
Abstract
Introduction:
Robot-assisted laparoscopic surgery has emerged as a significant element of minimally invasive surgical techniques. Nevertheless, the impacts of port placement and the forces exerted by surgical instruments on tissue integrity, wound healing, and scar development remain inadequately understood. This study retrospectively assesses postoperative incisional scars from robot-assisted laparoscopic procedures performed at our institution between 2017 and 2023, comparing them with those observed in traditional laparoscopic procedures.
Materials and Methods:
A review of 402 patients from July 1, 2017, to September 1, 2023, focused on 56 undergoing robot-assisted laparoscopic surgery. Three were excluded for follow-up issues, leaving 53 in the study group. A matched control group of 53 patients with conventional laparoscopic procedures was also included. Demographic variables such as age, gender, body mass index, and operation duration were compared. At 1 year postop, three independent surgeons assessed incision scars using the Manchester Scar Scale (MSS) and Modified Manchester Scar Scale (MMSS).
Results:
An analysis of scar tissue from 53 pediatric patients who had robot-assisted laparoscopic surgery was compared with 53 who underwent conventional laparoscopy. Parameters included vascularization, pigmentation, thickness, elevation, and elasticity. Early postoperative assessments in the robot-assisted group revealed scars with poor cosmetic outcomes—such as hyperpigmentation and elevation—necessitating a thorough review.
Conclusion:
This study presents the first clinical report of hypertrophic scar formation at incision sites after robot-assisted laparoscopic surgery. To generalize these results and elucidate possible pathophysiological mechanisms, further studies involving larger patient groups and supported by immunohistochemical analyses are required.
Introduction
The development of postoperative scars remains a significant concern across both pediatric and adult populations. These scars are of considerable importance to patients and their families. The formation of such scars can lead to various social and psychological challenges, which may subsequently result in decreased self-confidence and impaired socialization abilities in children. 1
An ideal scar is unnoticeable, level with the surrounding tissue, and of the same color as the surrounding skin. Wound healing occurs in three stages: inflammation, proliferation, and remodeling.2,3
