
Abstract
Background:
Mesh fixation strategy is a modifiable intraoperative factor that may influence postoperative recovery following totally extraperitoneal (TEP) inguinal hernia repair. Although self-fixating meshes were developed to avoid penetrating fixation and potentially reduce pain, their effect on multidimensional recovery trajectories remains unclear.
Methods:
This retrospective cohort study included consecutive adults undergoing elective unilateral TEP repair at a tertiary referral center. Patients were grouped according to fixation strategy: self-fixating mesh or polypropylene mesh secured with absorbable tacks. The primary outcome was early quality of recovery measured using the Quality of Recovery-15 (QoR-15) questionnaire at postoperative week 1. Secondary outcomes included longitudinal QoR-15 and visual analog scale (VAS) pain scores at postoperative months 1 and 3, analgesic consumption, and time to functional recovery. Recovery trajectories were analyzed using linear mixed-effects models, with additional stratification by defect size (<20 mm versus ≥20 mm).
Results:
A total of 134 patients were included (56 tack fixation, 78 self-fixating mesh). Early recovery at week 1 was comparable between groups. Mixed-effects modeling demonstrated significant improvement over time in both groups, without an independent association between fixation strategy and overall QoR-15 trajectory. However, in defects ≥20 mm, self-fixating mesh was associated with higher QoR-15 scores. Pain scores improved over time in both groups, with small but statistically significant differences favoring self-fixating mesh.
Conclusions:
In unilateral TEP repair, fixation strategy does not substantially influence overall early and short-term recovery. However, in larger defects (≥20 mm), self-fixating mesh may provide modest recovery advantages, suggesting a context-dependent rather than uniform effect.
Keywords
Introduction
Inguinal hernia repair is one of the most commonly performed surgical procedures worldwide, with the totally extraperitoneal (TEP) approach increasingly favored because of its association with reduced postoperative pain, faster recovery, and lower wound-related complication rates compared with open techniques.1,2 Despite these advantages, postoperative discomfort and delayed functional recovery remain clinically relevant concerns, particularly during the early postoperative period when patients resume daily activities and return to work. In this context, early recovery outcomes are particularly important in laparoscopic inguinal hernia surgery, where rapid functional restoration is a key advantage of the minimally invasive approach.
Mesh fixation technique represents a key modifiable factor that may influence early postoperative outcomes after TEP repair. 3 Conventional fixation using tacks provides secure mesh anchorage but has been associated with increased postoperative pain, likely related to nerve irritation, periosteal injury, and inflammatory response.4,5 In contrast, self-fixating meshes were developed to eliminate the need for mechanical fixation while maintaining adequate mesh stability, potentially reducing tissue trauma and postoperative pain. 6
While several studies have compared pain outcomes between different mesh fixation strategies, pain alone may not fully capture the multidimensional nature of postoperative recovery. 7 Consequently, the concept of quality of recovery (QoR) has emerged as a comprehensive patient-reported outcome measure encompassing physical comfort, emotional state, functional independence, and pain. 8 The 15-item Quality of Recovery score (QoR-15) is a validated and widely used instrument for assessing early postoperative recovery and has demonstrated strong psychometric properties across a broad range of surgical populations. 9
However, data specifically focusing on early quality of recovery following TEP inguinal hernia repair remain limited. 10 Moreover, unilateral and bilateral repairs are frequently analyzed together, despite the potential confounding effects of additional dissection and mesh fixation on postoperative recovery outcomes. 10 Restricting the analysis to unilateral TEP repairs may therefore allow a more accurate assessment of the true impact of mesh fixation technique on postoperative recovery.
The aim of this study was to compare early quality of recovery following unilateral TEP inguinal hernia repair between patients treated with self-fixating mesh and those undergoing tack fixation. We hypothesized that the use of self-fixating mesh would be associated with improved early quality of recovery and faster functional return compared with tack fixation.
Additionally, standardized preoperative ultrasonography and intraoperative technical variables were incorporated to allow a more refined evaluation of fixation-related recovery differences.
Methods
Study design and setting
This retrospective cohort study was conducted at a tertiary referral center and included consecutive adult patients who underwent elective unilateral TEP inguinal hernia repair between March 2021 and October 2025. The study was designed to evaluate postoperative recovery trajectories and the potential impact of mesh fixation strategy within a homogeneous unilateral cohort in order to minimize procedural and anatomical confounding associated with bilateral repairs.
Only patients with primary unilateral inguinal hernias were eligible. Patients with bilateral hernias, recurrent hernias, femoral-only repairs, emergency procedures, conversion to open surgery, non-TEP techniques, or concomitant abdominal procedures were excluded. Patients with incomplete perioperative data or unavailable postoperative patient-reported outcome measures were excluded from respective analyses.
All patients underwent standardized preoperative ultrasonography in standing position with Valsalva maneuver. Hernia type and maximal defect size were recorded in millimeters to ensure objective and reproducible characterization of defect morphology.
Patients were grouped according to intraoperative fixation strategy:
All procedures were performed by three experienced laparoscopic surgeons within the same institution (K.I., K.T., and B.T.). Although multiple surgeons contributed to the cohort, all adhered to a standardized three-port TEP technique protocol, thereby minimizing inter-operator variability.
Surgical technique
The preperitoneal space was created using a standardized approach, followed by systematic dissection of the myopectineal orifice and reduction of the hernia sac. Mesh size selection was based on intraoperative assessment of defect extent. In the tack fixation group, absorbable tacks were applied with careful avoidance of known neurovascular risk zones. No additional local anesthetic infiltration was administered at trocar or fixation sites in either group in order to reduce postoperative analgesic confounding.
