
Abstract
Objective:
The widespread use of online video platforms has transformed surgical education, particularly for minimally invasive procedures. This study aimed to evaluate the educational quality of laparoscopic adrenalectomy videos available on YouTube and to investigate whether digital popularity metrics reflect educational value.
Methods:
A YouTube search was conducted on January 1, 2026, using the keyword “laparoscopic adrenalectomy.” The first 250 videos were screened, and 135 videos meeting the inclusion criteria were analyzed. Educational quality was assessed independently by 2 experienced surgeons using LAP-VEGaS, JAMA benchmark criteria, Modified DISCERN, and Global Quality Score (GQS). Videos were categorized as institutional or individual according to the uploader profile. Digital engagement metrics, including view ratio, like ratio, and Video Power Index (VPI), were calculated. Independent predictors of educational quality were analyzed using multiple linear regression.
Results:
Of the included videos, 36 (26.7%) were uploaded by institutional sources and 99 (73.3%) by individual users. Institutional videos demonstrated significantly higher educational quality scores across all structured assessment tools, including LAP-VEGaS, GQS, JAMA, and Modified DISCERN (P < .001). In multiple regression models, channel type was identified as the only independent predictor of educational quality scores (P < .05). In contrast, digital popularity indicators such as view ratio, like ratio, and VPI were not significantly associated with educational quality. No meaningful correlation was observed between video popularity and LAP-VEGaS score (R2 = 0.013).
Conclusion:
Laparoscopic adrenalectomy videos on YouTube show substantial variability in educational quality. Institutional videos provide higher educational value, while popularity metrics do not reliably indicate educational quality. Surgical trainees should preferentially use academically produced content for educational purposes.
Keywords
Introduction
With the widespread adoption of minimally invasive surgery, video-based learning resources have become increasingly important in surgical education. Particularly in laparoscopic and endoscopic procedures, the ability to visually demonstrate surgical techniques has transformed online video platforms into valuable educational tools. Today, surgical residents and early-career surgeons frequently utilize open-access platforms such as YouTube during preoperative preparation.1,2
However, previous studies have demonstrated that the educational quality of online surgical videos is highly heterogeneous, and many videos fail to adequately demonstrate critical procedural steps.3–6 Furthermore, digital engagement metrics such as view counts and like ratios do not always correlate with content quality.7–10 These findings highlight the need for systematic evaluation of online surgical content using structured quality assessment tools.
Recent studies suggest that video-based learning can contribute significantly to the development of surgical skills and serve as an important adjunct educational tool in minimally invasive surgery training.11–14 Nevertheless, for online surgical videos to function as reliable educational resources, they must adhere to established quality standards.
The aim of this study was to evaluate the educational quality of laparoscopic adrenalectomy videos available on YouTube and to investigate the relationship between video characteristics and educational quality. In addition, potential differences in quality between academic and individually uploaded videos were assessed.
Materials and Methods
The YouTube™ platform was searched on January 1, 2026. During the search, the user account was logged out and default search settings were used. To minimize the effect of algorithmic personalization, the browser history was cleared before conducting the search. The term “laparoscopic adrenalectomy” was entered into the search bar, and only the “video” content type was selected in the filter section.
The first 250 videos listed on the results page were screened for eligibility. This approach was chosen to reflect the visibility ranking encountered in a typical user experience.
Inclusion/Exclusion criterias
Videos were included if they met the following criteria: Uploaded between January 2015 and January 2026 English language Clearly demonstrated a laparoscopic adrenalectomy procedure in humans Video duration ≥3 minutes
The duration threshold was introduced to ensure adequate evaluation of surgical steps and technical details.
Videos were excluded if they:
Were duplicates Were uploaded outside the defined time period Demonstrated procedures performed on animal models Included only animation or theoretical explanations Presented partial or incomplete surgical footage Focused solely on complication management Were promotional or industry-sponsored content Were technically unsuitable for evaluation
Of the initial 250 videos, 115 were excluded, and 135 videos were included in the final analysis. The selection process was reported using a flow diagram similar to the PRISMA framework.
Educational quality assessment
The educational quality and procedural completeness of the videos were evaluated using structured scoring systems commonly used in the literature (Table 1).
