
Abstract
Background:
This study reports our 5-year experience in performing lymphography using indocyanine green (ICG)-enhanced fluorescence to perform lymphatic-sparing laparoscopic Palomo varicocelectomy.
Patients and Methods:
The records of 103 patients who underwent laparoscopic left varicocelectomy from March 2018 to April 2023 were retrospectively evaluated. The average patients’ age was 13.7 years (range: 12–16). High-degree varicocele was associated with left testicular hypotrophy, and symptoms were present in all patients. At the beginning of our experience, in 41 cases, we injected 2 mL of ICG solution into the testis, then we reduced the amount of ICG solution to 1 mL, having the same results. The lymphatic vessels were clearly identified and spared, then the entire spermatic bundle was clipped and divided according to Palomo’s principle.
Results:
We reported no conversions to open surgery and no adverse reactions induced by ICG. The average operative time was 18 minutes (range: 10–35). We performed clinical evaluations at 1 week, 1 month, 6 months, 1 year, and 2 years after surgery, and Ultrasound (US) was performed at 1 and 2 years postoperatively. In 3 patients, we discovered a small calcification due to the injection of the dye inside the testis; for this reason, we reduced the amount of ICG from 2 to 1 mL with the disappearance of this problem. No recurrence of varicocele or postoperative hydrocele was recorded.
Conclusions:
Our 5-year experience showed that the intratesticular injection of ICG and use of fluorescence vision allowed identification of lymphatic. ICG fluorescence lymphography is a safe and effective option to perform lymphatic-sparing laparoscopic Palomo varicocelectomy in children and adolescents with high-degree varicocele. No allergy to ICG or postoperative hydrocele was reported in our experience. It is preferable to inject 1 mL of ICG solution in the testis to avoid the risk of having small calcification in the testis at US controls.
Introduction
Currently, the most frequently used surgical technique for treating high-grade testicular varicocele in children is laparoscopic varicocelectomy, according to Palomo.1,2 This technique involves ligating the internal spermatic vessels. This procedure has a recurrence rate of 3%–5% and a postoperative hydrocele incidence of approximately 10%–30%.3,4 In fact, the most common conditions that can arise after varicocelectomy surgery are hydrocele and testicular edema, conditions that can cause testicular discomfort and/or require further surgery. 5 In this regard, in order to reduce the incidence of secondary hydrocele, numerous lymphatic-sparing procedures associated with varicocele correction have been described in the literature.
Recently, we reported in a clinical study the standardization of Palomo’s technique with lymphatic sparing by means of preoperative intradartoic/intratesticular injection of isosulfan blue. 6 Despite the excellent results in terms of lymphatic sparing, this technique has the disadvantage of coloring the patient’s urine blue/green for 2–3 days after surgery. In addition, after the injection of isosulfan blue, the patient’s scrotum was bluish in color for approximately 1–2 weeks postoperatively. In order to minimize these problems, we began using indocyanine green (ICG) as a new lymphography technique to perform Palomo’s laparoscopic varicocelectomy with lymphatic sparing in pediatric patients. 7
This study reports our 5-year experience in performing lymphography with ICG-enhanced fluorescence to perform laparoscopic varicocelectomy according to Palomo with lymphatic preservation.
Patients and Methods
We performed a retrospective analysis of the medical records of 103 patients who underwent left laparoscopic varicocelectomy at our unit between March 2018 and April 2023. The patients’ ages ranged from 12 to 16 years, with a mean age of 13.7 years. All had high-grade varicocele (grade II or III according to Dubin’s clinical classification), painful or uncomfortable symptoms in the left testicle, and left testicular hypotrophy, defined as a reduction in volume of at least 20% compared with the contralateral testicle.
Before surgery, each patient underwent testicular ultrasound and venous Doppler examination to assess venous reflux.
In the postoperative follow-up, patients were re-evaluated 1 week after surgery to check the surgical wound and then at 1, 6, 12, and 24 months, checking for any persistence or recurrence of varicocele or the appearance of a hydrocele.
The study was approved by the Ethics Committee of the Federico II University of Naples.
Surgical technique
The operation was carried out under general anesthesia with the patient intubated. Patients were positioned supine with a slight Trendelenburg tilt. 6 Three trocars were always used. The first trocar—either 5 or 10 mm for the 0-degree scope—was inserted at the umbilicus using an open transumbelical technique, and the remaining two 5-mm working trocars were placed under direct vision to form a triangulated setup with the camera port. Once pneumoperitoneum was established, a peritoneal window was created around the dilated spermatic vessels, approximately 3–5 cm from the internal inguinal ring. Afterward, a vial of ICG (5 mg/dL) was diluted in 10 mL of distilled water, and 1 mL of this solution was injected directly into the left testicular body using a 32-gauge needle. Under near-infrared imaging, lymphatic vessels became fluorescent, allowing for clear identification and preservation. The entire spermatic bundle was then clipped and divided following Palomo’s technique (Fig. 1).
