
Abstract
Purpose:
This exploratory study aimed to compare the surgical outcomes of ultrasonic dissection and monopolar electrocautery in single-incision laparoscopic totally extraperitoneal repair (SILS-TEP) for inguinal hernia.
Methods:
A single-center exploratory randomized controlled trial was conducted between July 2022 and December 2023, enrolling 62 patients with unilateral inguinal hernias. Patients were randomized to undergo SILS-TEP using ultrasonic dissection (U group, n = 30) or monopolar electrocautery (E group, n = 32). The primary outcome was the completion rate of SILS-TEP. Secondary outcomes included the intraoperative complication rate, operative time, blood loss, and postoperative complication rate.
Results:
Patient characteristics were similar, except for a higher proportion of right-sided hernias in the U group (66.7% versus 31.3%, P = .010). Completion rates were comparable (96.7% versus 96.9%, P = 1.00). Operative time (60 [interquartile range {IQR} 53.5–71.5] minutes versus 62.5 [IQR: 51–74.5] minutes, P = .72) and blood loss were also similar. Lens cleaning was more frequently required in the U group (4 [IQR: 2.5–5] times versus 1 [IQR: 1–4] time, P = .025). Intraoperative and postoperative complications, length of postoperative hospital stay, and recurrence rates showed no notable differences.
Conclusion:
In this exploratory analysis, monopolar electrocautery in SILS-TEP showed comparable surgical outcomes to ultrasonic dissection. Larger confirmatory studies are warranted to validate these findings. (UMIN000057091).
Keywords
Introduction
Inguinal hernia is one of the most common surgical conditions in Japan, and approximately half of the surgeries are performed endoscopically. 1 Totally extraperitoneal repair (TEP) is a standard laparoscopic procedure, along with the transabdominal preperitoneal (TAPP) approach. In our hospital, single-incision laparoscopic surgery for totally extraperitoneal repair (SILS-TEP) has been the standard approach for adult inguinal hernia since January 2011.2–4
We commonly performed ultrasonic dissection in SILS-TEP. This technique demonstrates excellent vessel-sealing capacity and effectively minimizes thermal damage to the surrounding tissues. However, ultrasonic energy devices cut and coagulate tissue through high-frequency vibrations, generating fine aerosols via cavitation. These aerosols can contaminate the laparoscopic lens and reduce visibility during surgery.5,6 In contrast, monopolar electrocautery is more cost-effective and generates fewer aerosols, although it has a lower vessel-sealing capacity and greater thermal spread to the surrounding tissues.
No previous studies have compared the surgical outcomes of these energy devices for TEP procedures. Therefore, we conducted this exploratory randomized controlled trial to evaluate whether monopolar electrocautery is non-inferior to ultrasonic dissection in terms of surgical feasibility. We hypothesized that monopolar electrocautery would achieve comparable technical performance and perioperative outcomes to ultrasonic dissection, while potentially offering advantages in instrument availability and broader applicability in surgical practice.
Materials and Methods
Study design
This was a single-center, exploratory randomized controlled trial comparing the surgical outcomes of ultrasonic dissection and monopolar electrocautery in SILS-TEP. This study was registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN000057091) and was approved by the Institutional Review Board of Osaka Keisatsu Hospital (No. 1526). The study conformed to the provisions of the Declaration of Helsinki. Informed consent was obtained from all the patients.
Patient enrollment
Patients with inguinal hernia were enrolled between July 2022 and December 2023. The eligibility criteria are as follows: (a) age ≥20 years, (b) unilateral inguinal hernia, (c) initial hernia, and (d) scheduled for elective SILS-TEP surgery. The exclusion criteria were as follows: (a) unsuitability for laparoscopic inguinal hernia repair, (b) bilateral inguinal hernia, (c) recurrent hernia, and (d) giant inguinoscrotal hernia (defined as a hernia extending below the midpoint of the inner thigh when the patient was in the standing position.). 7 To eliminate differences in surgical outcomes among the operators, the surgeons were limited to 2 individuals experienced in SILS-TEP, each of whom had performed more than 300 SILS-TEP procedures (Y.N. and K.I.).
