
Abstract
School-based health activities that involve parents are more likely to be effective for child health and well-being than activities without a parent component. However, such school-based interventions tend to recruit the most motivated parents, and limited evidence exists surrounding the involvement of hard-to-reach parents with low socioeconomic status (SES). Mothers remain responsible for the majority of family care; therefore, this study investigated mothers with low SES to establish the reasons and barriers to their involvement in school-based health activities and to propose strategies to increase their involvement in those activities. Interviews were conducted with mothers with low SES, who were typically not involved in school-based health activities (n = 16). An inductive–deductive approach to hierarchical analysis revealed that there are several barriers resulting in mothers being less involved, particularly due to issues surrounding the schools’ Parent Councils and the exclusivity of school-based events. Efforts made by the school to promote health activities and involve parents in such activities were revealed, alongside recommendations to improve on these practices. The findings offer multiple ways in which future school-based health interventions can recruit and involve mothers with low SES.
Schools are one setting recommended by the World Health Organization as an ideal site to implement activities that encourage children to improve their health and well-being. Currently, the U.K. government is encouraging schools to address health issues (e.g., Public Health England, 2015), and there are a wide variety of activities that can occur: health-promoting teaching practices, classes on health and well-being topics, school projects or challenges, physical activity (PA) breaks during school time, health-related homework, and after-school clubs. Researchers have evaluated numerous school-based health interventions focusing on the key determinants of health including mental well-being, nutrition, sexual health, and PA (Lloyd et al., 2018; Mackenzie & Williams, 2018; Sani, Abraham, Denford, & Ball, 2016). However, findings from recent systematic reviews and meta-analyses have demonstrated equivocal results (Evans, Christian, Cleghorn, Greenwood, & Cade, 2012; Love, Adams, & Sluijs, 2018; Mackenzie & Williams, 2018). Indeed, school-based interventions can have positive effects on children’s health in the short-term (Gonzalez-Suarez, Worley, Grimmer-Somers, & Dones, 2009); however, there is a lack of evidence regarding the sustainability of such effects (Evans et al., 2012; Verjans-Janssen, van de Kolk, Van Kann, Kremers, & Gerards, 2018). Further research is needed to identify health initiatives and activities that schools can implement to create long-term health benefits.
Involving children’s proximal adults (e.g., parents) in school-based health activities could be a crucial way of improving the sustainability of positive outcomes, by encouraging positive health behaviors at school and at home. School-based health initiatives involving parents have revealed promising health outcomes (Niemeier, Hektner, & Enger, 2012), and parents may be key contributors to the success of interventions (Van Cauwenberghe et al., 2010; Verjans-Janssen et al., 2018). For example, research has indicated that changes to dietary and PA behaviors of parents can influence such behaviors in their children (Blaine, Kachurak, Davison, Klabunde, & Fisher, 2017; Yao & Rhodes, 2015). Furthermore, systematic reviews suggest that school-based health interventions involving parents are more effective than interventions without a parent component (Van Cauwenberghe et al., 2010). Thus, efforts to enhance parent involvement in such interventions are crucial and often proposed (Kipping, Jago, & Lawlor, 2012; Ruiter, Fransen, Molleman, Van der Velden, & Engels, 2015), but for whom these recommendations are for is unclear.
Many researchers struggle with the recruitment and retention of parents of low socioeconomic status (SES) (Robinson, Adair, Coffey, Harris, & Burnside, 2016), a limitation that is common within school-based health interventions (Norman, Nyberg, Elinder, & Berlin, 2016). Moreover, parents with low SES tend to be less involved with their child’s education than more affluent parents (Roksa & Potter, 2011) and experience multiple barriers to being involved (Hornby & Lafaele, 2011). As such, they are also less likely to engage in additional activities such as school-based health initiatives. While robust recommendations exist to engage parents of varying levels of SES in school activities (Reid, Eddy & Fetrow, 1999), these are provided in the context of children’s academic achievement and behavior. Whether the recommendations are appropriate for engaging within school-based health initiatives is unclear. Furthermore, it is unclear if the proposed recommendations to enhance parental involvement in school-based health interventions (e.g., Centers for Disease Control and Prevention, 2012) would be relevant for those who are typically uninvolved, with low SES. As it is important to ensure that health interventions are accessible and inclusive to all children, more information regarding the experiences and involvement of these hard-to-reach families with low SES in school-based health programs is needed.
Mothers remain responsible for the bulk of family care regardless of their employment status (Craig, 2006; Sayer & Gornick, 2012). Mothers play an essential role in their child’s development and are highly influential in their children’s health outcomes. For example, maternal care behaviors play an important role in children’s weight (Rodgers et al., 2013) and mental well-being (Stafford, Kuh, Gale, Mishra, & Richards, 2016). Therefore, it is important to understand the specific reasons that deter mothers with low SES from being involved in school-based health activities so that specific strategies and recommendations can be provided to encourage their future involvement. Therefore, this study aimed to interview mothers with low SES, who are not typically involved in school-based health activities, to establish the reasons and barriers to their involvement, and to gain insight into their perceptions of school health initiatives. Based on this information, we propose strategies that schools can use to increase parent involvement in future school-based health activities.