LAP-VEGaS (Laparoscopic Video Educational Guideline Score), JAMA Benchmark Criteria, Modified DISCERN and Global Quality Score (GQS) Scales
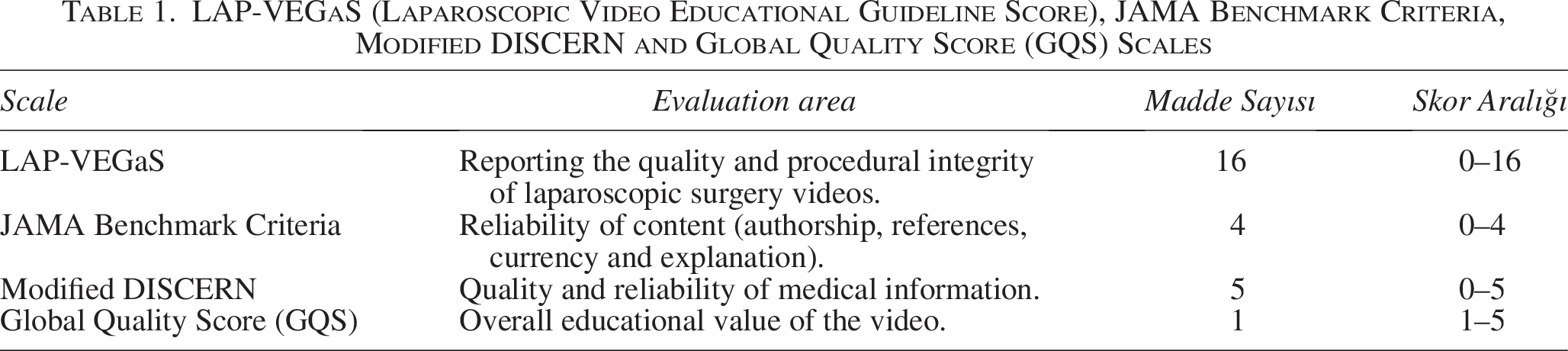
LAP-VEGaS (Laparoscopic Video Educational Guideline Score), JAMA benchmark criteria, Modified DISCERN, and Global Quality Score (GQS).
LAP-VEGaS score
The LAP-VEGaS score is a 16-item checklist designed to assess reporting quality and procedural completeness in laparoscopic surgical videos. It evaluates key elements including: clarity of title and objectives, patient positioning, port placement, identification of anatomical structures, sequential presentation of surgical steps, reporting of critical technical details, complication management, and outcome reporting.
Each item is scored present/absent, yielding a total score between 0 and 16.
JAMA benchmark criteria
The JAMA benchmark criteria consist of four components:
Authorship, attribution, disclosure, currency that scores range from 0 to 4.
Modified DISCERN
The modified DISCERN instrument evaluates the reliability and quality of online medical information using five questions, producing scores between 0 and 5.
Global quality score
GQS is a subjective measure of the overall educational value of the video, rated from 1 (very poor quality) to 5 (excellent quality).
Popularity metrics
Digital popularity and viewer engagement were assessed using quantitative parameters are total views, number of likes, number of dislikes.
Additional metrics were calculated as follows:
View Ratio = total views/days since upload
Like Ratio = likes/(likes + dislikes) × 100
Video Power Index (VPI) = (Like Ratio × View Ratio)/100
Videos were categorized according to uploader type:
Institutional channels (universities, academic hospitals, and professional associations) and individual channels.
Video evaluation process
All videos were independently evaluated by 2 researchers experienced in laparoscopic surgery. In cases of disagreement, a third independent reviewer was consulted. Prior to evaluation, a standardization meeting was conducted to ensure calibration between reviewers.
Inter-rater reliability was assessed using intraclass correlation coefficient (ICC) analysis:
LAP-VEGaS: ICC = 0.86
JAMA: ICC = 0.83
Modified DISCERN: ICC = 0.84
GQS: ICC = 0.75
ICC values greater than 0.75 indicated good inter-rater agreement.
Statistical analysis
Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
The distribution of continuous variables was assessed using the Shapiro–Wilk test.
Normally distributed variables were presented as mean ± standard deviation.
Nonnormally distributed variables were presented as median (minimum–maximum).
Group comparisons were conducted using the Mann–Whitney U test.
To identify independent predictors of educational quality, multiple linear regression analyses were performed. LAP-VEGaS, GQS, JAMA, and Modified DISCERN scores were analyzed as dependent variables in separate models using the Enter method.
