
Abstract
Refugee children are less likely than their non-refugee peers to receive timely diagnoses and treatment for mental and/or behavioral health problems, despite facing multiple risk factors including potential exposure to trauma during premigration, migration, and postmigration experiences. Social–Emotional Learning offers preventive mental health education for children through well-established, evidenced-based curricula. Although there are clear benefits of Social–Emotional Learning curricula, which can help children achieve long-term success emotionally and academically, Social–Emotional Learning curricula are not easily accessible for refugee children, often because of language and socioeconomic barriers. In this pilot study, we evaluated the feasibility and acceptability of an adapted Social–Emotional Learning program that included culturally specific, multilingual, trauma-informed wellness, and physical education during the COVID-19 pandemic: EMPOWER (Emotions Program Outside the Clinic With Wellness Education for Refugees). We used the Intervention Mapping framework which guided the (1) planning, (2) program development, and (3) mixed-method evaluation of the feasibility and acceptability of the EMPOWER pilot. We found that this adaptation was well-received by Afghan refugee families and that COVID-19 safety measures were well-understood after participation. Challenges emerged around videoconferencing connectivity and around finding a common language for discussing emotions. Future iterations of the program and evaluations will require continued partnerships with community members and organizations. As we continue and expand EMPOWER, we aim to evaluate short-term improvement in Social–Emotional Learning competence as well as long-term mental and behavioral health outcomes for children and their families.
Refugee children are less likely than their nonrefugee peers to receive timely diagnoses and treatment for mental and/or behavioral health problems, despite facing multiple risk factors including potential exposure to trauma during premigration migration and postmigration stages (Alemi et al., 2014; Alemi & Stempel, 2018; Bronstein & Montgomery, 2011). In the era of COVID-19, barriers to timely diagnosis and care as well as mental health risks have increased, especially for refugee populations (Brickhill-Atkinson & Hauck, 2021; Rees & Fisher, 2020). Risk factors during the COVID-19 pandemic that may exacerbate mental health concerns already faced by refugees include food insecurity, inability to social distance, and educational disruptions. Refugees are particularly vulnerable to exacerbations of language barriers, isolation, and economic insecurity (Campion et al., 2020; Endale et al., 2020; Mattar & Piwowarczyk, 2020; Rees & Fisher, 2020). Improving access to preventive mental health initiatives is one approach to reduce disparities in access to mental and behavioral health care for refugee children and their families.
Social–Emotional Learning (SEL) offers preventive mental and emotional health education for children through well-established, evidenced-based curricula with education in five domains: self-awareness, self-management, social awareness, relationship skills, and responsible decision making (CASEL, 2021). SEL has been found to improve multiple skills for children; a recent systematic review and meta-analysis found that, compared with control groups, children who participated in SEL curricula demonstrated improvement in social and emotional competence, behavioral self-regulation, and early learning skills along with reduced behavioral and emotional difficulties (Blewitt et al., 2018). Specifically, emotional competence—the ability to identify one’s own feelings, to identify the feelings of others, and the skills to communicate and cope with emotions to guide thinking and actions—is associated with successful school and work performances and decreased susceptibility to disease (Goleman, 1995; Lau & Wu, 2012; Rockhill & Greener, 1999; Salovey & Mayer, 2016).
Although there are clear benefits of SEL curricula, to our knowledge, no studies to date have adapted SEL tools for use with refugee children. In this pilot, we used the Intervention Mapping framework to plan, develop, and evaluate an adapted SEL program that focused on emotional competence and self-awareness for refugee children during the COVID-19 pandemic (Bartholomew et al., 1998). We selected the framework by using the Dissemination and Implementation Science Tool, a resource to guide the selection of theories and frameworks (Dissemination & Implementation Models, 2021). Intervention Mapping is a well-established framework used in the design and analysis of health education interventions that aligned well with our goals to adapt and implement EMPOWER (Emotions Program Outside the Clinic With Wellness Education for Refugees). With this adaptation, rooted in needs identified in prior community-based participatory research (Rosenberg et al., 2021), we sought to augment the components of the evidence-based SEL curricula focused on emotional competence with novel, trauma-informed, and culturally specific wellness components. We aimed (1) to describe program development through adaptation of an evidenced-based SEL curriculum with wellness components for refugee children (2) to assess the feasibility and acceptability of this initiative, and (3) nurture engagement and trust within the community for future wider-scale SEL initiatives with refugee children and families.
