
Abstract
Settings-based approaches have become an increasing health promotion focus since the World Health Organization’s 1986 Ottawa Charter. While schools, cities, and prisons have implemented this approach, its development within sports environments is recent. Sports are a popular leisure-time activity, requiring validated tools to measure health promotion activity. This study’s aim was to develop a measurement tool based on international consensus that measures perceptions of health promotion within sports clubs. It is grounded in the settings-based approach and builds on theory from previous works expanding their context and knowledge. An online, three-round international Delphi study was conducted, inviting experts in sports and health fields to participate in designing the tool. Round 1 created a collaborative list of items; Round 2 validated items based on relevance, importance, and feasibility; and the final round classified items into one determinant category—social, cultural, environmental, or economic. Panelists (69 experts) from 13 countries participated, creating a final list of 62 items at 3 organizational levels; the sports club level included 23 items, the officials level retained 20 items, and the coaching level contained 19 items. This study provides several innovations: (1) applying the settings-based approach to health promotion within sports clubs, (2) defining each club level (sports club, official, coaching) and determinants (social, cultural, environmental, economic) within 3-levels, (3) creating a tool that measures perceptions of health-promotion activities per level and determinant, and (4) obtaining expert consensus on included items. These advancements allow further research on promoting health within sports clubs.
Keywords
According to the World Health Organization, health promotion is “the process of enabling people to increase control over and to improve their health.” To develop this, the Ottawa Charter (World Health Organization, 1986) pointed out the importance of a settings-based approach in health promotion based on the idea that change is not solely focused on individuals and their health problems, but that changes are generated in organizations and communities to ensure the development of environments that support population-wide changes in health-related behavior (Whitelaw et al., 2001) . The objective is to go beyond a behaviorally focused approach and move toward a socioecological approach, by working on cultural, social, economic, and environmental determinants of health (Glanz & Bishop, 2010). Multiple settings, such as schools (Rees et al., 2006), hospitals (Johnson & Baum, 2001), workplaces (Noblet, 2003), and cities (de Leeuw, 2009), have used this framework when implementing health promotion programs. While these settings are established, the application of the socioecological approach has been limited regarding leisure settings such as sports (Fredriksson, Geidne, & Eriksson, 2018).
According to the Eurobarometer, in Europe alone, more than 33% of the population participates in sports (European Commission, 2017). Thus, studies have supported the recognition of sports club as health-promoting settings (Kokko, 2014). Grounded in the socioecological approach, the health-promoting sport club includes four determinants of health (cultural, social, environmental, and economic; Golden & Earp, 2012) applied at three club levels: macro level (overall policies and orientations of club activities), meso level (activities of club officials), and the micro level (coaches’ activities in guiding, altering, or supporting actions of club members; Kokko, 2014). The application of the settings-based model into sports clubs has received less attention thus, evaluation tools to measure health promotion in sports clubs are rare and primarily focused on interviews and self-reported questionnaires (Casey, Harvey, Eime, & Payne, 2011). A recent literature review on health promotion interventions in sports clubs found that most studies used nonvalidated, qualitative measurement tools (Geidne et al., 2019). Furthermore, those that were validated are culturally specific (Casey et al., 2011; Kokko, Kannas, & Villberg, 2009). To our knowledge, two national Delphi studies were conducted, one identified indicators of health-promoting sports clubs and one aimed at policies, practices, and capacity. One international Delphi study focused on how health promotion fits in with social responsibilities of sports clubs was also completed.
