
Abstract
Supermarkets located near schools influence adolescents’ food consumption. The aims of this study were (1) to measure dietary behaviors during school hours, (2) to investigate the effect of a nutrition peer-education intervention in supermarkets within walking distance to secondary schools on nutritional knowledge and attitudes toward healthy eating, and (3) to assess how the intervention was appraised by adolescents with a lower education level. The participants were adolescents aged 12 to 14 years from four secondary schools in Amsterdam, the Netherlands (n = 432). Cross-sectional analyses were performed to establish dietary behaviors (pretest). A quasi-experimental pre–post design with a comparison school was used (n = 3 intervention, n = 1 comparison). Intervention schools received the intervention in a supermarket near their school. The comparison school received no intervention. The appraisal of the intervention was assessed in the intervention schools (posttest). Most of the adolescents who purchased foods from retail food outlets near the school (71.1%) did so from supermarkets (88.6%). The nutritional knowledge scores (β = 0.69, 95% CI [0.23, 1.15], p = .003) as well as the attitudes toward healthy eating (β = 0.17, 95% CI [0.04, 0.29], p = .009) of adolescents from the intervention schools were statistically significantly higher after the intervention, relative to the comparison school. Nutrition peer education in supermarkets can improve nutritional knowledge and attitudes toward healthy eating among adolescents with a lower education. Future research on the short- and long-term effects of nutrition peer education on food purchases and dietary intake of adolescents is needed.
The majority of Dutch adolescents consume less than the recommended amounts of fruit, vegetables, and fibre, in addition to consuming excessive amounts of energy-dense, nutrient-poor foods (Van Rossum et al., 2016). Unhealthy diets increase the risk for overweight, obesity, and nutrition-related chronic diseases later in life (Reilly & Kelly, 2011). It has been well established that adolescents of lower socioeconomic position (SEP) have less favorable diets and lower adherence to dietary guidelines, than is the case for adolescents of higher SEP, thus placing them at higher risk for overweight, obesity, and nutrition-related chronic diseases (Zarnowiecki et al., 2014). For this reason, it is particularly important to promote healthier diets among adolescents of lower SEP.
Although multiple factors contribute to the dietary intake of adolescents, the current school food environment has been identified as an important driver of unhealthy diets (Glanz et al., 2005; Vandevijvere et al., 2016). This environment includes food that is accessible within schools (e.g., in canteens or from vending machines), as well as from food outlets (e.g., supermarkets, fast-food outlets) within walking distance of schools. On weekdays, adolescents spend a considerable amount of their time at school, thus making the school food environment an important setting for eating behaviors (Gebauer & Laska, 2011; Katz et al., 2008; Micha et al., 2018; Welker et al., 2016). In the Netherlands, most secondary school students are allowed to leave the school building during breaks in order to visit nearby retail food outlets, where they frequently purchase foods that are predominantly unhealthy (Middelbeek et al., 2007; Timmermans et al., 2018). Although it has been suggested that supermarket-based interventions could offer an opportunity for making positive changes in the dietary behaviors of adolescents (van der Horst et al., 2008; Wechsler et al., 2000), little is known about the effectiveness of such interventions. Previous studies have demonstrated that a supermarket tour including information about healthy food choices can enhance the knowledge and intentions of elementary schoolchildren and their parents with respect to healthy food purchases in supermarkets (Lafferty et al., 2006; van Assema et al., 1996).
A growing body of evidence suggests that peer education is an effective strategy for improving dietary behaviors among adolescents. In peer education, young people with similar key characteristics (e.g., social and cultural backgrounds) serve as role models and educate their peers (Harden et al., 2001). When adolescents identify with their peers, they tend to imitate their behaviors (Festinger, 1954; Salvy et al., 2012). Peer education is based in part on social cognitive theory, which suggests that knowledge and positive attitudes toward specific health behaviors are key factors in determining change in those health behaviors (Bandura, 1977). For example, two reviews have demonstrated that participation in peer-led nutrition education interventions enhanced the nutritional knowledge and positive attitudes of students in elementary and secondary schools with regard to healthy eating, in addition to improving their self-reported dietary intake (e.g., higher intake of fruits and vegetables) (Nelson & Nickols-Richardson, 2014; Yip et al., 2015). It has even been suggested that nutrition education may be more effective for adolescents when it is provided by their peers than when it is provided by older professionals (Mellanby et al., 2000). However, most nutrition peer-education interventions are conducted within the school, whereas conducting such programs in supermarkets around schools has the potential to influence the knowledge and attitudes of adolescents with regard to selecting healthy food choices at the point of purchase.