Method
We assessed the development and evaluation of the EMPOWER program using the Intervention Mapping framework which guided the (1) planning (identifying gaps and selecting theoretical constructs); (2) program development and adaptation (creating a matrix of proximal program objectives, selecting and adapting a theory-based intervention, adapting the intervention, and developing an evaluation plan); and (3) mixed-method evaluation of feasibility and acceptability (Bartholomew et al., 1998).
Planning
Planning the EMPOWER curriculum began with a needs assessment. We used principles of community-based participatory research to engage with community members (including refugee resettlement agency employees, nongovernmental agency directors, educators, and health care providers) and partnered with community stakeholders during all stages of planning, implementation, and analysis (Israel et al., 1998). Based on emerging pandemic-related needs, prior qualitative interviews conducted with Afghan families in the community (most recently resettled refugees were from Afghanistan in this community), and known deficiencies in available mental and physical health preventative resources (Asgary & Segar, 2011; Barghadouch et al., 2016; Nosè et al., 2015; Saunders et al., 2018), we developed a plan which addressed the following key areas of need and gaps: (1) COVID-19 education, (2) social–emotional competence (using theoretical constructs), and (3) physical health and wellness.
Program Development
We followed the five steps of the Intervention Mapping framework to develop the EMPOWER curriculum (Bartholomew et al., 1998). First, we created a matrix of proximal program objectives for the pilot program, which included (1) demonstration of feasibility of delivering a curriculum focused on emotional competence to a refugee community, (2) establishment of trust, and (3) dissemination of COVID-19 safety education. Second, we selected and adapted a theory-based intervention: emotional self-awareness within SEL. Third, we worked with a cross-disciplinary team to adapt the SEL curricula for Afghan families during the COVID-19 pandemic which included in-person and videoconferencing (Zoom Video Communications Inc, San Jose, CA) activities (see Programmatic Elements section). Fourth, we specified adoption and implementation plans, including safety, location, recruitment, preparedness, and programmatic elements. Finally, we generated an evaluation plan that focused on evaluation of the three programmatic objectives.
Programmatic Elements
The full curriculum, which we compiled in an online research manual (EMPOWER, 2021), included five in-person, 75-minute activities and 4 weekly 1-hour Zoom sessions. The in-person curriculum included social–emotional awareness activities through games and art, COVID-19 education, yoga-based physical activities (each child received a yoga mat for a socially distanced physical activity). Zoom curricula offered opportunities for reinforcement with larger groups, and “refresher” Zoom sessions were held throughout the year during children’s school breaks. Due to time limitations, the scope of the SEL activities in the EMPOWER pilot was limited to emotional competence through self-awareness, as this component of the SEL curriculum is foundational to the other four domains (CASEL, 2021).
Participants and Setting
We recruited families in partnership with Elena’s Light, a community nonprofit organization that supports refugee families in New Haven, Connecticut, the United States and surrounding areas. The majority of recent refugees in the New Haven area are from Afghanistan, and thus EMPOWER participants included Afghan refugee children, 5 to 15 years old, who have completed ≥1 year of school in the United States. Sessions occurred in safe outdoors spaces within walking distance of family homes and on Zoom.
Mixed-Method Evaluation
Rationale for Mixed-Method Evaluation
We elected to perform a mixed-method, cross-sectional evaluation to assess prespecified quantitative measures of interest—feasibility, COVID-19 knowledge, and at-home continuation of programmatic elements—while also allowing opportunities to explore parents’ overall impressions about barriers to and facilitators of engagement for future iterations after the EMPOWER pilot using qualitative inquiry. Questionnaires and interviews were conducted concurrently over Zoom. The evaluation, conducted after the pilot intervention was complete, was approved by the institutional review board (ID#2000030455). The survey questions and interview guide (see Supplemental Appendix table) were developed with coauthors and with direct feedback from global health researchers at our institution from across disciplines who have worked with Afghan refugee families (Ventevogel et al., 2013).