Randomization
Sixty-two patients were enrolled into the study. The CONSORT diagram is shown in Figure 1. Patients were randomly allocated to either the U group which underwent SILS-TEP with ultrasonic dissection, or the E group, which underwent SILS-TEP with monopolar electrocautery. Simple randomization was performed using a computer-generated random sequence created with Microsoft Excel, with no allocation factors applied to the randomization process. Thirty patients were assigned to the U group, and 32 patients were assigned to the E group.
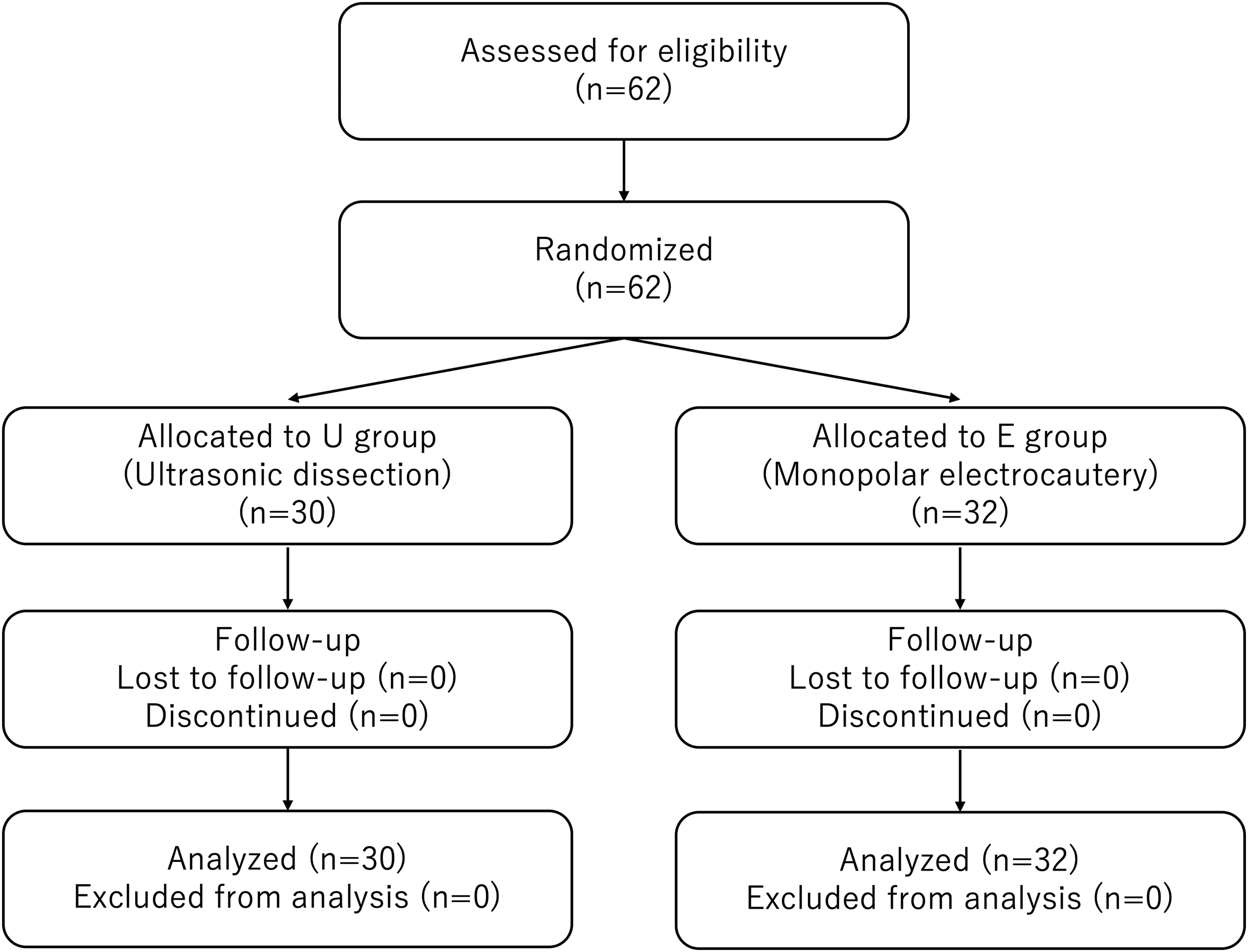
CONSORT diagram of the study.