The first study, based on the Ottawa Charter and the settings-based approach, aimed to identify standards for health-promoting sports clubs (Kokko, Kannas, & Villberg, 2006). Consensus on 22 health promotion standards was reached by 27 Finnish experts. Standards were classified into four categories, policy, ideology, practice, and environment, and tested among a Finnish sample of clubs, officials, and coaches, which resulted in the Health Promoting Sports Club Index (HPSC; Kokko et al., 2009). This measurement tool has been used at the official, coach, and youth sports participant level in Finland (Kokko, Kannas, Villberg, & Ormshaw, 2011; Kokko, Villberg, & Kannas, 2015) and the official level in Belgium (Meganck, Scheerder, Thibaut, & Seghers, 2015). A modified version was tested at the club (macro) level in Ireland (Lane, Murphy, Donohoe, & Regan, 2017), and the coaches and youth sports participant level in France (Van Hoye, Heuzé, Meganck, Seghers, & Sarrazin, 2018; Van Hoye, Sarrazin, Heuzé, & Kokko, 2015).
The second national Delphi study was conducted in Australia to determine aspects necessary for sports clubs to develop healthy sporting environments for children (Kelly et al., 2014). This study invited 46 experts to rate standards relating to 7 health-promoting themes: healthy eating, sponsorship and fundraising, injury prevention, alcohol management, smoke-free environment, sun protection, and social inclusion Key health promotion areas were added from the Finnish Delphi study including smoking and tobacco use, healthy eating, and social inclusion (Kokko et al., 2006). These standards have yet to be directly used or tested among sports clubs.
The third national Delphi study captured sport-related policies, practices, and organizational capacity across events and sports clubs, by questioning state sport organizations (Casey et al., 2011), rather than sports clubs. Incorporating these responses and some HPSC index items (Kokko et al., 2009), it produced the Health Promotion in Sport Assessment Tool (HP-SAT). It included a general organizational capacity section and the following dimensions: smoke-free environment, responsible serving of alcohol, sun protection, healthy eating, injury prevention, club management, welcoming and inclusive, violence in sport, and other. Validation was done using a test–retest reliability method among 22 sport state organizations in Australia.
The international Delphi study was primarily concerned with the social responsibility of sports clubs and how health promotion fits into this framework (Robertson, Eime, & Westerbeek, 2018). It included a panel of 56 experts (sport management journal academics and national sport organization managers) from 14 countries. Consensus identified 33 items among 7 social responsibility dimensions: human rights, labor practices, economic, governance, community development, fair operating practices, and environment. These items have not been tested within sports clubs to validate a measurement tool (Casey et al., 2011).
Health priorities vary between countries that can influence individual health behaviors (e.g., sun protection, nutrition factors); thus, indicators relevant to a range of sports cultures and systems are required (Kokko et al., 2016). Furthermore, approaches to health-promoting sports clubs vary, including settings-based approaches (Kokko, Villberg, et al., 2015), capacity building (Casey, Harvey, Eime, & Payne, 2012), social responsibility (Robertson et al., 2018), or specific behaviors (Kelly et al., 2014), which should be considered when building measurement indicators. Several limitations of previous works were identified: (1) mostly nonvalidated, nontheoretically based tools exist; therefore, no instrument rooted in a theory-based framework has been fully validated; (2) only culturally specific tools were found; thus, no international consensus exists; and (3) current tools do not take into account the many determinants of health (social, cultural, environmental, economic), each classified at the three sports club levels. The aim of this study is to reach an international consensus to create a measurement tool grounded in the settings-based approach at the macro (club), meso (official), and micro (coach) levels of health promotion in sports clubs. It is proposed that this tool will be used by officials, coaches, and sports participants to evaluate perceptions of health promotion orientation, guidance, and activities within their club.
Method
Study Design
A modified Delphi method was chosen to elicit expert opinion on items to include at each level of the sports club, for each determinant of health. The Delphi method is a method for structuring group communications, so that the process is effective in allowing a group of experts to reach consensus regarding a complex problem (Okoli & Pawlowski, 2004). This method has the advantage of collecting experts’ perspectives without confronting them directly, thereby keeping responses anonymous. The Delphi method establishes rounds of questions where each round builds on the previous rounds’ responses. A series of three rounds was conducted that included stages of item selection, generation, modification, and ranking.