Operative time (skin incision to closure), mesh size, and intraoperative hernia classification (direct, indirect, femoral, pantaloon) were prospectively recorded in the institutional database.
Outcome measures
The primary outcome was early postoperative quality of recovery assessed using the validated QoR-15 questionnaire at postoperative week 1.
Secondary outcomes included QoR-15 at postoperative month 1 and month 3, visual analog scale (VAS) pain scores at week 1, month 1, and month 3, analgesic consumption, time to return to daily activities, time to return to work, and early postoperative complications (Clavien–Dindo classification).
QoR and pain outcomes were collected using structured postoperative questionnaires. Postoperative patient-reported outcomes (QoR-15 and VAS) were collected through standardized follow-up protocols routinely implemented at our institution. These data were obtained either during scheduled outpatient visits or through structured telephone interviews conducted by trained clinical staff. The same standardized questionnaire format was used across all time points to ensure consistency of data collection.
Rationale for defect-size stratification
Because larger hernia defects may require wider preperitoneal dissection and greater mesh deployment area—potentially amplifying fixation-related tissue effects—additional analyses were stratified according to maximal defect size (<20 mm versus ≥20 mm). This stratification was performed to explore whether fixation-related recovery differences may be context-dependent rather than uniform across all defect sizes.
Handling of missing data
Patient-reported outcomes were not available for all patients at each time point. Analyses were therefore performed using a complete-case approach for each respective outcome. Baseline characteristics of responders and nonresponders were compared with assess potential nonresponder bias. No data imputation was performed, as missingness was assessed to be nondifferential between fixation groups.
Statistical analysis
Statistical analyses were performed using R statistical software (R Foundation for Statistical Computing, Vienna, Austria).
Continuous variables were assessed for normality using the Shapiro–Wilk test. As most outcome variables demonstrated non-normal distributions, non-parametric methods were used for unadjusted comparisons. Continuous variables are presented as median and interquartile range (IQR) and were compared using the Wilcoxon rank-sum test. Categorical variables were compared using the chi-square or Fisher’s exact test as appropriate.
Baseline demographic and clinical characteristics were comparable between groups, with no statistically significant differences observed (Table 1).
Baseline Demographic and Clinical Characteristics of Patients Undergoing Unilateral Totally Extraperitoneal Inguinal Hernia Repair According to Mesh Fixation Strategy
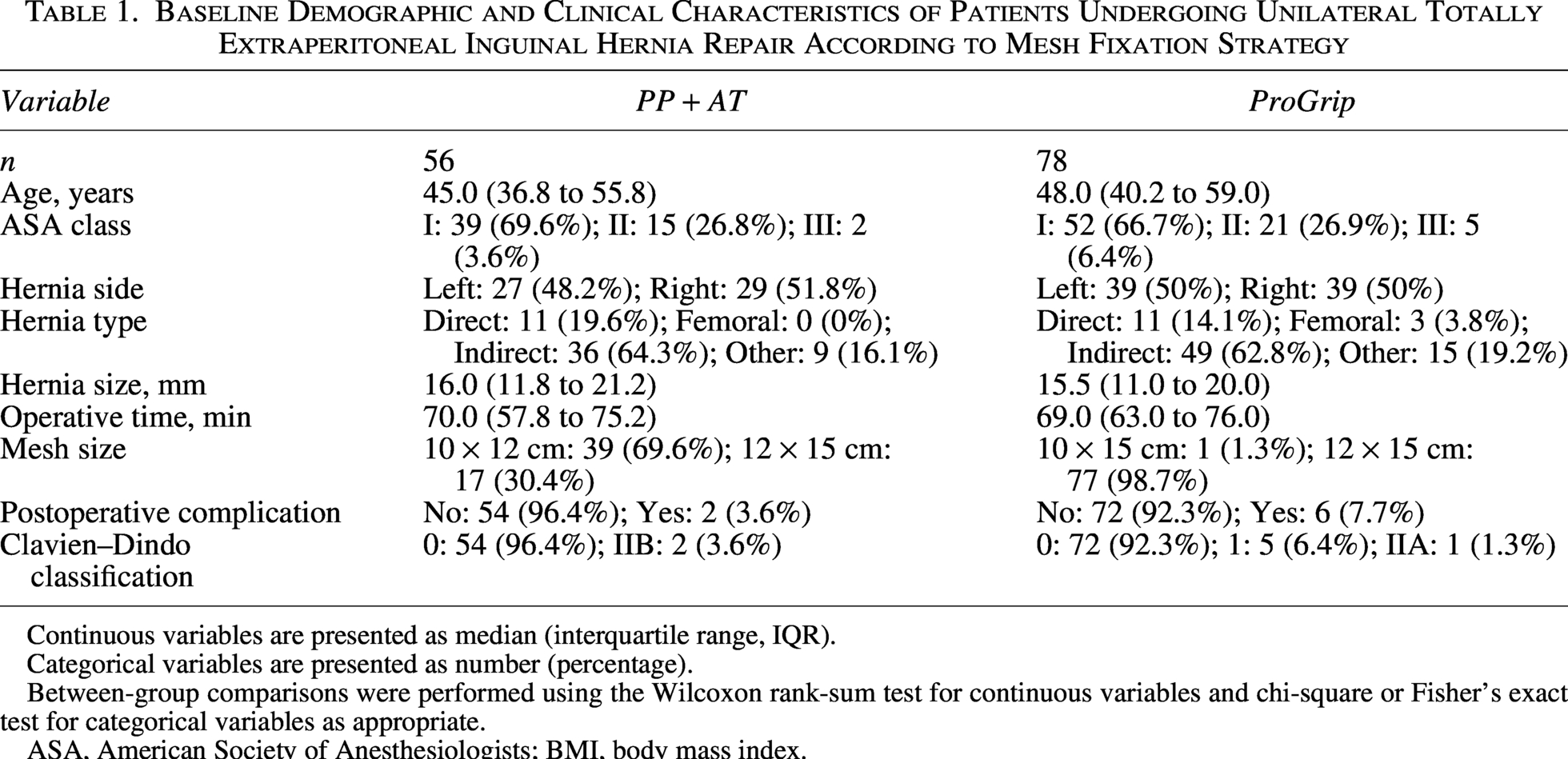
Continuous variables are presented as median (interquartile range, IQR).