Today, robotic surgical applications are increasingly favored among pediatric patients. The primary reasons for opting for minimally invasive procedures include decreased postoperative analgesic requirements, reduced hospitalization duration, and favorable cosmetic outcomes.4,5
During the first year of follow-up for patients who underwent robotic-assisted laparoscopic surgery at our clinic, we assessed those presenting with suboptimal incision scars—characterized by hyperpigmentation and elevation above the skin—distinguishing them from patients who underwent laparoscopic procedures at our facility (Fig. 1). The incision scars were evaluated using a wound scar scoring system, and the study was conducted as a retrospective cohort analysis.
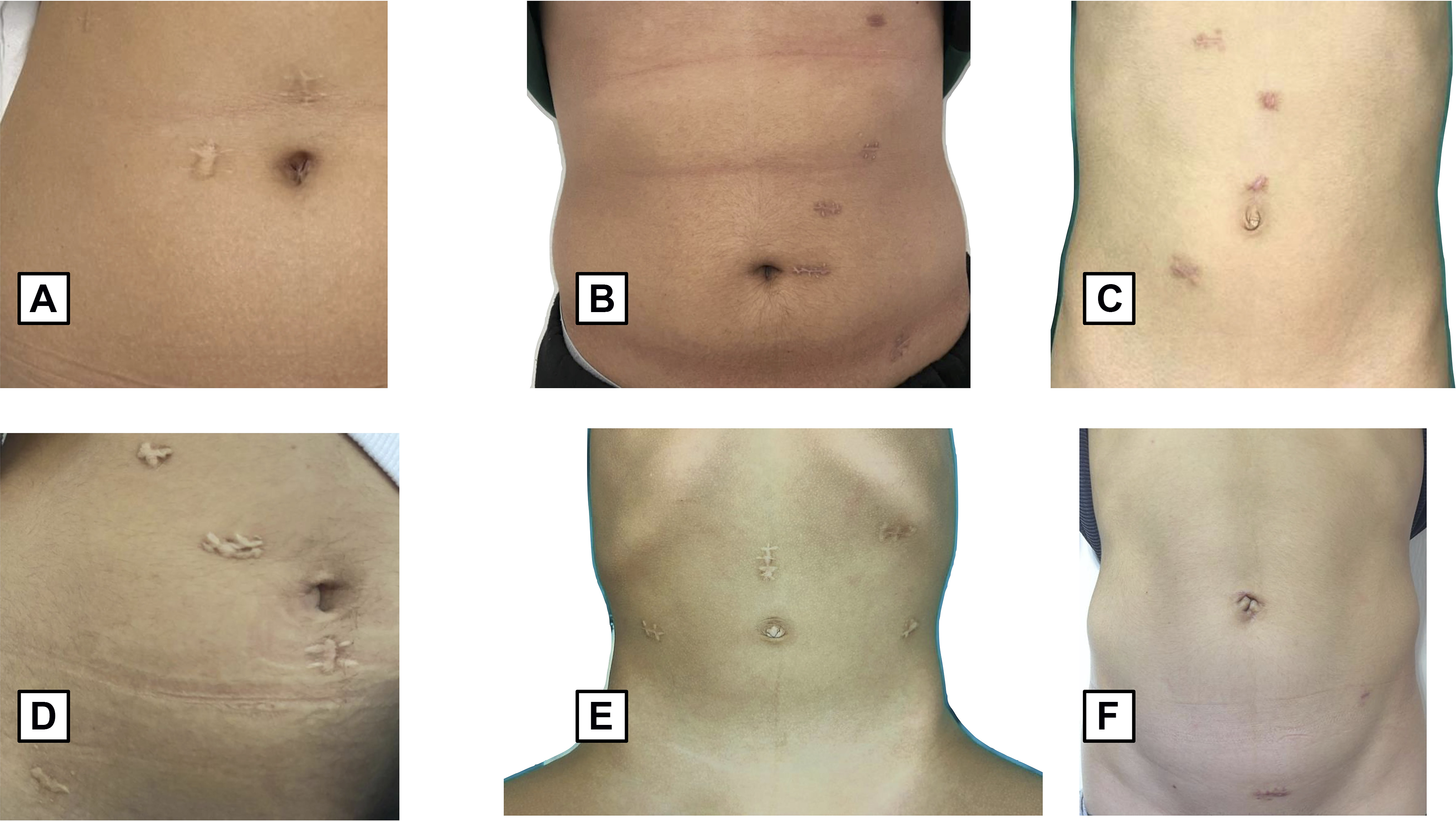
Appearance of incision scars at 12 months postoperatively
Materials and Methods
This study was approved by the Gulhane Clinical Research Ethics Committee (approval number: 2022/74). A retrospective review was conducted on 8402 patients who underwent surgical procedures between July 1, 2017, and September 1, 2023. Within this cohort, 106 pediatric patients were included. Of these, 53 patients received robot-assisted laparoscopic surgery (robotic group), and 53 underwent conventional laparoscopic surgery (control group).
Initially, a retrospective evaluation was conducted on 56 patients who underwent robot-assisted laparoscopic surgery. Three patients expired during follow-up due to causes unrelated to the surgical procedures; as a result, 53 patients (30 males and 23 females) were included in the final robotic surgery cohort.
The robotic surgical procedures conducted in these patients encompassed the following: pyeloplasty in 18 patients; fundoplication with gastrostomy in 9 patients; fundoplication alone in 2 patients; heminephrectomy in 3 patients; ureteral tapering and ureteral reimplantation for ureterovesical junction stenosis in 7 patients; antireflux surgery for vesicoureteral reflux in 7 patients, including 4 with bilateral vesicoureteral reflux; appendicovesicostomy in 1 patient; ovarian mass excision in 2 patients; urachal remnant excision in 1 patient; adrenal mass excision in 1 patient; thoracic mass excision in 1 patient; and diverticulectomy with ureteral reimplantation for bladder diverticulum in 2 patients (Fig. 2).