Independent variables included:
channel type
View Ratio
Like Ratio
VPI
Multicollinearity was evaluated using tolerance and variance inflation factor (VIF) values. Acceptable limits were defined as:
Tolerance >0.10
VIF < 5
Model fit was assessed using R2 and adjusted R2 values.
A P value <.05 was considered statistically significant.
Results
A total of 250 videos identified from the YouTube search results were screened for eligibility. After applying the predefined inclusion and exclusion criteria, 115 videos were excluded and 135 videos were included in the final analysis (Fig. 1).
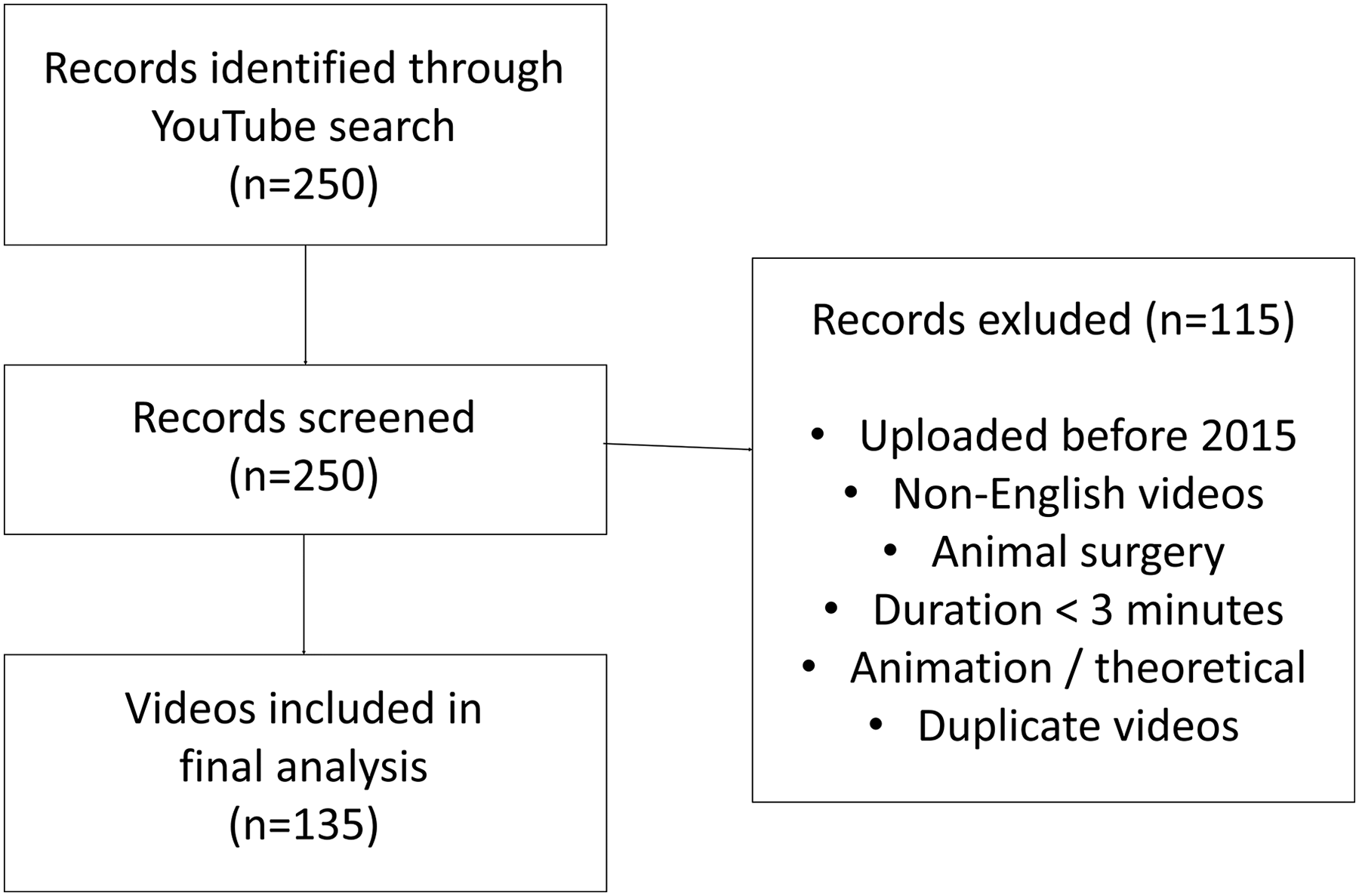
PRISMA video selection diagram.
