of .817 (Landis & Koch, 1977; Viera & Garrett, 2005). A total score was determined based on an assessment of each of the 11 Food Rules for each participant and by each Food Rule thereby measuring how well a particular participant understood the Food Rules overall and how well a particular Food Rule was understood. A participant-level score was generated by summing the participant’s individual 11 Food Rules scores (scored on a 1 to 3 scale: 1 = no comprehension, 2 = good comprehension, and 3 = high comprehension) divided by the total possible score that could be achieved (33 points). The coders grouped participants into three categories—low comprehension, moderate comprehension, and high comprehension—based on substantively driven cut-points ≤0.60 (≤20/33 points) = low; >0.60 to <0.80 (>20/33 points to 26/33 points) = moderate; >0.80 (>26/33 points) = high. These cut-points were determined based on standard cutpoints used to assess competence and learning in education.
Second, the coders generated a total score for each Food Rule across the cohort by summing each participant’s score for a particular Food Rule, divided by the total possible scores that could be reached. We imported qualitative notes into NVivo11 (QSR International, Melbourne, Australia, 2015) for analysis and reviewed them for emergent codes within each comprehension group and across the sample.
Semistructured Interview
The lead investigator created an interview script including six open-ended core questions, probes, follow-up questions, and member checks during the interview. Questions aimed to understand the target mediators and behavioral outcomes, for example, asking about “outcome expectations” (What are the benefits of eating fruits and vegetables?) or “attitudes” (What are your thoughts and feeling about eating phuds?)