Quantitative Methods
Binary (yes/no) questions addressed feasibility to attend, with the opportunity to verbally describe any challenges in more detail. Satisfaction was assessed by asking if participants: (1) would refer a friend, (2) would enroll again, and (3) felt the program was worthwhile. COVID-19 knowledge questions were based on a previously administered survey (see Table 3 and Alsan et al., 2020). Parents were also asked to reflect on the continuation of curricular components at home, including (1) yoga (the physical activity taught in EMPOWER) and (2) discussions of emotions.
Qualitative Methods
According to the COREQ (consolidated criteria for reporting qualitative studies checklist), we describe methodology within three domains: (1) research team, (2) study design, and (3) analysis (Tong et al., 2007).
Members of the interviewing research team (Julia Rosenberg [JR], Caroline O’Brien [CO], Patricia McDonough Ryan [PMR], and Fereshteh Ganjavi [FG]) met and interacted with the respondents prior to the Zoom interviews and had worked with nonprofit organizations in the region for at least 6 months. The primary interviewer (JR) is a female pediatrician and research fellow.
The primary interviewer conducted interviews over Zoom with a Farsi, Dari, and/or Pashto interpreter. After verbal informed consent was read in the respondent’s preferred language, with permission, responses were audio-recorded. Interviews were transcribed in real time with postinterview proofreading and comparison with the audio recordings. Respondents were either the mother, the father, or both parents together. Parents of all participating family units (N = 13) participated. A $25 gift card was distributed to respondents. All interviews were approximately 1 hour.
Mixed-Method Analysis and Integration
Qualitative and quantitative components, which included parental responses as well as attendance data, were separated for analysis. Descriptive statistics were conducted on quantitative elements. We used the constant comparative method to analyze themes in the qualitative data and iteratively refined the interview guide over the course of the interviews (Corbin & Strauss, 2008). A two-person coding team (JR, CO) analyzed written transcripts using grounded theory methodology (Corbin & Strauss, 2008). Discrepancies were resolved by discussion, and the research team then reviewed codes and emerging themes and agreed on trends and themes from qualitative responses. We used established mixed-methodology approaches to integrate quantitative and qualitative results with merged analysis which compared and contrasted divergences (Curry & Nunez-Smith, 2015).
Results
Participant Characteristics
As shown in Table 1, a total of 35 children from 13 families participated in and completed the EMPOWER pilot. The number of participants from each family ranged from one to five children, with a median age of 10 years. About half (54.3%) of child participants were female. Primary languages were Dari (46.2%) and Pashto (53.9%). Median time residing in the United States for parents was 5 years. The majority (69.2%) of guardians who attended the sessions were mothers. From this sample of participating families, all 13 completed the survey and interview (response rate = 100%). Respondents included mothers alone (53.9%), fathers alone (15.4%), or both together (30.8%).
Child and Family Characteristics.

Possible responses in response to question, “What is highest grade level you completed”: None (0), 1st, 2nd, 3rd, 4th, 5th, 6th, 7th, 8th, 9th, 10th, 11th, 12th grade, college, graduate school.
Implementation Outcome: Feasibility
A total of two families withdrew after their first EMPOWER course, and 13 families (87%) completed the curriculum. Zero parents among those who completed the course reported problems with (1) understanding written or verbal materials, (2) travel, or (3) timing of the program. Four respondents (30.8%) reported challenges with Zoom, including prolonged loss of power after a severe storm (n = 1), a child feeling too shy (n = 1), forgetting the class (n = 1), and children being unable to set up Zoom while parents were working (n = 1; Table 2).
Programmatic Outcomes (N = 13).

