
Abstract
Introduction
Somali American adolescent tobacco use has increased over the past decade amid a high prevalence of tobacco use among Somali American adults. While established adolescent tobacco use determinants may apply for Somali youth, a deeper understanding of these influences is imperative to the development of effective prevention strategies for this population. This study aimed to identify risk and protective factors influencing Somali American adolescent tobacco use decision making and potential family and community roles in tobacco prevention.
Method
We conducted 15 semistructured, in-depth interviews with 12 Somali and 3 non-Somali professionals serving Minnesotan metropolitan Somali communities in clinical, educational, religious, and other community organizations. Grounded Theory informed our data collection and analysis.
Results
Key informants cited three major influences on Somali adolescent tobacco use: evolving norms and increasing exposure to tobacco products in the United States, low risks perception, especially for waterpipes, and conflicting interpretations of faith. Informants highlighted the important roles of families in Somali youth tobacco prevention while acknowledging areas where families would benefit from greater support. Proposed sources of support included faith communities and nonparental, ethnically similar adult mentors. Informants acknowledged challenges to addressing youth tobacco prevention in clinics and underscored the importance of youth involvement in developing prevention strategies.
Conclusions
Our results indicate Somali adolescent tobacco prevention efforts should address the evolving tobacco use exposures and norms, low risk perceptions, and clarify faith messaging. Effective strategies may include strengthening family-based tobacco prevention approaches that also engage faith and other community leaders along with youth themselves.
Adolescent use of e-cigarettes and waterpipes (also referred to as shisha or hookah), a form of tobacco use originating in the Middle East, South Asia, and other locales with significant Arab influences, has grown in recent years (Cooper et al., 2018; Cullen et al., 2018; Lauterstein et al., 2014). While e-cigarettes may represent a risk-reduction strategy for adult combustible cigarette smokers (Hartmann-Boyce et al., 2016), identified links between adolescent and young adult use of these products and initiation of combustible cigarettes jeopardize the notable progress of youth tobacco prevention initiatives (Barrington-Trimis et al., 2016; Loukas et al., 2017; Salloum et al., 2016). Furthermore, waterpipe use is associated with direct health risks, including cardiopulmonary disease and certain cancers, that overlap with combustible cigarettes (Cobb et al., 2010; Waziry et al., 2017).
Among Somali adolescents in Minnesota, home to the largest Somali diaspora in the United States (Refugee Processing Center, 2021), e-cigarettes and waterpipe use represented the predominant forms of tobacco use in 2016 (Wilhelm et al., 2020), reflecting broader adolescent tobacco use trends (Cooper et al., 2018; Lauterstein et al., 2014). Cigarette (Giuliani et al., 2012) and waterpipe use (Giuliani et al., 2010; Marigi et al., 2013) are also more prevalent among Minnesotan Somali adults (Giuliani et al., 2012) relative to the state’s general adult population (Centers for Disease Control and Prevention, 2011). Female stigmatization of tobacco use likely contributes to underestimates of Somali female tobacco use, yet waterpipes appear to be a popular—and perhaps more culturally accepted—form of Somali female tobacco use (Giuliani et al., 2008; Marigi et al., 2013).
Amid the changing landscape of adolescent tobacco use and the growing U.S. diversity through immigration, elucidating subpopulation tobacco use influences is essential to guide novel prevention efforts (National Cancer Institute Board of Scientific Advisors, 2016). The risk and protective factor paradigm, one approach to conceptualizing adolescent substance use determinants, centers on the premise that reducing adolescents’ risk factors while increasing their protective factors aides in the prevention of adolescent substance use behaviors (Hawkins et al., 1992). This paradigm acknowledges interactions between factors across adolescent spheres of influence (e.g., peers, families, and schools), supporting the need for comprehensive interventions that span ecological domains as described by Bronfenbrenner in his socioecological framework (1994). Adolescent substance use prevention and treatment evidence-based interventions have applied the risk and protective factor paradigm and demonstrated that these methods are amenable to community stakeholder engagement in their design and implementation (Hawkins et al., 2002). Recent applications of the paradigm have been strengthened by inclusion of adolescent cultural and ethnic identity development (Porta et al., 2016; Prado et al., 2009; Rivas-Drake et al., 2014).