A purposeful sample (two to four participants from each classroom) was selected to capture a range of participants observed to demonstrate varying degrees of understanding of the material. Thirty-minute interviews were held in a private room at each respective site and was led by the lead investigator (female) who has experience conducting interviews with adolescents. All interviews were audio-recorded.
Interviews were transcribed verbatim by an outside source and reviewed with their original audio recordings a minimum of two times to ensure accuracy. The lead investigator reviewed transcripts beginning with an open-coding process using line-by-line coding to identify themes, patterns of words, perceptions, and ideas, which were then classified into categories. An initial codebook of themes included a priori themes based on the target mediators from social cognitive theory and self-determination theory and emergent themes. Two independent coders met to review the coding scheme after reviewing two transcripts together, and the lead investigator and a trained research associate (male) met to come to a consensus on their codes after coding 3 of the 12 transcripts. Discrepancies between coding pairs were resolved through discussion to generate the final coding scheme. A percent agreement of 85% across coding pairs indicated acceptable levels of reliability. Each interview transcript was imported into the qualitative software NVivo 11 (QSR International, Melbourne, Australia, 2015), and themes were extracted from the imported text files and coded in NVivo.
Results
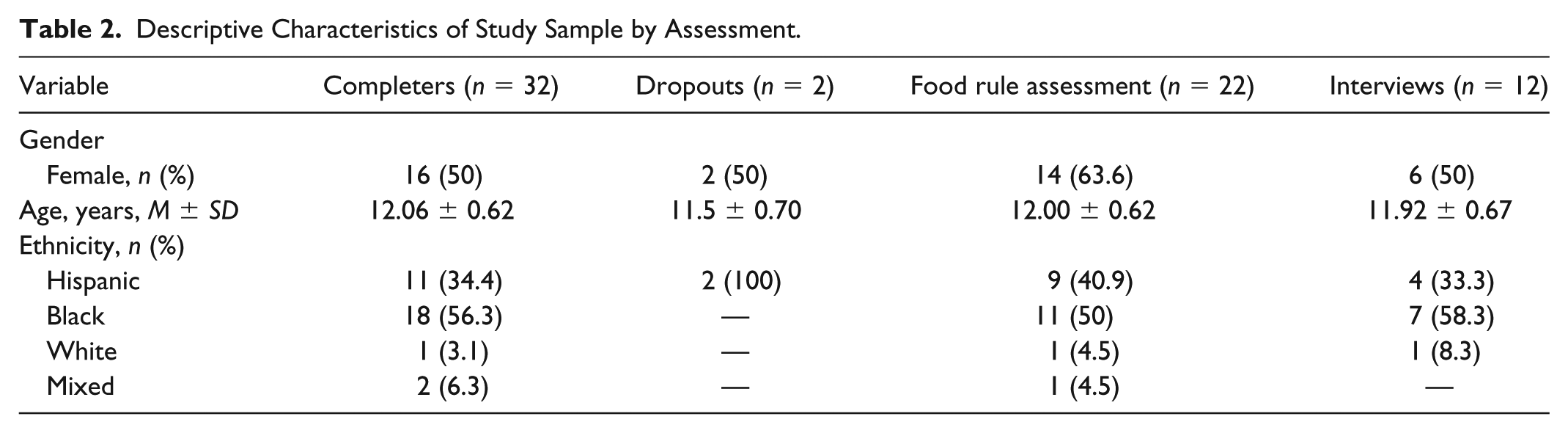