Implementation Outcome: Participant Satisfaction and Areas for Improvement
As noted in Table 2, all of the 13 interviewed parents reported satisfaction in measures we assessed. When we asked parents for feedback on future iterations of EMPOWER, many of their responses addressed acculturation and additional support around parenting skills to support social–emotional well-being. This included increasing opportunities to connect with and integrate within the Afghan refugee community and to gain tools to integrate into the American community, especially through language education and through more in-depth lessons related to EMPOWER.
Regarding interaction with others in the Afghan community, one parent shared, If I had control of this program, I would love to add more engagement between Afghan kids . . . I’d try to introduce the kids to each other more so they could know each other and be friends and continue friendships. I know with COVID-19 kids are not as regular, but that is something I would love when my kids see them in the next years. Making more friendship between kids is important. Because here in this country they don’t know anybody and we don’t have many family members and we don’t know many kids to communicate with. (Interview #4)
Regarding language acculturation and English acquisition, one mother emphasized her concerns and desires to have more opportunities for English interaction and learning, especially with remote learning during the COVID-19 pandemic: I do, I’m always stressed 24/7 about their English and their studies. Their English isn’t that good, it’s hard for them to do it. It’s hard because they can’t learn from Zoom, and it’s hard with the schools closed. (Interview #12)
Related to opportunities for further learning, many parents requested more sessions and more in-depth education. One example father articulated interest in anger management with role-playing. This parent had experience with similar programs in Afghanistan: There were some aspects that could be enriched, for instance more practical work with kids. When we’re talking about emotions and anger and how to manage, we need more specific role-plays before reaching the stage of controlling anger. Before reaching the stage of controlling anger, there are causes. Specifically, if you tell why a kid gets angry, what is the reason, to provide information about the background, the causes of anger, and then show them how they can avoid getting angry, before reaching the stage that they cannot control their anger. (Interview #2)
This father also offered specific guidance on how to continue programs for whole-family units while respecting cultural norms: Culturally, we are not ready to sit male and female with each other, still that is a barrier for bringing families together. To avoid not sending their children to these programs, it will be good to have different stations for children and for parents. For parents, I’m not sure if would be able if you would be able to get participants for female directly but it would be possible to go through their husband and then coordinate through them to get female participants. (Interview #2)