Many established risk and protective factors for adolescent tobacco use, such as risk perceptions (Wang et al., 2018) and positive self-identity (Scal et al., 2003), extend to Somali youth (Giuliani et al., 2008, 2010; Pinsker et al., 2017; Wilhelm et al., 2020). Peer and family attitudes and behaviors are also well-established tobacco use determinants for both general adolescent populations (Cooper et al., 2018; Komro et al., 2003; Sargent & Dalton, 2001; Scal et al., 2003) and Somali adolescents (Giuliani et al., 2010; Pinsker et al., 2017; Wilhelm et al., 2020). While Somali youth exposed to peer and/or family tobacco users are more likely to use tobacco (Giuliani et al., 2010; Pinsker et al., 2017), adolescents with higher levels of parental connectedness (Wilhelm et al., 2020), sense of obligation to their parents (Giuliani et al., 2008), and parental antismoking norms (Wilhelm et al., 2020) report lower tobacco use.
Other established sociocultural influences on adolescent tobacco use outside of the traditional risk/protective paradigm, both evolving U.S. societal norms (i.e., the denormalization of cigarette smoking [Kelly et al., 2018]) and those specific to Somali communities (i.e., the stigmatization of tobacco use that is especially severe for females [Giuliani et al., 2008]) collectively shape Somali adolescent tobacco use decisions. Among these, religious faith is an important protective influence on general adolescent population (Gryczynski & Ward, 2011) and other Muslim adolescent tobacco use (Alzyoud et al., 2015), and Somali youth are no exception (Giuliani et al., 2008). However, the protective mechanisms of faith for Somali adolescent tobacco use appear to be driven more by their religious interpretations of the Islamic prohibition of tobacco (Giuliani et al., 2010) than by their regular participation in religious activities, which has been associated with higher levels of waterpipe use (Wilhelm et al., 2020). These seemingly contradictory findings hint at other cultural and social factors that may differentially influence Somali adolescent tobacco use.
Impact Statement
This study provides a deeper understanding of how immigration, culture, and family shape risk and protective factors for tobacco use among Somali American adolescents. Our findings highlight potential influential targets to consider in the development of tobacco prevention approaches for Somali American youth, such as family-based interventions and mentorship, and identify resources at the family and community levels that could support these efforts.
The documented high prevalence of U.S. Somali adult tobacco use (Giuliani et al., 2012) and recent increases in Somali adolescent use of emerging tobacco products (Minnesota State Epidemiological Outcomes Workgroup, 2015; Wilhelm et al., 2020) underscore the importance of clarifying tobacco use determinants for this population. While earlier studies have begun to characterize influences on Somali adolescent tobacco use decision making (Giuliani et al., 2010; Pinsker et al., 2017; Wilhelm et al., 2020), questions remain about how these influences operate for Somali adolescents, particularly the understudied religious and cultural factors.
This study further characterizes influences on Somali adolescent tobacco use in Minnesota through in-depth interviews with professionals serving these youth and their families. We aimed to (1) expand and contextualize the individual, family, and community factors that influence Somali adolescent tobacco use decision making within this large U.S. diaspora and (2) to assess community assets and barriers to Somali adolescent tobacco use prevention efforts. This valuable information will inform the development of culturally rooted tobacco prevention and cessation interventions for Somali adolescents growing up within these communities.
Method
Study Sample and Recruitment
Purposive sampling was used to identify key informants (KIs) for this study, targeting experts serving the Minnesota metropolitan Somali community in clinic, public health, education, religious, and other community organizations. Additional selection criteria included over 18 years of age and English proficiency. Researchers contacted leaders of Somali-serving organizations to formulate a list of potential participants, who were contacted by email or telephone, given information about the study, and invited to participate. KIs received a $40 gift card to compensate them for their time. Of the 24 experts contacted, 15 agreed to participate in the study. The authors’ institutional review board deemed this study exempt from review. We included all components of the Standards for Reporting Qualitative Research checklist when preparing this manuscript (O’Brien et al., 2014).