Method
A qualitative approach was employed whereby interviewees were selected based on questionnaire responses from a range of parents. From the questionnaire results, mothers who had low SES and were less involved in school activities were identified and then invited to be interviewed.
Recruitment
Institutional ethical approval was granted, and participants were recruited using a face-to-face recruitment method across five primary schools within a 12-mile radius of the university conducting the current research. Three schools were serving deprived communities, and two were in more affluent areas. Each school had a Parent Council that represents parents’ views and encourages parents to be actively involved in school life. Parents were recruited via awareness building strategies (e.g., flyers, pupil assembly visits that were attended by parents), followed by in-person recruitment at parents’ evenings to increase the likelihood of recruiting less-involved parents. Parents’ evenings are in-school events where teachers and parents discuss their child’s academic and behavioral performance. All parents are expected to attend, and the events normally have very high parental attendance rates (Two head teachers of recruited schools, personal communication, February 27, 2019). During these events, we set up a recruitment table, and the first and fourth authors directly approached all parents who walked past. While at the stall, parents received information about the study and completed consent forms, filled a family involvement questionnaire, provided demographic information, and were asked for their availability/times to participate in a telephone interview.
Eligibility Criteria and Instrumentation
Eligibility criteria for the interviews included (a) the mother of the child, (b) score below the median response of parents in the sample (below two) on the Family Involvement Questionnaire–Elementary (FIQ-E; Manz, Fantuzzo, & Power, 2004), and (c) low levels of SES based on an index of deprivation linked to their home address, which suggested that they resided within 20% of the most deprived areas in the country (Scottish Index of Multiple Deprivation [SIMD], 2016).
The FIQ-E (Manz et al., 2004) is a validated self-report scale measuring parent involvement in school activities using three subscales: school-based involvement, home-based involvement, and home–school communication. For the purposes of the current study, the 13 items from the school-based involvement subscale were used to select mothers who had lower than median levels of school-based involvement. The FIQ-E was deemed relevant for this study as it has been tested with lower-income urban caregivers of children attending primary school (Manz et al., 2004) and has demonstrated good factorial fit according to conventional criteria (Hu & Bentler, 1999) and excellent internal consistency (α = .91-84).
The SIMD identifies areas of deprivation across all of Scotland in a consistent way. SIMD ranks small areas from most deprived (ranked 1) to least deprived (ranked 6,976) that are then converted into a relative decile score between 1 and 10 (1 being the most deprived areas and 10 being the least deprived areas). Scores for each area are calculated based on objective criteria across six domains including the following: residents’ income, employment, housing, health education, skills and training, and geographic access to services and telecommunications (see SIMD, 2016, for more information). SIMD scores for all locations in Scotland were publicly available at the time of the research and were used to select participants with low SES based on the location of the participant’s home address scoring a decile score of 2 or below.
Participants
Parents (n = 132) completed an informed consent document, provided demographic information, and completed the FIQ-E. Of the 132 parents who completed these forms (113 female, 19 male), 120 agreed to be interviewed. Of the 120 parents, 24 eligible mothers were identified and 16 mothers were interviewed. All eligible mothers were contacted by telephone up to four times, five mothers were contacted but did not answer the telephone, and three rearranged the call for more convenient times but failed to answer subsequent calls. The mothers in our study (Mage ± SD = 35.88 ± 7.67 years) included single parents (n = 5) and coparents (n = 7); some mothers did not specify their family type (n = 4). Of these mothers, 11 were employed, four were unemployed, and one was a student. The highest educational qualifications obtained by mothers were lower secondary school qualification (n = 2), upper secondary school qualification (n = 2), college qualification (n = 3), a university qualification (n = 1), a degree qualification (n = 1), and some mothers did not report any qualifications (n = 7).