Panelists
Sixty-nine experts were contacted via e-mail, having one of three profiles (sport science or public health academics, sport club director/management, regional, national, or international sport/health institution), at least 5 years of experience within their field, and a working knowledge of English. Location and profession were taken into account to ensure diversity and international representation. Panelists were chosen from members of the Erasmus + Sports Clubs for Health group (SCforH), the Health Enhancing Physical Activity (HEPA) Europe working group, researcher networking, and snowballing. Experts were invited to take part in each round regardless of previous round participation.
Preparation
The research team convened twice to review the existing tools, compile indicators, detect similarities, and reformulate items. Initial items were chosen based on a literature review (Geidne et al., 2019), the three previously mentioned Delphi studies (Kelly et al., 2014; Kokko et al., 2006; Robertson et al., 2018), and the two validated measurement tools: the HPSC index (Kokko et al., 2009) and the HP-SAT scale (Casey et al., 2011). Items from the adapted versions of the HPSC index were also included (Kokko et al., 2011; Kokko, Selänne, et al., 2015; Van Hoye, Heuzé, Van den Broucke, & Sarrazin, 2016). The research team clarified and refined the definitions of each sports club level (macro, meso, micro) and the determinants within each level (cultural, social, environmental, economic) based on the work of Kokko (2014).
Round Description and Analysis
Round 1
Item selection
The first round helped to select and propose initial items for each of the three levels (macro, meso, micro). Respondents were given the opportunity to delete and/or reformulate items in order to establish a stable list. Experts were able to duplicate items from one sports club level to another (i.e., macro, meso, micro), to reformulate, modify, clarify, and add supplemental information such as explanations. For example, the item “All youth events are held in an alcohol free environment” can be seen at the macro, meso, and micro levels.
Indicator rating
Panelists used three indicators for item selection: health promotion relevance (How relevant is the item with regard to health promotion in sports clubs?), feasibility (How feasible/doable is it for sports clubs?), and importance (How important is this item with regard to other priorities?). Items were rated on a 6-point Likert-type scale (1 = Do not agree at all to 6 = Totally agree).
Analysis
Consensus was achieved only when ≥80% of experts rated the Item 4 or above for all the indicators. Strong consensus was described as any response that received a mean score of ≥4 and an interquartile range (IQR) ≤ 1, moderate consensus to any mean score ≥ 3.75, or if an IQR ≤ 1.25 (von der Gracht, 2012). Items that fell below 80% for any indicator underwent qualitative analysis by the research team. The research team came to agreement whether to keep the original item, reformulate it, or exclude it for the second round.
Round 2
Item selection
The second round included new suggested items and reformulated items from Round 1. Experts were asked to validate the proposed items and to delete or add new items if they had suggestions or felt items were problematic, duplicated, or complicated.
Indicator rating
In addition to the three indicators from Round 1, experts also rated items based on relevance to sports culture in order to ensure items were applicable across multiple countries. Items were again rated on the same 6-point Likert-type scale from Round 1.
Analysis
Analysis was conducted using the same method as Round 1 with consensus being achieved when ≥80% of the experts rated Items 4 or above on the Likert-type scale for each of the four indicators. Researchers qualitatively analyzed items receiving <80% for health promotion relevance, feasibility, and importance indicators but immediately deleted items below 80% agreement on culture relevance.
Round 3
Item ranking
Researchers organized items into a specific determinant of health at each sports club level to propose to experts (Figure 1). Experts were asked to rank each item within the designated determinant per level. Item ranking was based on feasibility, importance, and health promotion relevance. If an item was not considered necessary, they were not required to rank it. The aim was to prioritize between 5 and 10 items per determinant with a minimum of 3 per category.

Four determinants at three sports club levels.
Analysis
In order to analyze items in Round 3, a weighted-point value based on number of items per club level and determinant was used to rank items for each panelist’s answer. Depending on the number of items per determinant (e.g., 7), 7 points were awarded for the highest ranked item, 6 points for the second item, 5 points for the third item, and so forth. Median scores were then calculated per item; only items with the five highest scores within each determinant/level were retained. If there were less than five items in a determinant at a particular level, researchers retained all items for the final questionnaire.