Among the analyzed videos, 36 (26.7%) were uploaded by institutional channels, whereas 99 (73.3%) were uploaded by individual users. Institutional videos tended to be longer in duration; however, this difference did not reach statistical significance.
The mean educational quality scores of the evaluated videos were as follows: GQS 2.96 ± 1.03, LAP-VEGaS score 9.73 ± 3.47, JAMA score 1.24 ± 0.46, and Modified DISCERN score 2.94 ± 0.79. With regard to digital popularity indicators, the mean view ratio was 2.57 ± 5.37, the mean like ratio was 2.38 ± 2.21, and the mean VPI was 0.05 ± 0.16.
When videos were compared according to channel type, institutional videos demonstrated significantly higher educational quality scores than videos uploaded by individual users. Institutional videos had significantly higher GQS, LAP-VEGaS, JAMA, and Modified DISCERN scores (all comparisons P < .001). In contrast, no statistically significant differences were observed between institutional and individual videos in terms of view ratio, like ratio, or VPI values (P > .05) (Table 2). The distribution of educational quality scores according to channel type is illustrated in Figure 2.
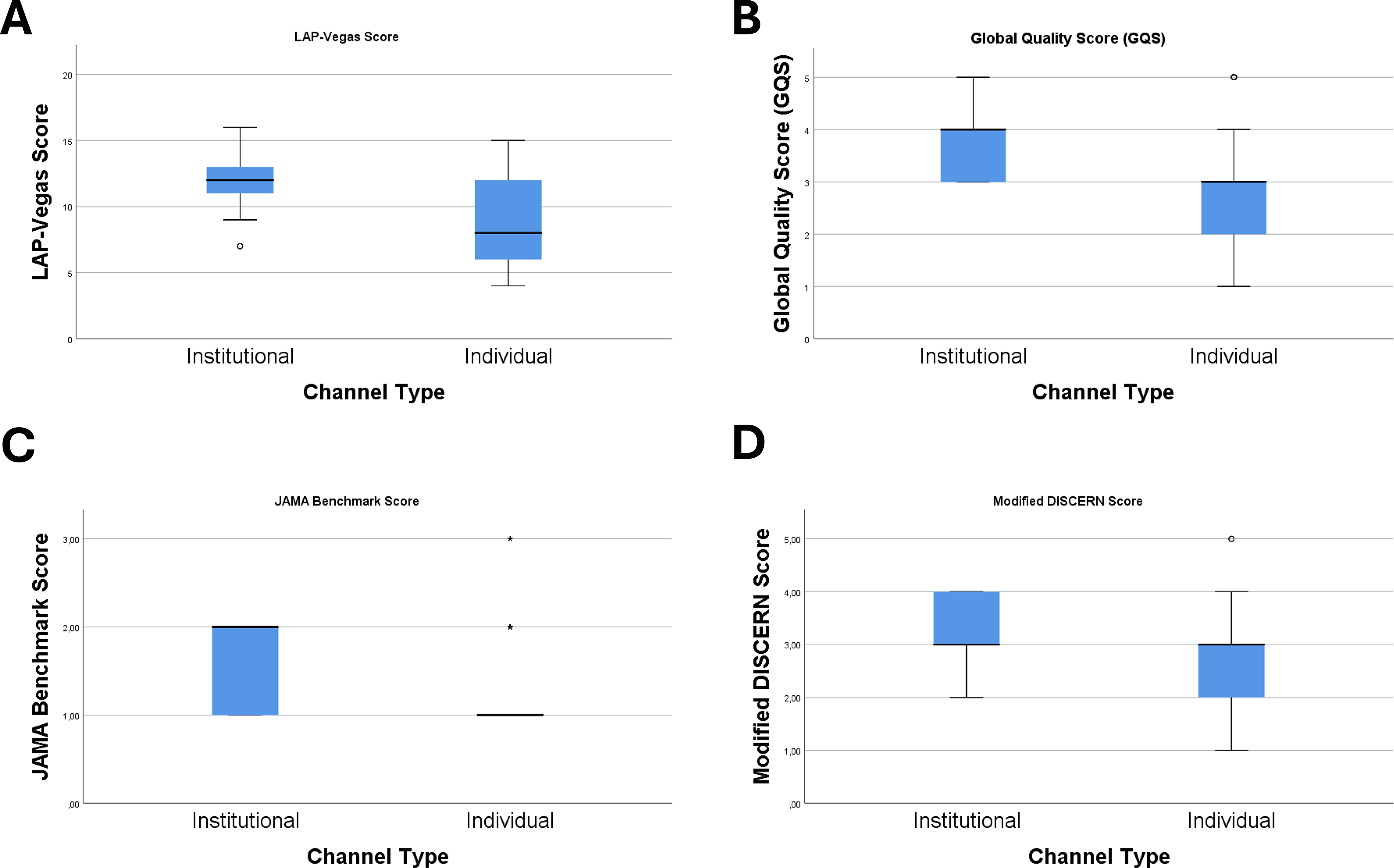
Comparison of educational quality scores between institutional and individual channels.