Operative procedure
The SILS-TEP method for inguinal hernia repair was standardized in our hospital, as previously described.2,3 Under general anesthesia, the patient was placed supine with both arms adducted, then positioned in the Trendelenburg position with the contralateral side tilted down. A single, 25-mm, intraumbilical incision was made, and the subcutaneous tissue was dissected to the rectus abdominis sheath. After opening the anterior sheath, blunt dissection using a finger or gauze created an initial preperitoneal space. The remainder of the dissection was conducted using energy devices (ultrasonic dissection or monopolar electrocautery) according to group allocation. After placing the Lap-Protector Mini (Hakko Co., Nagano, Japan) in this space, three 5-mm trocars (one for the 5-mm flexible scope and two for surgical devices) were inserted through a single-port access device (EZ Access; Hakko Co.). The preperitoneal space was dissected using an energy device (ultrasonic dissection or monopolar electrocautery), without a dissection balloon. A polypropylene mesh was placed in this preperitoneal space, covering the inguinal floor. The preperitoneal space was carefully deflated to avoid displacing the mesh. The anterior rectus sheath was closed with a 2-0 Vicryl suture, and the skin was closed with a 3-0 Maxon suture.
In the U group, either Harmonic ACE® +7 (Ethicon Endo-Surgery Inc., Cincinnati, OH, USA) or SonoSurg® (Olympus USA, Center, Valley, PA, USA) was used according to the availability of the generators. Harmonic ACE® +7 was used in 17 cases, while SonoSurg® was used in 13 cases.
In the E group, Metzenbaum scissors and Maryland dissectors (KARL STORZ GmbH and Co. KG, Tuttlingen, Germany) equipped with a monopolar electrical cable were used. Monopolar electrocautery was mainly used in the coagulation mode with intermittent use of the cutting mode for tissue division. The surgical forceps used were common between the two groups.
A 3D MAXTM mesh (standard type; Bard, Inc., New Providence, NJ, USA) was mainly used. Mesh fixation was basically not performed. A ProGripTM laparoscopic self-fixating mesh (Medtronic, Dublin, Ireland) was used in the cases of L3 hernia or direct hernia, as classified by the European Hernia Society (EHS) Groin Hernia Classification. 8
Study outcomes
The primary endpoint was the completion of SILS-TEP, chosen as an objective and reproducible indicator of technical feasibility. This allowed unbiased comparison between devices and generation of preliminary data to guide future studies, including those involving trainees. The secondary endpoints were intraoperative complication rate, operative time, blood loss, postoperative complication rate and additional costs associated with the energy devices used. Patient age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) score, history of abdominal surgery, hernia site and type, operative time, blood loss, number of times the laparoscopic lens was cleaned, conversion to a different procedure, intraoperative complications, length of postoperative hospital stay, follow-up duration, and postoperative complications were recorded.
Statistical analysis
Variables are shown as the number (and percentage) of patients or as the median (and interquartile range) value. All statistical analyses were performed using JMP statistical software version 17.0.0 (SAS Institute, Cary, NC, USA). Student’s t-test was used for continuous parametric data, while the Mann–Whitney U test was applied to non-parametric data. Fisher’s exact test was used for categorical variables. P-values were interpreted descriptively due to the exploratory nature of the study.
In this exploratory study, the sample size was determined primarily based on practical considerations, including the feasible study period and the expected number of eligible patients at our institution. Although the sample size was relatively small (approximately 30 cases per group, totaling 62 cases), it was considered sufficient to provide preliminary insights into the impact of energy device selection on surgical outcomes in SILS-TEP. This study was not powered to detect small differences between groups.