A total of 32 participants (n = 2 lost to attrition; 94% response rate) completed the surveys at both pretest and posttest. A subsample of this group was selected for the qualitative assessments. Demographic characteristics of participants grouped by assessment (pretest/posttest, Food Rule assessment, and interviews) are presented in Table 2. Overall, the mean age of participants was 12 years ± 0.62, 50% (n = 16) were female, and 56% were Black/African American. See Table 2 for demographic characteristics.
Descriptive Characteristics of Study Sample by Assessment.
Behavioral Outcomes and Mediators
There was a significant increase in mean frequency of FV intake at posttest compared with pretest (t = 3.359, p < .01)—an effect size that is considered to be large (d = 0.59). Small effect sizes (d = 0.34) were seen for mean intakes of HPF but change in score was not statistically significant (p = .06).
Statistically significant increases in outcome expectations and self-efficacy for FV intake occurred from pretest to posttest; all other mediators showed no statistically significant changes (Table 3).
Behavioral and Psychosocial Mediator Outcomes for Participants From Pretest to Posttest.
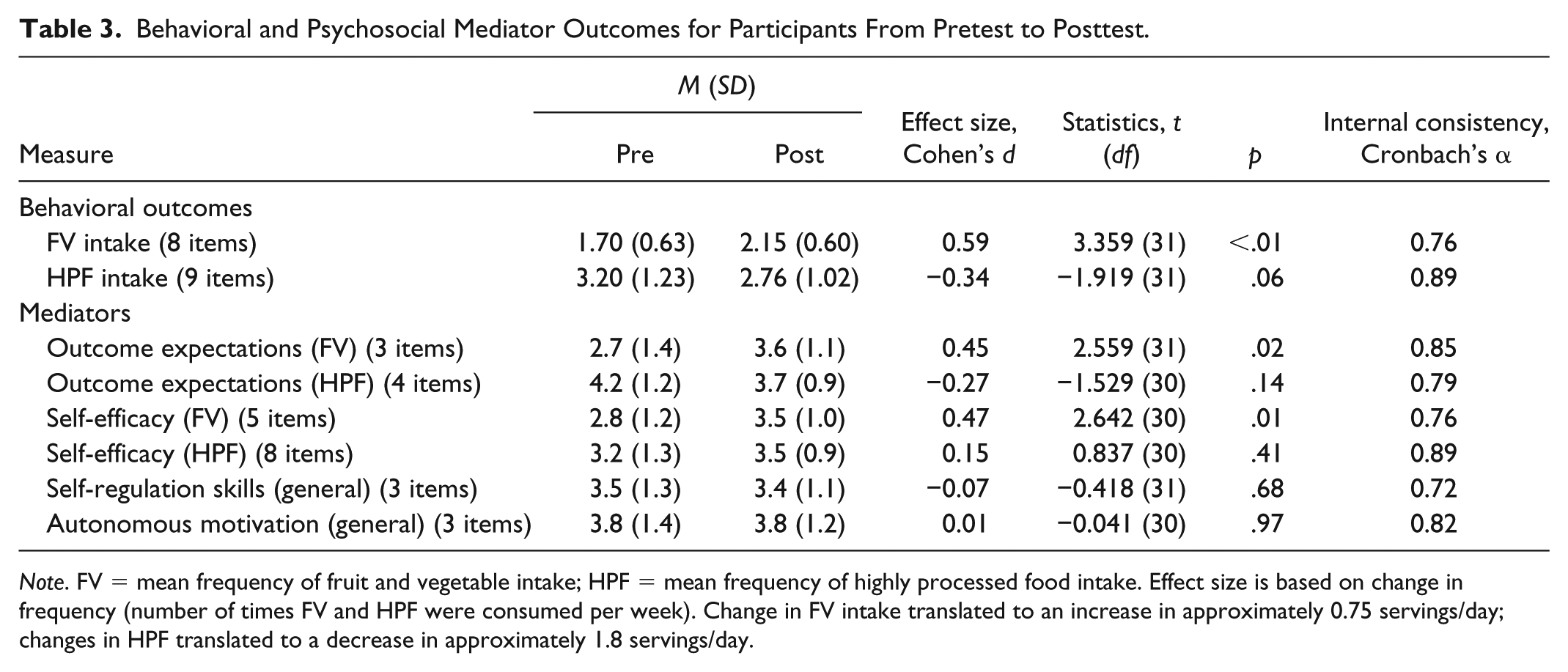
Note. FV = mean frequency of fruit and vegetable intake; HPF = mean frequency of highly processed food intake. Effect size is based on change in frequency (number of times FV and HPF were consumed per week). Change in FV intake translated to an increase in approximately 0.75 servings/day; changes in HPF translated to a decrease in approximately 1.8 servings/day.
Food-Rule Assessment