Categorical variables are presented as number (percentage).
Between-group comparisons were performed using the Wilcoxon rank-sum test for continuous variables and chi-square or Fisher’s exact test for categorical variables as appropriate.
ASA, American Society of Anesthesiologists; BMI, body mass index.
Unadjusted postoperative recovery and functional outcomes are summarized in Table 2.
Unadjusted Postoperative Recovery, Pain, and Functional Outcomes following Unilateral Totally Extraperitoneal Inguinal Hernia Repair according to Mesh Fixation Strategy
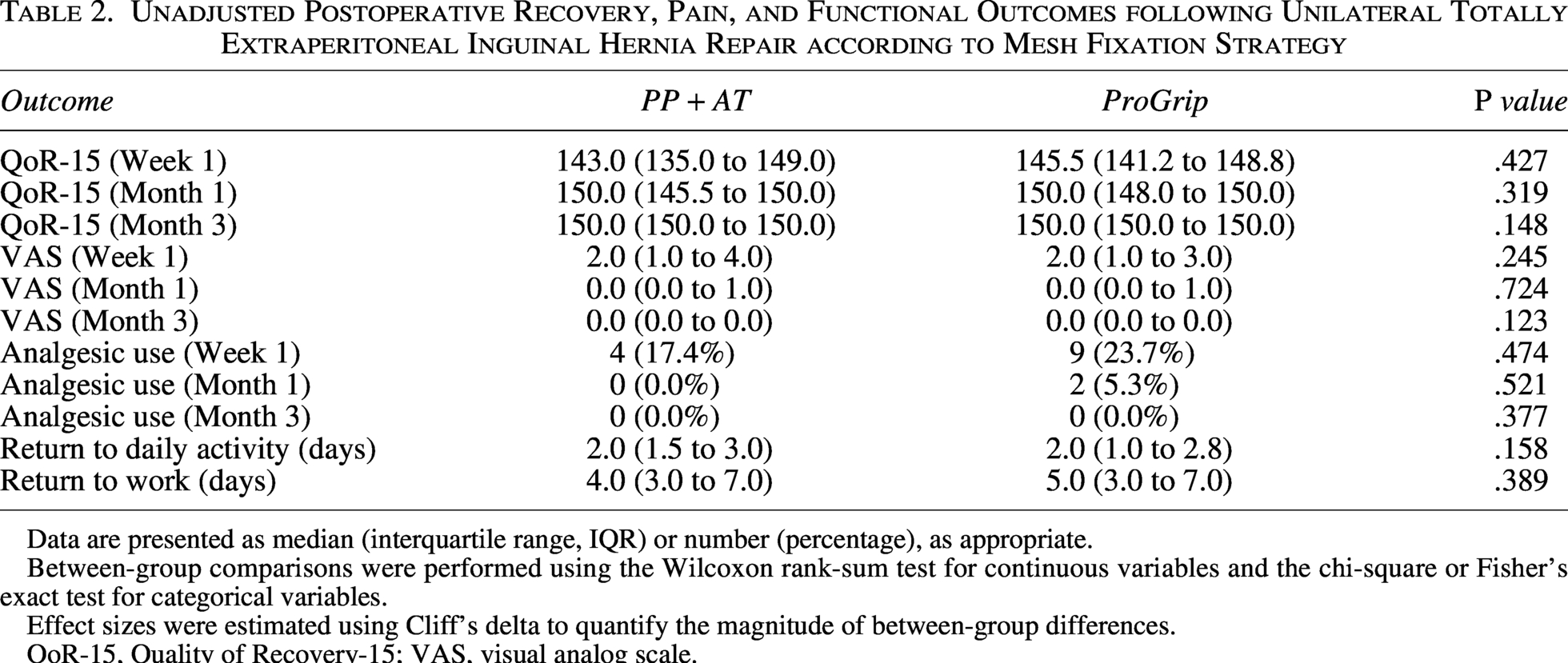
Data are presented as median (interquartile range, IQR) or number (percentage), as appropriate.
Between-group comparisons were performed using the Wilcoxon rank-sum test for continuous variables and the chi-square or Fisher’s exact test for categorical variables.
Effect sizes were estimated using Cliff’s delta to quantify the magnitude of between-group differences.
QoR-15, Quality of Recovery-15; VAS, visual analog scale.
To complement P values and assess clinical relevance, effect sizes were estimated using Cliff’s delta for nonparametric comparisons.