General Characteristics of Videos and Channel-Type-Specific Characteristics
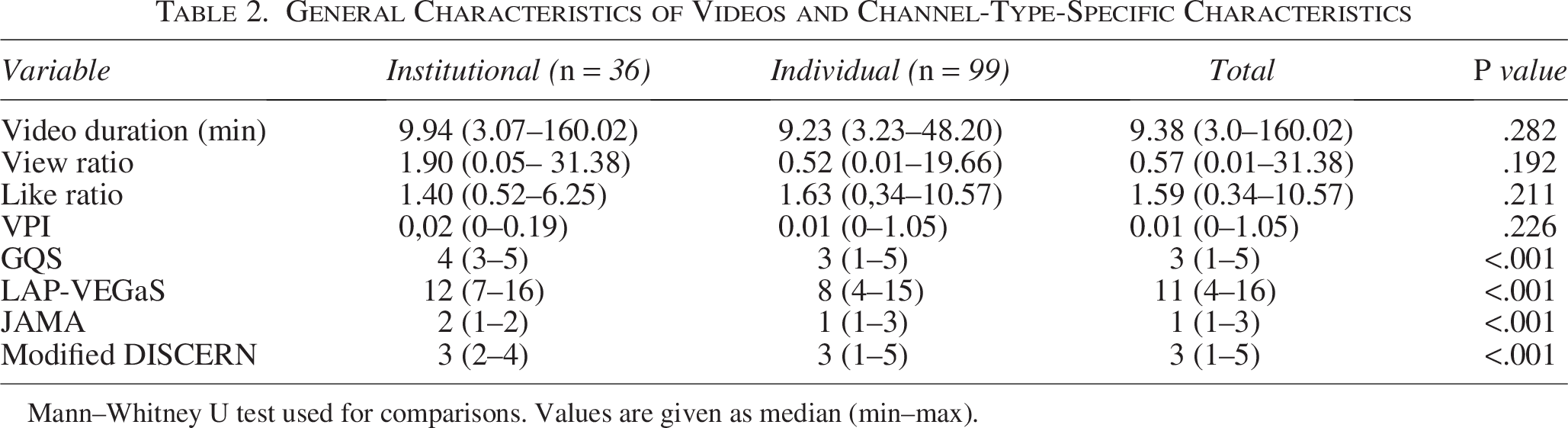
Mann–Whitney U test used for comparisons. Values are given as median (min–max).
Multiple linear regression analyses were performed to identify independent predictors of educational quality. For the LAP-VEGaS score, the regression model was statistically significant (R2 = 0.177; P = .012). Within this model, channel type emerged as the only independent predictor of the LAP-VEGaS score (β = −0.411; P = .001), whereas view ratio, like ratio, and VPI were not significant contributors (P > .05) (Table 3).