A total of 22 participants were included (64% female; mean age of 12 [± 0.62]; 40.9% Hispanic, 11% Black, and 9% White/Other); 66% of the participants were categorized into the high comprehension group (18% in the moderate and 18% in the low) based on their summative food-rule assessment scores. Qualitative subgroup analysis among the high comprehension groups revealed the demonstration of the application of self-regulation skills, which was not seen with any members of the low comprehension group; no notable themes emerged among the low comprehension group.
Analysis by Food Rule revealed some rules were better understood (e.g. “Break the rules once in a while,” “Make water your beverage of choice”) and others were less-well understood (e.g. “Avoid products that make health claims”; “If it came from a plant, eat it; if it was made in a plant, don’t”). Subgroup analysis revealed that youth demonstrated an application of self-regulation skills for the highest-ranking Food Rules (those most understood); no themes emerged across the lowest-ranking Food Rules.
Table 4 presents illustrative quotes from each Food Rules grouping. Figure 2 presents each Food Rule ranked from highest to lowest in scores.
Illustrative Quotes From Food Rules Assessment Demonstrating Self-Regulation Skills.
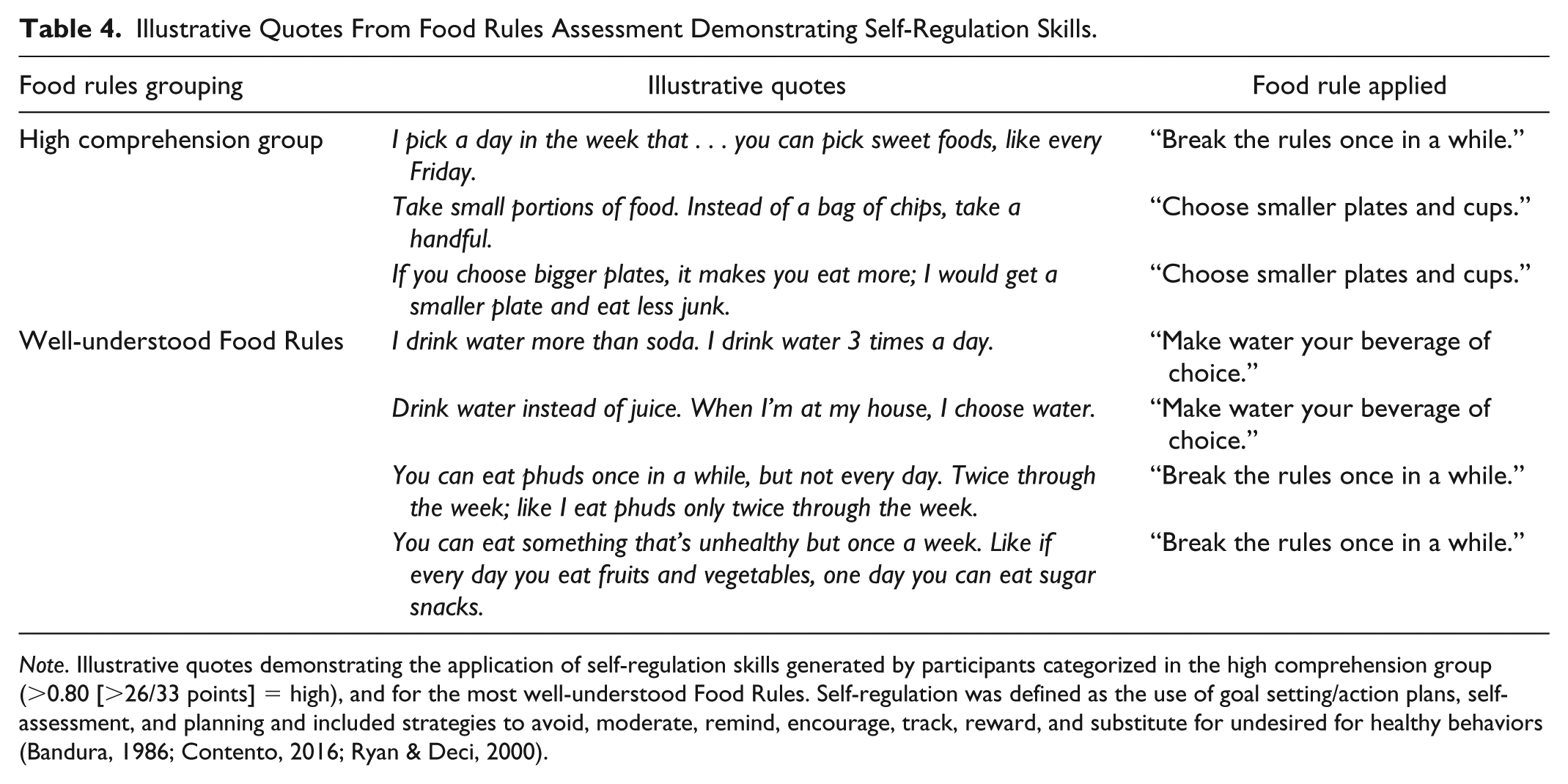
Note. Illustrative quotes demonstrating the application of self-regulation skills generated by participants categorized in the high comprehension group (>0.80 [>26/33 points] = high), and for the most well-understood Food Rules. Self-regulation was defined as the use of goal setting/action plans, self-assessment, and planning and included strategies to avoid, moderate, remind, encourage, track, reward, and substitute for undesired for healthy behaviors (Bandura, 1986; Contento, 2016; Ryan & Deci, 2000).