Programmatic Outcome: Reaching Beyond Planned Objectives and Planned Participants
When asked their perspectives of “what the program was about,” most parents identified COVID-19 safety and physical activity as objectives, and some also described emotions and wellness. Many also identified a perceived objective that was not in the initial EMPOWER design objectives: safe social interaction during the COVID-19 pandemic. As one parent stated as follows: It was good for them to see others. (Interview #1)
Another parent described this social interaction and its connection to her children’s well-being: I feel my kids were anxious and unhappy and really bored at home. There was no school, as you know, and we didn’t have anywhere to take them out. That was helpful for them to go out to have some activity. It emotionally and mentality helps them a lot, and it opens their minds; they know there is another life out there. (Interview #3)
Although the EMPOWER curriculum was geared toward children, many parents described that they also valued the lessons learned and shared many of the experiences with their children. As one parent stated, I learned through my kids. (Interview #2)
Even parents who did not attend the sessions learned from some of the activities and ideas the children brought home: Before, the kids were at home with no physical activity. [Now,] they practice the sport that they did in the outside. They’re active and inspired us to be active too. I was not involved directly in the class; I had two jobs but when I came back I saw they were playing at home, this was the advantage. (Interview #10)
Other parents described how they learned about and valued interactive enrichment activities, which empowered them to reframe their family playtime and activities: You know, before, my wife and I were thinking, “Just take the kids outside and take them to the mall and bring them home as activity.” But that’s not a real activity. After, we’ve seen several other activities and games you do with the kids. Now, we know if we sit with them and do a real activity, do painting and requesting things to do, that will be more helpful than just taking them outside and then bringing the home. We have to be more meaningful with what we are doing with them. They can learn something from us and do a real activity with them. That was a really good outcome from this program for me and my wife. (Interview #4)
Programmatic Outcome: COVID-19 Safety Knowledge
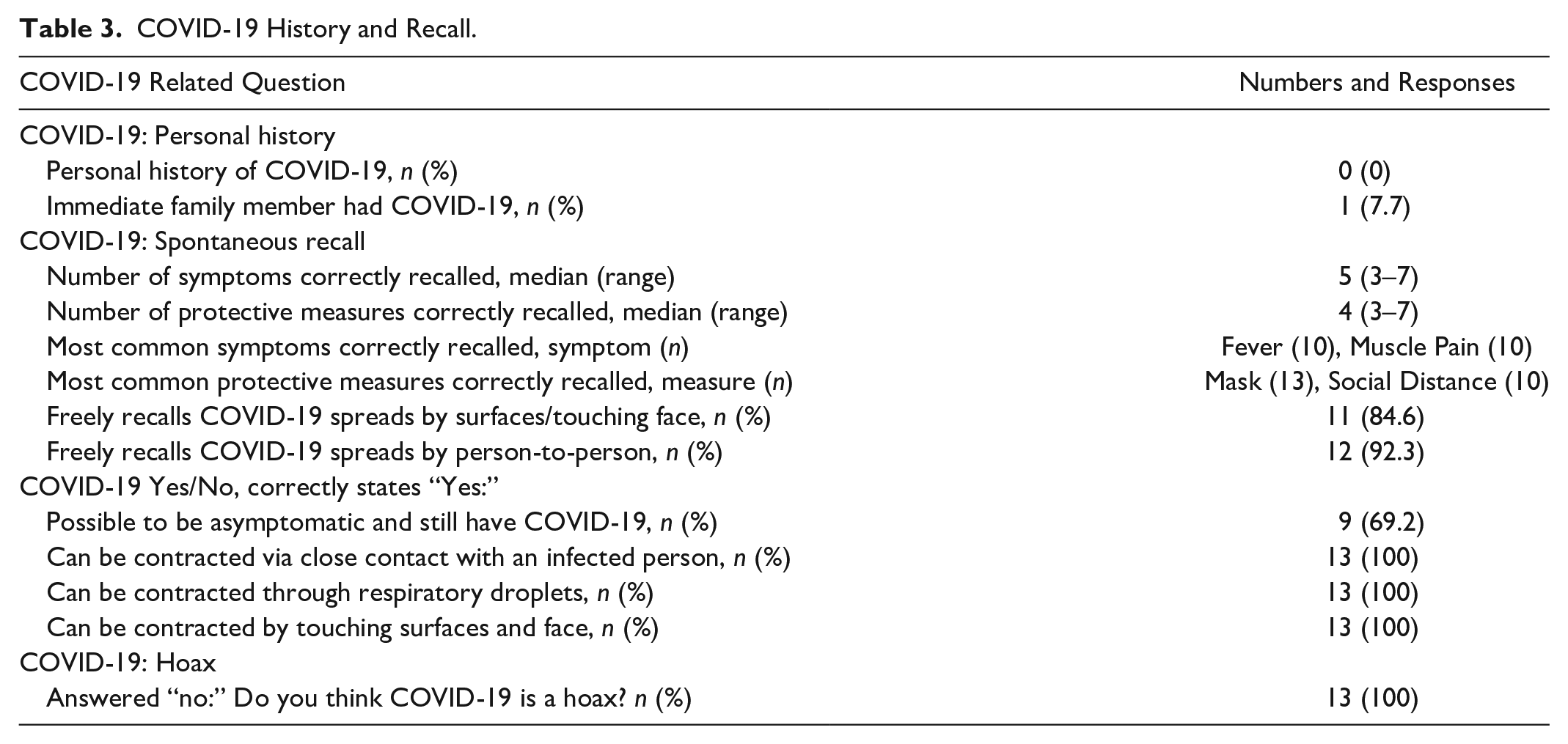
Many parents described a main purpose of EMPOWER was to provide COVID-19 education. As shown in Table 3, after completion of the program, all of the surveyed parents did not think COVID-19 was a hoax, and all correctly identified modes of COVID-19 transmission. Parents were asked to freely recall symptoms of COVID-19 and protective measures. The symptoms most frequently recalled by parents were fever and muscle pain (both recalled by 10 [76.9%] of the parents). All (100%) freely recalled that masks were a protective measure, and 10 parents freely recalled social distancing. None of the participants reported a personal history of COVID-19.