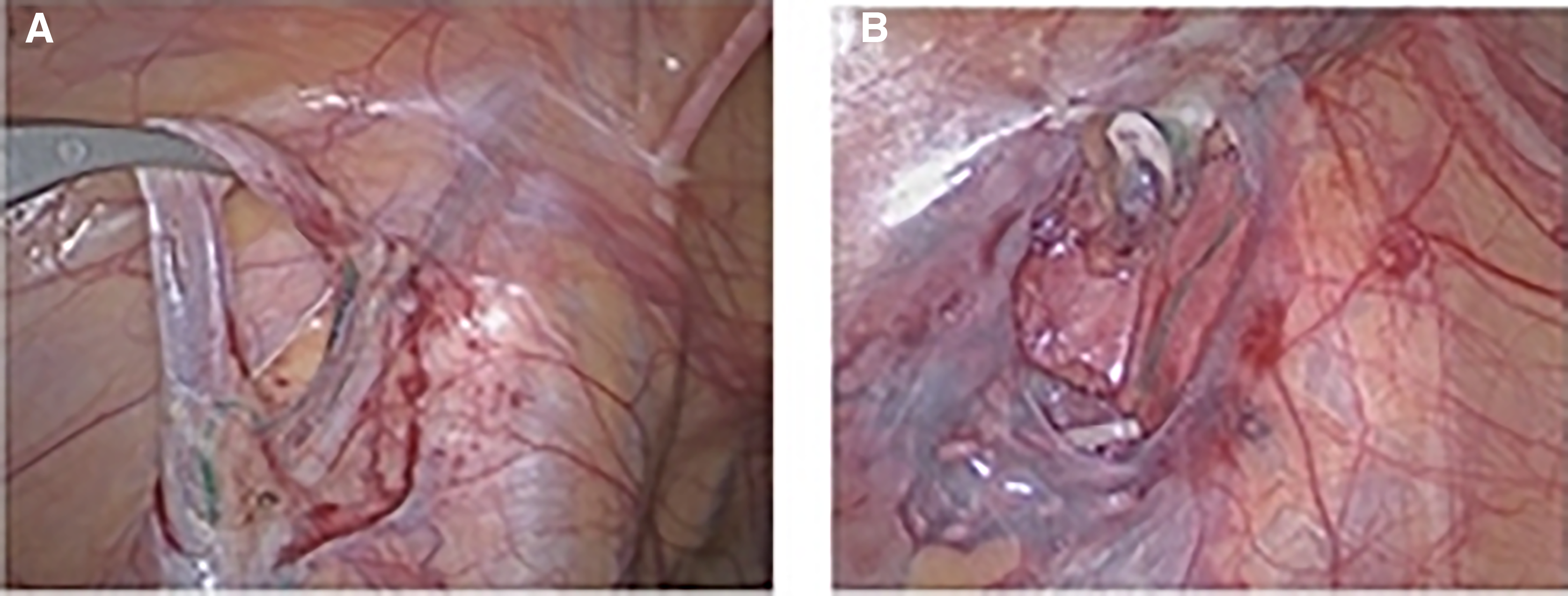
Even under standard white-light visualization, the lymphatic vessels were easy to distinguish because they showed a green coloration (Fig. 2). In recent years, we have incorporated a newer NIR fluorescence system—the IMAGE1 S™ Rubina® 4K, 3D, NIR/ICG platform by Karl Storz. Its overlay function projects the NIR/ICG fluorescence signal onto the white-light image, providing additional useful detail. The IMAGE1 S Rubina system also includes an intensity map of the NIR/ICG signal and a pure near-infrared monochromatic mode, which enhances the definition of anatomical structures (Fig. 3). Because ICG is primarily metabolized by the liver, patients’ urine maintained its normal appearance after surgery, and no dye residue was visible at the scrotal injection site. Early in our study, 2 mL of ICG was injected intratesticularly, but in the last 62 procedures, we switched to using a 1-mL intratesticular dose, obtaining the same results.