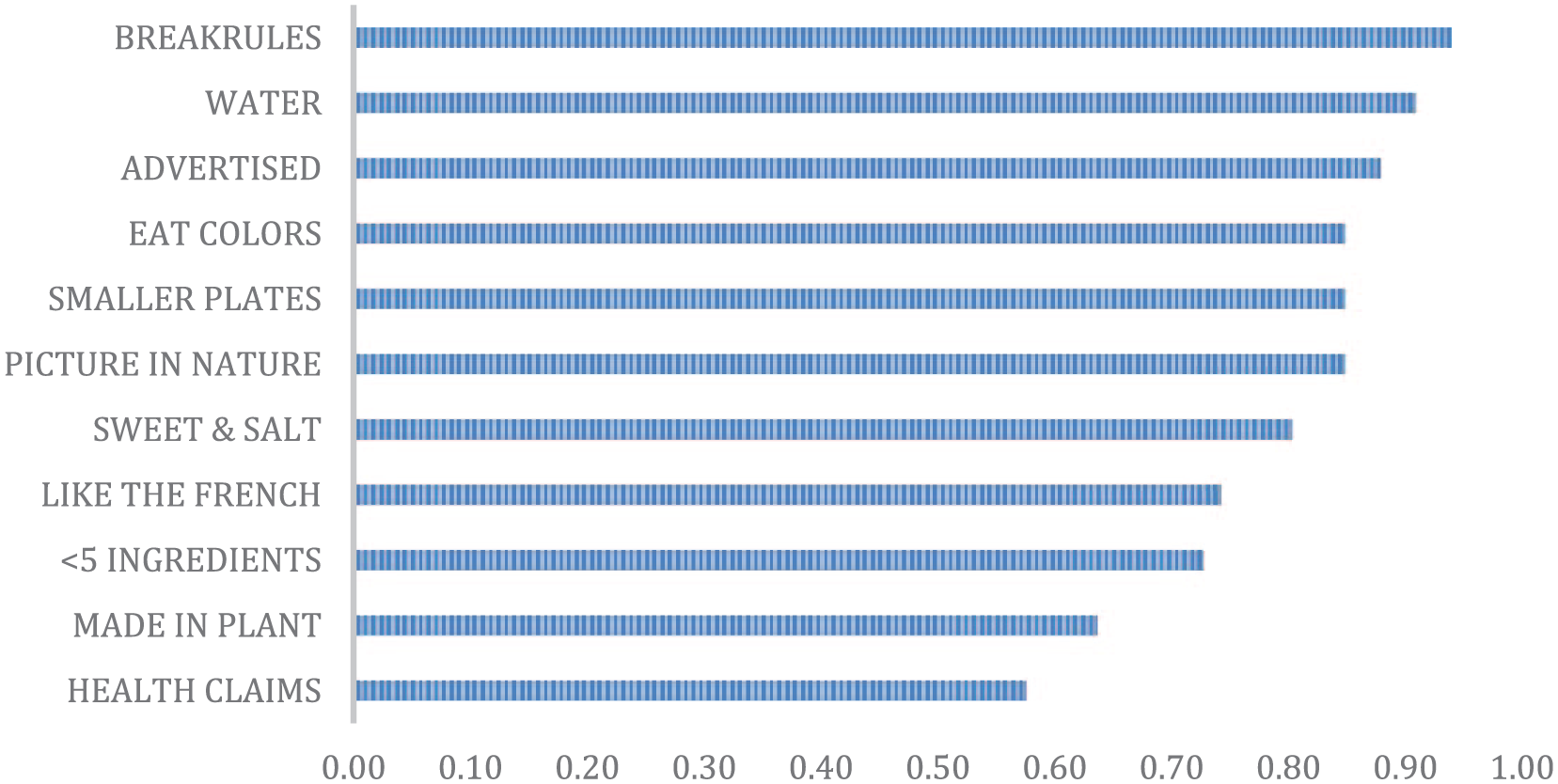
Distribution of scores for each Food Rule.
In-Depth Interviews
Table 5 provides themes and illustrative quotes from the semistructured interviews with the 12 participants (50% female; mean age 11.92 ± 0.67 years; 33% Hispanic, 58% Black, and 8.3% White/Other). Youth discussed supports for eating FV, including social support and modeling, the application of self-regulation skills to increase intake, and their expressed preferences for FV. They discussed the application of self-regulation skills, critical thinking skills, and strategies to decrease salience of HPF but revealed that the social and physical environment made it difficult to do so. Youth were also preoccupied with the negative physical outcome expectations of eating HPF, such as developing diabetes.
Themes and Illustrative Quotes From In-depth Interviews.