Results
Table 1 shows the characteristics of the patients in each group. No statistically significant differences were observed between the groups with regard to patient age, sex, BMI, ASA score, history of abdominal surgery, and hernia type. Two patients in the U group had combined hernias (direct + indirect hernia and indirect + femoral hernia). One patient in the E group had a femoral hernia. A higher proportion of right-sided inguinal hernias was observed in the U group compared to the E group (66.7% versus 31.3%, P = .010).
Clinical Characteristics of the Patients and Inguinal Hernias
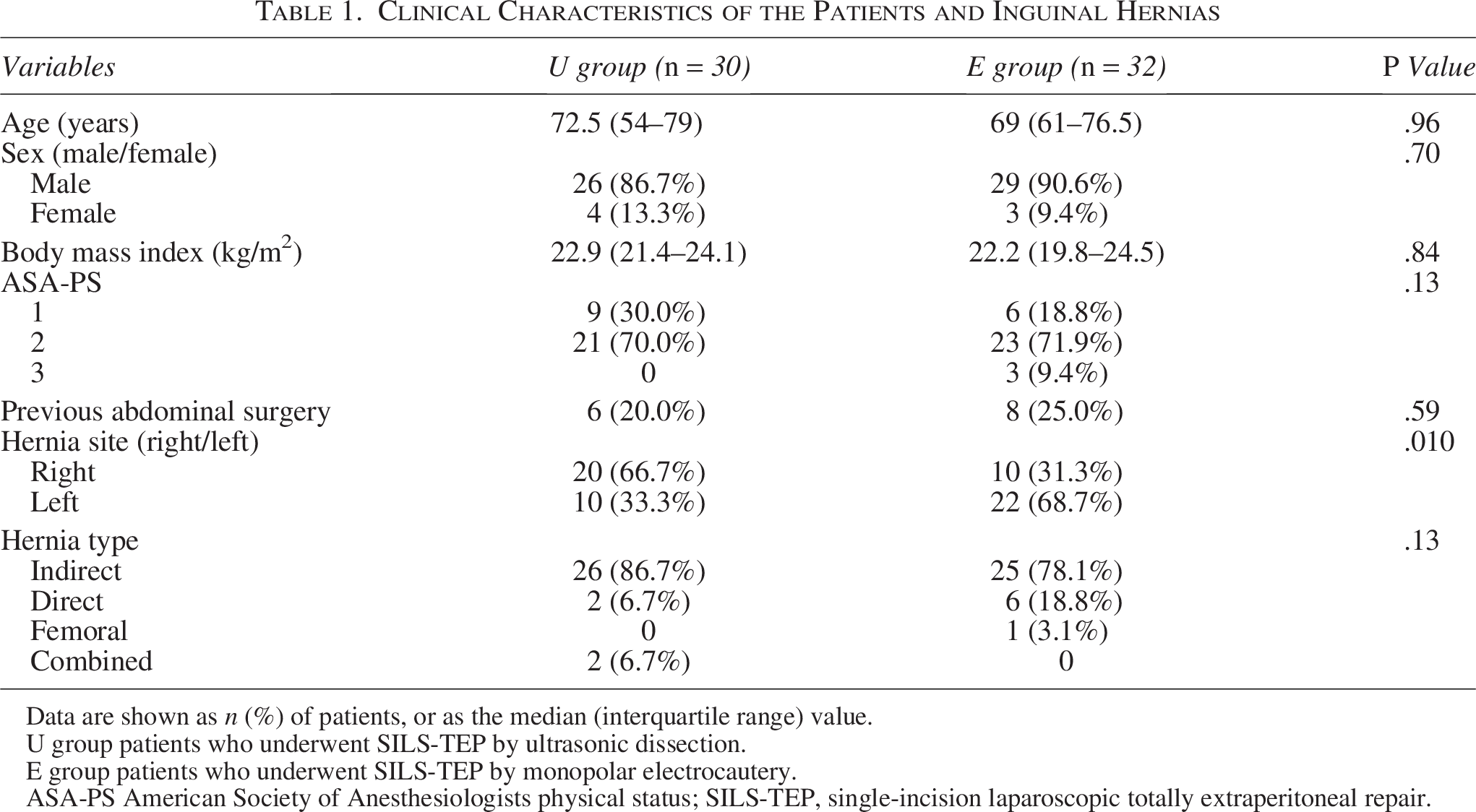
Data are shown as n (%) of patients, or as the median (interquartile range) value.