Data Collection
An email explaining the study’s purpose, procedures, and a consent clause was sent requesting participation. Surveys were sent in English to all 69 experts in each round regardless of previous round participation via web-based software (limesurvey.com). Rounds were expected to take 45 minutes to complete. Panelists were given 2 to 3 weeks to complete each round; nonrespondents were sent an email reminder after 7 days.
Results
Mean item scores on the Likert scale per indicator including expert agreement percentages for Rounds 1 and 2 are displayed in Table 1. A flow chart of the number of panelists participating per country in each round is displayed in Figure 2.
Rounds 1 and 2 Indicator Results.

Note. Items in grey were added to Round 2. Items with a (*) were reformulated by the research team.
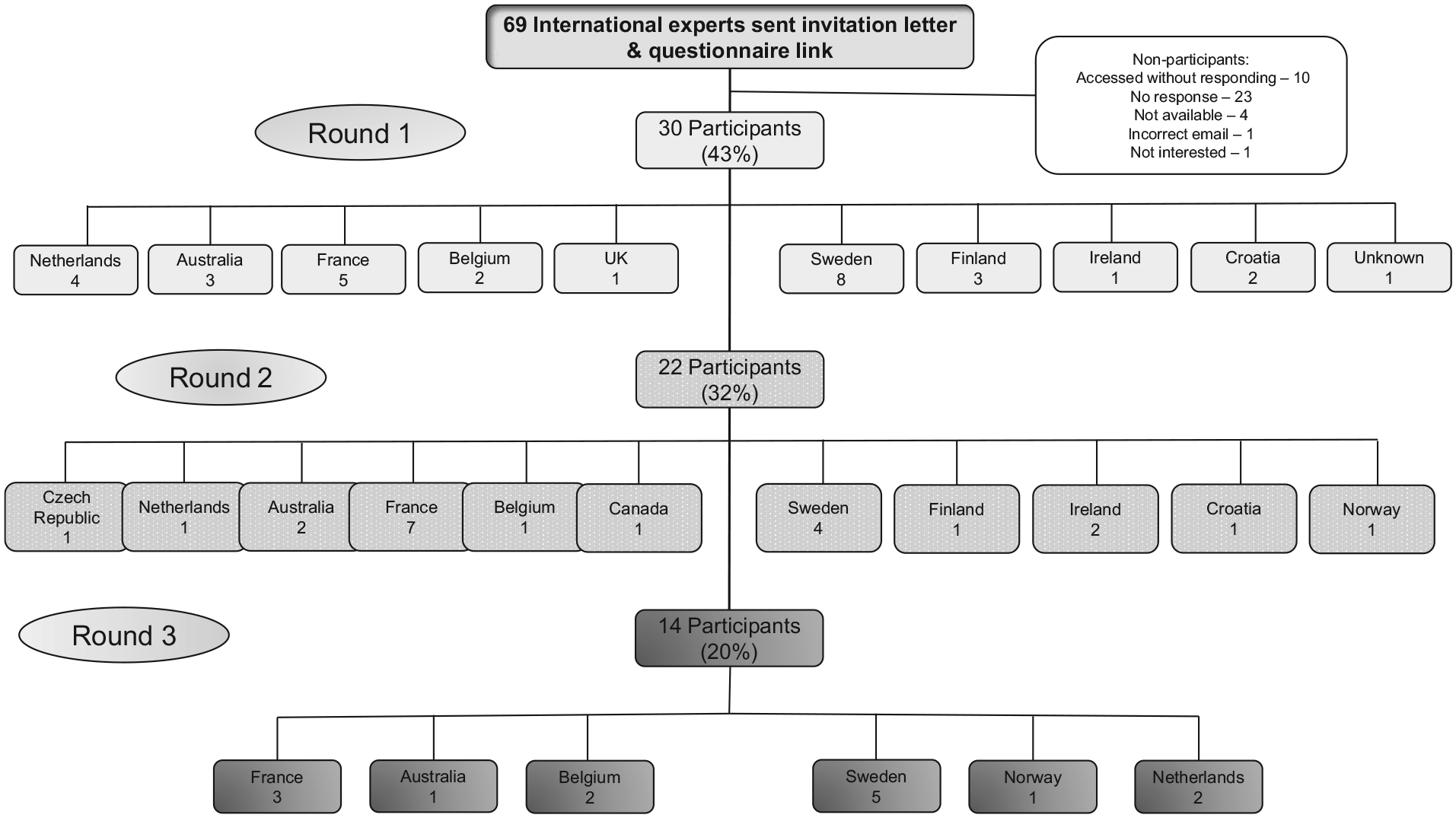
The three-round expert panelist flow chart.