Data Collection
The lead author (A.W.) conducted fifteen semistructured, in-depth KI interviews in the fall of 2018 and winter of 2019. Each interview occurred in the KI’s workplace or a quiet meeting space of their choosing (e.g., a public library). All interviews took place in English, were approximately 60 minutes in length and were audio-recorded with consent from participants. Basic demographic information was collected, including age, ethnicity, place of birth, duration of time living in the United States, educational attainment, and profession. The guiding domains of each interview included characterization of the KI’s role in the community, the relative priority of Somali adolescent tobacco prevention compared with other issues, factors influencing Somali youth tobacco decision making, and primary community assets and barriers related to adolescent tobacco use and prevention efforts with a particular focus on the parent–child relationship (Supplemental Table 1). Thematic saturation was achieved by the 14th and confirmed in the final interview.
Data Analysis
Interview recordings were transcribed verbatim. Researchers used NVivo 12 software to organize excerpts and to facilitate coding (QSR International Pty Ltd, 2018). Data analysis occurred concurrently with data collection. The lead author reviewed and coded the transcripts using a grounded theory approach described by Charmaz (1996), which comes from a relativist epistiomological paradigm. This approach builds from line-by-line inductive coding to focused coding (to develop higher level categories and iteratively recode data) and finally to theme and subtheme development honed through memo-writing, constant comparative methods, and theoretical sampling in later stages of the analysis and data collection to ensure rich data collection to clarify concepts and to explore gaps in knowledge. Other team members independently co-analyzed a subsample of the data followed by a team review of coding and thematic discrepancies. The team collaborated throughout the analysis to develop a consensus on themes and data interpretation, a process that allowed each researcher to reflect on how their perspectives shaped their framing of the analysis. The lead author shared high level themes with KIs to further contextualize and solidify our findings.
Results