Longitudinal modeling of recovery trajectories
To evaluate recovery trajectories across postoperative week 1, month 1, and month 3, linear mixed-effects models were constructed with patient-level random intercepts to account for within-subject correlation.
Fixed effects included:
Time (categorical: week 1, month 1, month 3). Fixation strategy. Interaction between time and fixation strategy.
Results of the mixed-effects analysis for QoR-15 and VAS trajectories are presented in Tables 3 and 4, respectively. Graphical representations of longitudinal QoR-15 and VAS trajectories are shown in Figures 1 and 2, respectively.

Longitudinal trajectory of Quality of Recovery-15 (QoR-15) scores by fixation method over time. Points represent model-based estimated marginal means from a linear mixed-effects model with patient ID as random intercept; error bars indicate 95% confidence intervals.
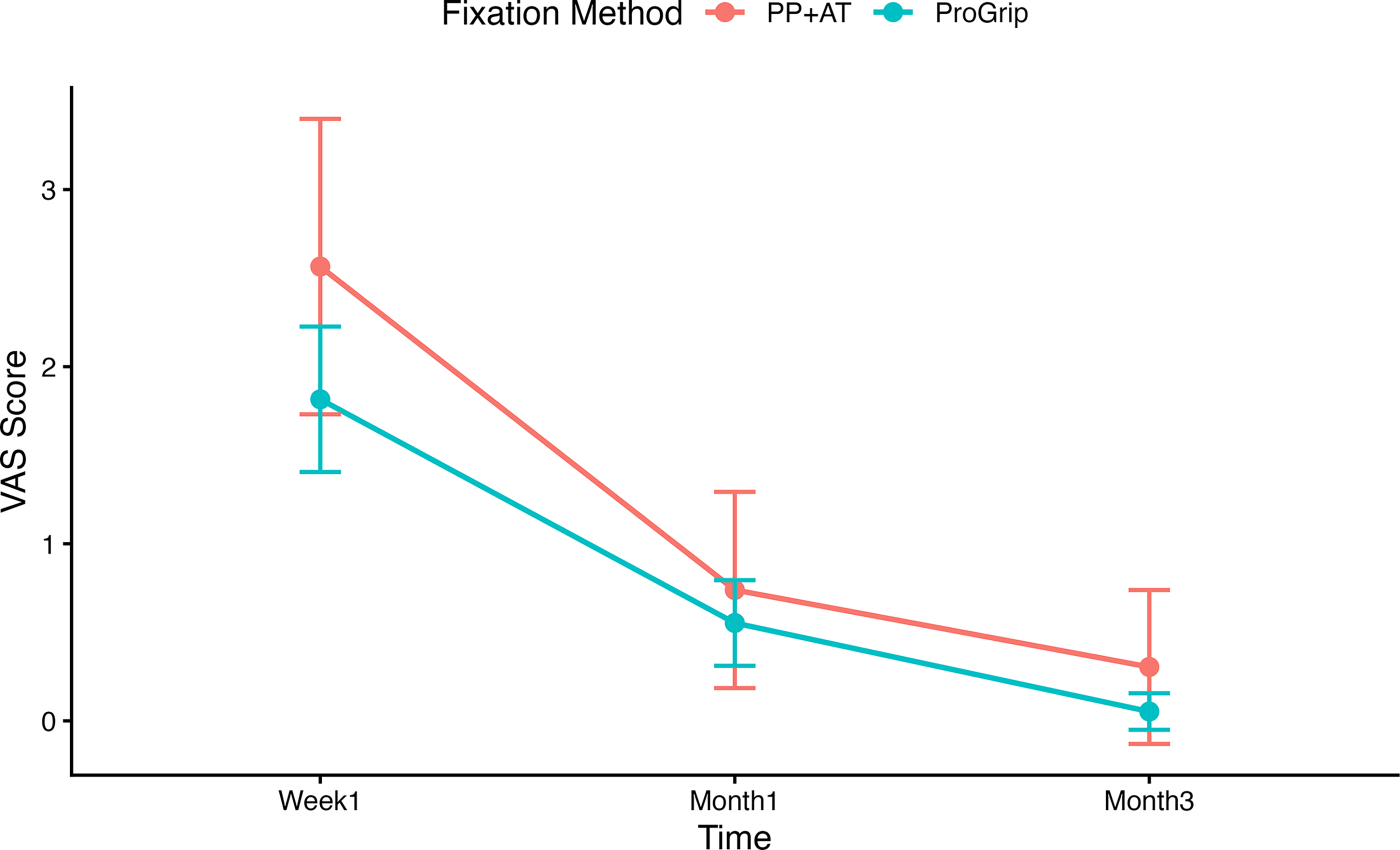
Longitudinal trajectory of postoperative pain (VAS) by fixation method over time. Points represent model-based estimated marginal means from a linear mixed-effects model; error bars indicate 95% confidence intervals. VAS, visual analog scale.