Interview Procedure
All interviews were conducted by the first author, a female researcher with 4 years of experience conducting qualitative inquiry including a Master of Research (MRes) in qualitative research. She was completing her PhD at the time of the interviews. The interviewer grew up in an area of deprivation (SIMD 2) near to the recruited schools; however, none of the participants had met the interviewer prior to study recruitment. Interviews were conducted via telephone using a semistructured interview guide with questions centered on healthy lifestyle promotion at school and parent involvement within health activities at school (see Supplemental Material for complete interview guide). All interviews were audio recorded and lasted on average 43.34 minutes (±12.20). Pilot interviews were conducted with a random selection of mothers recruited from the first school visit (n = 6 out of 11), and recordings were reviewed by both the first and the fifth authors upon which small amendments were made to the interview guide. Of these six pilot participants, only one met the inclusion criteria of being less involved, with low SES. This mother was interviewed again to cover the alterations made to the interview guide, and her pilot interview (22.25 minutes) and additional interview (16.21 minutes) were included in the analysis. No other pilot data was included in the final analysis. For anonymity purposes, all participants were assigned a participant number. The interviews were then transcribed verbatim by an independent transcription company. 1
Data Analysis
An inductive–deductive approach using hierarchal content analysis was taken to develop knowledge concerning our subject and the experience of the participants (Sparkes & Smith, 2014, p. 273). A social constructivist philosophy was adopted focusing on understanding how the mothers constructed their own reality of being involved in school activities (Patton, 2002, p. 97). The first author undertook the qualitative analysis by first reading the transcripts while listening to the interviews to become familiar with the data. Using NVivo 11, she then independently examined the transcripts, and each comment or meaningful unit was identified and labelled inductively as nodes. Then similar nodes were grouped together according to both: the key research questions and emergent ideas. We sought to establish themes with internal homogeneity (where all nodes in one theme share meaningful characteristics) and external heterogeneity (the differences between nodes in different themes are clear) and grouped themes into higher order themes. Ensuring rigor and transparency in analysis is a vital component to assess the quality of research (Gale, Heath, Cameron, Rashid, & Redwood, 2013). Thus, to ensure quality in the analysis, the second, third, and fifth authors who were not present during data collection independently reviewed the data at several stages of the analysis, and multiple iterative discussions between all the authors took place to ensure the representativeness of themes. An opportunity for member checking was provided by disseminating an overview of themes to all parents via email. One mother replied via email seeking to differentiate her views from those of other mothers. She was reassured that the themes represented the views of all mothers, rather than solely her own views.
Results
Four overall themes emerged from the data: (a) barriers to being involved in health activities at school, (b) active ingredients to being involved in health activities at school, (c) school efforts, and (d) recommendations to the schools (see Figure 1).
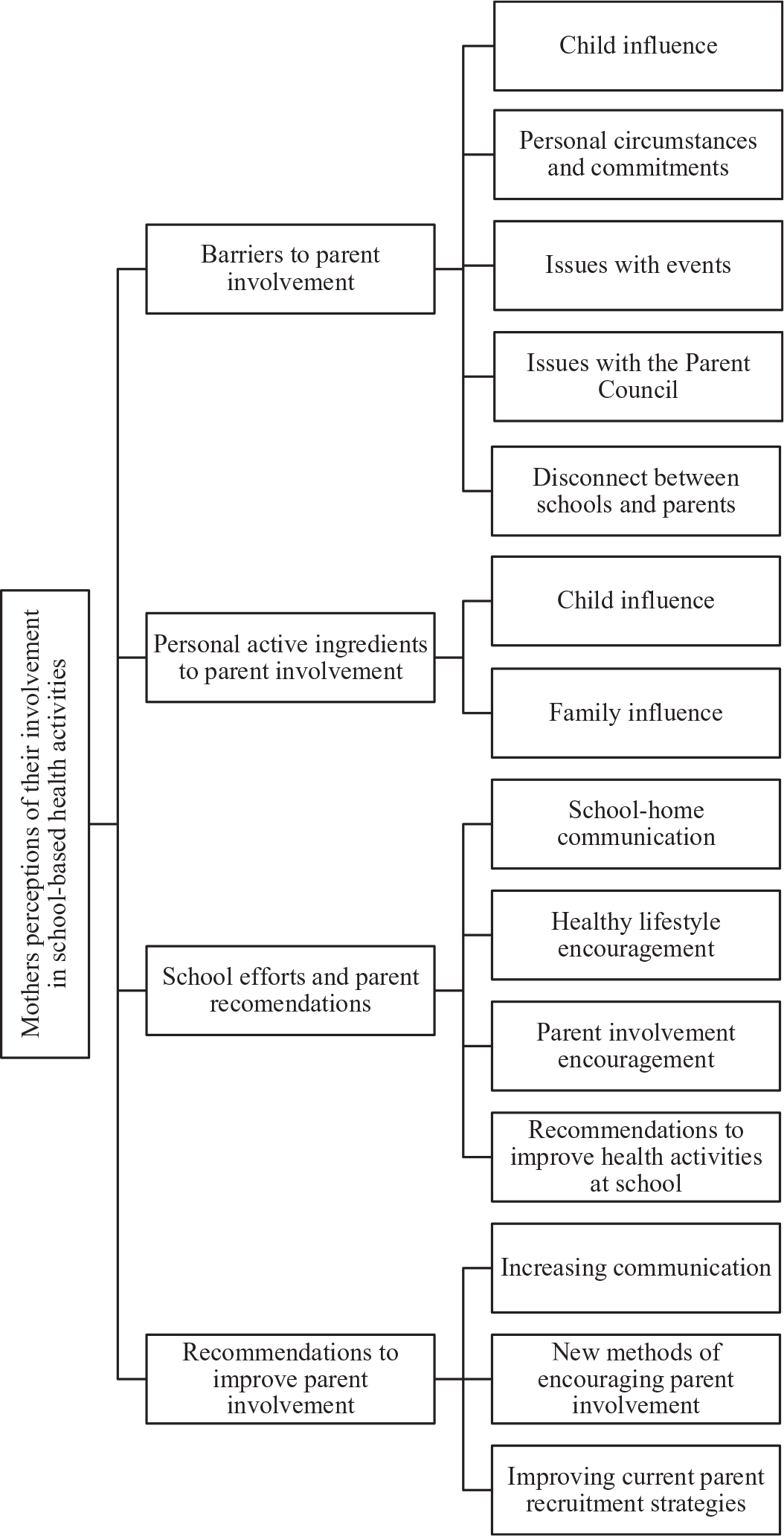
Mothers’ perceptions of their involvement in school-based health activities, including the overall and second-order themes that emerged from the analysis process.