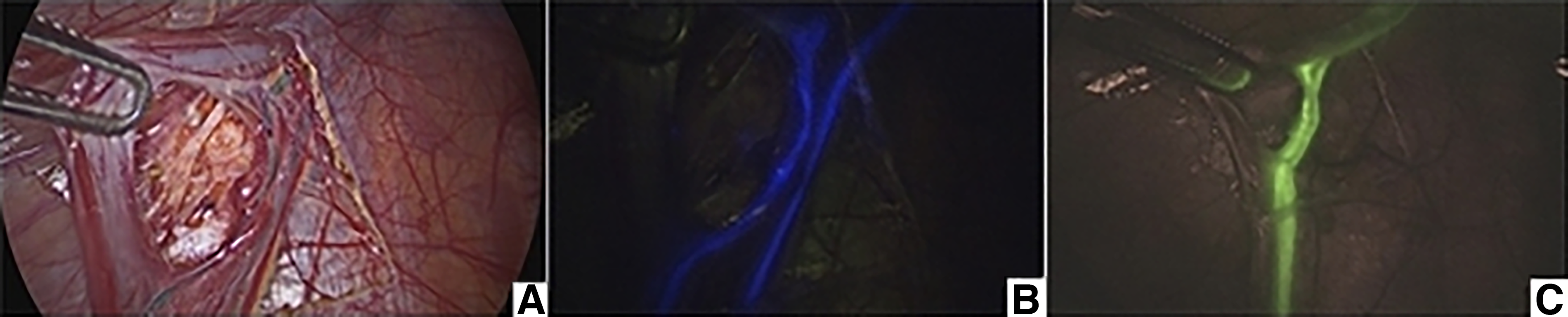
Mapping of lymphatic vessels in different NIRF modes:

Results
No intraoperative complications occurred, and none of the cases required conversion to open surgery. The mean operative time was 18 minutes, with a range of 10–25 minutes. Within approximately 10–20 seconds after intratesticular ICG administration, lymphatic fluorescence was successfully visualized in all patients. Under near-infrared imaging, the lymphatic vessels appeared fluorescent (Fig. 2), while in standard white-light mode, they showed a green coloration (Fig. 1).
In every case, approximately two to three lymphatic vessels were identified and preserved. All patients were able to resume a full oral diet about 2 hours after surgery, and the average need for analgesia lasted 12 hours (range: 8–28 hours). The mean hospital stay was 36 hours (range: 22–48 hours). No ICG-related allergic reactions or other adverse effects occurred. None of the patients experienced testicular discomfort related to the intratesticular injection, either in the immediate postoperative period or later on. With follow-up of up to 24 months (excluding those treated in 2023), no varicocele recurrence or persistence was identified, and no postoperative hydrocele developed. Five patients (5%) developed an umbilical port-site infection, which was managed with oral antibiotics and local treatment (Clavien grade II).