Linear Mixed-Effects Model Evaluating Longitudinal QoR-15 Recovery Trajectory in the Overall Cohort
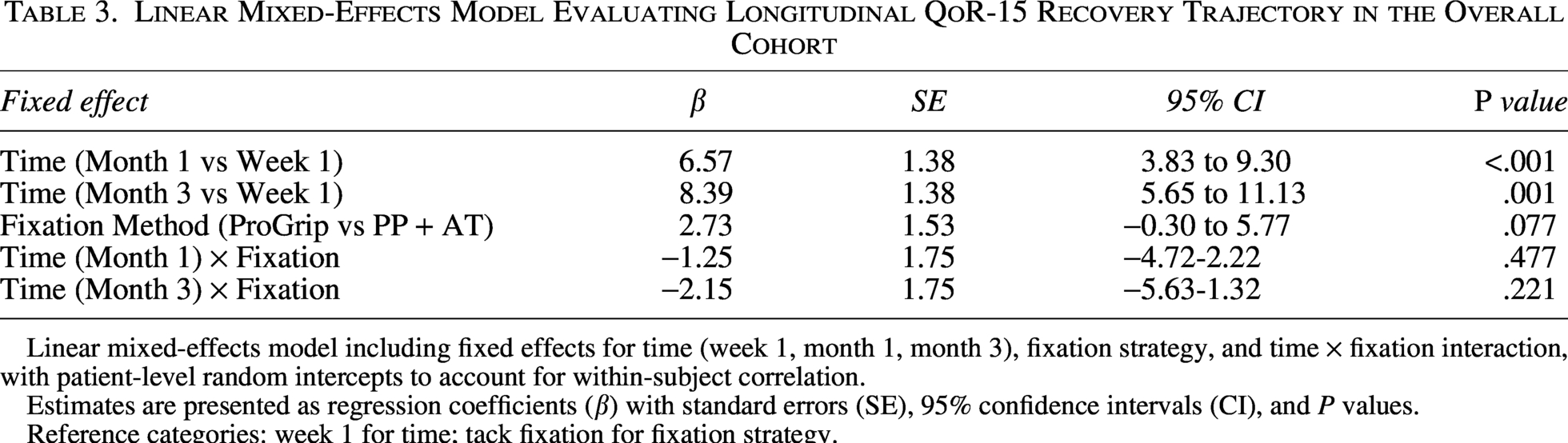
Linear mixed-effects model including fixed effects for time (week 1, month 1, month 3), fixation strategy, and time × fixation interaction, with patient-level random intercepts to account for within-subject correlation.
Estimates are presented as regression coefficients (β) with standard errors (SE), 95% confidence intervals (CI), and P values.
Reference categories: week 1 for time; tack fixation for fixation strategy.
Linear Mixed-Effects Model Evaluating Longitudinal VAS Pain Trajectory in the Overall Cohort
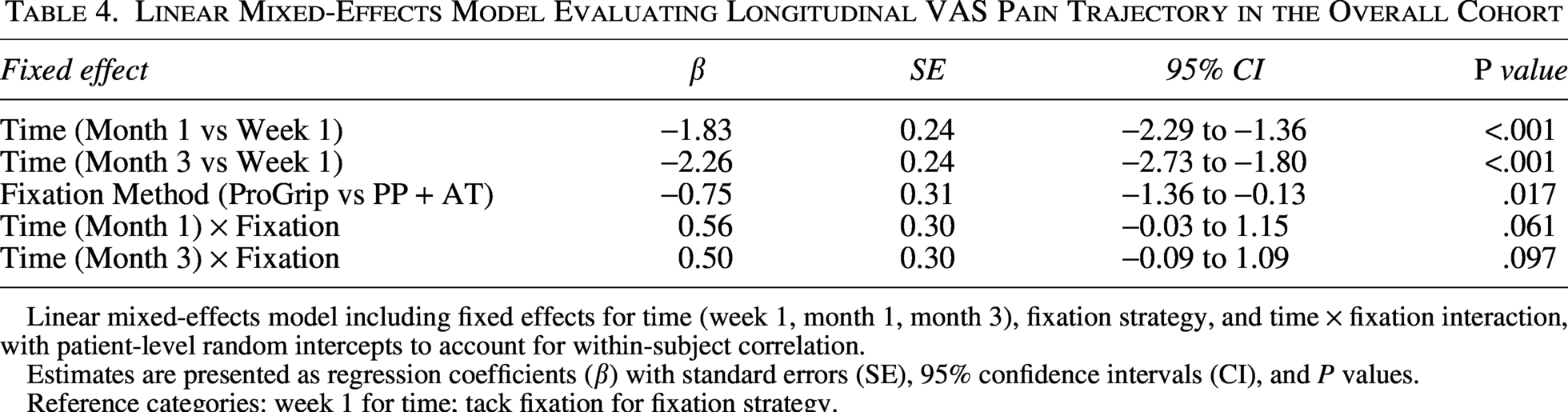
Linear mixed-effects model including fixed effects for time (week 1, month 1, month 3), fixation strategy, and time × fixation interaction, with patient-level random intercepts to account for within-subject correlation.
Estimates are presented as regression coefficients (β) with standard errors (SE), 95% confidence intervals (CI), and P values.
Reference categories: week 1 for time; tack fixation for fixation strategy.
Model assumptions were evaluated through residual diagnostics and inspection of random-effects distributions.
Defect-size–stratified and interaction analyses
Additional mixed-effects models were constructed separately for defect size subgroups (<20 mm and ≥20 mm) to evaluate potential context-dependent fixation effects. Subgroup-specific models are provided in Tables 5 and 6.