Multiple Linear Regression Analyses
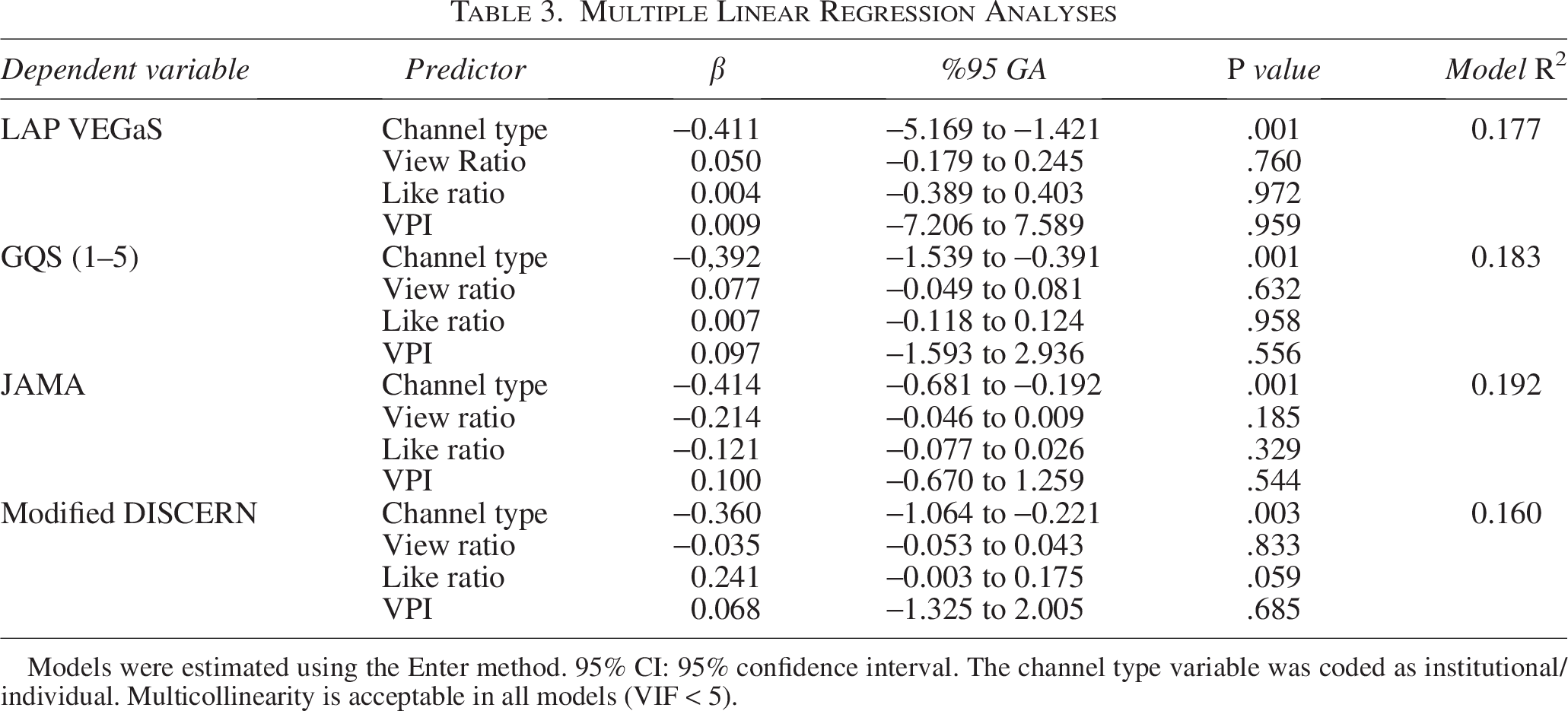
Models were estimated using the Enter method. 95% CI: 95% confidence interval. The channel type variable was coded as institutional/individual. Multicollinearity is acceptable in all models (VIF < 5).
Similarly, regression models constructed for GQS (R2 = 0.183; P = .010), JAMA (R2 = 0.192; P = .007), and Modified DISCERN (R2 = 0.160; P = .021) also identified channel type as the only independent determinant of educational quality scores. None of the digital popularity metrics demonstrated a significant independent effect.
Overall, the findings indicate that institutionally uploaded videos demonstrate superior structured educational quality, whereas commonly used digital popularity metrics do not independently reflect educational value. To evaluate whether video popularity reflects educational quality, the relationship between view ratio and LAP-VEGaS score was analyzed. As shown in Figure 3, no meaningful correlation was observed between video popularity and educational quality (R2 = 0.013). Both institutional and individual videos demonstrated a wide dispersion of LAP-VEGaS scores regardless of view ratio.