Barriers to Being Involved in Health Activities at School
The barriers that deter mothers from being involved in school-based health activities were grouped into second-order themes: personal circumstances, child influence, issues with events, issues with the Parent Council, and a disconnect between the school and the parents (see Table 1).
Barriers to Mothers’ Involvement in Health Education Activities at School.
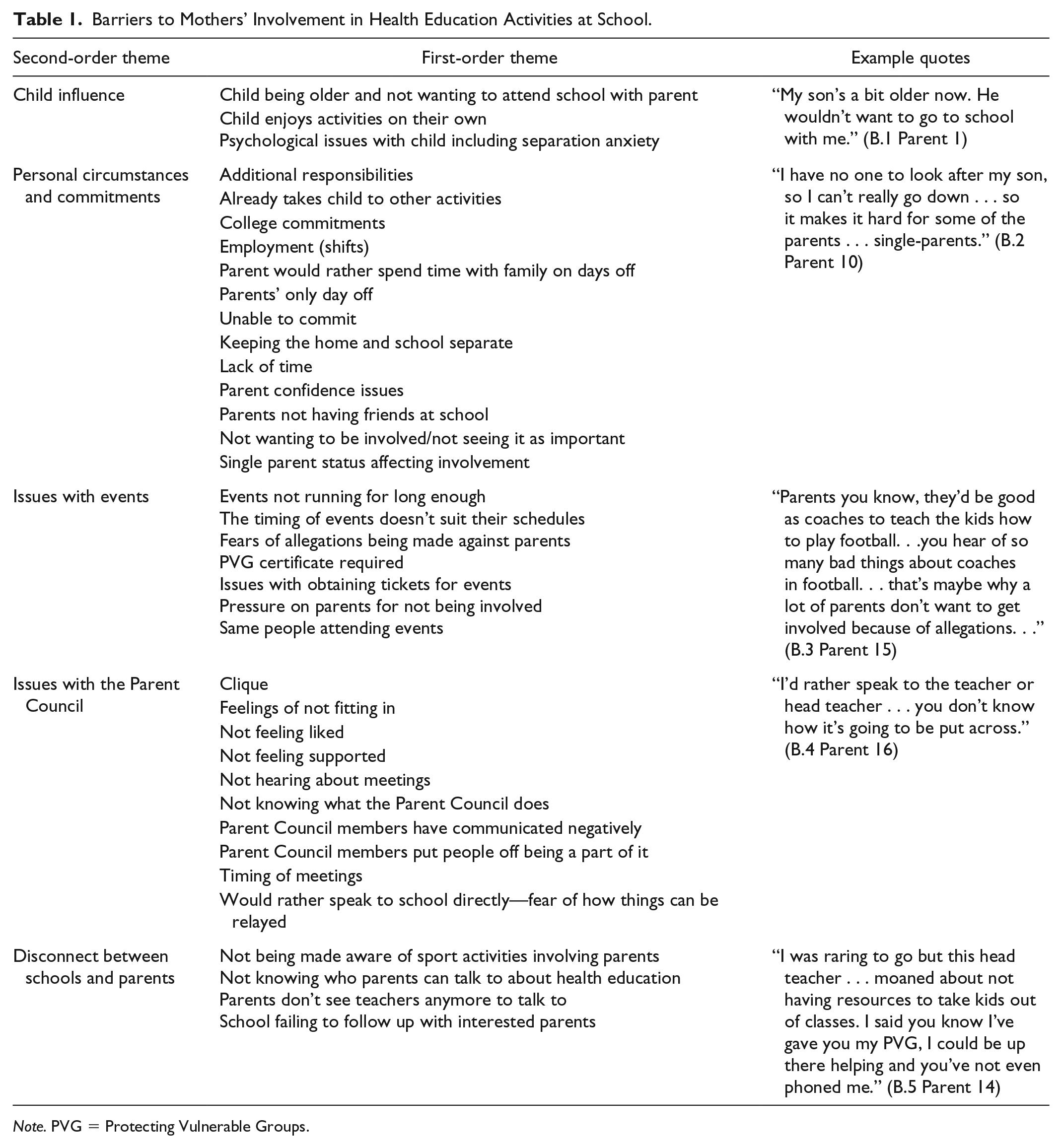
Note. PVG = Protecting Vulnerable Groups.