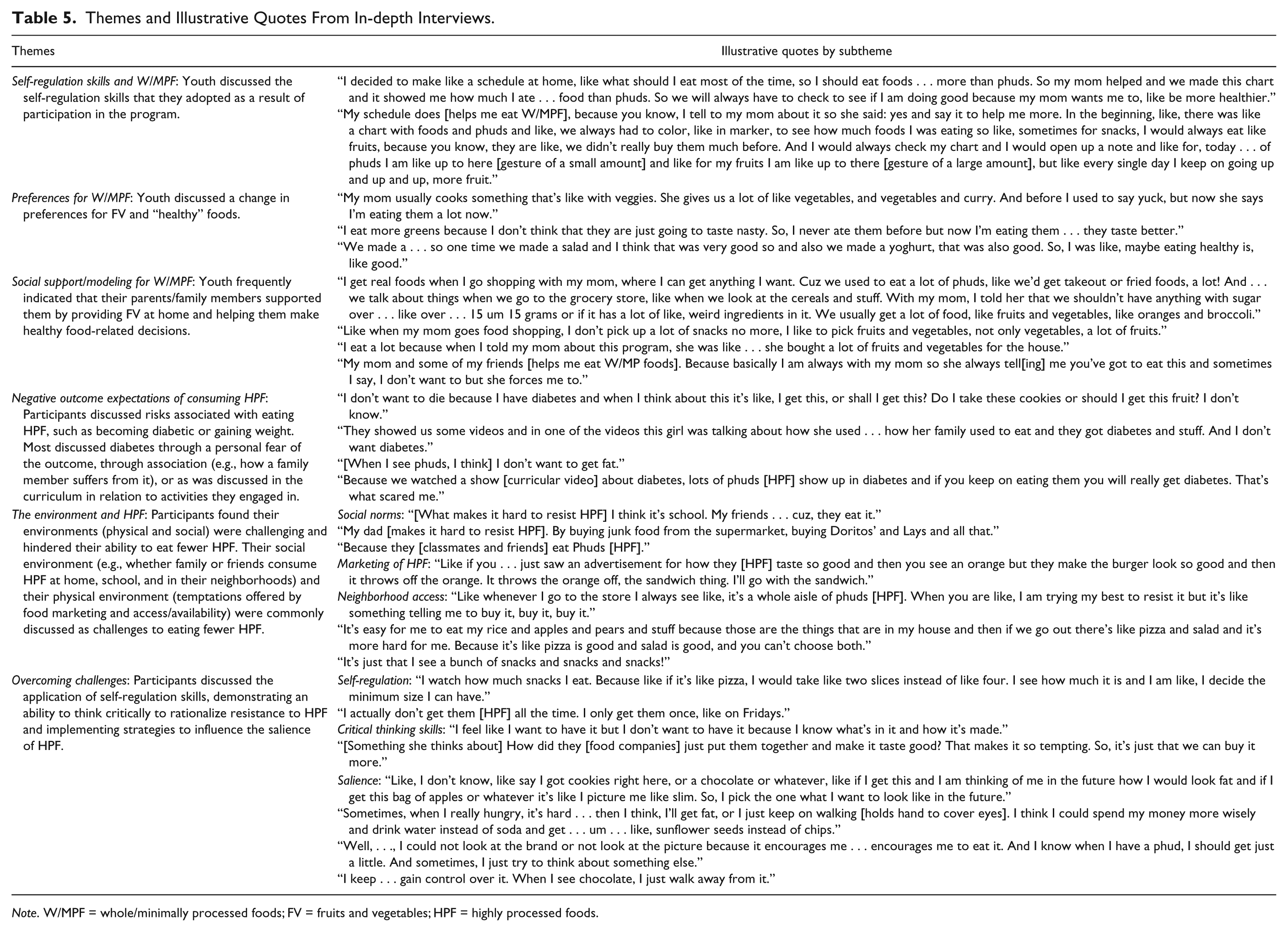
Note. W/MPF = whole/minimally processed foods; FV = fruits and vegetables; HPF = highly processed foods.
Discussion
The aim of the IDOF curriculum is to improve eating behaviors by increasing intake of W/MPF, operationalized as FV, and by decreasing intake of HPF. The current study is a pilot evaluation and part of a larger curriculum development project (Bhana, 2017). This study is not an efficacy trial, and a control group was purposefully not selected to allocate resources toward a richer understanding of the program’s outcomes through both qualitative and quantitative methods at this early phase of evaluation (Urban et al., 2014).