In the first round, 30 experts (43%) answered the questionnaire (16 males, 13 females, and 1 nonspecified gender). Panelists were from nine different countries across Europe and Australia with a balance of academics (n = 12), nongovernmental sports organization (NGOs) members (n = 11), a governmental sports organization (n = 1), and others in sports and health–related sectors (n = 6). The first round included 31 items at the macro level, 11 at the meso level, and 17 at the micro level. All items were considered relevant and important to health promotion at the meso and micro levels. One item fell below 80% at the meso level and three items at the micro level; all of these in the feasibility indicator. More items fell below 80% at the macro level; seven in relevance, seven in feasibility, and five in importance. These items were reformulated for the second round. Panelists added two items at the macro level. Duplicated items included 18 from both the macro to the meso level and from macro to the micro level, 2 items were duplicated from the meso to the macro level, and 4 items from the meso to the micro level, as well as 2 from the micro to the meso level and 3 from the micro to the macro level. After duplication and reformulation of items, the second round consisted of 38 items at the macro level, 28 at the meso level, and 29 at the micro level.
The second round included 22 experts (32%, 14 males, 8 females) from 11 countries across Europe, Australia, and Canada. Panelists were composed of 9 academics, 9 NGO members, and 4 others from sports-related sectors. Of these panelists, 12 completed the first round and 10 were new to this round. After the second round, 80% consensus was not achieved for several items at each sports club level (10 macro, 10 meso, and 13 micro). At the macro level, six items were deleted: five for a low cultural relevance consensus and one for low feasibility. Researchers reformulated four items with a low feasibility consensus and experts added one extra item. The meso level included deletion of eight items. Low consensus in cultural relevance resulted in seven items being deleted and another item was removed due to low consensus on feasibility. Researchers reformulated two items with a low feasibility consensus and experts added three items. At the micro level, 11 items were deleted due to lack of cultural relevance and 1 due to low feasibility. Two items were reformulated and experts suggested six additional items. Going into Round 3 expert panelists were proposed 33 items at the macro level, 23 items at the meso level, and 23 items at the micro level.
The third round required experts to order and rank the items. At each level, panelists arranged items within the four determinants of health in order of highest priority. The five highest ranked items were retained. Whenever less than five items were ranked, all items for that particular sports club level and determinant of health were retained. Fourteen (20%) experts responded (eight males and six females) from six countries across Northern Europe and Australia, comprising six academics, four NGO employees, and four others in the sports sector.
At the end of the third round, the macro level contained 23 items: 7 cultural, 6 social, 5 environmental, and 5 economic determinants. The meso level included 20 items: 6 cultural, 5 social, 5 environmental, and 4 economic determinants. The micro level had 19 items: 6 cultural, 5 social, 4 environmental, and 4 economic determinants. The majority of items dropped (10) were at the macro level, most from the cultural and environmental determinants. Due to the lack of participation from North America, Asia, and Africa, an e-mail was sent to eight experts from these countries requesting their validation on the final list of items. Two North American academics provided validation. The ranked item list, divided by sports club level and categorized into their respective health determinants with the weighted point scores, can be seen in Table 2.