U group patients who underwent SILS-TEP by ultrasonic dissection.
E group patients who underwent SILS-TEP by monopolar electrocautery.
ASA-PS American Society of Anesthesiologists physical status; SILS-TEP, single-incision laparoscopic totally extraperitoneal repair.
The perioperative variables and complications are shown in Table 2. The completion rate was 96.7% (29/30) in the U group and 96.9% (31/32) in the E group (P = 1.00). The operative time was 60 (53.5–71.5) in the U group and 62.5 (51–74.5) minutes in the E group (P = .72). The intraoperative blood loss was minimal in both groups. The laparoscopic lens trended to be cleaned more frequently in the U group than in the E group (4 [2.5–5] times versus 1 [1–4] time, P = .025).
Intraoperative and Postoperative Data
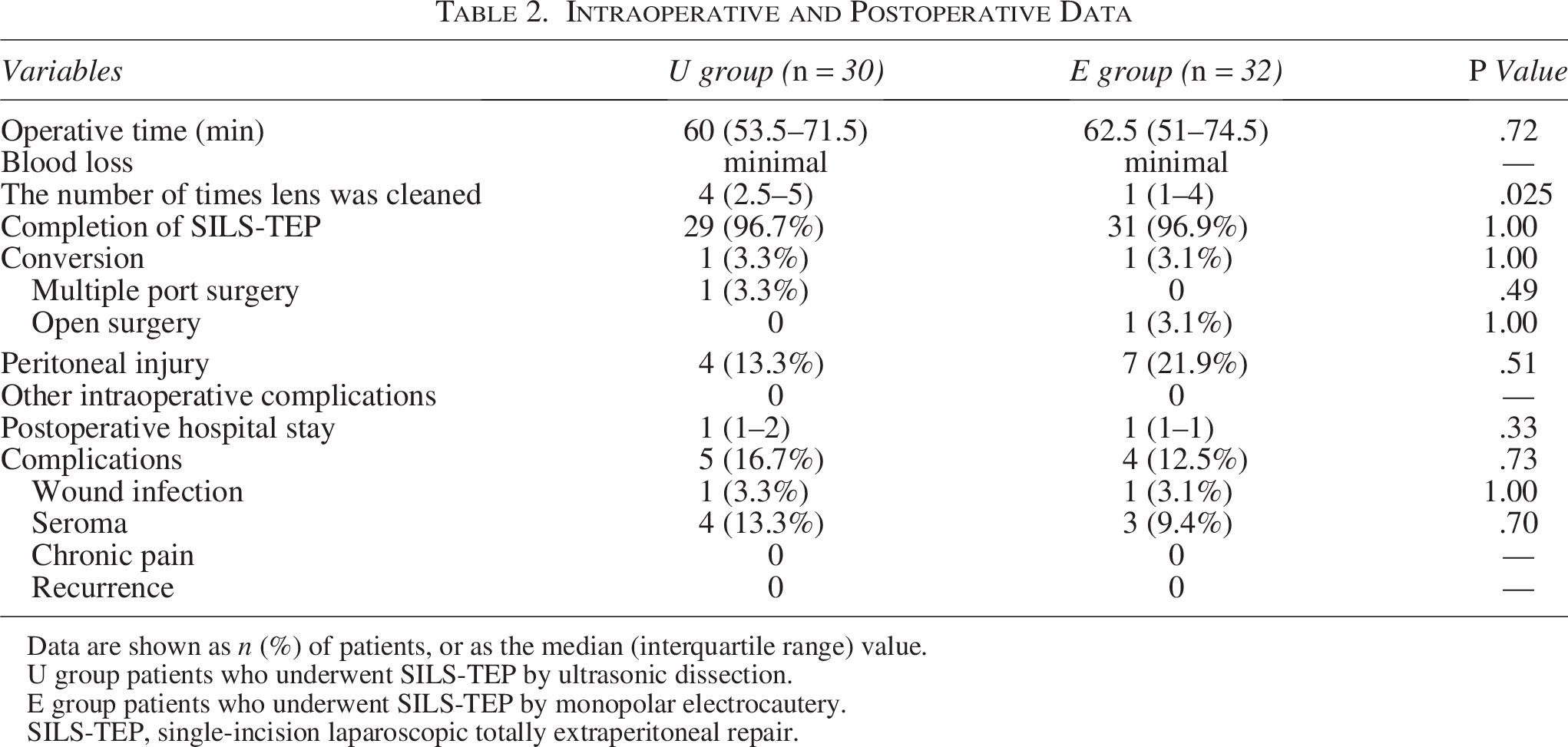
Data are shown as n (%) of patients, or as the median (interquartile range) value.