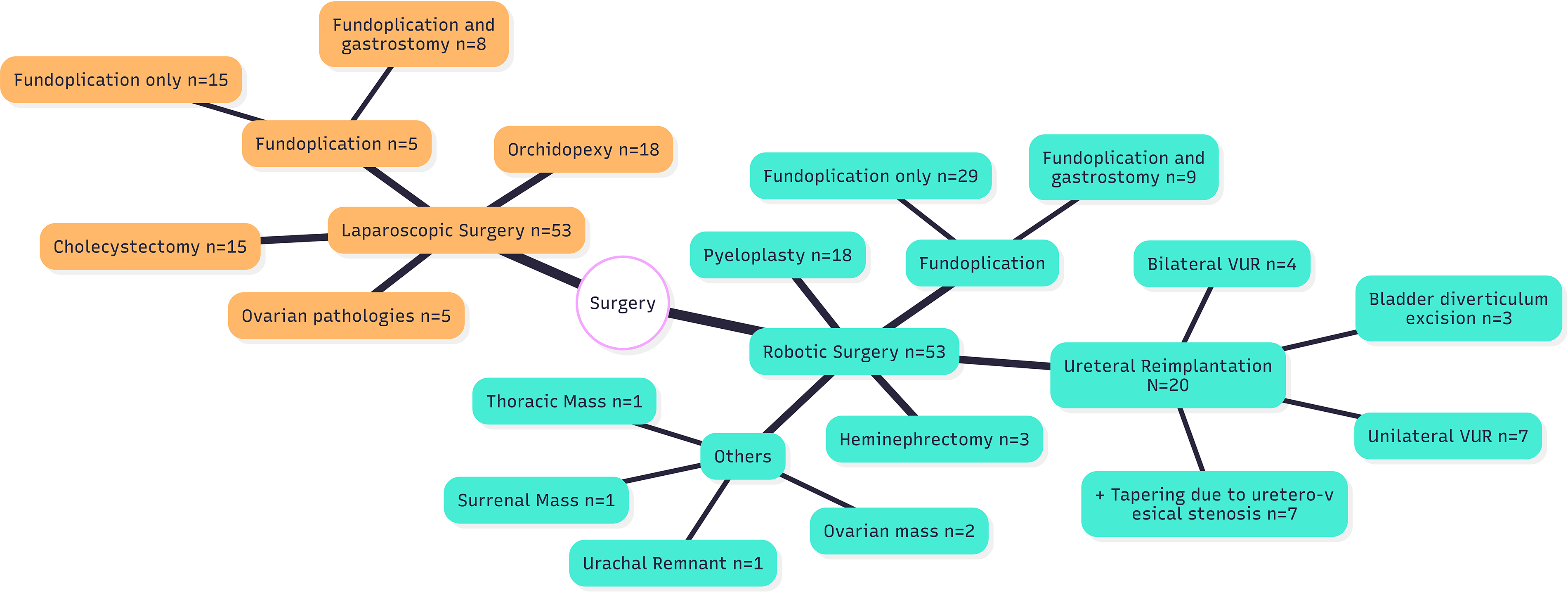
Distribution of procedures involving robotic-assisted laparoscopic surgery and conventional laparoscopic surgery.
The control cohort consisted of 53 pediatric patients who underwent conventional laparoscopic surgery during the same period of the study. Within this cohort, cholecystectomy was performed on 15 patients (mean age 14.1 years; range 11–17 years), orchidopexy on 18 patients (mean age 2.9 years; range 8 months–12 years), and surgical intervention for ovarian pathologies on 5 patients (mean age 15.5 years; range 12–17 years). Fundoplication was performed in 15 patients, and a combined procedure of fundoplication and gastrostomy was performed in 8 patients (mean age 4.12 years; range 9 months to 14 years). An additional five patients underwent orchidopexy, with a mean age of 3.75 years (range 9 months to 7 years). The cholecystectomy group exhibited a higher body mass index (BMI) compared with the fundoplication group (Fig. 2).