Round 3 Attributed Points With Final Item List.
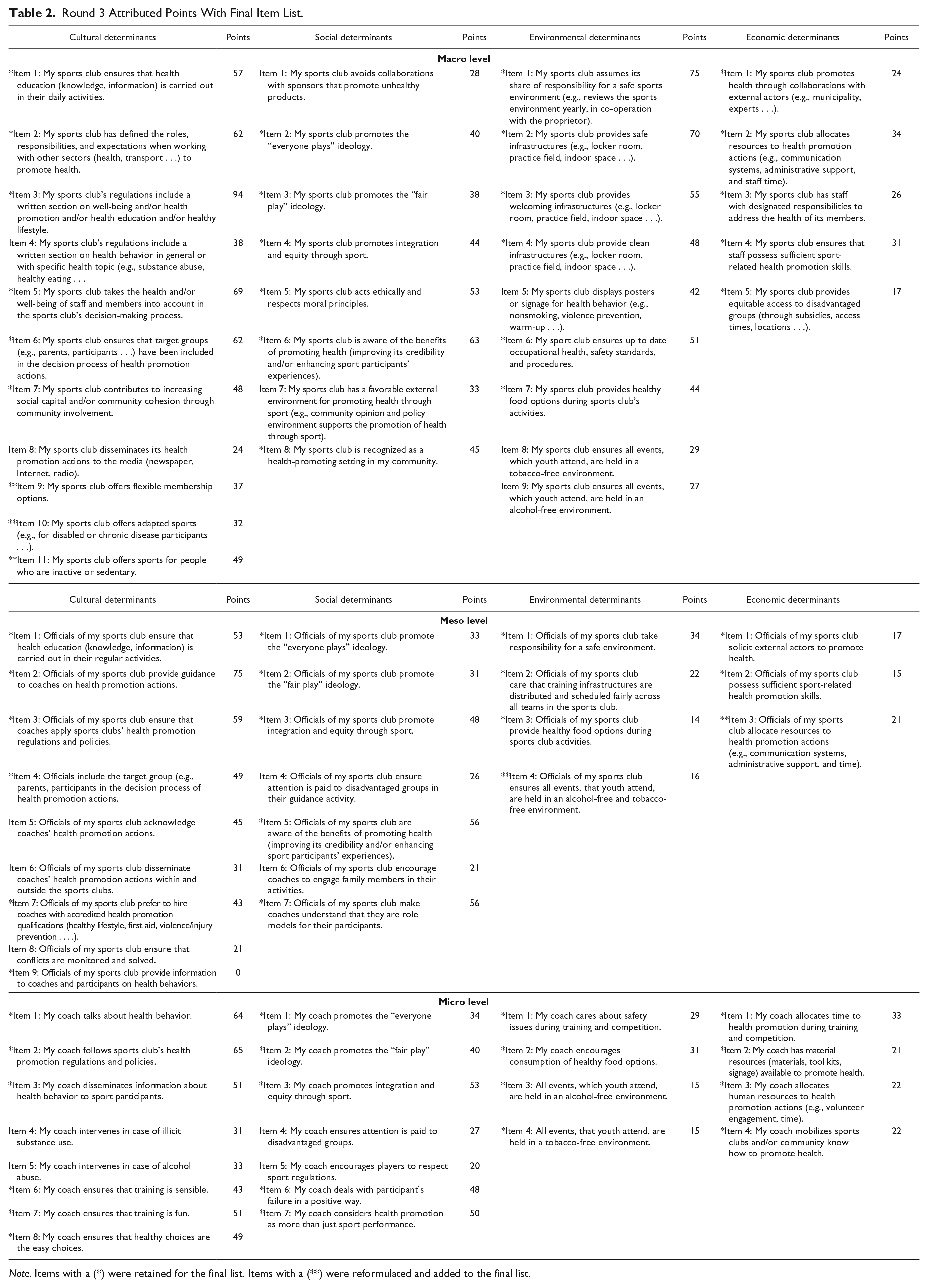
Note. Items with a (*) were retained for the final list. Items with a (**) were reformulated and added to the final list.