Nine male and six female KIs participated in this study’s in-depth interviews (Table 1). Most informants identified as ethnically Somali (80%), reported foreign birth (86.7%), and had lived in the United States for a substantial period (14–40 years). Informants represented a wide range of ages and professional expertise, many of them through work with multiple professional organizations. All informants had completed college and 53% held graduate degrees in their professional fields.
Key Informant Demographic Characteristics.
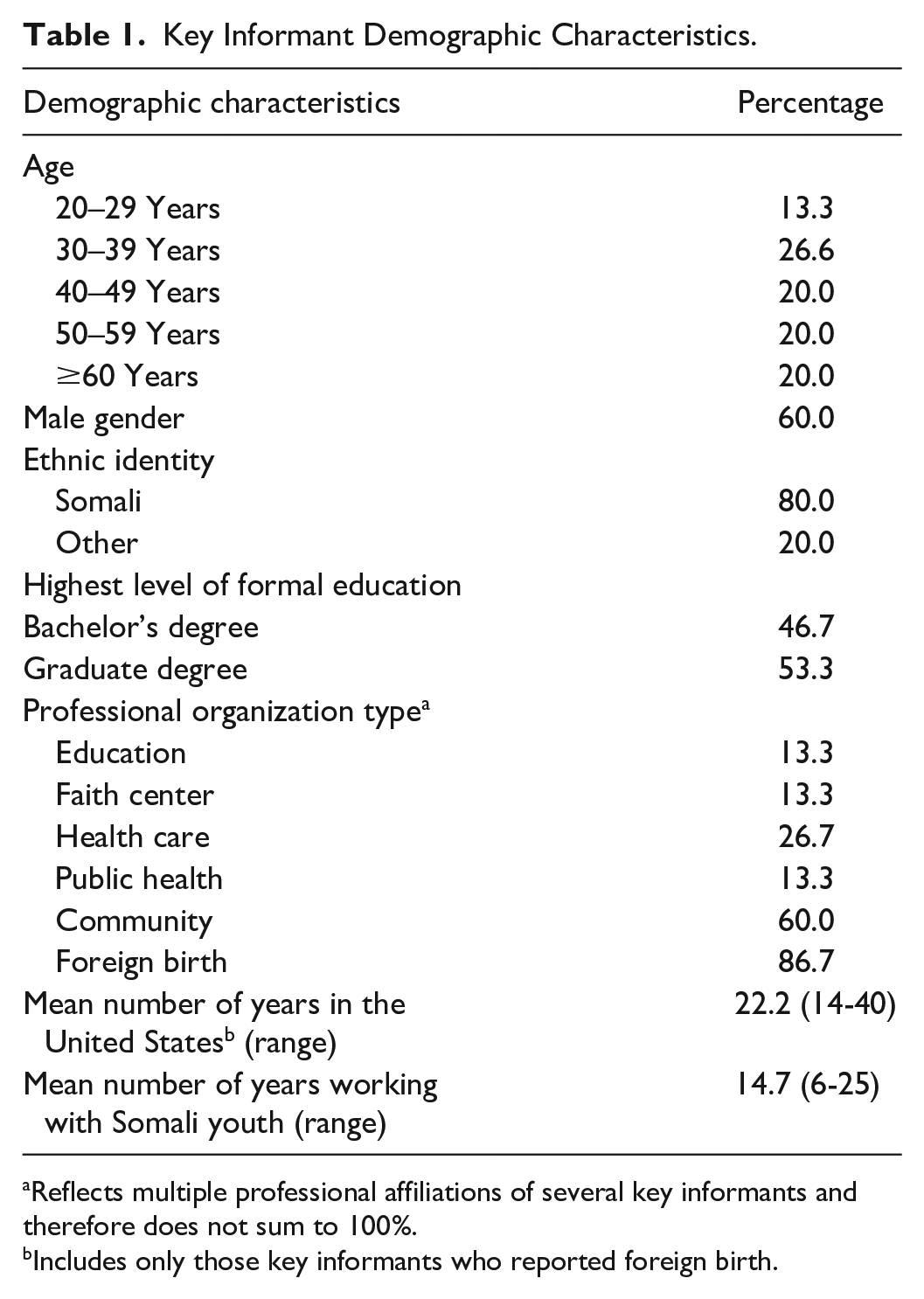
Reflects multiple professional affiliations of several key informants and therefore does not sum to 100%.
Includes only those key informants who reported foreign birth.
Influences on Somali Adolescent Tobacco Use in the United States
Informants uniformly perceived increasing Somali youth tobacco use in the United States, especially waterpipe use (hereafter referred to as shisha), and they agreed that tobacco prevention is an important public health issue for the U.S. Somali diaspora. They noted several contributors to these trends in youth tobacco use that spanned three main themes, which are presented below.
Evolving Norms and Increasing Exposure to Tobacco Products in the United States
Several informants described how tobacco use norms began to change among Somali adults prior to and during the immigration related to the civil war and have continued to evolve in Somalia toward more acceptance of shisha use in particular. As one informant (Education, male, Somali, aged 50–59 years) sums up, “[shisha] was not culturally part of the Somali communities [ . . . ] It’s only [been there] for the last, I can say, 10 or 15 years.” Several other informants tied traditional shisha use only to regions of Somalia bordering Ethiopia and connected increasing shisha use in Somalia to shisha exposure in Ethiopian refugee camps. One informant (Community organization, male, Somali, aged 30–39 years) illustrates this: “they used to see [shisha lounges] back in Ethiopia—the camps that they used to be in—they see this as a hangout spot.” This evolution continued with resettlement to Western countries, where informants perceived tobacco use culture as more permissive and individualistic. As one informant (Education, male, Somali, aged ≥60 years) stated, America is a place where “you cannot limit my freedom.”