In the cohort of robotic patients operated using the da Vinci Xi Surgical System (Intuitive Surgical, Sunnyvale, CA, USA), a 12 mm trocar was used for the robotic camera optics, two 8 mm trocars were placed for the robotic working arms, and an 11 mm assistant trocar was employed for the introduction of materials such as sutures, nylon tape, and staplers into the abdominal cavity.
In one patient undergoing Nissen fundoplication, diaphragmatic hernia repair, gastrojejunostomy, and gastrostomy, an additional 12 mm trocar was introduced. During robotic surgery, the robotic arms were suspended, and CO2 insufflation was utilized to expand the operative field (Fig. 3).

In robotic-assisted laparoscopic surgery, the robotic arms are suspended to provide more intra-abdominal space.
In the cohort of patients undergoing laparoscopic procedures, a 10 mm camera trocar was inserted to facilitate endoscopic visualization, along with two or four 5 mm working ports. In some instances, an additional 10 mm trocar was employed (cholecystectomy: 2 × 10 mm + 3 × 5 mm). All patients received closure of the fascia at trocar sites using an absorbable suture, specifically polyglactin 910 (Ethicon, Somerville, NJ, USA). The subcutaneous fascia was approximated with an absorbable suture, and the skin was secured with a fast-absorbing suture (Ethicon, Somerville, NJ, USA).
The Manchester Scar Score (MSS) assesses and categorizes seven scar-related parameters. These parameters encompass scar color (which may be perfect, light, prominent, or incongruous with the surrounding skin), skin texture (matte or shiny), relationship with adjacent skin, texture (ranging from normal to firm), borders (distinct or indistinct), size (<1 cm, 1–5 cm, >5 cm), and whether the scar is solitary or multiple. According to this scoring system, the minimum possible score is 4, while the maximum score is 18. 6
In the Modified Manchester Scar Scale (MMSS), three scar parameters are evaluated: scar surface appearance, scar height, and color discrepancy. The scoring range extends from 3 to 12 points. The advantages of this scoring system include providing an objective assessment, facilitating posthealing follow-up, evaluating treatment efficacy, and ensuring standardization. Its widespread adoption in the scholarly literature enables comparability with other studies.
Photographs of surgical incision scars collected during postoperative follow-up appointments were categorized as those taken within the first month and within the first year postsurgery. During the scar assessment process, each port site scar was presented individually as a cropped image. The full abdomen and overall port configuration were not shown to the evaluators. Three surgeons assessed the patients’ scars at both the 1-month and 1-year postoperative intervals employing the Manchester Scar Score and the Modified Scar Assessment Score (Table 1).