U group patients who underwent SILS-TEP by ultrasonic dissection.
E group patients who underwent SILS-TEP by monopolar electrocautery.
SILS-TEP, single-incision laparoscopic totally extraperitoneal repair.
Conversion to a different procedure was performed in 2 patients in both groups. One patient in the U group required multi-port TEP. The reason for conversion was peritoneal injury caused by adhesion of the preperitoneal space due to a previous history of laparoscopic rectal cancer surgery. One patient in the E group required conversion to open surgery. The reason for conversion was the very strong adhesion in the midline of the preperitoneal space due to a previous history of SILS-TEP for inguinal hernia on the opposite side. The frequency of peritoneal injury was 13.3% in the U group and 21.9% in the E group (P = .51). No intraoperative complications were observed in either group. Postoperative hospital stay was 1 (1–2) day in the U group and 1 (1–1) day in the E group (P = .33).
The median follow-up duration of all the patients was 6.6 (3.2–13.0) months: 6.2 (3.2–13.0) months in the U group and 10.1 months in the E group (range: 3.2–13.2 months). Postoperative complications occurred in 16.7% (5/30) of the patients in the U group and in 12.5% (4/32) of those in the E group (P = .73). Wound infection was observed in 1 patient in each group (P = 1.00). A seroma was observed in 13.3% (4/30) of the patients in the U group and in 9.4% (3/32) of those in the E group (P = .70). One patient in the E group required a one-time puncture for a seroma. In the other cases, the seromas were managed conservatively. No chronic pain was observed in either group. No other complications, including mesh infections, hematomas, incisional hernia of the umbilical wound, or other organ injuries, were observed during the follow-up period in either group. No recurrence was observed in either group.
Regarding device costs, the additional cost of surgical devices was incurred in the U group: SonoSurg® (198,000 JPY, amortized over 20 cases, resulting in 9,900 JPY per case) and Harmonic ACE®+7 (89,000 JPY, disposable). Considering the proportion of cases using each device (Harmonic ACE®: 17 cases, SonoSurg®: 13 cases), the average cost per case in the U group was approximately 27,966 JPY. In contrast, monopolar electrocautery did not incur any additional device costs.
Discussion
This exploratory randomized controlled trial compared the surgical outcomes of ultrasonic dissection and monopolar electrocautery in SILS-TEP of adult inguinal hernias. To the best of our knowledge, this is the first prospective study to evaluate and compare these two energy devices in a SILS-TEP setting, providing a preliminary addition to the existing literature on laparoscopic hernia repair.
Our findings suggest that both ultrasonic dissection and monopolar electrocautery techniques result in comparable surgical outcomes in terms of operative time, intraoperative complications, and postoperative recovery. However, given the limited sample size and exploratory nature of this study, these findings should be interpreted with caution.