COVID-19 History and Recall.
Programmatic Outcome: Yoga-Based Physical Activity
Many families (69.2%) described that their children continued yoga after completion of EMPOWER. About half (46.2%) of parents surveyed had tried yoga themselves and nearly all (92.3%) were interested in learning more about yoga for themselves (Table 2).
Programmatic Outcome: Social–Emotional Wellness
Parents provided a variety of responses without a clear pattern when surveyed about changes for themselves and their children when discussing emotions (Table 2). When discussing the emotional component of the curriculum and parents’ comfort with discussing emotions at home, several areas of strength as well as gaps in knowledge emerged.
Some parents freely recognized emotions as an important part of the curriculum. For example, when asked what the program was about, one parent responded as follows: Awareness about COVID-19 and symptoms and child emotion and stress during the pandemic lockdown, to have support for children to deal with the lockdown. (Interview #2)
Several referred to the cards and games to help exemplify this point: Sometimes they take their cards and show me [emotions]. (Interview #1) Now that they have the cards and they’ve been introduced to them, I try to join them and talk about emotions with them too. (Interview #5)
When asked about comfort with discussing emotions in the home, nearly all parents described comfort to some degree. For example: It’s pretty easy and I feel comfortable because I learn from them and they learn from me. Every human feels their own emotions but it’s good to talk about it. (Interview #5)
While these areas of strength and recognition of and comfort with emotions are important, we encountered challenges finding common language to discuss emotions with respondents. For example, when asked about emotions, many of the parents would not talk about emotions but, rather, would discuss hopes and dreams for their children’s futures (whether this was in Pashto, Dari, or English). Some examples are below, with responses from parents who were asked about discussing emotions at home with children: Yes we are talking with them, what you want to be in future and we talk with them and they listen. (Interview #4) They tie the emotions with the future and what they want to become. A doctor, a teacher, a cop, so they turn feelings into something where they talk about the future. They also talk about emotions leading to talking about things they want to do, like helping the poor. (Interview #5) We do talk about it, my kids start talking about their future and that’s how we get into the topic (I like this or that and how their future will be). (Interview #8)
Discussion
In this pilot study of EMPOWER, we used Intervention Mapping to adapt an SEL and wellness curriculum for refugee families and implemented the adapted curriculum while addressing knowledge about COVID-19. Findings from our analysis of this pilot suggest general acceptability and feasibility and good COVID-19 knowledge after participation. Opportunities to improve the program include increasing parental involvement, securing optimal outdoor spaces, and preparing language about emotions with community partners.
This pilot program was well-received. Two families withdrew after the first session, but subsequent attendance was sustained by all participants. This included returning months later for Zoom “refresher” sessions, which the majority of participating children attended during their winter and spring breaks. All parents stated that they found the program worthwhile and would recommend to friends.
The COVID-19 pandemic necessitated curriculum redesign, and while some of these pandemic-related directives may be lifted in the future, many of the adaptations were well-received and will be incorporated even after the pandemic. These adaptations included Zoom “refresher” sessions and grouping by family unit (rather than by age). Parents and observers alike noted that siblings supported each other and enjoyed a variety of age-appropriate SEL activities. Parents participated with their children and continued lessons at home; they learned through their children. These observations are supported by robust literature describing the effectiveness of parental-training interventions, which can reduce behavioral problems in children (Furlong et al., 2012; Kaminski et al., 2008; Perrin et al., 2014). Thus, future iterations of EMPOWER will incorporate parents and will involve more explicit parental training while respecting cultural norms as advised by parents and community partners.