Linear Mixed-Effects Model for Longitudinal QoR-15 Recovery Trajectory in Patients with Hernia Defects < 20 mm
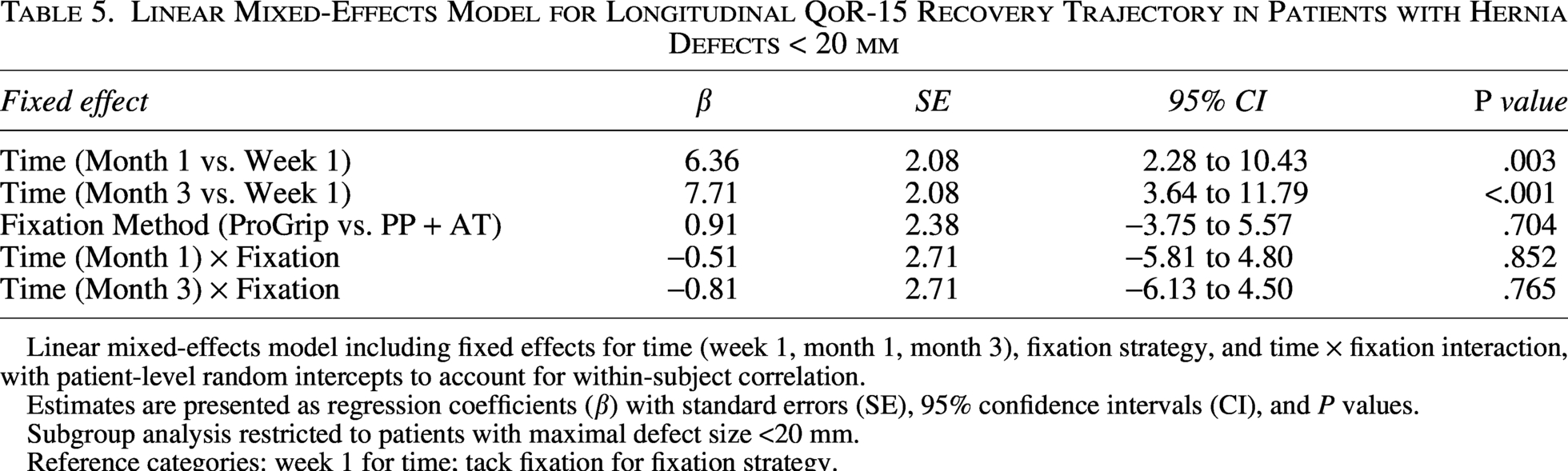
Linear mixed-effects model including fixed effects for time (week 1, month 1, month 3), fixation strategy, and time × fixation interaction, with patient-level random intercepts to account for within-subject correlation.
Estimates are presented as regression coefficients (β) with standard errors (SE), 95% confidence intervals (CI), and P values.
Subgroup analysis restricted to patients with maximal defect size <20 mm.
Reference categories: week 1 for time; tack fixation for fixation strategy.
Linear Mixed-Effects Model for Longitudinal QoR-15 Recovery Trajectory in Patients with Hernia Defects ≥20 mm
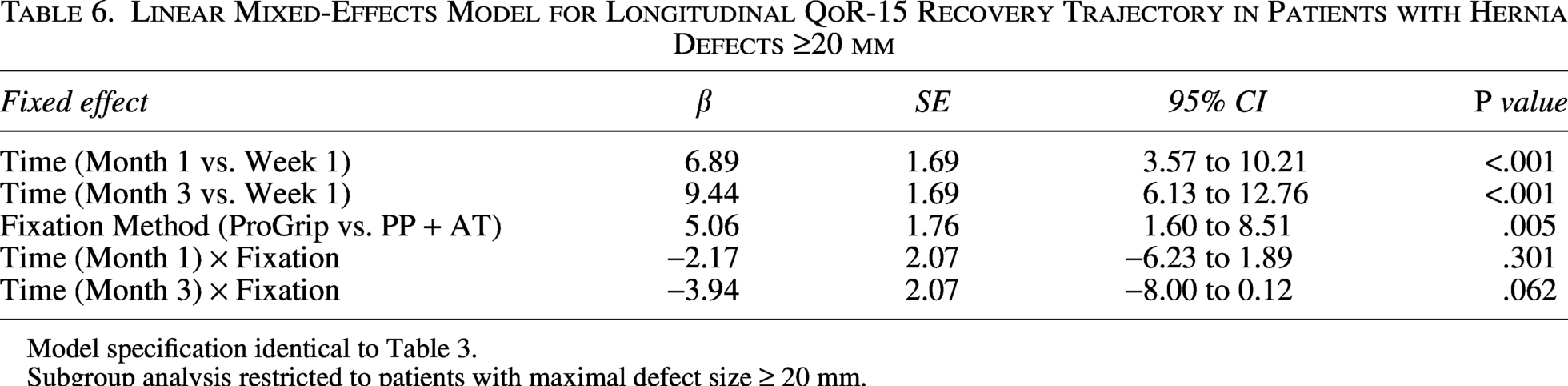
Model specification identical to Table 3.
Subgroup analysis restricted to patients with maximal defect size ≥ 20 mm.
Furthermore, three-way interaction models incorporating time, fixation strategy, and defect size were developed to explore potential effect modification. These analyses are presented in Supplementary Tables S1 and S2.
A two-sided P value <.05 was considered statistically significant.
Ethical approval
The study was approved by the Ege University Medical Research Ethics Committee (Approval No: 25-12.1T/19; Date: 18 December 2025) and conducted in accordance with the Declaration of Helsinki. Due to the retrospective nature of the study, written informed consent was waived.
This observational study was reported in accordance with the STROBE guidelines. 11
Results
Patient characteristics
A total of 134 patients undergoing unilateral TEP inguinal hernia repair were included in the final cohort, comprising 56 patients in the tack fixation (PP + AT) group and 78 patients in the self-fixating mesh (ProGrip) group.