Behavioral Outcomes
Findings from this study demonstrate that youth participating in the IDOF curriculum increased their intake of FV with a large effect size. While a statistically significant change in HPF intake was not seen, there was a small effect size in the direction hypothesized. These findings are based on changes in frequency of consumption per week. Participants reportedly consumed FV only one to two times per week at baseline, which increased to approximately three to four times per week. Although these changes generated large effect sizes, the magnitude of change is low in comparison with dietary recommendations that encourage consumption of three to five servings per day (U.S. Department of Agriculture, 2012). The effect sizes obtained in this study have been demonstrated in comparable studies with children and adolescents in school-and-afterschool-based settings (Diep, Chen, Davies, Baranowski, & Baranowski, 2014; Thompson et al., 2009; Wilson et al., 2002) and with the same instrument in minority youth in New York City (Majumdar et al., 2013). Other research demonstrates that dietary behavioral additions may be easier to implement than dietary behavioral subtractions and may have also contributed to the findings revealed in this study (Verplanken & Faes, 1999).
Psychosocial Mediators and HPF
A ceiling effect was seen for negative outcome expectations associated with HPF demonstrating that participants had a high relative understanding of the connection between diet and disease at baseline. Negative outcome expectations are beliefs about the aversive physical outcomes that may result from eating HPF, for example, developing cardiovascular disease or diabetes. Most youth do not tend to be preoccupied with these often abstract and indirect future consequences. However, some studies support these findings, showing that minority youth in particular tend to be familiar with the negative outcomes associated with developing diabetes (Bandura, 2004; Mahajerin, Fras, Vanhecke, & Ledesma, 2008).
Findings from the in-depth interviews triangulate those collected quantitatively by demonstrating that many participants have personal experiences with diet-related diseases, having ill family members and observing them managing or failing to manage diabetes and other health complications.
Activities from the IDOF curriculum that focused on diabetes, and in particular trigger films (short educational clips used to elicit emotion) presenting minority community members struggling with inequality as it relates to health, were particularly salient to participants. Elements of this research suggest that messages surrounding diet-related diseases may resonate when community representation is an essential feature of the message. For instance, when messages include relatable reflections of race and class experiences. Other research supportive of these findings suggests that adolescents are more likely to personalize health-related messages if they believe that there are similarities between themselves and the program messaging (Cuijpers, 2002; Stephenson et al., 2004). Furthermore, other researchers (Necheles et al., 2007; Vangeepuram, Carmona, Arniella, Horowitz, & Burnet, 2015) have demonstrated that urban minority youth are viewing health differences through an equity lens and feel that large community-based advocacy initiatives and changes to their neighborhood “foodscapes” are necessary to support dietary changes.
Last, this research highlights some of the difficulties that participants express in making dietary changes. Although participants discussed the application of both critical thinking skills and self-regulation skills to help them decrease HPF intake, these may not be enough to compete with the realities of their physical and social environments—which are often inundated with highly processed foods.
Psychosocial Mediators and FV
Positive outcome expectations and self-efficacy significantly increased from pretest to posttest. Previous literature indicates that these mediators are typically associated (directly and indirectly) with changes in FV intake. For example, self-efficacy has been shown to be a strong behavioral predictor for FV intake in school-based health education with adolescents (Bruening, Kubik, Kenyon, Davey, & Story, 2010; McClain, Chappuis, Nguyen-Rodriguez, Yaroch, & Spruijt-Metz, 2009; Pearson, Ball, & Crawford, 2011).
General Psychosocial Mediators
Although the survey instrument applied in this study was tested for validity and reliability, there is a methodological concern and potential for measurement error associated with the three-item scale measuring self-regulation skills. Self-regulation skills are complex and may not have been captured adequately in the three-item scale used and may need a more robust scale then applied here.
While mean scores for self-regulation skills did not quantitatively shift from pretest to posttest, in-depth interviews and one-on-on assessments demonstrated that participants were applying self-regulation skills toward the target behaviors. For example, youth reported keeping records of their intake of FV versus HPF with the support of their parents, a strategy that has also been identified in the literature to enhance health behavior change (Cullen, Baranowski, & Smith, 2001). They applied reward structures to increase intake of FV (e.g., eating FV throughout the week for an unhealthy reward on Friday) while limiting HPF and self-management strategies, such as actions to decrease portion sizes.