Although COVID-19 knowledge before participation was unknown, parents demonstrated excellent knowledge of COVID-19 health and safety and correctly identified symptoms, mechanisms of transmission, and protective measures at the program’s conclusion. COVID-19 education will likely be a consistent component of the curriculum in the near future, as there is an ongoing need for mitigation measures, and children do not have early access to COVID-19 immunizations. However, even when COVID-19 is no longer a preeminent concern, future iterations of the program can be adapted to identify and disseminate timely, up-to-date, translated, culturally appropriate health and wellness information to refugee families.
Although our results support feasibility, acceptability, and consistent attendance, several barriers to participation and areas for improvement were noted. Parents identified that challenges related to connecting to Zoom. Although we provided help with Zoom connectivity in the beginning of the program, in future iterations of EMPOWER, we can offer additional support to connect families to remote learning hubs (such as through libraries). Additionally, choosing a safe, protected, outdoor space was an iterative process, and one park location was changed to an area where participants felt more comfortable.
Future iterations of the SEL curriculum will also explore avenues to describe and discuss emotions across languages and cultures. Challenges with interpreting and finding a common language around emotions and idioms used in evaluating psychosocial distress were noted in this pilot and in prior literature (Bernal & Sáez-Santiago, 2006; Cork et al., 2019). This manifested in variable responses when reflecting on discussion of emotions before and after EMPOWER, as shown in Table 2. Thus, future evaluations will explore the concept of emotions through in-depth discussions with interpreters and community members. Finally, many parents discussed the desire to augment the curriculum for themselves and for their children. More opportunities for children to interact with each other and for concurrent parental education can be incorporated into future curricula, especially as COVID-19 safety restrictions are lifted.
There were several limitations to this pilot evaluation. This study, conducted after the EMPOWER curriculum was administered, did not include pretests. The primary aim was to study feasibility and acceptability along with postintervention measurements to inform future effectiveness evaluations. This was also a pilot with a total of 13 families, so it is possible we did not reach thematic saturation in our qualitative analysis. However, the responses did provide guidance for future directions. There is also concern for social desirability bias in this evaluation, but consistent attendance, including attendance at recent “refresher” Zoom sessions during school breaks, provides evidence that parents and children are interested in continued participation. This pilot was performed with a specific refugee group in one community, so future studies with families from other backgrounds are needed to assess generalizability.
Conclusions
In this pilot study, we evaluated the feasibility and acceptability of EMPOWER, an adapted SEL program that included culturally specific, multilingual, trauma-informed wellness and physical education during the COVID-19 pandemic. We found that this adaptation was well-received by Afghan refugee families and that COVID-19 safety measures were well-understood after participation. Challenges emerged around Zoom connectivity and around finding a common language for discussing emotions. Future iterations of the program and evaluations will require continued partnerships with community members and organizations. As we continue and expand EMPOWER, we aim to evaluate short-term improvement in SEL competence as well as long-term mental and behavioral health outcomes for children and their families.
Supplemental Material
sj-docx-1-heb-10.1177_10901981211048830 – Supplemental material for Pilot Wellness Program With Adapted Social–Emotional Learning and COVID-19 Curriculum for Refugee Youth
Supplemental material, sj-docx-1-heb-10.1177_10901981211048830 for Pilot Wellness Program With Adapted Social–Emotional Learning and COVID-19 Curriculum for Refugee Youth by Julia Rosenberg, Patricia McDonough Ryan, Caroline O’Brien, Fereshteh Ganjavi and Mona Sharifi in Health Education & Behavior
Footnotes
Acknowledgements
The authors would like to thank the community partner organizations and leaders who collaborated with EMPOWER: Elena’s Light, Junior Arts and Music, NeighborWorks New Horizons, Integrated Refugee and Immigration Services, Yale Pediatric Refugee Clinic supported by Camille Brown, Yale Health Education and Literacy for Asylees and Refugees, and Yale Patient Navigator Program. They would also like to thank the Pediatric Scholar Program in the Yale Department of Pediatrics for their support of this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Yale Department of Pediatrics Pediatric Scholar Program.
Ethics Approval
The evaluation was deemed exempt by the Yale Institutional Review Board.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.