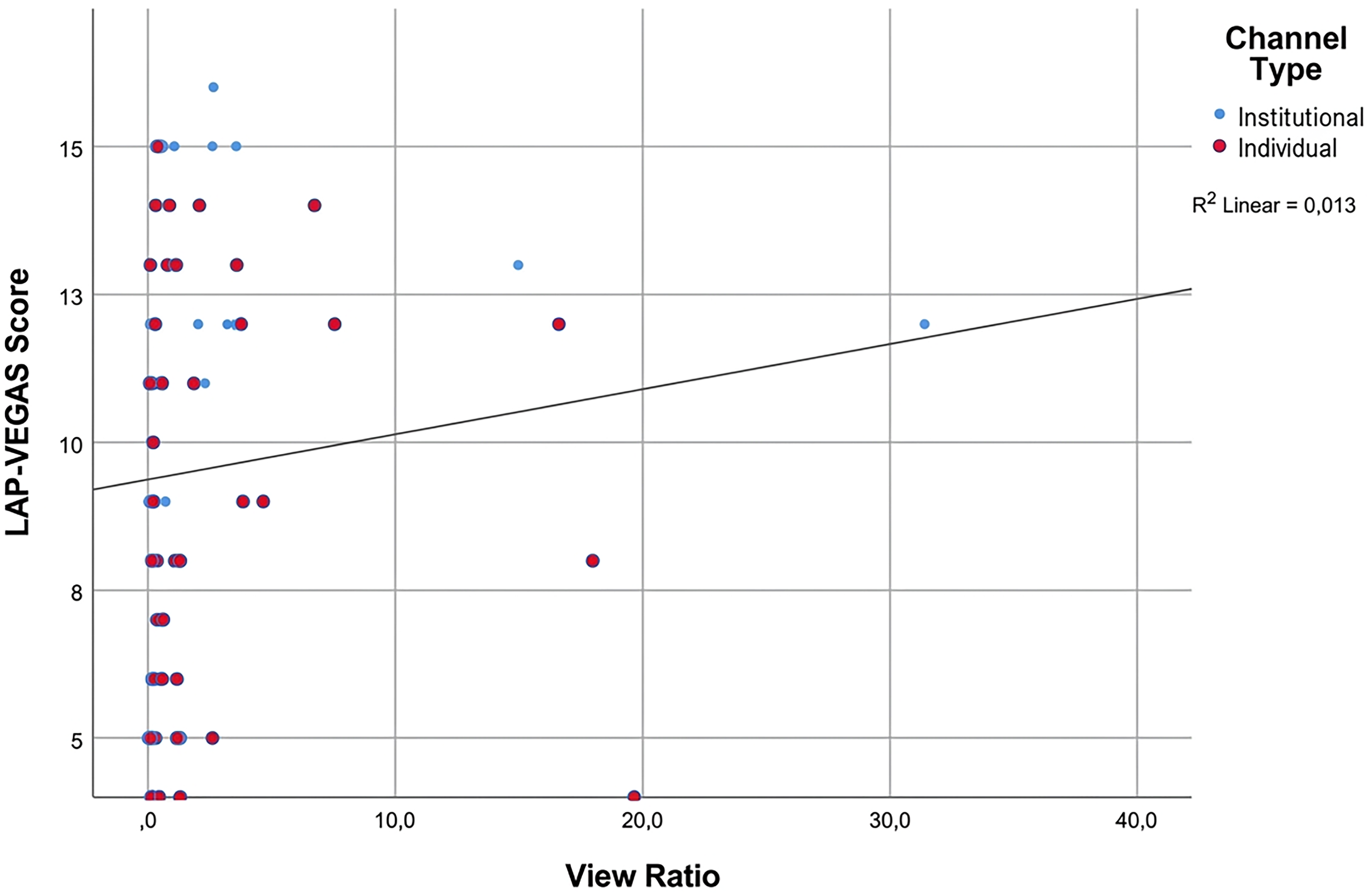
Relationship between video popularity and educational quality.