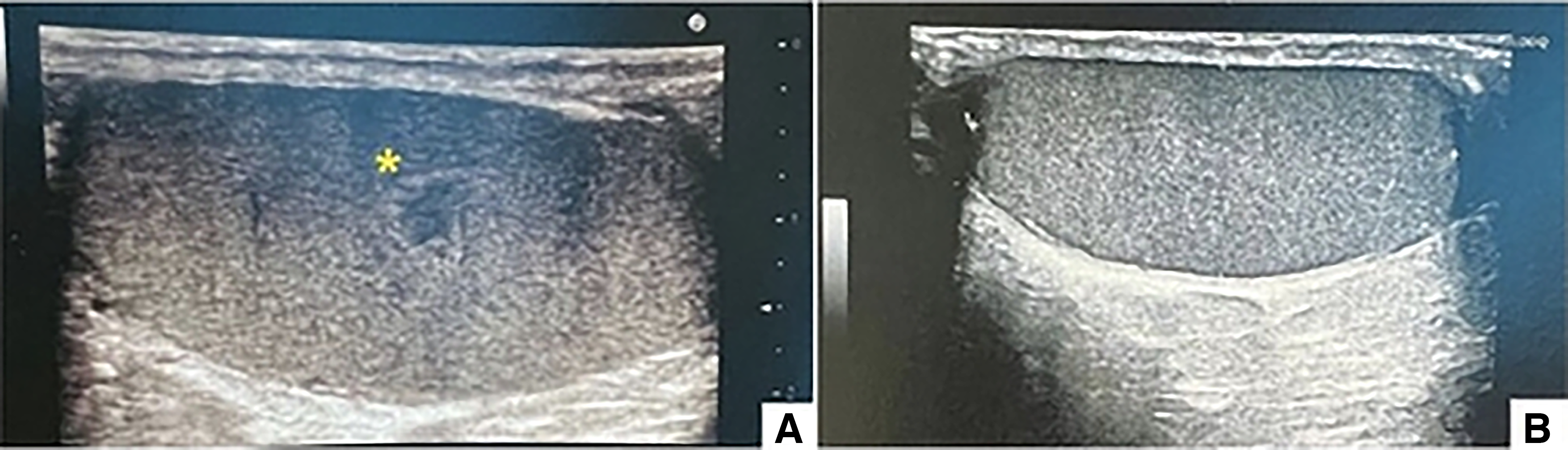
Ultrasound follow-up revealed small intratesticular calcifications in three patients, attributable to the dye injection (Fig. 4). All patients reported high satisfaction with the cosmetic appearance of their postoperative scars. Serum markers (alpha-fetoprotein, beta-hCG, and lactate dehydrogenase), obtained as a precaution, were normal in all three cases. Testicular ultrasound at 6 months showed that the calcific area had resolved in 2 of the 3 patients (66.7%) by 1 year (Fig. 5), while the third remains under observation. Postoperative ultrasound confirmed varicocele resolution in 97 of 103 patients (94.2%). A low-grade (I–II) persistent varicocele (Clavien I) was seen in 6 of 103 patients (5.8%), none of whom required reintervention. Semen analysis was repeated 1 year after surgery in those who had undergone testing preoperatively, and all demonstrated a marked improvement in asthenospermia, with motility increasing by more than 40% compared with baseline (Table 1).

US follow-up with a small hypoechoic area and showing no vascularization.
Results
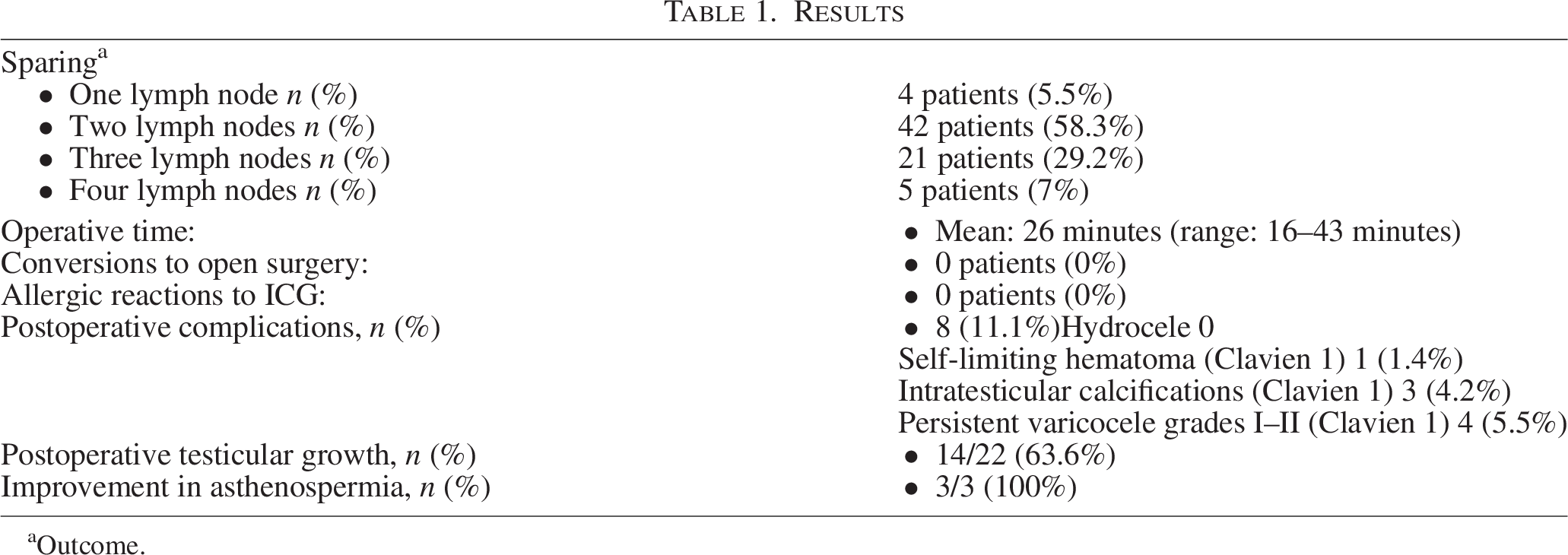
Outcome.