The mothers discussed personal circumstances as barriers to their involvement, including having additional commitments such as attending college, other child-related activities (e.g., sports clubs), and employment (e.g., shift work). Being a single parent was a barrier to involvement for some mothers, particularly as it often wasn’t possible to bring their other children to the school events (quote B.2 Parent 10). Also, a lack of time was cited as an issue, and some mothers discussed that they would rather not spend the free time they did have being involved in school activities. Some participants also had a general disinterest in being involved in such activities and did not view their involvement as important. As well as personal circumstances, it was suggested that the child and their preferences could also deter involvement, particularly if the child was older or experienced issues such as anxiety (quote B.1 Parent 1).
There were several barriers that deterred mothers from being involved in specific school events such as practical issues (e.g., obtaining tickets) and issues related to the safety and the social aspects of the events. Most notably, mothers consistently discussed the timing of events, which acted as a barrier to their involvement in school-based health activities. For example, mothers were unable to attend events being held during school hours due to employment. Mothers also discussed the timing of events as being difficult, particularly if weekly sessions take place on the same day and they have unpredictable and inflexible work schedules.
To ensure the safety of children in Scotland, a Protecting Vulnerable Groups (PVG) certificate is required for adults to work with children, which was reported as a barrier to volunteering at school as some mothers did not have a PVG certificate or know how to obtain one. Furthermore, some mothers indicated that due to recent reports of abuse by those working within sport, a fear of allegations could deter some parents from being involved as volunteers (quote B.3 Parent 15).
With reference to the social aspects of school-based health activities, some mothers lacked confidence to be involved and not having other parents as friends could deter some parents. Furthermore, mothers suggested that it was often the same parents attending events, who were most likely to be affiliated with the Parent Council. The Parent Council is a group of volunteer parents who meet regularly to work with the school in order to represent the views of parents/carers and encourage links between the school and the parents. The Parent Council groups are often pivotal to organizing health-related activities in schools (e.g., sport days, fund-raising events for playground equipment and sports clothes) and were repeatedly described as “cliques” with mothers feeling neither liked nor supported by the Parent Council. Furthermore, mothers not being made aware of Parent Council meetings, not knowing what the Parent Council does, and the timing of council meetings were highlighted as barriers to their involvement. Indeed, some mothers suggested that they would rather speak and provide feedback to teachers directly in fear of how information could be relayed by members of the Parent Council (quote B.4 Parent 16).
More generally, mothers also suggested a degree of disconnect between the school and the parents, as they did not know who to talk to about health-related activities, they were not always made aware of activities taking place, and, in some situations, teachers failed to follow up with parents who were interested in being involved (quote B.5 Parent 14). In general, some mothers did not feel that they had a partnership with the staff, and it was difficult to access teachers and discuss health-related activities with them.
Personal Active Ingredients to Being Involved in Health Activities at School
The data regarding personal aspects that encourage parents to be involved in health activities related to child and family influence are shown in Table 2. Both the mothers’ and their child’s interest in activities and perceiving benefits to their child would encourage these mothers’ participation in health activities (quote A.I.1 Parent 11). Specifically, the opportunity to create life-long healthy habits, set a good example to their children, provide enjoyment for their child, and improve their relationship with their child via shared activities all encouraged parents to be involved (quote A.I.2 Parent 2). Extended family involvement (e.g., the possibility of grandparents attending events) was also highlighted as a method of facilitating more home-school connection and family involvement in school-based health activities (quote A.I.3 Parent 1).
Personal Active Ingredients to Mother’s Involvement in Health Education Activities at School.

School Efforts
The mothers recognized the efforts made by the school regarding healthy lifestyles, parental involvement, and communication with home regarding health activities (see Table 3). Mothers identified numerous health activities run by the school to encourage healthy lifestyles including PA events (e.g., walk to school, sports day, afterschool clubs, and the daily mile) and dietary-related activities (e.g., cooking classes, promotion of healthy snacks, and garden club). Most of such activities were free for the children, and overall, the mothers held positive views of the schools’ encouragement of healthy lifestyles. In some schools, the mothers thought that rewards systems where children received class points for healthy behaviors encouraged positive behavior (quote S.E.5 Parent 1). While these activities were geared toward the children’s health behaviors, many activities involved or depended on parents including assisting their children to take healthy snacks to school and walking younger children to school. Mothers also provided recommendations to improve the promotion of health activities at school including hosting a healthy buffet and the possibility of providing a variety of different foods to promote healthy eating in children (quote S.E.8 Parent 8). Mothers also recommended increasing extracurricular clubs and activities to promote PA time.
School Efforts to Encourage Parental Involvement in Health Education Activities at School.