The aims of this study were as follows: (1) to measure dietary behaviors during school hours, (2) to investigate the effect of a nutrition peer-education intervention in supermarkets within walking distance to secondary schools in the Netherlands with regard to nutritional knowledge and attitudes toward healthy eating, and (3) to assess the ways in which the intervention was appraised by adolescents with a lower education level.
Method
Context and Design
This study was conducted as part of a collaboration between the Amsterdam Public Health Service, the Municipality of Amsterdam, the Amsterdam Health & Technology Institute, Albert Heijn (the supermarket chain with the largest market share in the Netherlands), and Vrije Universiteit Amsterdam in the Netherlands. The overall aim of this collaboration is to create a healthier food environment for children and their parents in low-SEP neighborhoods in Amsterdam and to study the effectiveness of these efforts. Compared with other districts in the Netherlands, these neighborhoods are characterized by more inhabitants of lower SEP and higher rates of overweight and obesity.
We used a quasi-experimental pre–post design including three intervention schools and one comparison school in Amsterdam, the Netherlands, to investigate the effect of the Healthy Supermarket Coach (HSC) on the nutritional knowledge of adolescents and their attitudes toward healthy eating. Data were collected from December 2015 through March 2016. The study was conducted according to the ethical standards declared in the Declaration of Helsinki 1975, as revised in 2000, and it was approved by the Medical Ethics Committee of the VU University Medical Center. Active written informed consent was given by all adolescents, and passive written informed consent was obtained from the caregivers of all of the adolescents.
School and Participant Recruitment
Supermarkets were selected from a list provided by the head office of the participating supermarket chain, containing addresses of supermarkets that had expressed interest in the HSC. The researchers approached secondary schools that had students with a lower education level and that were located in close proximity to the supermarkets, based on multiple criteria: (1) A school needed to be situated in a low-SEP neighborhood, as determined according to the Valuation of Immovable Property Act (VIPA), which is estimated annually (https://www.wozwaardeloket.nl/). This act establishes how municipalities are to assess the value of homes and businesses within specific neighborhoods, which is strongly associated with the average SEP of the people living in those neighborhoods. Neighborhoods with low or very low VIPA scores were defined as low-SEP. (2) The school needed to be located within a walking distance of approximately 5 minutes (≤500 meters) from a supermarket (Huisman & de By, 2009), such that students are able to visit the supermarket during school hours. The walking distance of 500 meters was established using Google Maps. (3) Only first- and second-year students (12–14 years of age) in these schools were selected for participation. The HSC intervention focused on these students, as the eating habits of children who are undergoing the transition from primary school to secondary school are likely to be changing and becoming less healthful (Lytle et al., 2000). (4) Only students following a lower educational level were invited to participate, as they are particularly likely to be at increased risk for adapting unhealthy dietary behaviors (Hanson & Chen, 2007; van Dorsselaer et al., 2010). In the Netherlands, the secondary education system comprises three levels, based on the intellectual abilities of students: prevocational, senior general, and preuniversity. All of the adolescents participating in the current study were following the prevocational track. The researchers approached all five schools that met the criteria by sending an email explaining the rationale of the study and including an invitation for participation. Three schools ultimately agreed to participate. Two schools declined to participate due to lack of time. To recruit a comparison school, we selected a school that was matched to the intervention schools based on neighborhood VIPA, as well as according to inclusion criteria similar to those adopted for the intervention schools. The first school we approached was willing to participate, and it was thus included in this study. Only one comparison school was included, due to resource constraints and logistical reasons. The comparison school was located in a different part of the city to prevent cross-contamination between the intervention and comparison schools. As a result, the final sample for this study consisted of four schools (n = 3 intervention schools, n = 1 comparison school).
To address the first aim, all adolescents who had completed the baseline questionnaire were included (n = 432). The total number of questionnaires included participants of the intervention schools (n = 351) as well as those of the comparison school (n = 81; Figure 1). To address the second aim, only those who had completed both the baseline and posttest questionnaires and who had received the HSC intervention were included, in order to investigate the effect of the HSC (n = 370). The total number of questionnaires included participants of the intervention schools (n = 299) as well as those of the comparison school (n = 71). To address the third aim, adolescents in the intervention schools who had completed the posttest and who had received the HSC intervention were included, in order to examine their appraisals (n = 338). Reasons for attrition included absence due to illness or logistical reasons (e.g., unexpected changes in class schedules).