Discussion
Online video platforms have increasingly become an important component of surgical education, particularly for minimally invasive procedures where visual demonstration of surgical techniques is highly valuable. Surgical residents and early-career surgeons frequently rely on platforms such as YouTube for preoperative preparation and technical learning. However, the educational reliability of such platforms remains a matter of debate due to the absence of standardized quality control.1,7
The present study demonstrated that laparoscopic adrenalectomy videos on YouTube exhibit considerable heterogeneity in educational quality. One of the most notable findings was that videos uploaded by institutional or academic sources consistently demonstrated significantly higher educational quality scores compared with those uploaded by individual users. This finding aligns with previous studies evaluating online surgical videos for various minimally invasive procedures, which have reported that videos produced by academic centers tend to present surgical steps more systematically and provide clearer identification of anatomical structures and technical details.7,9,13
Another important finding of the present study is the lack of a meaningful relationship between video popularity and educational quality. Although metrics such as view counts, like ratios, and engagement indices are frequently used as indicators of content visibility and popularity, these parameters do not appear to reliably reflect educational value. This observation has also been reported in previous investigations evaluating surgical videos on YouTube, suggesting that highly viewed videos are not necessarily those with the highest educational quality.7,11 The algorithms used by online platforms generally prioritize viewer engagement rather than educational accuracy, which may explain why educationally valuable content does not always receive greater visibility.
The use of structured scoring systems such as LAP-VEGaS, JAMA benchmark criteria, and Modified DISCERN has become increasingly important for the objective evaluation of online surgical videos. These tools allow researchers to systematically assess key educational components, including the presentation of procedural steps, clarity of anatomical descriptions, reporting transparency, and overall informational reliability. In the present study, institutional videos achieved higher scores across all evaluation systems, suggesting that adherence to structured reporting principles contributes significantly to educational quality.
Video-based learning has been shown to enhance surgical skill acquisition and facilitate the understanding of complex minimally invasive procedures. However, the effectiveness of this educational approach depends heavily on the quality and completeness of the video content.12,14 Therefore, it is essential that surgical videos intended for educational purposes follow standardized reporting guidelines and present procedures in a structured and comprehensive manner.
Academic institutions and professional surgical societies may play a critical role in improving the reliability of online surgical education by producing high-quality educational videos and disseminating them through accessible platforms. Encouraging the adoption of standardized video reporting frameworks such as LAP-VEGaS may further enhance the educational value of surgical videos available online.
Limitations
Several limitations of this study should be acknowledged. First, the analysis was limited to videos available on the YouTube platform. Other educational platforms and institutional video libraries used for surgical training were not included in the evaluation. Therefore, the findings may not fully represent the overall landscape of online surgical educational resources.
Second, YouTube content is dynamic, and video numbers, view counts, and engagement metrics may change over time. Because this study represents a cross-sectional analysis performed at a single time point, the results reflect the characteristics of the platform during the study period and may evolve as new videos are uploaded.
Third, some of the evaluation tools used in this study, particularly GQS and Modified DISCERN, include subjective components that depend on reviewer judgment. Nevertheless, the high level of inter-rater agreement observed in this study supports the reliability of the evaluation process.
Finally, the relatively modest explanatory power of the regression models suggests that additional factors may influence the educational quality of surgical videos. Variables such as narration quality, the surgeon’s level of expertise, the presence of annotations or step-by-step explanations, and the overall video production quality may also play a role. Future studies incorporating these parameters may provide a more comprehensive understanding of factors affecting online surgical education.
Conclusion
In conclusion, laparoscopic adrenalectomy videos available on YouTube demonstrate significant variability in educational quality. Videos uploaded by institutional or academic sources provide higher educational value and demonstrate better adherence to structured reporting standards. In contrast, commonly used digital popularity metrics such as view ratio, like ratio, and VPI do not reliably reflect the educational quality of surgical videos.
For surgical trainees and clinicians seeking educational material, prioritizing content produced by academic or institutional sources may provide a more reliable learning experience. Additionally, encouraging video producers to adopt standardized reporting frameworks such as LAP-VEGaS may help improve the overall quality of online surgical educational content.
Authors’ Contributions
Conceptualization: İ.T.; Methodology: R.Ç. and İ.T.; Data collection: İ.T.; Data analysis: R.Ç., B.D., and İ.T.; Writing—original draft: R.Ç.; Writing—review and editing: R.Ç., İ.T., and B.D.; Supervision: İ.T.
Footnotes
Acknowledgments
The authors thank all colleagues who contributed to the evaluation process of the surgical videos. No external writing or editorial assistance was received in the preparation of this article.
Ethical Approval
This study analyzed publicly available YouTube videos and did not involve human participants, patient data, or clinical intervention. Therefore, formal ethical approval was not required.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.