While some informants reported that Somali community members disapproved of all tobacco use, and most agreed that tobacco use was not traditional to Somali culture, a majority identified shisha as increasingly accepted and present in U.S. Somali homes. As one informant (Health care, female, Somali, aged 20–29 years) relayed, “women with small children will gather at homes and kind of smoke [shisha] together. [ . . . ] They do it to socialize.” Another informant (Education, male, Somali, aged ≥60 years) captured how youth appear to have internalized this acceptance of shisha: “I asked a group of young girls and boys, ‘why have you guys been smoking?’ And basically they told me that ‘our moms were smoking [shisha] when we were babies.’” Informants shared that the media’s portrayal of shisha use in predominantly Muslim Middle Eastern and South Asian countries contributes to shisha’s perceived acceptability. Somali adolescent shisha experimentation was perceived as taking place in the home, often at “shisha parties” during school hours or immediately following when parents are not around to supervise. Several informants also described shisha lounges as attractive alternatives to alcohol-focused bar culture for Somali young people to socialize: When people who are maybe in their [twenties] can’t say, ‘Let’s go drink,’ what they can say is, “Let’s go Shisha lounge.” [ . . . ] I went to one a while ago; it was a really fancy place, very beautiful, nice sofas [ . . . ] It’s where young people would say, “Oh, it’s a place to chill” . . . (Community organization, male, Somali, aged 30–39 years)
Low Perceptions of Risks of Tobacco Use, Especially Shisha
Informants described that while the community has a growing awareness of tobacco-related risks of smoking, there were gaps in knowledge about the shisha risks. Informants reported that most Somali shisha users, adolescents and adults alike, believe that shisha is less detrimental to their health than other tobacco products, which several informants attributed to misleading tobacco industry advertising and the ubiquitous use of shisha. Perceptions of shisha as a healthier alternative to cigarettes stemmed from shisha’s fruit content, the belief that water filtration of the shisha removed harmful chemicals, and general confusion about whether shisha contained tobacco. One informant (Community organization, male, Somali, aged 30–39 years) explains: “People know that vegetables and fruits are healthy things, so when they hear that, ‘Oh, this is made from apples’ they believe that, ‘Oh, it has to be healthy.’”
Faith Influences on Tobacco Use
Varied interpretations of Islamic perspectives on tobacco use were described as shaping Somali adolescent tobacco use. Several informants noted the “borderline” Islamic classification of tobacco use—since it is not expressly haram (prohibited by Islamic law) nor accepted—as contributing to perceptions among Muslims that tobacco use is more acceptable than other substances. However, most informants described that tobacco use conflicts with key Islamic tenets, including the mandate for Muslims not to harm themselves, which includes their mental and spiritual wellbeing beyond the physical body. Informants generally agreed that faith and connection to their mosque protected Somali youth from engaging in risk behaviors like tobacco use and described mosques as places where adolescents are surrounded by positive peer influences and build relationships that can strengthen their sense of identity.
However, informants reported that some youth, particularly those already involved in risk behaviors, may not feel connected to mosques or participate regularly in mosque activities. Generational and cultural differences in expectations between adolescents and Imams may contribute to this disconnect. One informant (Public health, female, Somali, aged 40–49 years) shared how even adolescents who attend the mosque often feel unable to open up to their faith leaders about certain topics because Imams are [the] older generation [ . . . ] so how do you create a space that is very welcoming? [ . . . ] that’s what all the teen that I talked to told me it’s not [ . . . ] there isn’t that safe space for them to really explore who they are.
Furthermore, informants discussed how Somali adolescents may not perceive religion as relevant to their lived experiences. Blanket mandates from family and religious leaders on avoiding tobacco use may therefore fall flat for these adolescents, especially when influential adults don’t help them to connect their behavioral choices with future consequences: We are told, you know, “Don’t touch that bottle.” But I don’t give you the reasoning and don’t explain to you [ . . . ] It’s kind of like telling a 2-year-old, “don’t touch the hot oven.” It’s like, okay, I’m going to put my hand in there to see what would happen. (Community organization, female, Somali, aged 30–39 years)
This informant echoed others in sharing opportunities to make religious doctrines more relatable to help youth understand how their faith can enrich and guide their decisions.