Discussion
A three-round Delphi method was used to achieve international consensus from 13 countries to create a multilevel tool for measuring the health promotion orientation of sports clubs. The final tool encompassed 62 total items: 23 at the macro level, 20 at the meso level, and 19 at the micro level. During Rounds 1 and 2, ratings were based on feasibility, importance, health promotion relevance, and specific to Round 2, cultural relevance. Feasibility was rated in terms of the item’s capacity to be accomplished within a sports club setting. Importance was considered with regard to the item being useful enough to be a priority. Health promotion relevance was regarding item applicability to the sports club setting, and cultural relevance was regarding the sports culture in the expert’s country. Because sports clubs primarily rely on volunteers with limited resources (Casey et al., 2011) and health promotion is not their core activity, but an “added value” (Kokko, Selänne, et al., 2015), including multiple indicators to measure these factors is a major strength of this study. In both these rounds, the feasibility indicator received the lowest consensus. Many panelists felt items were important and relevant for health promotion but not feasible, especially at the macro and micro levels. In comparison to other settings, such as schools which have curriculums and paid employees, sports clubs are often run by volunteers with limited budgets, viewing their primary objective as sports performance (Geidne, Quennerstedt, & Eriksson, 2013; Kokko et al., 2009; Van Hoye et al., 2016). This reinforces results from a previous literature review showing that the settings-based approach is rarely implemented within sports clubs (Geidne et al., 2019). Another strength of this study lies in the development of a tool with cultural applicability in many sport systems, as broad variations have been noticed in previous works (Casey et al., 2011; Kelly et al., 2014; Kokko et al., 2016) and suggestions have been made for wider diversity with regard to geographical reach (Kokko et al., 2016). Therefore, Round 2 specifically incorporated a rating of cultural relevance. Several items fell below the 80% agreement level for this indicator, for example, the item: “My sports club ensures the balance between sport activities and participants’ other daily activities is considered in coaching practice” was duplicated in Round 2 at all three levels but not found to be culturally relevant at any level. This may demonstrate cultural differences as it was originally in the micro level, and an expert suggested duplication into the meso and macro levels. Round 2 consensus indicated low cultural relevance for this item across all three sports club levels. In addition, one of the lowest agreed upon items for health promotion relevance was with regard to financing: “The sports club ensures that health promotion activities are being properly resourced (e.g., staffing, financial summaries, highlights, or case study reports).” Sports clubs are funded in different ways depending on the country; therefore, they may consider financing health promotion as the duty of their governing body while the club typically targets increasing participation rates (Eime, Payne, & Harvey, 2008). Interestingly, one of the lowest ranking items in importance had to do with offering flexible membership options, which is frequently cited as a barrier to sport club participation (Somerset & Hoare, 2018). If flexible membership options were offered in more clubs, this might attract new members.
Current research has centered on the sports club as an entity (macro level; Kokko et al., 2016), whereas this measurement tool is based on three levels (sports club, officials, and coaches), offering the ability to compare perceptions of sports participants to those of their coaches and likewise comparisons from coaches to officials. Actions at one level often depend on policies and guidance of higher levels (Kokko, 2014); therefore, intervention effectiveness can be altered by considering all involved stakeholders. For example, at the macro level, the highest ranked item for importance and relevance was, “My sports club’s regulations include a written section on well-being and/or health promotion and/or health education and/or healthy lifestyle.” This item directly links to a highly ranked item for importance at the micro level, “My coach(es) follow(s) sports club’s health promotion regulations and policies.” Because each level addresses the levels below (coaches and volunteers answer the macro and meso levels), if no written policies exist or are not expressed to the coaches from officials, health promotion efforts are difficult to realize. The addition of determinants at each level displays the complexity of the relationship between individuals and the sports club environment, as well as the difficulty of the implementation and measurement of settings-based approaches (Dooris, 2009). The classification of items into determinants at each level is grounded in scientific literature, reflecting the importance of rooting measurement tools and interventions into theoretical models (Glanz & Bishop, 2010). Moreover, both the socioecological approach (Dooris, 2009) and health promotion literature have shown that multiple-level actions (Jackson et al., 2006) are more efficient, underlying the need for measurement tools at different levels (setting, professional, participants).