One retrospective study reported on the comparison of ultrasonic energy devices and monopolar energy devices in TAPP. 9 The study found no significant differences in surgical outcomes other than operative time between ultrasonic dissection and monopolar electrocautery. The authors reported that the operative time was significantly shorter for monopolar electrocautery than for ultrasonic dissection. However, because monopolar electrocautery was introduced after the period of ultrasonic dissection, the learning curve likely had a substantial influence on the results.
In our study, the proportion of right-sided hernias was higher in the U group (66.7% versus 31.3%, P = .010). However, in both groups, surgical outcomes—including completion rate, operative time, blood loss, lens cleaning frequency, and complications—showed no significant differences between right- and left-sided hernias (data not shown). These findings suggest that hernia laterality does not substantially affect surgical performance or outcomes in SILS-TEP.
A unique observation of our study was the higher frequency of laparoscopic lens cleaning required for ultrasonic dissection. In our technique, dissection of the preperitoneal space was mainly performed using energy devices. The TEP procedure is conducted within a restricted anatomical area,10,11 resulting in a confined working environment and a short distance between the laparoscopic camera and the surgical field. Ultrasonic dissection generates fine aerosols via cavitation, which leads to more frequent cleaning of the laparoscopic lens.
Although not statistically significant, peritoneal injury occurred more frequently with monopolar electrocautery than with ultrasonic dissection (21.9% versus 13.3%). We used monopolar electrocautery mainly in the coagulation mode, with limited use of the cutting mode. This trend might be attributed to the broader heat dispersion characteristics of monopolar electrocautery. A wider thermal spread can potentially lead to unintended thermal damage to adjacent tissues,12,13 including the peritoneum. In contrast, ultrasonic dissection generates more localized thermal effects, potentially explaining the lower incidence of peritoneal injury.
Monopolar electrocautery is a financially advantageous alternative to ultrasonic dissection, particularly in settings where cost constraints are a significant consideration. In this exploratory study, monopolar electrocautery achieved comparable surgical outcomes without compromising safety or efficiency, while avoiding additional device costs. Although ultrasonic devices offer precise dissection and minimal thermal spread, their high procurement and maintenance costs are a limitation. However, a formal cost comparison was not included in the statistical analysis because two different ultrasonic systems (Harmonic ACE® +7 and SonoSurg®) were used in the ultrasonic group, making direct cost evaluation inappropriate. These preliminary findings suggest that monopolar electrocautery could be a viable option for SILS-TEP procedures in resource-conscious environments.
This study has several limitations inherent to its exploratory design. First, the sample size of 62 patients was determined based on feasibility within the study period. While a larger sample size would provide greater statistical power, conducting a large-scale RCT is impractical in our setting. Consequently, this study was not powered to detect small between-group differences, and all results should be interpreted descriptively. Second, because this was a single-center study, the generalizability of the findings to other clinical settings may have been limited. Finally, the short follow-up period limits conclusions regarding long-term outcomes, such as recurrence rates and chronic pain. Future multicenter studies with larger sample sizes and extended follow-up periods are required to confirm and expand upon these preliminary observations.
Conclusion
This exploratory randomized controlled trial suggests that monopolar electrocautery in SILS-TEP may achieve surgical outcomes comparable to those of ultrasonic dissection. Given the cost-effectiveness and accessibility of electrical devices, they may serve as a viable option in resource-conscious settings. These findings provide valuable preliminary insights that may inform the design of future large-scale, confirmatory trials. Further multicenter studies with larger sample sizes and longer follow-up are warranted to validate and expand upon these observations.
Authors’ Contributions
Y.N. designed the study, performed data collection and analysis, and drafted the article. K.I. performed data collection and analysis. S.T., M.P., T.O., H.T., and T.A. contributed to data analysis. C.M., T.O., K.N., and I.T. provided critical supervision and advice. T.M. designed the study and provided critical supervision and advice. All authors reviewed and revised the article and approved the final version.
Footnotes
Acknowledgments
The authors express gratitude to their colleagues, including surgical staff and nursing teams at Osaka Keisatsu Hospital, for their invaluable support in patient care and data collection.
Funding Information
No funding was received for this article.
Disclosure Statement
No competing financial interests exist.