
Abstract

Keywords
Every 10 years, the U.S. Surgeon General has released Healthy People, a set of health promotion and disease prevention targets to evaluate the nation’s health and to guide the allocation of public health resources for the coming decade (Office of Disease Prevention and Health Promotion, 2020a). Healthy People’s goals and objectives shape local, state, and national policies, programming, and funding. In each of the five iterations of Healthy People, there are few men’s health-specific goals and objectives, despite the persistent finding that men live shorter lives than women (Griffith, 2020; Griffith, Bruce, & Thorpe, 2019; National Center for Health Statistics, 2017). These differences between men and women and among men have economic (Thorpe et al., 2013), health (Bilal & Diez-Roux, 2018), and programmatic implications (i.e., limits awareness of preventive screenings and regular health care for men of all ages; Office of Disease Prevention and Health Promotion, 2020b). In this commentary, we argue that explicitly including goals and objectives for men that mirror their leading causes of death will be particularly important to improving the nation’s health and to achieving health equity.
From Healthy People 2000 to 2030, the majority of objectives and subobjectives specific to men have focused more on men’s sexual health behaviors than their leading causes of death. Looking back at previous iterations of Healthy People, language specific to men in Healthy People 2010 was included in only one of 28 leading health indicators, and 26 subobjectives out of approximately 900, whereas the leading health indicators and subobjectives for women were, 2 and 58, respectively (National Center for Health Statistics, 2012). The Healthy People 2010 subobjectives focused heavily on sexual health and family planning with the exception of one subobjective each for low-risk drinking, prostate cancer, and hip fractures for males aged 65 years and older (Centers for Disease Control and Prevention, 2015). Healthy People 2020 did not specify men as a topic area, but did have data by gender and included 28 objectives specifically targeting males (Porche, 2010). Of the 355 total objectives in Healthy People 2030, there are 30 objectives that explicitly mention women, females, or maternal health, but only four objectives that specifically mention males or men: one regarding prostate cancer, one regarding family planning, and two regarding sexually transmitted infections (Office of Disease Prevention and Health Promotion, 2020c). Thus, with the exception of prostate cancer, none of the four objectives presented in Healthy People 2030 (Figure 1) align with the five leading causes of death for men: heart disease, cancer, unintentional injuries (e.g., motor vehicle accidents, drowning, falls, and poisoning [e.g., drug overdoses]), chronic lower respiratory diseases (mainly chronic obstructive pulmonary disease), and stroke (Centers for Disease Control and Prevention, 2019).
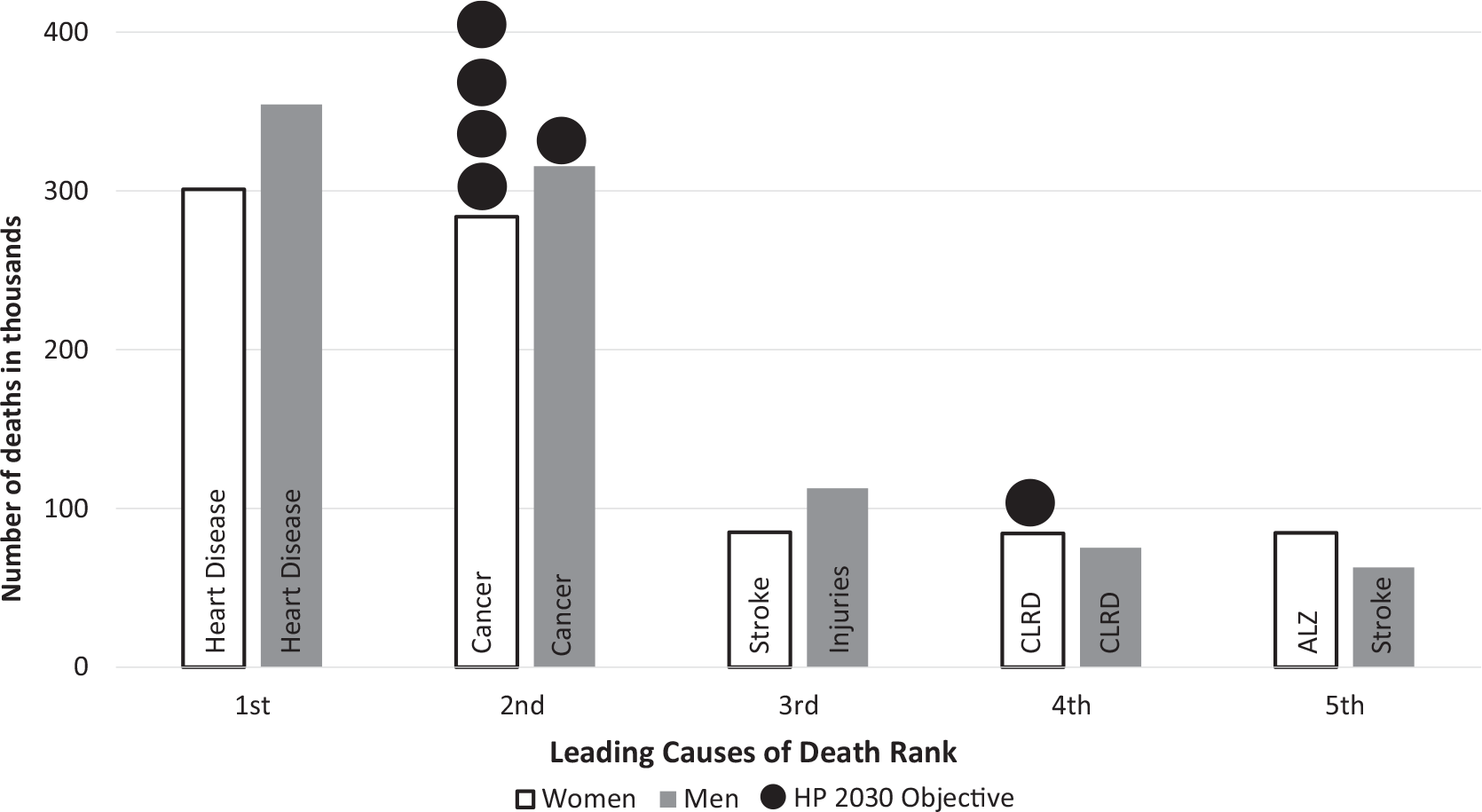
Number of deaths, top five leading causes of death for men and women in the United States, 2018 and Healthy People 2030 corresponding objectives.