Community Roles and Resources for Somali Adolescent Tobacco Prevention
Informants noted the important role of community organizations in previous Somali adolescent tobacco prevention efforts while also underscoring the need for ongoing, sustainable funding and culturally and linguistically adapted approaches. Here we discuss the different roles and resources that they identified.
Families Play Important Roles in Tobacco Prevention but Would Benefit From Further Support
Informants stated that strengthening parents’ abilities to address tobacco use with their children is an important tobacco prevention target. However, informants shared examples of Somali parents who felt unprepared to speak to their adolescent children about tobacco use due to their own knowledge limitations, particularly in the realm of shisha and newer tobacco products like e-cigarettes—products that may be easier for young people to hide. Parents also may be wary of addressing a stigmatized subject that could stimulate their child’s interest in tobacco experimentation. Educating parents about tobacco influences and how to navigate conversations on tobacco with their children struck informants as important areas for strengthening parental roles in tobacco prevention. Several informants described the importance of parental openness to seeing things from their children’s perspectives to facilitate effective conversations on tobacco use and other sensitive topics.
Faith Communities Provide Important Support in Tobacco Prevention Efforts
Informants identified faith communities and leaders as trusted sources of support for Somali parents and families for tobacco prevention. Informants described mosques as one of few culturally relevant locations where parents, especially mothers, come together to socialize and share information. Additionally, informants detailed how Somali parents often rely on imams for advice on family issues and to provide moral guidance for their children through Islamic education. Due to their connections and influence, imams were seen as instrumental in disseminating important messages. Informants discussed how working closely with imams could strengthen an intervention both in terms of informing its design through co-creation and in expanding its reach through their Friday sermons and outreach.
When, say, an Imam or faith leader and their doctor kind of sit side by side [ . . . ] and the Imam kind of use the why the faith came to this world. The faith came here to the benefit of the human being, whether it be soul or mind or body, [ . . . ] to encourage the people to listen and accept it for the guide coming from the professionals. [ . . . ] If they see that the Imam or the faith leader can work together side by side, I think the community will trust. (Faith center, male, Somali, aged 50–59 years)
Connecting With Mentors May Help Support Youth in Navigating Tobacco Use Decisions
Informants discussed how forging connections with mentors through after-school programming positively shapes adolescents’ exposures and reduces their risk of engaging in tobacco use. Positive connections with nonparental role models provide a safe space for Somali adolescents to discuss topics that they don’t feel comfortable bringing up with their parents: [They] come to me and ask me a lot of questions related to maybe tobacco, related to sexual activity [ . . . ] Young people also, they have a lot of different needs, but a place they can, for example, feel safe. They can feel respected, they can feel also guided. (Faith center, male, Somali, aged 50–59 years)
Young adult role models who share Somali adolescents’ cultural background were described as well positioned to support adolescents in navigating decisions related to risk behaviors like tobacco use because they understand the multicultural immigrant experience and are perceived as relatable and less judgmental. Conversely, informants reported that it’s when youth are not plugged into opportunities to build connections that they become more likely to engage in risky behaviors. Most informants felt that investments in culturally tailored after-school programs would increase Somali youth engagement in positive opportunities.
Opportunities for Clinics and Health Care Providers to Strengthen Their Tobacco Prevention Approaches
Informants discussed the roles that clinicians might play in addressing tobacco prevention. However, all clinician informants shared potential challenges in addressing Somali youth tobacco prevention in traditional clinical settings. For example, several informants cited uncertainty about the extent and types of tobacco use among Somali adolescent patients. One informant (Health care, female, non-Somali, aged 30–39 years) attributed this to Somali youth being reluctant to respond truthfully to provider inquiries about tobacco use out of concerns for provider judgment or breaches of confidentiality: “Often times they seem surprised. ‘No, of course not. Why are you asking me? I’m Muslim; of course, I don’t drink alcohol.’” Additionally, informants shared Somali parents’ strong cultural value of family-based health and a suspicion of the potential topics to be raised as contributing to their reluctance for providers to engage in confidential conversations with their adolescent children. This limited opportunities for providers to talk with adolescents about tobacco use without undermining the trust and relationship with their parents. In some instances, clinicians reported that they found themselves responding by not asking targeted tobacco use questions with their Somali adolescent patients.