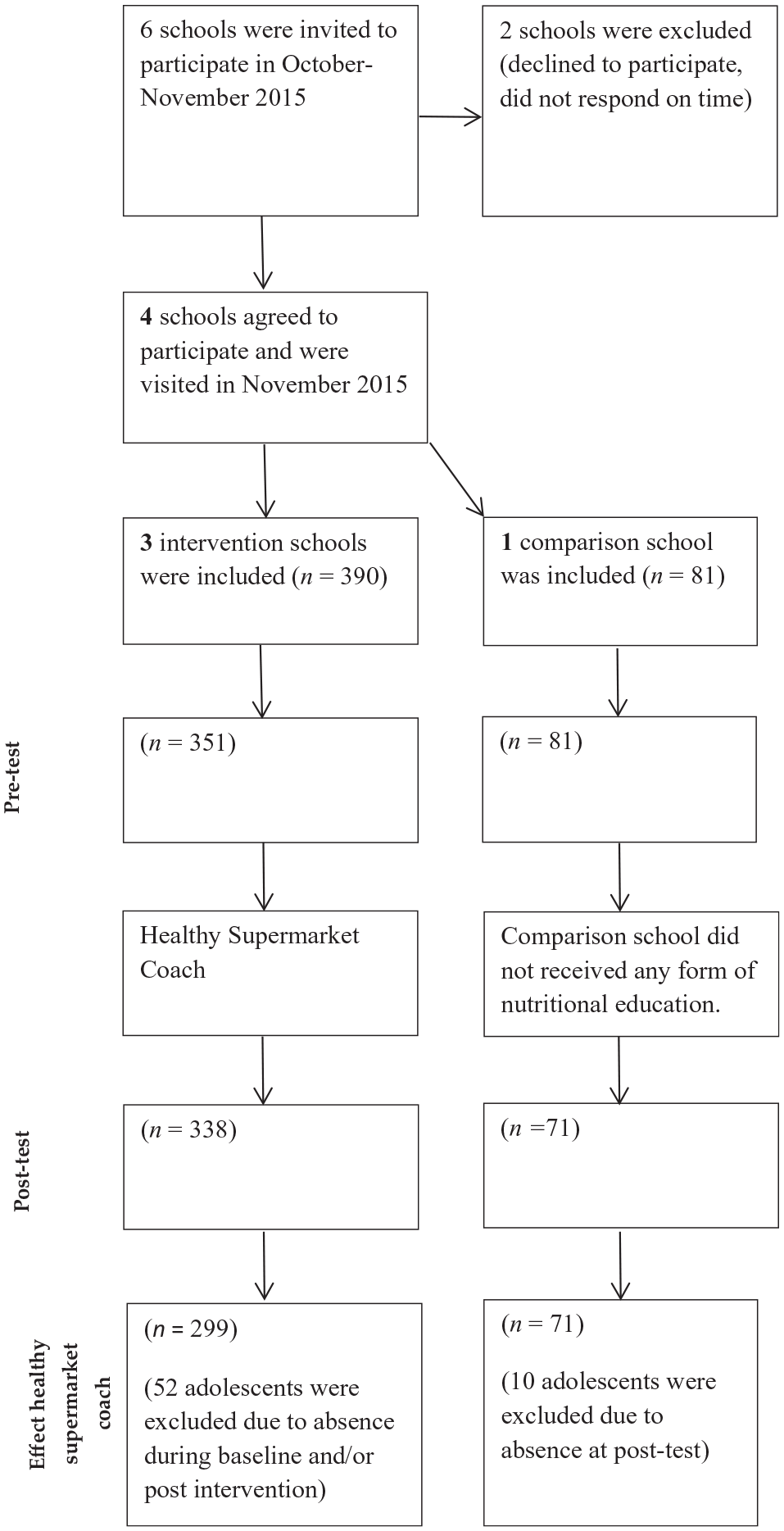
Flowchart.
Supermarket Recruitment
Three supermarkets of the participating supermarket chain that were located within walking distance of the intervention schools (one per intervention school) were approached between October and November 2015. An employee of the head office contacted store managers of the selected supermarkets by telephone to inform them about the study and to request their participation. Store managers who agreed to participate were visited by the head office employee and a researcher for purposes of introductions and the provision of practical information about the study. Throughout the intervention period, each supermarket manager was phoned weekly by a researcher to discuss the progress of the project.