Baseline demographic and clinical characteristics were comparable between groups, including age, ASA classification, hernia type, hernia side, defect size, operative time, and postoperative complication rates (Table 1). No statistically significant baseline imbalances were identified.
Unadjusted postoperative outcomes
At postoperative week 1, QoR-15 scores were similar between fixation groups (median 143.0 [IQR 135.0–149.0] versus 145.5 [141.2–148.8], P = .427) (Table 2). Similarly, VAS pain scores at week 1 did not differ significantly between groups (P = .245).
At postoperative months 1 and 3, both QoR-15 and VAS scores improved substantially in both groups, with no significant differences observed in unadjusted comparisons (Table 2). Functional recovery outcomes, including time to return to daily activities and return to work, were also comparable.
These findings suggested similar early and short-term recovery in the overall cohort when assessed using conventional unadjusted comparisons.
Longitudinal recovery trajectories
To further characterize recovery dynamics over time, linear mixed-effects models were constructed.
For QoR-15, significant improvement over time was observed in the overall cohort (Table 3). Compared with postoperative week 1, QoR-15 scores increased significantly at month 1 and month 3 (both P < .001). However, fixation strategy was not independently associated with the overall QoR-15 recovery trajectory in the full cohort (P = .077), and no significant time–fixation interaction was detected. The longitudinal QoR-15 trajectories are illustrated in Figure 1.
For VAS pain scores, significant improvement over time was similarly observed (P < .001) (Table 4). In contrast to QoR-15, fixation strategy demonstrated a small but statistically significant independent association with lower VAS scores favoring self-fixating mesh in the adjusted mixed-effects model (P = .017) (Table 4). No significant time–fixation interaction was identified. Pain trajectories are shown in Figure 2.
Defect-Size–stratified analyses
When stratified by maximal defect size, distinct patterns emerged. Stratified mixed-effects models for defects < 20 mm and ≥20 mm are shown in Tables 5 and 6, respectively.
In patients with smaller defects (<20 mm), fixation strategy was not associated with differences in QoR-15 recovery trajectories.
In contrast, among patients with larger defects (≥20 mm), self-fixating mesh was independently associated with higher QoR-15 scores in the mixed-effects model (P = .005). Although time–fixation interaction terms did not reach statistical significance, the magnitude of the fixation effect was greater in this subgroup, suggesting a context-dependent influence of fixation strategy in larger defects.
Three-way interaction models incorporating time, fixation strategy, and defect size are presented in Supplementary Tables S1 and S2. Nevertheless, the subgroup findings support the hypothesis that defect size may modulate fixation-related recovery effects.
Subgroup-specific VAS trajectories according to defect size are illustrated in Figure 3.
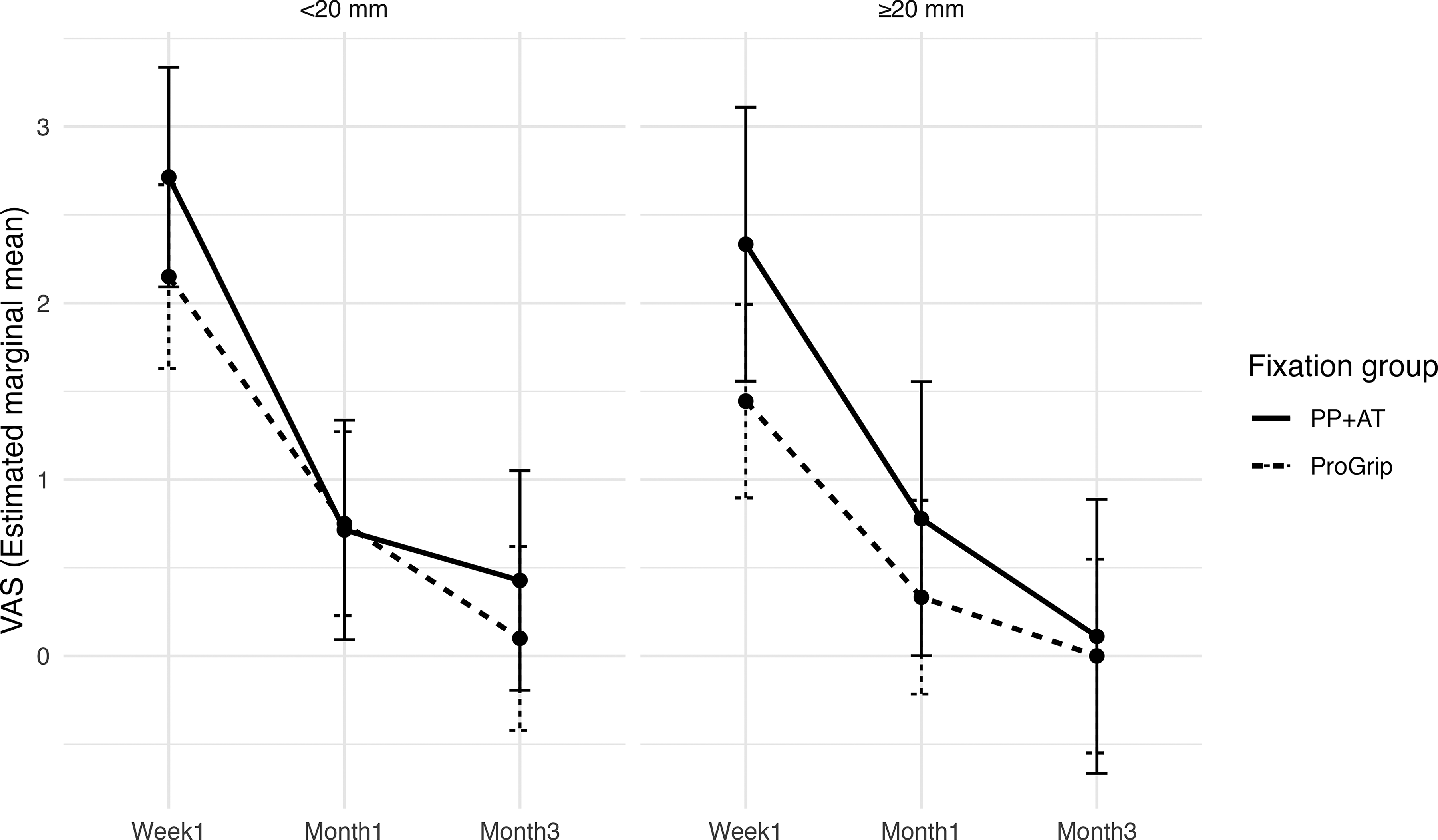
Subgroup analysis of longitudinal postoperative pain (VAS) trajectories stratified by hernia defect size (<20 mm versus ≥20 mm) according to fixation method.