Prevention Efforts Should Engage Youth
Finally, multiple informants shared examples of youth leadership during previous prevention campaigns and discussed how peers can help forge positive connections within families, faith communities, and schools. Informants discussed specific ways that youth could engage one another to raise awareness of tobacco use risks, including through youth ambassador programs within community organizations and at large events like weddings or cultural celebrations. Several informants expressed that youth should also be at the table guiding intervention design to increase the relevance and reach of tobacco prevention approaches.
Discussion
This qualitative study with professionals serving Somali youth and families highlights three major influences on Somali adolescent tobacco use and provides suggestions for how community resources may support culturally specific tobacco use prevention efforts for these young people.
First, we found that evolving tobacco use norms within the U.S. Somali diaspora, more permissive American tobacco norms, and increasing tobacco product exposure, particularly shisha use within the home environment—may increase the likelihood of Somali adolescent tobacco use. Though data on tobacco use are scant in Somalia (World Health Organization, 2021), previous qualitative research has suggested a similar influence of country-of-origin patterns of tobacco use shaping behaviors among immigrant youth (Hammal et al., 2016). Given that family members often introduce adolescents to shisha (Akl et al., 2015), the normalization and increased shisha use in Somali family homes (Giuliani et al., 2010; Pinsker et al., 2017) is troublesome. While our findings support prior descriptions of shisha as not traditional within Somali culture (Marigi et al., 2013), our informants identified shisha use as a culturally acceptable alternative to the alcohol-focused U.S. bar culture as described in other North American immigrant populations (Hammal et al., 2016).
Second, our findings reinforce prior studies indicating that lower harm perceptions of shisha among Somali adults and young people may increase adolescent tobacco use (Giuliani et al., 2010; Pinsker et al., 2017). Knowledge limitations of the risks of shisha use, including uncertainty about whether shisha contains tobacco and potential health benefits related to shisha’s fruit content (Akl et al., 2015), have been linked to higher levels of shisha use in other immigrant (Hammal et al., 2016) and general adolescent populations (Wang et al., 2018).
Finally, while there is a protective influence of mosque participation on Somali adolescent tobacco use, we found that Somali youth may also experience a lack of connection to their faith communities. As with other adolescents (Alzyoud et al., 2015; Islam & Johnson, 2003; Steinman & Zimmerman, 2004), religiosity (Giuliani et al., 2008, 2010), and more particularly a strengthened sense of spirituality and identity as Somalis and Muslims (Ellison, 2001), are generally protective against Somali adolescent tobacco use. However, a previously demonstrated positive association between regular religious participation and shisha use (Wilhelm et al., 2020) suggests that faith community membership alone may not be driving the protective effect of religiosity on Somali adolescent tobacco. Rather, positive peer influences developed when participating in mosque activities may help discourage substance use, reflecting the protective effects of prosocial peer influences on adolescent substance use in other communities (Hodge et al., 2001; Steinman & Zimmerman, 2004).
Our findings echo the wider adolescent literature and previous studies of Somali adolescents that suggest that parents significantly influence the tobacco use outcomes of their adolescent children through establishing clear antitobacco norms and expectations (Giuliani et al., 2008; Komro et al., 2003; Sargent & Dalton, 2001; Wilhelm et al., 2020) and building supportive relationships that foster open communication (Scal et al., 2003; Wilhelm et al., 2020). Although Somali adolescents raised within close-knit families with strong cultural norms and ties appear to have lower tobacco use intentions (Giuliani et al., 2010), we found that most Somali parents would benefit from support in preparing for more explicit conversations about tobacco use. Furthermore, barriers related to Somali parents’ knowledge may contribute to their unfamiliarity with tobacco use risks of specific products (Bowie et al., 2017; Scuglik & Alarcon, 2005), which can limit parental effectiveness in establishing boundaries for and overseeing risk behaviors like tobacco use among their adolescent children. Our findings suggest that strengthening Somali parental confidence and skills in parenting their adolescent children through formal parenting support programs may be effective in reducing Somali adolescent tobacco use as it has been shown to be for Somali (Osman et al., 2017) and other immigrant parent groups (Guillermo Prado et al., 2009; Martinez & Eddy, 2005) that aimed to improve mental health and to reduce adolescent risk behaviors. Given the high levels of Somali adult tobacco use and the normalization of shisha use in the home environment, Somali adolescent tobacco prevention interventions would also likely be strengthened by addressing parental tobacco use.