Description of the HSC Intervention
The HSC intervention was developed by the research team, in cooperation with a noncommercial communication agency that specializes in peer education for children and adolescents. The intervention was developed during two cocreation sessions involving experts in peer education, a nutritionist, a health psychologist, 14 young supermarket employees (15–21 years of age; Session 1), and 10 students with a lower education level (age 12–14 years) from three secondary schools (Session 2). The employees and students were involved in the development of the intervention to ensure that the intervention would correspond to the level and needs of the target population. The HSC intervention consisted of a 45-minute workshop given by two young supermarket employees in each of the three supermarkets located close to the intervention schools. The HSC was based on principles from social cognitive theory and the theory of planned behavior (Ajzen, 1991; Bandura, 1986). It was also based on successful nutrition peer education interventions conducted elsewhere that have shown to improve nutritional knowledge and attitudes toward healthy eating (Story et al., 2002; Venditti et al., 2009).
The following behavioral-change strategies were incorporated into the HSC: (1) providing information about healthy foods and drinks and on the outcomes of a healthy diet, (2) improving self-efficacy through skill development, and (3) goal setting (Michie et al., 2011). The three strategies were translated into the following intervention components, respectively. First, adolescents participated in an interactive quiz (11 questions) about healthy (or unhealthy) foods and drinks. The main goal of the quiz, which was held on the shopping floor amid the product shelves, was to assess the participants’ nutritional knowledge (e.g., daily fruit and vegetable recommendations) and ability to understand and use food labels (e.g., amounts of sugar). After each question, the answers were discussed within the group. Furthermore, detailed information relating to the specific question was provided by the HSC in order to increase the participants’ nutritional knowledge. Second, the adolescents created an affordable, healthy lunch to stimulate positive attitudes and self-efficacy with regard to healthy eating (Fitzgerald et al., 2013). Third, the adolescents formulated action plans (implementation intentions) with their classmates with regard to healthy food and drink purchases in the supermarket (Adriaanse et al., 2011).
Store managers from each of the participating supermarkets selected a total of 12 employees (15–21 years of age)—approximately four from each supermarket—based on the criteria for peer educators (e.g., having an outgoing and assertive character and of diverse gender and cultural background; Nelson & Nickols-Richardson, 2014; Yip et al., 2015). The employees in our study were slightly older than the adolescents, to ensure that they would be accepted as positive role models by the adolescents. Moreover, the employees were acquainted with most of the adolescents visiting the supermarket during school hours. After selection, the employees were trained as peer educators by two peer education experts. During the training, they learned how to implement the elements of the HSC intervention and to promote healthy food and drink choices among the adolescents during the workshop (Michie et al., 2011). After the training, they were awarded the official title of Healthy Supermarket Coach. The extent to which the intervention was implemented as intended in the three supermarkets was assessed in several ways. Each HSC received a standardized delivery format, accompanied by clear, simple instructions. In addition, after each workshop, the HSCs completed evaluation forms to assess their performance, in addition to discussing possible improvements with their partners. Throughout the entire intervention period, the researcher paid unannounced weekly visits to the intervention supermarkets. During each visit, the researcher observed compliance with the program and discussed it with the store managers. In all, the HSCs conducted 27 workshops in total in the three participating supermarkets during a 2-month period. Each workshop contained a new set of adolescents who participated in groups of approximately 15 classmates during school hours.
Study Procedures
Adolescents in the intervention schools completed the baseline questionnaire before participating in the workshop, and they completed the posttest questionnaire 1 week after the workshop. The students in the comparison school completed questionnaires at the same time as the adolescents in the intervention schools. The comparison school did not receive any form of nutritional education. The students completed the questionnaires in their classrooms under the supervision of a teacher, accompanied by research assistants and/or a researcher.
Measurements
The baseline questionnaire consisted of 29 questions measuring demographic characteristics (gender, school year [first, second], age [in years]), regular dietary behaviors during school hours, nutritional knowledge, and attitude toward healthy eating. The adolescents were asked to use a 5-point Likert-type scale to indicate how often they brought foods or drinks from home to school (never to every day), whether they finished the lunches that they brought from home to school (never to always), and how often they purchased foods or drinks within the school building (e.g., from the school canteen or vending machines; never to more than once a day). They were also asked to indicate whether they purchased foods or drinks in retail food outlets within walking distance of their schools during school hours (“no,” “yes”) and, if so, where they usually did that (“from supermarket,” “at a fast-food restaurant,” or “somewhere else, namely, . . .”). In this study, retail food outlets were defined as places selling ready-to-eat foods and drinks during regular school hours (e.g., supermarkets and fast-food restaurants). The students were also asked to describe the kinds of foods or drinks that they usually brought from home to school, or purchased within the school building or from retail food outlets near the school, and the amount of money that they spent on foods or drinks (open-ended answers). The three kinds of foods or drinks that were described most often are presented for each point of purchase (home, school, food outlets).