Given the gendered patterns of disease morbidity and mortality and the economic and social costs associated with them, one might wonder why these gendered patterns of mortality do not play a bigger role in guiding Healthy People in particular and U.S. health policy in general. Though we have no definitive answers, we offer two potential explanations. One explanation may be that discourse explaining men’s health problems and patterns tend to suggest that the primary sources of men’s poor health are located in men’s biology, men’s internalized notions of masculinity, or social norms and pressures among men rather than the social determinants of men’s health (Elder & Griffith, 2016; Fleming et al., 2014; Griffith, 2018). Framing men’s health in this way locates men’s poor health in their biology, thinking patterns, and emotions rather than policy and programmatic deficits. Second, Healthy People and other policy guidelines use singular demographic characteristics like sex (e.g., men) or race (e.g., non-Hispanic Black) to prioritize disadvantaged groups (Braveman, 2006) rather than considering how the intersection of characteristics (e.g., sex and race [non-Hispanic Black men]) helps identify populations at unique risk (Griffith, 2018, 2020). Using a singular approach rather than an intersectional one is limited because it does not consider how a fundamental determinant such as racism is gendered in ways that need to be considered to mitigate or undo its effects on health and well-being (Griffith, 2018).
Recommendations
To address the gaps noted above, we offer four recommendations to “avoid the silence of men’s health issues among the national objectives” (Porche, 2010, p. 6). First, we recommend devising a men’s health supplement that is based on the leading causes of death and key social determinants of leading causes of death for men. Second, we recommend emphasizing sex and gender in the Healthy People 2030 “Tools for Action” webpage in more nuanced and sophisticated ways. Additional emphasis on the concept that a gendered approach is not synonymous with women and must include men is an important viewpoint to encourage Healthy People 2030 readers and consumers to understand. To help facilitate the use of these objectives, the Healthy People 2030 evidence-based resources webpage should establish a tab for men and reorganize the men’s topic area section to highlight objectives that disproportionately impact men—as was done with the five nongender specific objectives that disproportionately affected women—to help local and state health departments create targeted goals and programs for men and boys. This would address the lack of state-level infrastructure observed by the Men’s Health Network’s 2018 survey that found only 35% of state public health agencies have a website with information specific to men’s health and only 8% have an established commission to study and create men’s health recommendations (Fadich et al., 2018; Williams & Giorgianni, 2010).
Third, within Healthy People, there seems to be no attention given to the heterogeneity among sex categories. Healthy People could facilitate health promotion efforts that educate the public health workforce and communities on how sex and gender are distinct yet interconnected concepts. Most health outcomes are a combination of both biological (e.g., sex) and psychosocial (e.g., gender) factors, not sex or gender exclusively (Springer et al., 2012). Using sex categories obscures biological males’ and females’ gender identities (i.e., how they view themselves), gender expressions (i.e., how one chooses to express themselves on the continuum of masculine and feminine), and sexual orientations (i.e., who they are attracted to in relation to their own sex/gender). Health promotion efforts are likely to be more effective if they are designed to reflect the populations whose health they seek to promote.
Finally, we recommend developing a U.S. men’s health report or report card to evaluate the progress and refine the focus of specific Healthy People 2030 objectives for men. Healthy People objectives already are used as guideposts for men’s health policies and programs in the Tennessee Men’s Health Report Card (Center for Research on Men’s Health, 2021; Griffith, Semlow, et al., 2019) and the Connecticut Report Card on Health Equity among Men and Boys of Color (UConn Health Disparities Institute, 2018). These reports could be models for a nationwide U.S. men’s health report card (Treadwell & Young, 2013) that could be released in the middle of the decade to provide an opportunity to refine policies and programs before the previously articulated pattern of overlooking men’s health objectives repeat yet again in Healthy People 2040.
Conclusion
Men’s health issues are understated in comparison to other gender-specific health issues targeted by the national objectives and national patterns of disease mortality (Porche, 2010). A gendered approach should include men and not be synonymous with women (Varanka, 2008). By having more Healthy People goals and objectives that mirror the leading causes of death for men and consider the heterogeneity among men, Healthy People would facilitate national efforts to improve health and well-being as well as to achieve health equity in order to evaluate policies and tailor programs to improve health outcomes for all.
Footnotes
Authors’ Note
Andrea R. Semlow is now at Parkland Hospital and Health System, Dallas, TX, USA. Derek M. Griffith is now at Georgetown University in Washington, DC. At Georgetown, he is a founder and codirector of the Racial Justice Institute, founder and director of the Center for Men’s Health Equity, and professor of health systems administration and oncology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported in part by the American Cancer Society (RSG-15-223-01-CPPB) and the National Institute on Minority Health and Health Disparities (5U54MD010722-02).