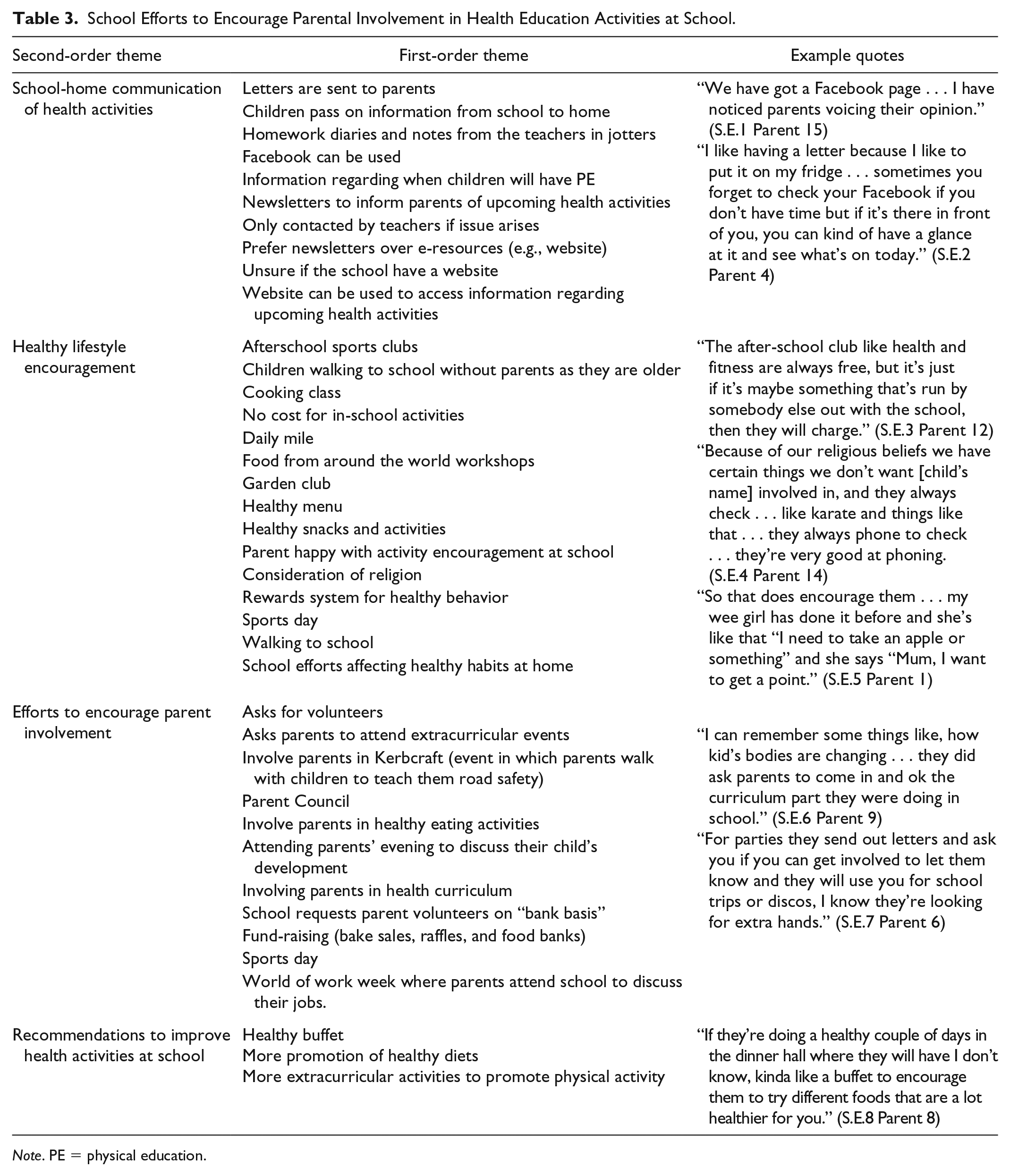
Note. PE = physical education.
The participants discussed school efforts to encourage parents to be involved in health activities. Parents were invited to discuss the health curriculum and encouraged to take part in healthy eating activities with their child. Some schools asked for volunteers on a “bank basis” where they would request the participation of interested parents when required. These extracurricular events included Parent Council events, parents’ night, and sports day. One school’s consideration of religion toward diet and sporting activities was positively recognized (quote S.E.4 Parent 14), as those with specific religious beliefs reported that they were often contacted to check if diet and sport-related activities were appropriate for their children.
The mothers discussed the ways in which the schools communicated with regard to school-based health activities (e.g., letters and newsletters, school websites, the school Facebook page, via notes in the children’s homework diaries, information days; quote S.E.1 Parent 15). The mothers preferred printed information (e.g., newsletters) over e-resources (e.g., websites), as they were less likely to forget about upcoming events if they were on display (e.g., on the fridge). Some mothers did not know whether their child’s school had a website (quote S.E.2 Parent 4) and suggested that they mostly received information via their child rather than the schools.