Nutritional knowledge was assessed according to questions taken from validated surveys used in previous studies among adolescents (Ferro-Lebres et al., 2014; Grosso et al., 2013). Various aspects of nutritional knowledge that are thought to influence the food choices of adolescents were measured according to 11 multiple-choice items. The following is one example: “On average, how many calories should girls consume per day?” (response categories: “1 = 2,000,” “2 = 2,500,” “3 = 3,000”). For 10 of the questions, there was one correct answer for each of the questions, corresponding to one obtainable point. For one item, there were two correct answers, and two points could be obtained. The sum of the points obtained on all questions was taken as the nutritional knowledge score (0–12), with higher scores indicating greater nutritional knowledge.
Attitudes toward healthy eating were assessed according to six items scored on 5-point Likert-type scales ranging from −2 to +2 (Ajzen, 1991). For example, the respondents indicated how important (very unimportant to very important) they considered healthy eating. The internal consistency (Cronbach’s alpha) of the items measuring attitude toward healthy eating was α = .64 at baseline and α = .69 at posttest (Kline, 1999). Cronbach’s alpha scores indicate the internal consistency of items and assess whether multiple-question Likert-scale items form a reliable construct. A mean sum score (ranging from −1 to +2) was calculated for attitude, with higher scores indicating more positive attitudes toward healthy eating.
Like the baseline questionnaire, the posttest questionnaire consisted of questions relating to nutritional knowledge and attitude toward healthy eating. In addition, the posttest questionnaire for the intervention schools included 11 questions assessing the appraisal of the HSC intervention. First, adolescents were asked to use 5-point Likert-type scales to indicate whether they had enjoyed the workshop (not at all [−2] to very much [+2]) and to rate the HSC (0–10). They were then asked to indicate their agreement with nine statements about the HSC workshop, again along a 5-point Likert-type scale (totally disagree [−2] to totally agree [+2]). For example, the students were asked whether they were interested in following the HSC’s recommendations about healthy eating. Mean scores were calculated, with higher scores indicating more positive evaluations.
Data Analyses
We used descriptive statistics to summarize the demographic characteristics and dietary behaviors of the participating adolescents, along with their appraisals of the HSC program. To test if there were baseline differences in demographics between the intervention and comparison schools, chi-square and one-way analyses of variance were used. Linear regression analyses were conducted to investigate the effect of the HSC intervention with regard to nutritional knowledge and attitude toward healthy eating. Condition (intervention [yes = 1, no = 0]) was used as an independent variable, with the dependent variable being the score on the posttest, adjusted for the score at baseline. Both a crude model (adjusted only for baseline scores) and an adjusted model (i.e., crude model + age, gender, school year) were calculated and presented.
Results
Participant Characteristics
The study sample comprised 432 adolescents: 390 (82.8%) in the intervention schools and 81 (17.2%) in the comparison school (Table 1). The mean age of the respondents was 13 years (SD = 0.94), with boys accounting for around half of the group (48.8%). Most (87%) of the adolescents were first-year secondary school students (p < .05).
Baseline Characteristics of the Adolescents (n = 432).

Significant difference between the intervention schools and comparison school (p < .05).
Dietary Behaviors of Adolescents
A majority of the adolescents (307, 71.1%) reported that they purchased foods or drinks in retail food outlets located within walking distance of their schools; 227 (86.6%) did this in the supermarket, with 22 (7.2%) purchasing foods or drinks in fast-food outlets and 13 (4.2%) purchasing it somewhere else. The adolescents spent an average of €2.30 (~USD 2.45) per day to purchase foods or drinks on an average school day. The foods or drinks purchased most frequently from the supermarket were potato chips (36%) and energy drinks (56%), with those most frequently purchased within the school being sandwiches (48%) and sugary drinks (30%). The foods and drinks that were most frequently brought from home to school were sandwiches (91%) and water (43%). Additional details on the dietary behaviors of the adolescents on an average school day are provided in Table 2.
Frequency and Kinds of Food That the Adolescents Brought From Home and Purchased in and Around School During School Hours at Baseline (n = 432).