Discussion
Varicocele is one of the most common conditions in the pediatric population, occurring in roughly 15%–20% of cases. 8 It is often linked to testicular injury, reduced testicular volume, sperm DNA abnormalities, and male infertility—all of which can improve after surgical 9 correction.10–13 Three primary surgical approaches have been described for managing this prevalent pediatric condition: Suprainguinal high ligation, subinguinal microsurgical low ligation, and laparoscopic repair. 14 In recent years, multiple studies have highlighted the safety and effectiveness of laparoscopy as a treatment option for pediatric varicocele.1,2
The laparoscopic Palomo technique is the most widely used minimally invasive approach in pediatric patients.1,8 According to the international literature, this method shows a lower operative failure rate than artery-sparing techniques, without an associated rise in testicular hypotrophy or atrophy.1,8 However, its main drawback is the relatively high incidence of postoperative hydrocele (10%–30%), largely because the procedure does not involve intentional preservation of lymphatic vessels, which are challenging to visualize.3–5 To address this issue, lymphatic-sparing methods have been introduced to reduce the risk of hydrocele formation after varicocele repair.15–17 Various vital dyes—such as methylene blue, patent V, and its isomer isosulfan blue—have been used to perform lymphography during lymphatic-sparing procedures.13,18–21 We recently described a standardized lymphatic-sparing Palomo technique that uses preoperative intradartoic/intratesticular injection of isosulfan blue. 6 This method allows excellent outcomes, including a 0% postoperative hydrocele rate, and no complications related to the dye—such as orchitis, allergic reactions, or anaphylaxis—were observed in our cohort.6,8 In recent years, the adoption of fluorescence-guided minimally invasive surgery using ICG technology has enhanced the ability to visualize anatomical structures and obtain detailed intraoperative information.22,23
ICG can be safely administered intravenously, with virtually no adverse effects. It becomes fluorescent when exposed to light of a specific near-infrared wavelength produced by a xenon light source. 24 After entering the bloodstream, ICG rapidly binds to plasma proteins—primarily lipoproteins—and is efficiently cleared by the liver, being excreted almost entirely unchanged into the bile within approximately 8 minutes after injection. 25 Fluorescence is captured using specialized scopes and cameras and displayed on a video monitor, allowing surgeons to visualize anatomical regions where ICG gets, such as bile ducts, blood vessels, and lymph nodes. Over the past several years, ICG-enhanced fluorescence imaging has been applied for improved visualization of the biliary system during laparoscopic cholecystectomy, assessment of lymphatic drainage, sentinel lymph node mapping in oncology, identification of vascular structures, and evaluation of organ and bowel perfusion.22–27 In the past 5 years, we have implemented intratesticular ICG injection to enhance visualization of lymphatic vessels during lymphatic-sparing laparoscopic Palomo varicocelectomy, and we have standardized this injection technique. After ICG administration, lymphatics can be visualized in two ways: They show fluorescence under near-infrared imaging (Fig. 2) and appear green under standard white-light imaging (Fig. 1). Switching between white-light and near-infrared modes is easily accomplished using a foot pedal or a camera button. Fluorescence typically appears within 10–30 seconds of injection and lasts for about 15 minutes. This duration allows the entire procedure to be completed with a single injection, without any loss of fluorescence. The method of ICG delivery—direct injection into the testicular parenchyma—is technically easy to perform. The primary limitations of using ICG include the requirement for specialized equipment in the operating room—specifically, a camera system capable of functioning in both white-light and fluorescence modes, as well as an ICG-compatible laparoscope with a dedicated filter to ensure accurate imaging during ICG-enhanced fluorescence and standard visualization. The new IMAGE1 S Rubina system by Karl Storz provides three distinct NIR/ICG imaging options: Overlay, intensity map, and monochromatic modes (Fig. 3). In summary, our 5-year experience demonstrates that lymphatic-sparing laparoscopic Palomo varicocelectomy with ICG fluorescence lymphography is a practical and adaptable technique for managing varicocele in children and adolescents. Intratesticular ICG administration combined with fluorescence imaging proved to be a safe and effective approach, enabling lymphatic vessel identification in 100% of cases. Moreover, no ICG-related allergic reactions or postoperative hydroceles occurred during long-term follow-up.
Authors' Contributions
Conceptualization: M.C., A.T., M.E., and C.E. Methodology: F.T., V.C., V.G., and G.E. Analysis: G.E., M.C., M.E., A.T., and M.P. Writing original draft: M.C. Revision and editing: C.E.
Disclosure Statement
The authors have no relevant financial disclosures.
Footnotes
Funding Information
This research did not receive any specific funding from any agencies in the public, commercial, or not-for-profit areas.