In addition to parent-focused resources, our results point to other potential community resources to support Somali adolescent tobacco prevention efforts. Our study demonstrates how faith center and leadership collaboration within tobacco prevention intervention design and implementation could serve to strengthen Somali youth tobacco prevention interventions, by increasing their relevance and reach as seen in previous faith and public health partnerships (Pratt et al., 2017, 2020). However, given generational differences between imams and adolescents noted in our study and the perception that not all adolescents are connected to a faith community, younger adult mentors with shared cultural heritage (Bridging Refugee Youth and Children’s Services, 2009) in community organizations or other nonfaith-based cultural centers with strengths-based extracurricular activity participation may be better positioned to deliver tobacco prevention messages to a wider population of Somali adolescents. Previous studies demonstrating the power of clinician partnerships with adolescents and their families to reduce health risk behaviors, especially partnerships with culturally congruent clinicians or community health workers (Svetaz et al., 2014), may also fit well with Somali parents’ preference for family-based approaches. Improving communication and clarifying expectations related to adolescent confidentiality using family-friendly approaches (Hutchinson & Stafford, 2005; Svetaz et al., 2016) could further augment patient–provider and provider–parent trust and strengthen clinician roles in addressing tobacco use in this population. Finally, our findings underscore the roles that youth can and should play in developing and disseminating tobacco prevention efforts, reflecting the success of previous youth-engaged approaches to tobacco prevention in the Somali community (Pinsker et al., 2017).
Limitations
These findings expand on the major influences on Somali adolescent tobacco use and potential community resources for tobacco use prevention. However, this study has several important limitations. First, it represents a small convenience sample of highly educated KIs with interest in this topic and therefore is subject to sampling bias. Collecting data from our KIs in face-to-face interviews with one researcher who is also a clinician may have contributed to bias. While most informants identified as Somali and many were parents, future research should directly assess Somali parent and youth perspectives on tobacco prevention and control using multiple data collection methods to further examine cultural and immigration influences. Additional exploration of how gender roles and the interaction between gender and religious and cultural factors shapes Somali adolescent tobacco use is also important to informing future intervention development. Finally, findings within this sample in one urban geographic area may not generalize to the greater Somali diaspora.
Conclusions
This study deepens our understanding of individual, family, and community level influences on Somali adolescent tobacco use decision making within the Minnesota Somali diaspora and identifies potential community resources for tobacco prevention for this population. Our findings highlight the influences of immigration, culture, and family in shaping young people’s tobacco use within this community and illuminate the importance of culturally rooted tobacco prevention interventions that incorporate these influences.
Supplemental Material
sj-docx-1-heb-10.1177_10901981211052892 – Supplemental material for Key Informant Perspectives on Somali Adolescent Tobacco Use: Contextualizing Influences and Prevention Opportunities
Supplemental material, sj-docx-1-heb-10.1177_10901981211052892 for Key Informant Perspectives on Somali Adolescent Tobacco Use: Contextualizing Influences and Prevention Opportunities by April K. Wilhelm, Rebekah J. Pratt and Michele L. Allen in Health Education & Behavior
Footnotes
Acknowledgements
The authors wish to acknowledge the key informants and other community members who assisted in recruitment for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through funds from the Joanna Simer Research Fellowship from the University of Minnesota Department of Pediatrics, Division of General Pediatrics and Adolescent Health. Dr. Wilhelm’s role on the project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under National Research Service Award in Primary Medical Care grant number T32HP22239 (PI: Borowsky), Bureau of Health Workforce. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the U.S. Government.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.