Comparison of Manchester Scar Scale and Modified Scar-Rating Scale Scores Between Laparoscopic and Robotic Surgery
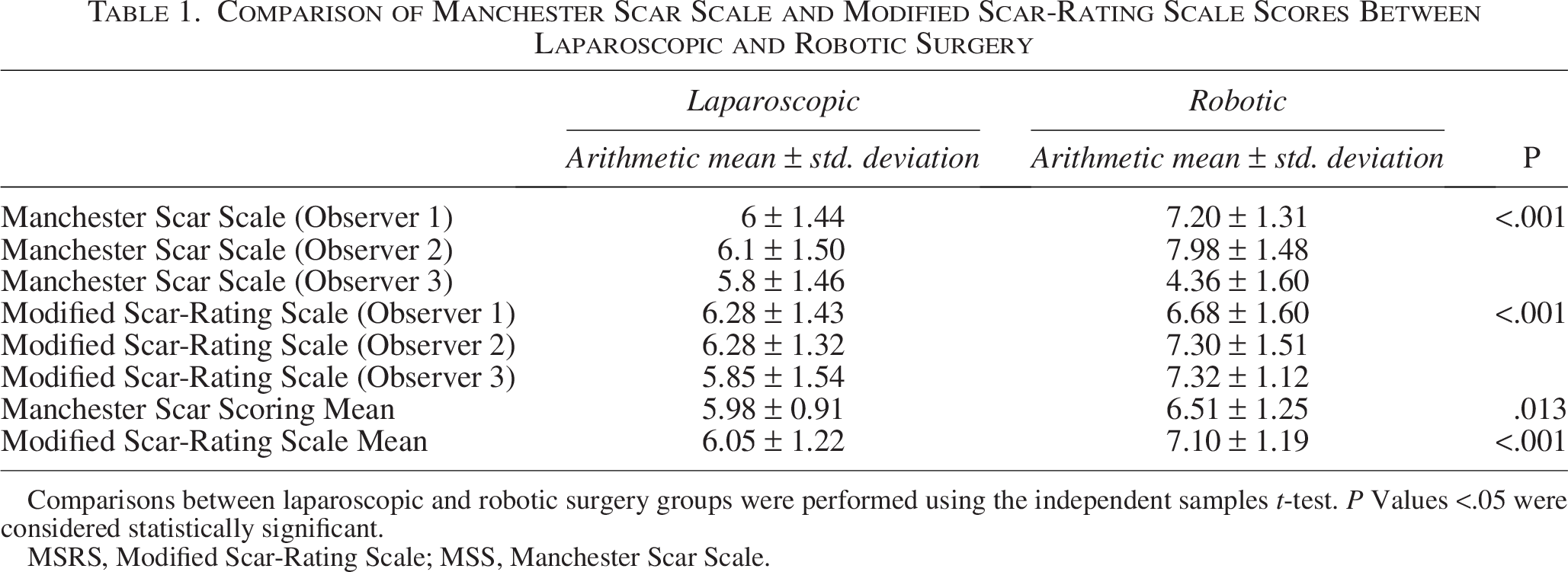
Comparisons between laparoscopic and robotic surgery groups were performed using the independent samples t-test. P Values <.05 were considered statistically significant.
MSRS, Modified Scar-Rating Scale; MSS, Manchester Scar Scale.
The correlation between scar assessment scores obtained after robotic-assisted and laparoscopic surgeries was evaluated using a correlation matrix, which revealed a significant association between the two scoring methods. Descriptive statistics were computed for all variables and were presented as arithmetic means ± standard deviations, medians with minimum–maximum ranges, or frequencies (n) and percentages (%), depending on the measurement level and data distribution.
Before conducting hypothesis testing, the normality of continuous variables was assessed using the Shapiro–Wilk test. The homogeneity of variances was evaluated using the Levene test, and sphericity was examined using the Mauchly test.
Changes in scar scores across both assessment scales were analyzed using the Friedman test. When a statistically significant difference was identified, post hoc pairwise comparisons were performed using the Dunn–Bonferroni correction.
The relationships between variations in scar scores and variables such as age, BMI, and the duration of surgery were examined employing the Spearman rank correlation coefficient. The impact of gender on differences in scar scores was evaluated using the Mann–Whitney U test.
The concordance among the three scar assessment scales was appraised utilizing the intraclass correlation coefficient (ICC) within a two-way mixed-effects model with absolute agreement. All statistical analyses were performed using IBM SPSS Statistics for Windows (Version 27.0; IBM Corp., Armonk, NY, USA). A P value of less than 0.05 was regarded as indicating statistical significance.