Food Rules
Participants demonstrated self-regulation skills through the operationalization of many of the Food Rules, though some more so than others. This study reveals that more conceptually accessible Food Rules were commonly described as strategies to achieve the target behaviors. For example, “Break the rules once in a while,” “Make water your beverage of choice,” “Eat your colors,” and “Choose smaller plates and cups” were discussed in detail by participants across qualitative assessments. Whereas those that required first a necessary understanding of terms or did not provide easily actionable or concrete meaning, for example, “Avoid products that make health claims” and “If it came from a plant eat. If it was made in a plant, don’t” were not discussed and adopted by participants.
Social psychological research of self-regulation reveals that the adoption of a new goal can be influenced by the level of specificity (e.g., how concrete versus abstract) or their motivational orientation (e.g., approach—“do this actions”—versus avoidance—“don’t do this actions”), which may have influenced why some Food Rules more than others resonated with the participants (Mann, De Ridder, & Fujita, 2013). The thematic focus of a particular actionable Food Rule tied to curricular activities may have driven the common application of these self-regulation strategies and should be considered when developing other health education with youth.
These findings suggest that the IDOF curriculum may be most effective for promoting consumption of FV, rather than decreasing intake of highly processed foods. In addition, in this young age-group, short actionable food rules may support self-regulation and behavior change.
Limitations
These results are constrained by the small sample size and low statistical power, which may contribute to the lack of observed intervention effect for HPF and some of the psychosocial mediators. Also, by studying mean differences, regression to the mean biases may have been introduced. Behavior change is complex and at the time of posttest assessment (only 2 weeks following the completion of the curriculum) may not have actualized. Furthermore, this study is limited by self-reported dietary intake data collection and for which social desirability was not accounted for. However, almost all dietary behavior studies with groups, whether school-aged or adults, use self-reports. Here, comparisons are made pre to post intervention and between groups using the same method so that social desirability and validity issues are minimized. Still, the results need to be interpreted with caution but provide reasonable evidence for scaling up and testing this program within a larger sample.
Implication for Research and Practice
Despite the small sample size, the findings of this study suggest a possible mechanism for change in FV intake (as related to positive outcome expectations and self-efficacy) that could be explored further and more vigorously with a larger sample. It also draws attention to the social and environmental temptations that exist in the food environments of minority youth that should also be addressed in the development of health education programs in order to better support dietary change and to the importance of cultural representation in education materials. This study also contributes to a growing body of literature that demonstrates that minority youth may already be aware of the long-term chronic disease implications of poor dietary choices, as made salient by exposure to family members, friends, and members of their community with chronic diet-related diseases.
The use of thematically focused, conceptually accessible, and actionable “rules” or guidelines may be a promising approach to help students recall and enact self-regulation strategies and warrants further investigation in more controlled settings. While some of these findings are promising, future research is needed to determine whether a causal link can be drawn and whether or not dietary changes persist over a longer period of time.
Difficulties in the recruitment phase (related to a last-minute dropout and low enrollment) is a challenge, echoed by other researchers working in afterschool settings (Singh, Chinapaw, Brug, & Van Mechelen, 2009) and highlights the precarious nature of setting-based research. This challenge may also draw attention to either a low general interest in or capacity for these types of programs in the afterschool context or inclusion criteria for this study that were too strict. Although afterschool programs typically offer their programming as hourly, 1.5-hour, 2-hour programs, we were only able to accommodate those sites that offered 2-hour programming. The final IDOF curriculum was edited to ensure that it the lessons could be divided into either 20, 1-hour lessons, or 10, 2-hour lessons, and these logistical considerations may also be important for other health-focused afterschool curricula.
Footnotes
Acknowledgements
The authors gratefully acknowledge the contributions of Michael Swartz of Kikim Media and Mark Shelly of Sea Studios for their contributions to the original curriculum development on which this outcome evaluation is based.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.