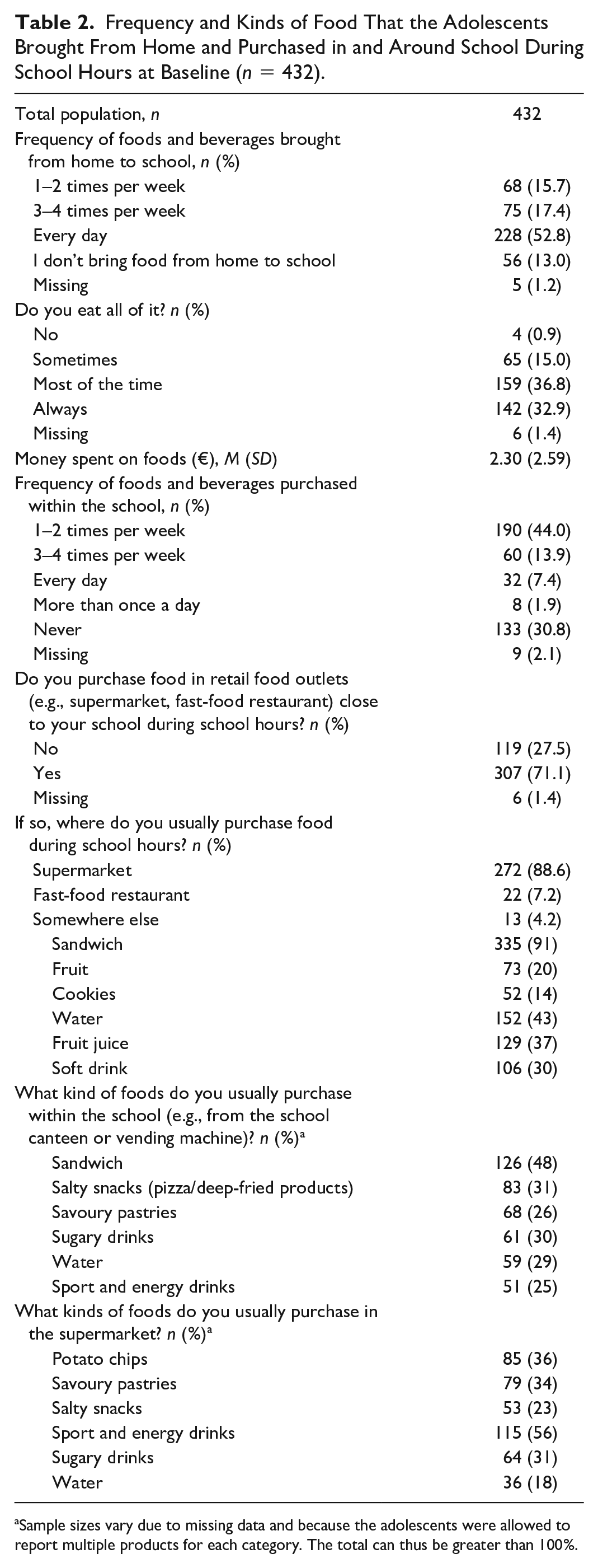
Sample sizes vary due to missing data and because the adolescents were allowed to report multiple products for each category. The total can thus be greater than 100%.
Nutritional Knowledge and Attitudes Toward Healthy Eating Before and After the HSC Intervention
Nutritional knowledge (preintervention: M = 7.71, SD = 1.72 vs postintervention: M = 8.24, SD = 1.76, p ≤. 001) and attitudes toward healthy eating (pre: M = 0.81, SD = 0.56 vs post: M = 0.94, SD = 0.58, p ≤ .001) improved among the adolescents who participated in the workshop (Table 3, for the frequencies of scores on the 5-point scale for each attitude item separately and the overall attitude toward healthy eating, see Supplemental Material 1). At posttest, nutritional knowledge (pre: M = 7.35, SD: 1.49 vs post: M = 7.36, SD = 1.79, p = .941) and attitudes toward healthy eating (pre: M = 0.85, SD = 0.45 vs post: M = 0.89, SD = 0.55, p = .416) among the adolescents from the comparison school remained stable relative to their scores at baseline. Adjusted linear regression analyses indicated that the HSC intervention generated a statistically significant improvement in both nutritional knowledge, β = 0.69, 95% CI: [0.23, 1.15], p = .003, and attitudes toward healthy eating, β = 0.17, 95% CI: [0.04, 0.29], p = .009 (Table 3).
Intervention Effect on Nutritional Knowledge and Attitudes Toward Healthy Eating (n = 370).

Adjusted for gender, school year, and age.
p < .05.