Results
A total of 106 pediatric patients were enrolled in the study, including 53 patients who underwent robotic-assisted surgery and 53 patients who underwent laparoscopic surgery. The gender distribution was identical across the two groups, with 30 boys and 23 girls in each cohort, and there was no statistically significant difference (P = 1.000). The mean age was 7.43 ± 5.46 years in the robotic group and 6.99 ± 6.15 years in the laparoscopic group, with no significant difference observed between the groups (P = .698). Similarly, BMI values were comparable between the robotic group (18.88 ± 6.31 kg/m2) and the laparoscopic group (19.51 ± 5.91 kg/m2) (P = .595).
The mean duration of the procedure was markedly longer in the robotic group (3.92 ± 1.22 hours) compared with the laparoscopic group (1.41 ± 0.70 hours) (P < .001). Likewise, the average length of postoperative hospitalization was significantly extended in the robotic cohort (6.08 ± 4.11 days) relative to the laparoscopic cohort (2.30 ± 2.13 days) (P < .001) (Table 2).
Age, BMI, Duration of Surgery, and Length of Hospital Stay During Surgery for Both Groups
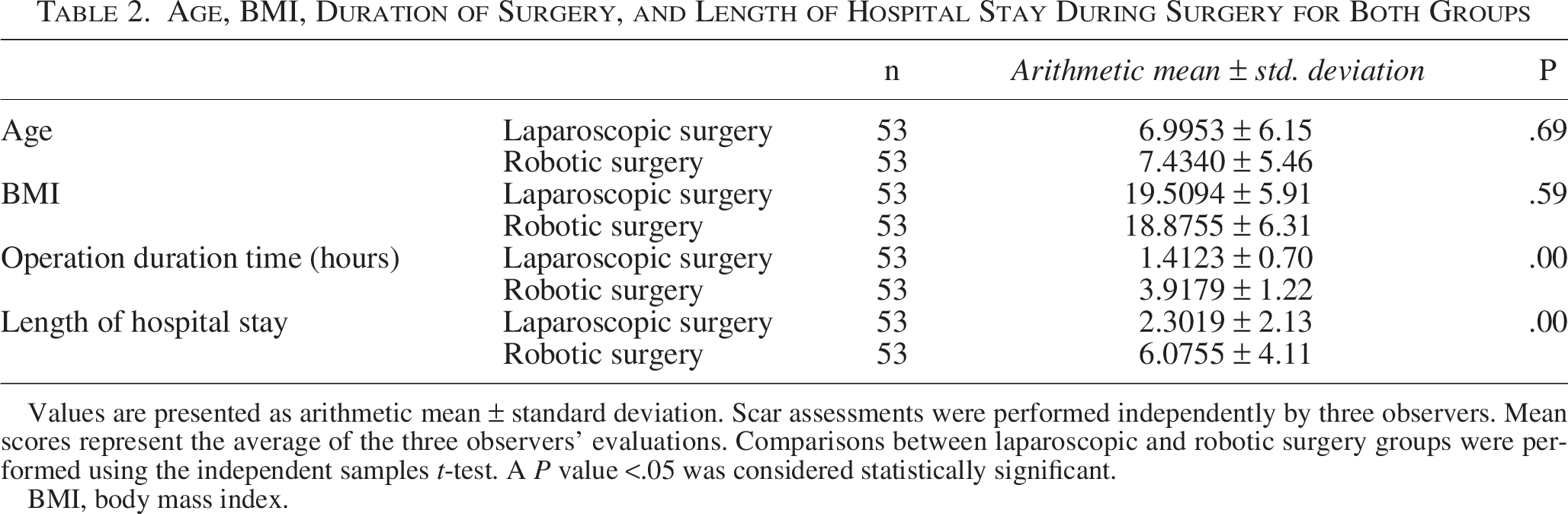
Values are presented as arithmetic mean ± standard deviation. Scar assessments were performed independently by three observers. Mean scores represent the average of the three observers’ evaluations. Comparisons between laparoscopic and robotic surgery groups were performed using the independent samples t-test. A P value <.05 was considered statistically significant.
BMI, body mass index.