Recommendations to Improve Parent Involvement in School-Based Health Activities
A host of recommendations were provided including increasing communication, developing new methods of encouraging parent involvement, improving current parent recruitment strategies, and improving the promotion of health activities at school (see Table 4).
Recommendations to Improve Parent Involvement in School-Based Health Activities.

Note. PE = physical education.
The need for more effective communication was consistently emphasized. Most notably, mothers considered an increase of information both with relation to parent involvement and health activities at school to be of the utmost importance. Mothers recommended increasing the inclusivity of Parent Council meetings as a way of increasing information (quote R.1 Parent 4).
Encouraging parent involvement was also recommended by the participants, and recommendations were offered including hosting coffee mornings, text message systems, parent-child joint activities, school trips, and home-based activities. Mothers also suggested that parents and teachers could work together to design a parent involvement program (quote R.2 Parent 11). The ways in which parents themselves could encourage parent involvement in school-based health activities were highlighted including electing a parent champion (quote R.3 Parent 16) and encouraging more communication between parents. In terms of improving on current parent recruitment strategies, mothers recommended providing parents with more information of meetings beforehand, as well as providing sufficient notice of these meetings and school events. Moreover, participants suggested that providing parents with various event times to accommodate all parents would increase recruitment (quote R.4 Parent 12).
Discussion
These findings revealed that the mothers in our sample face multiple barriers to their involvement in school-based health activities including single parent status, unpredictable working patterns, a lack of confidence to provide feedback to the school, and not feeling liked or supported by parents within the Parent Council. Previous research suggests that conflicting commitments and a lack of time are barriers for all parents’ involvement in school activities (Murray et al., 2014); however, the unpredictability of these mothers’ schedules alongside their fears and lack of confidence seem to be related to their specific experiences. Therefore, it could be suggested that the barriers these mothers face are exacerbated by the effects of their low SES. Some mothers did not want to be involved and viewed the school and home as separate environments, whereas others wanted to be involved but felt that the school did not encourage their involvement. While mothers with low SES face some similar barriers to parents who are more affluent (Murray et al., 2014), the current results suggest that some mothers with low SES have lower motivation and experience more barriers to being involved in school-based health activities.
The current findings accord with previous work regarding a lack of confidence among mothers with low SES, who can be overlooked by schools (Lavee & Benjamin, 2015). Indeed, low self-efficacy levels of mothers with low SES have previously been highlighted as a barrier to involvement, as parents with limited educational backgrounds frequently lack the confidence to interact with teachers (Kim, 2009). They may also be vilified or blamed for not conforming to standards set by more affluent parents (Gillies, 2006). Requests for parent involvement have often been left unscrutinized in relation to the advantage provided to parents of specific social groups and the demands it imposes on socially vulnerable parents (Theodorou, 2007). Thus, schools should review whether their standard way of working with parents favors more affluent parents and whether changes can be made to increase the inclusivity of parent-related activities.
Self-determination theory (SDT; Ryan & Deci, 2000a) could offer a theoretical explanation regarding the low levels of involvement of the mothers within our study, as these participants did not feel competent in the school environment, lacked relationships with other parents and staff, and did not know how to autonomously feedback to the school. For example, Parent 13 within our study expressed how lack of friendships within the school meant that she did not get involved in school activities. “Well there’s not many friends I have in that school . . . like, mums. I just pick up the kids and bring them back.” SDT would suggest that such negative experiences may have affected on mothers’ need satisfaction and their subsequent motivation to be involved (Ryan & Deci, 2000b). Indeed, a study that examined parents’ motivation to be involved in schools suggested that higher autonomous motivation in mothers was associated with higher levels of involvement (Grolnick, 2015). Therefore, SDT could provide a theoretical framework that supports the needs of hard-to-reach parents in future school-based health interventions.
Social identity theory (Tajfel & Turner, 1979) may also explain the influence of social groups on these mothers. Social identity theory suggests that a person’s self-concept derives from the groups to which the individual belongs. An individual will compare his or her own in-group against other out-groups, tending to view members of competing groups negatively in order to increase their own self-esteem. If a Parent Council has a strong group identity as an exclusive “clique,” they would be likely to view less involved parents negatively and may discriminate against them. Parent 4 raised this issue: It always seems to be the same people that are attending. It’s always the people that’s close to the school, so then you don’t want to attend . . . There are a lot of people that are really cliquey . . . they’re in the Parents’ Council and they get everything first.
Parent 2 felt similarly regarding this issue: “I don’t think they like me . . . The Parent Council has needed new members and I did consider it but I didn’t go . . . I know half of the mums wouldn’t vote me in.” This could explain why some mothers felt excluded and disliked by the Parent Council, which acted as a barrier to their involvement in school-based health activities. Nonetheless, alongside barriers to involvement we also identified positive influences that encouraged the mothers to be involved in health activities.