Appraisal of the HSC
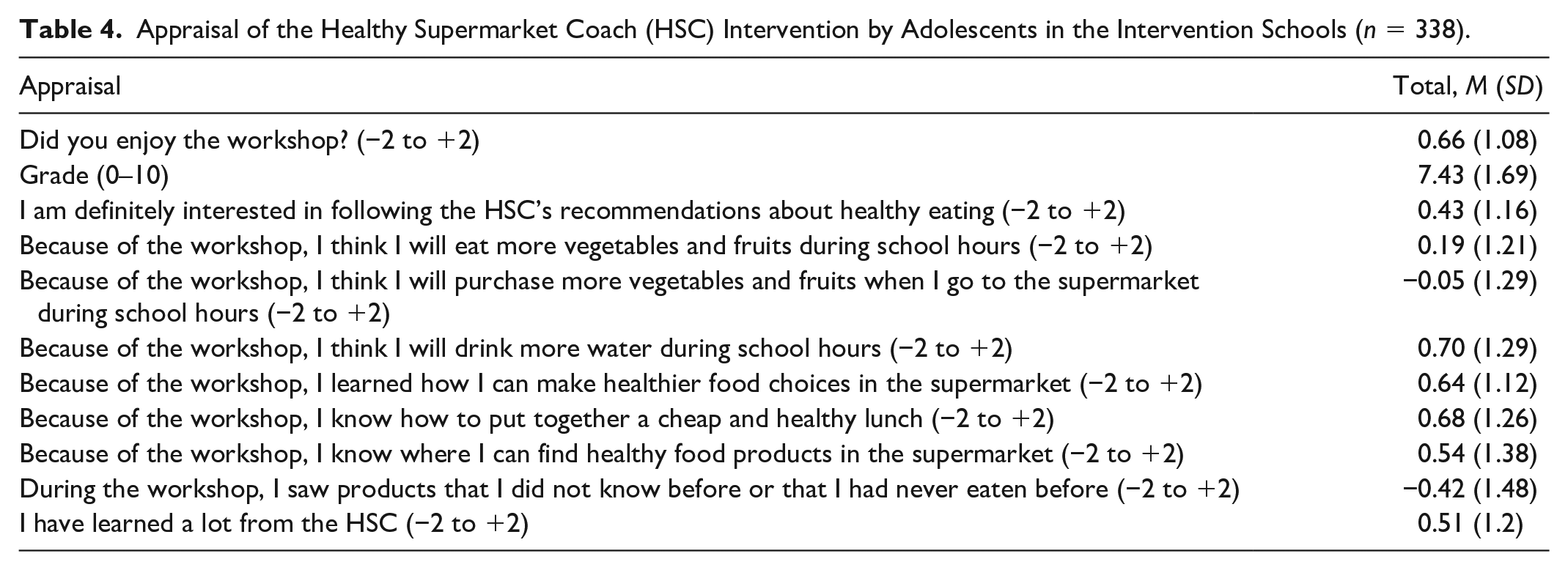
The adolescents evaluated the HSC intervention positively (Table 4). For example, they rated the workshop with an average of 7.43 points (on a scale from 0 to 10), and they reported having enjoyed the workshop, based on a scale ranging from −2 to +2 (M = 0.66, SD = 1.08). Moreover, they agreed (at least in part) that the workshop had taught them to make healthier food choices in the supermarket (M = 0.64, SD = 1.12) and that they intended to implement the lessons that they had learned (M = 0.43, SD = 1.16).
Appraisal of the Healthy Supermarket Coach (HSC) Intervention by Adolescents in the Intervention Schools (n = 338).
Discussion
The results of this study indicate that nutrition peer education in the supermarket generated a statistically significant improvement in the nutritional knowledge of adolescents, as well as in their attitudes toward healthy eating. They further evaluated the HSC intervention positively and indicated that they had learned to make healthy and affordable food choices in the supermarket.
Our findings are consistent with those of previous studies on the effectiveness of nutrition peer education programs (Yip et al., 2015). While most previous programs have been executed within schools, ours was held in supermarkets located within walking distance of schools. One previous review demonstrated that nutrition education tours in supermarkets increased the knowledge, skills, positive attitudes, and intentions of customers regarding healthy food choices after the tour (Nikolaus et al., 2016). Instead of adolescents, however, these supermarket tours targeted adult women or elementary school children with their parents. Although the outcomes are in line with ours, the review included only intervention studies that had no elements of peer education. Any comparisons should therefore be interpreted with caution.