Limitations
This study provides a first step toward an internationally developed measurement tool for assessing health-promoting sports clubs, but some limitations must be acknowledged. Although experts from each part of the world were invited to participate in each round, not all countries responded, meaning this tool might not be globally applicable. A second limitation exists regarding the panelists that chose to participate in the study. Their views may be different from those who declined participation; therefore, the final item list may not fully represent experts in both the health promotion and sports club fields. In order to minimize this limitation, one final email was sent out to the initial 69 experts requesting comments on the final list of items. Only two return emails were received; one from a Canadian academic expert and one from an American academic. Last, a limitation exists regarding the final number of items retained. The macro level included more items for panelist to rank within the four health determinants. Because the top 5 ranked items were retained, some items that reached 80% consensus in the previous two rounds could have been dropped for the final item list.
Implications for Practice and Future Research
Many researchers and government agencies have called for innovative settings to promote health (Geidne et al., 2019; Kokko et al., 2016; World Health Organization, 1986). Sports clubs offer an ideal setting but research is limited. To develop this setting, research is needed to understand orientations of sports clubs toward health promotion. This study offers expert consensus regarding the most important, feasible, and relevant items to monitor health-promoting sports clubs. Previous research has demonstrated a link between health promotion, positive sport experience, and perceived health; thus, increased activity to promote health within sports clubs is needed while keeping in mind clubs’ primary directives (Van Hoye et al., 2015; Van Hoye et al., 2016). By measuring social, cultural, environmental, and economic determinants of health at three levels, this is a more comprehensive measurement tool for comparing health promotion perceptions between sports participants, coaches, and officials. Several practical implications can be taken from the development of this tool: (1) it allows for comparisons of participants’, coaches’, and officials’ perceptions of health promotion done within sports clubs; (2) the tool highlights areas for improvement within each health determinant at each sports club level; and (3) it sheds light on the capacity of sports organizations to implement and monitor health promotion policies and practices. The measurement tool has been culturally adapted and translated from English into French and Swedish with a classic double-translation procedure. Answers are based on a 6-point Likert-type scale from strongly disagree to strongly agree. A user guide has been drafted in English and French to inform sports clubs on the importance of using the measurement tools and how to score and interpret results. Items on the tools have been tested for content clarity in English- and French-speaking populations of officials, coaches, and participants. Online psychometric testing of the three sports club levels in English and French is in progress. Validation testing includes factorial structure analysis, temporal stability, and predictive validity. Once validation is completed, this measurement tool can be used directly by sports clubs at one or multiple levels to determine and compare perceptions of health promotion within their club. The work undertaken in the present publication serves as a first step to inform policymakers about the ideal state of becoming a health-promoting sports club. The measurement tool helps identify and narrow the gap between the ideal and current state of health promotion within their sports club. Results can then be used to build policies at all sports club levels that focus on promoting a natural shift to increase the health and well-being of all club stakeholders.
Footnotes
Acknowledgements
The authors thank all the expert panelists who answered to any of the online surveys and gave insightful comments for the creation of this measurement tool, the SCforH group, and the HEPA Europe for assistance with expert contacts and Santé Publique France for their full support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is part of the PROSCeSS project, which was funded through a partnership between Santé Publique France, the University of Côte d’Azur, and the University of Lorraine.