Personal active ingredients were discussed, including the aid of extended family as a way of remaining involved in school activities, which has been highlighted as a facilitating factor in previous research (Bol & Kalmijn, 2016). The influence of their child was also noted as an active ingredient to involvement via perceiving potential benefits to their child’s health, and opportunities to improve parent-child relationships. The benefits of parent involvement for children have been recognized in previous research (Hesketh, Waters, Green, Salmon, & Williams, 2005); however, the current data suggest that some mothers with low SES seem particularly unaware of the positive influence they could have by being involved in school activities with their child. Therefore, when schools are running family-based health activities, it would be prudent to emphasize the relevant benefits parent participation could have for pupils. Indeed, providing parents with good reasons as to why they should participate or attend parental opportunities has been found to be a successful strategy for building bridges between low-income parents and schools (Jennings, 1992; Murray et al., 2014).
The schools’ efforts regarding health activities was appreciated by the participants; however, some aspects of communication could have been improved, as some mothers were unaware that the school had a website and some felt that the messages were mainly delivered via their child. Indeed, school websites are frequently cited as a useful means of parent-school communication (Piper, 2012). Mothers also felt that the school could improve on their communication regarding parent involvement, as some mothers stated that the school had failed to follow up when they expressed interest in being involved.
As a result of this research, there are a series of suggestions that could be used by schools, policy makers, and researchers seeking the involvement of mothers with low SES in school-based health activities. Parents suggested that joint parent-child activities, school trips, and home-based activities would be positive ways to increase their involvement in health activities. Our findings also highlight that using a variety of methods to communicate with parents regarding health activities could encourage less engaged parents to get involved (e.g., discussion groups, newsletters, homework diaries, social media, text messages). Schools should also consider the timing of events, the notice they provide to parents, and encourage other family members’ participation to improve the home-school connection for families and parents with complex and conflicting demands. Mothers in the current study also recommended parents and teachers planning health activities together, having a parent champion for health activities, and parents inputting in the promotion of sports clubs. Indeed, the aforementioned recommendations echo previous research relating to parental involvement in health projects more broadly (Clarke et al., 2015; Patino-Fernandez, Hernandez, Villa, & Delamater, 2013; Raftery, Grolnick, & Flamm, 2012) and align with best practice recommendations to involve end users in the design of school-based health initiatives (Craig et al., 2008; Patino-Fernandez et al., 2013). There are, however, some recommendations that reflect findings that seem to be more specific to parents with low SES who are already less involved. In particular, the data suggest that schools could focus more on nurturing these parents’ beliefs that their involvement in school-based health activities could make a worthwhile contribution to their own and their child’s well-being. Furthermore, the Parent Councils that are frequently responsible for organizing events at the schools were discussed as a barrier to parent involvement. Mothers described feeling excluded from the Parent Council, and as such, schools should make efforts to promote inclusivity and representation of families with low SES within Parent Councils. Furthermore, it would prudent to ensure that such committees do not become an overly powerful group of parents who run events without considering input from teachers and a diverse range of parents. Such methods are likely to increase parents’ feelings of autonomy, competence, and relatedness, thus increasing their motivation to be involved (Grolnick, 2015). However, while parents suggested valuable methods to increase parent involvement, the cost implications of such activities would need to be considered to ensure that parents with low SES would not be excluded.
There are several strengths within the current study. Due to our face-to-face recruitment methods, we interviewed 16 mothers with low SES, who were not usually involved in school-based activities. As such, mothers who were unlikely to participate in research or school-based activities were recruited, and their views were captured. However, this research is subject to limitations. Interviews were conducted in one region of the United Kingdom; therefore, the themes identified may not be reflective of mothers’ views in other locations, and father’s views are not represented. Indeed, the majority of research on parent involvement in school-based health activities focuses on mothers as the parent most likely to be the primary caregiver (Hill & Taylor, 2004). Future research could explore the involvement of parents in school-based health activities on a family level, taking into consideration the perspectives of fathers, siblings, and extended family.
Despite decades of research, there is still a lack of interventions that effectively affect children’s health behaviors (e.g., Love et al., 2018). Indeed, including caregivers and home-based activities within the interventions is often cited as a method of improving the impact of school-based health activities (Bleich et al., 2018). However, school-based health interventions are often only attended by the most affluent and motivated parents (Clarke et al., 2015; Ruiter et al., 2015). Such interventions should aim to address health inequalities by recruiting and including parents with low SES who are typically uninvolved. As such, these results offer valuable insight to schools, practitioners, and researchers to encourage uninvolved parents to participate in school-based health activities.
Supplemental Material
HEB871329_suppl_mat – Supplemental material for An Insight Into the Involvement of Mothers of Low Socioeconomic Status in Scottish Primary School Health Education Activities
Supplemental material, HEB871329_suppl_mat for An Insight Into the Involvement of Mothers of Low Socioeconomic Status in Scottish Primary School Health Education Activities by Samantha Donnelly, Duncan S. Buchan, Ann-Marie Gibson, Gillian Mclellan and Rosie Arthur in Health Education & Behavior
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.