Our results also indicate that most of the adolescents (89%) who reported purchasing foods or drinks in the school environment during school hours did so in the supermarket. This outcome confirms the notion that supermarkets constitute an important setting for food or drink purchases during school hours. In line with previous studies, most of the adolescents in our sample reported purchasing unhealthy foods or drinks during school hours (He et al., 2012; Ridder et al., 2017). In one study, almost one third of all Dutch adolescents between the ages of 13 and 15 years purchased unhealthy snacks and sugary drinks within the school (19.7% and 11.2%, respectively) or in stores nearby the school (17.9% and 14.4%, respectively) at least 3 days per week (Ridder et al., 2017). Almost 70% of the adolescents in our study indicated that they brought foods or drinks from home to school at least 3 days per week, which suggests that the unhealthy foods or drinks that they purchased in the supermarket during school hours were largely supplemental to their daily meals. This assumption is further supported by the observation that potato chips and sport and energy drinks were the foods or drinks most frequently purchased in the supermarket, as these foods and drinks are not regarded as components of a meal. This emphasizes the need for interventions to encourage healthy food purchases within the school food environment among Dutch adolescents.
To the best of our knowledge, this is the first study to investigate the effects of a nutrition peer-education workshop conducted in a supermarket for adolescents. This intervention thus occurred at a key point of purchase for adolescents. In addition, we targeted adolescents with a lower education level, given that lower educational levels have been associated with more unfavorable food or drinks purchases, as compared with those with higher levels of education (Turrell et al., 2002). In addition, both adolescents and the supermarket employees were involved in developing the workshop that was used in this study. In this way, we tried to ensure that the workshop would correspond to the level and needs of the target population, thereby increasing its effectiveness. Finally, the results regarding the adolescents’ eating behaviors during school hours contribute to a growing body of literature on the dietary behaviors of adolescents. In addition to its contributions, however, this study is subject to several limitations. First, it was limited to first- and second-year students with a lower secondary education level. The results can therefore not be generalized to other education levels or older adolescents. Another limitation concerns the use of self-reported data, which may have been subject to underestimation or overestimation, recall bias or social desirability bias. Another limitation is the use of determinants of dietary intake as outcome measures instead of measures of dietary intake. It is known that nutritional knowledge and positive attitudes toward healthy eating are important determinants of dietary intake among adolescents. For example, one study of children aged 4 to 16 years identified positive associations between nutritional knowledge and the consumption of vegetables and fruit, along with negative associations between nutritional knowledge and the consumption of snacks and sugary drinks (Grosso et al., 2013). We cannot know whether the HSC workshop actually resulted in healthier food or drink purchases in the supermarkets, however, as improvements in attitudes and knowledge do not always translate into desired behaviors (Croll et al., 2001; Story et al., 2008). One logical next step would be to study the short-term and long-term effectiveness of the HSC intervention on the food or drink choices of adolescents in the supermarket. Future research should also focus on the use of reliable and accurate measurements to examine the food and drink purchases of adolescents (e.g., by collecting cash register receipts during school breaks). The results of our study provide several insights for practice and policy. It could be worthwhile to consider further investigation on whether nutrition peer education could be part of the school curriculum. Moreover, the HSC intervention might be suitable for other points of purchase frequented by adolescents (e.g., school canteens or sports clubs). In addition to peer education, food outlets located in close proximity to schools should be encouraged to create a supportive food environment designed to encourage adolescents to make healthy food choices, especially in light of the fact that the healthiest choices currently tend not to be the easiest choices within these environments (Timmermans et al., 2018).
Conclusions
Our study demonstrates that nutrition peer education in supermarkets can improve nutritional knowledge and positive attitudes toward healthy eating among adolescents with a lower secondary education level. This could have a positive effect on the purchase and consumption of healthy foods and drinks by these students. Additional research is needed to generate further insight into the short-term and long-term effects of nutrition peer education on the actual food and drink purchases that adolescents make in supermarkets, as well as on their dietary intake.
Supplemental Material
Supplement_1_22-07-2019 – Supplemental material for The Healthy Supermarket Coach: Effects of a Nutrition Peer-Education Intervention in Dutch Supermarkets Involving Adolescents With a Lower Education Level
Supplemental material, Supplement_1_22-07-2019 for The Healthy Supermarket Coach: Effects of a Nutrition Peer-Education Intervention in Dutch Supermarkets Involving Adolescents With a Lower Education Level by Marlijn Huitink, Maartje P. Poelman, Jacob C. Seidell and S. Coosje Dijkstra in Health Education & Behavior
Footnotes
Authors’ Note
The authors declare that they have no financial relationships relevant to this article. The supermarket chain collaborated in the organization of the study but did not have any role in the analyses of this study. The supermarket chain signed a contract and agreed that the results of this research would be published regardless of the outcome.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported is funded by the municipality of Amsterdam and the Vrije Universiteit Amsterdam.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.