The results of the scar assessment revealed considerable variability between the two surgical approaches. Regarding the Manchester Scar Scale (MSS), all three evaluators documented scores indicating statistically significant differences between the robotic and laparoscopic groups (all P < .001). When averaged across evaluators, the mean MSS score was markedly higher in the robotic group (6.52 ± 1.25) compared with the laparoscopic group (5.98 ± 0.91) (P = .013).
Furthermore, analysis of the Modified Scar-Rating Scale (MSRS) showed significantly higher scores in the robotic cohort. The mean MSRS score among evaluators was 7.10 ± 1.18 for the robotic group and 6.05 ± 1.22 for the laparoscopic group, indicating a statistically significant difference between the two groups (P < .001) (Table 1).
Upon evaluation of the incision scars, no statistically significant difference was observed between the port scars of the suspended robotic arms and those of the nonsuspended assistant arm concerning MSS and MSRS scores (P = .917).
The interrater reliability analysis revealed notable discrepancies between the two surgical techniques. Specifically, for MSS, interrater agreement was limited in the laparoscopic group (ICC = 0.20), whereas it exhibited moderate-to-high reliability in the robotic group (ICC = 0.81). Conversely, MSRS demonstrated satisfactory interrater reliability across both groups, with ICCs of 0.81 in the laparoscopic cohort and 0.78 in the robotic cohort.
Discussion
This investigation constitutes the initial assessment of the progression of hypertrophic port-site scars following pediatric robotic procedures. The findings suggest that the probability of hypertrophic wound healing is significantly elevated after pediatric robotic interventions. An examination of the English-language scholarly literature reveals a scarcity of studies on port-site wound healing after laparoscopic surgery, even in adult populations. It is widely recognized that a principal advantage of minimally invasive surgery is its superior cosmetic outcome results.7,8
Multiple systemic, local, and genetic factors have been identified as catalysts of hypertrophic scar formation. These include single-nucleotide polymorphisms, cytokines, and growth factors. Such factors delay wound healing and prolong its duration beyond normal expectations. Nonetheless, the precise pathological etiology remains unidentified and requires further investigation. Because the underlying cause of impaired wound healing remains unidentified, a standardized treatment protocol for wound healing has not yet been established.9,10 The absorbable suture was compared with cyanoacrylate tissue adhesive and a strip for the closure of 5 mm trocar sites. It was reported that, although the mean closure time for the absorbable suture was longer, it was cosmetically superior and satisfactory.
In our patients, a fine, absorbable (5/0) suture was used to close the port-site incision. Furthermore, the suture material and technique were consistent across all patients. However, the use of fine, absorbable sutures and subcutaneous repair did not prevent the formation of hypertrophic scars.
Multiple experimental studies on postoperative intra-abdominal adhesions have shown that reducing the pneumoperitoneum pressure to 8–10 mmHg significantly diminishes the occurrence of postoperative adhesions. In our studies, a pressure of 10 mmHg was utilized during pneumoperitoneum. However, this modification did not inhibit the development of hypertrophic scars.11,12
In robotic-assisted laparoscopic surgery, the robotic arms are suspended and securely affixed to the robotic system to facilitate a broader intra-abdominal visual field. This suspension method inevitably exerts compression on the surrounding tissues (Fig. 3). Initially, it was hypothesized that the impaired scar healing observed in our patients was attributable to compression of the tissue by the suspension. Nevertheless, the observation of similarly poor scar outcomes at the assistant port—which is not connected to the robotic system and hence not suspended—challenged this hypothesis. In accordance with this finding, statistical analysis revealed no significant difference in scar characteristics between the robotic and assistant ports within the same patient (P = .917).
Although hypertrophic scarring may be partially attributable to localized compression from suspended robotic arms, the lack of a discernible difference between scars at robotic and assistant port sites suggests a more generalized biological response. It is postulated that mechanical stress associated with suspension could induce a systemic or regional wound-healing response, thereby indirectly affecting the assistant port. The current findings suggest that scar development may be associated not only with local pressure related to suspension but also with broader surgical and mechanical factors particular to robotic surgery. This hypothesis requires further investigation and could be validated through experimental animal models or studies involving larger patient cohorts.13–15
The principal limitations of this study are the restricted patient population and the retrospective study design. The retrospective nature and the relatively small sample size serve as primary constraints that limit the generalizability of the findings. Furthermore, variability in the surgical procedures performed and differences in their durations further reduce the applicability of the results. Nevertheless, it is posited that evaluating the nutritional status of pediatric patients, such as through BMI, yields a more accurate assessment than comparing the effects of various surgical interventions, including gastroesophageal reflux surgery, vesicoureteric reflux surgery, and pyeloplasty, on the surgical incision. Therefore, further research is necessary, involving larger patient populations, more homogeneous surgical groups, and standardized parameters such as developmental delay and BMI.
One of the most significant limitations of this study is the heterogeneity observed between the robotic-assisted and conventional laparoscopic surgery groups. Although no statistically significant differences were observed in age, sex, or BMI—indicating homogeneous selection with respect to fundamental demographic characteristics—there were notable disparities in surgical procedure duration.
These differences introduce potential confounding patient-related factors that could influence the duration of surgery, tissue processing, and scar formation. A matched analysis of procedures might have offered a more homogeneous comparison; however, the limited number of matched procedures hindered sufficiently powered subgroup analyses. Consequently, the observed differences in scar outcomes may partially reflect underlying differences in procedures and clinics rather than differences in the surgical system. Therefore, the results should be interpreted with caution.
Patients in the robotic surgery group frequently exhibited growth retardation, scoliosis, or decreased lower body mass, which influenced the selection of surgical procedures. Conversely, patients in the laparoscopic group, such as those undergoing cholecystectomy or surgeries for ovarian pathologies, were generally better nourished; this factor may have positively impacted wound-healing outcomes. One of the limitations of this study is the variation in trocar diameters between the robotic and laparoscopic cohorts. In the robotic group, procedures were conducted utilizing the da Vinci Si Surgical System (Intuitive Surgical, Sunnyvale, CA, USA), which necessitated a 12 mm camera trocar, two 8 mm working trocars, and an 11 mm assistant trocar. Conversely, laparoscopic procedures employed a 10 mm camera trocar and 5 mm working trocars. This discrepancy in port size constitutes a structural difference between the two methodologies and may have impacted the development of hypertrophic scarring. Future prospective studies utilizing newer-generation robotic platforms capable of accommodating smaller-diameter camera and working ports are warranted to better isolate the effect of the surgical approach on scar outcomes. Furthermore, operative times were notably longer in the robotic surgery cohort, constituting an additional source of heterogeneity and a potential confounder in the interpretation of scar-related outcomes. These considerations should be considered when assessing the results and regarding the limited generalizability of the findings.
Conclusions
In conclusion, robotic surgery in pediatric patients within this cohort was associated with hypertrophic scar formation at the port sites. two 8 mm trocars. To generalize the findings of this study, a larger patient cohort and the use of immunohistochemical techniques are recommended to elucidate the mechanisms underlying hypertrophic scar development following robotic surgery.
Declaration
Data of this research have not been presented or published elsewhere before.
Authors’ Contributions
Concept or design: G.B.B., S.E.Ü.B., and S.D. Acquisition of data: İ.Y., G.K., and Ö.E.C. Analysis or interpretation of data: H.E.A., S.E.Ü.B., Ö.E.C., and G.B.B. Drafting of the article: S.D., S.E.Ü.B., G.B.B., İ.S., and O.M.Ç. Critical revision for important intellectual content: S.D. and İ.S. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Footnotes
Disclosure Statement
All authors have disclosed no conflicts of interest.
Funding Information
No funding was received for conducting this study.