Summary of findings
Overall, longitudinal modeling confirmed significant recovery improvement over time in all patients. In the general cohort, fixation strategy did not materially influence QoR-15 recovery trajectory. However, in patients with larger defects (≥20 mm), self-fixating mesh was associated with improved recovery scores. Pain outcomes demonstrated a modest independent association favoring self-fixating mesh, although clinical differences were small.
Discussion
In this retrospective cohort study, we evaluated recovery trajectories following unilateral TEP inguinal hernia repair using self-fixating mesh versus polypropylene mesh secured with absorbable tacks. Our findings demonstrate that overall postoperative recovery improves significantly over time in all patients, with no substantial difference in global QoR-15 recovery trajectory between fixation strategies in the general cohort. However, defect-size–stratified analyses revealed that in patients with larger hernia defects (≥20 mm), self-fixating mesh was independently associated with higher recovery scores, suggesting that the impact of fixation strategy may be context-dependent rather than uniform across all patients.
Several previous studies comparing fixation techniques in laparoscopic inguinal hernia repair have primarily focused on postoperative pain as the principal outcome. 12 While pain remains clinically important, it represents only one dimension of postoperative recovery. The QoR-15 instrument provides a broader, multidimensional assessment of recovery, encompassing physical comfort, emotional state, and functional independence. In this context, the present findings extend prior work by evaluating not only early recovery at a single time point but longitudinal recovery trajectories using mixed-effects modeling.
Consistent with prior literature on patient-reported outcomes following groin hernia repair, 13 overall recovery in our cohort was favorable, with progressive improvement from week 1 to months 1 and 3. Importantly, longitudinal modeling demonstrated that time was the dominant determinant of recovery, underscoring the natural postoperative course after minimally invasive TEP repair. In the overall cohort, fixation strategy was not independently associated with QoR-15 trajectory, and no significant time–fixation interaction was observed. These findings support the interpretation that, in routine unilateral TEP repair, fixation method does not materially alter global short-term recovery. 14
However, subgroup analyses revealed a more nuanced pattern. In patients with larger hernia defects (≥20 mm), self-fixating mesh was associated with significantly higher QoR-15 scores in adjusted models. Although interaction terms did not reach statistical significance, the magnitude and consistency of the subgroup effect suggest potential biological plausibility. Larger defects typically require wider preperitoneal dissection and greater mesh coverage area, potentially increasing tissue manipulation and fixation surface. In such settings, avoidance of penetrating fixation may reduce local tissue trauma or mechanical irritation, thereby favorably influencing early recovery. This observation aligns with the concept that fixation-related effects may be more pronounced in anatomically extensive repairs rather than in smaller, limited defects. Notably, the defect-size–stratified analysis represents a key strength of the present study. The significant association observed in defects ≥20 mm suggests that fixation-related effects may only become clinically relevant beyond a certain anatomical threshold. This finding provides a more nuanced interpretation compared with prior studies that evaluated fixation strategies in unselected populations and may help explain previously inconsistent results in the literature.
With respect to postoperative pain, our longitudinal analysis demonstrated significant improvement over time in both groups. In adjusted mixed-effects models, fixation strategy showed a small but statistically significant association with lower VAS scores favoring self-fixating mesh. Previous investigations have implicated penetrating fixation devices in nerve irritation and chronic postoperative pain.15,16 While the present study did not assess long-term chronic pain outcomes, the modest independent association observed in early pain trajectories may reflect reduced mechanical fixation-related tissue interaction. Nevertheless, the clinical magnitude of this difference was small and should be interpreted cautiously. 17
Functional recovery outcomes, including return to daily activities and return to work, were comparable between groups, consistent with prior comparative studies of laparoscopic fixation strategies. 18 These findings reinforce the concept that both fixation methods are safe and effective in routine unilateral TEP repair.
From an economic perspective, demonstration of broadly comparable recovery outcomes may justify the selection of a fixation technique based on resource availability and institutional cost structures.19,20 However, as no formal cost-effectiveness analysis was performed, these implications remain exploratory and hypothesis-generating.
Several limitations warrant consideration. First, the retrospective design precludes randomization and introduces potential selection bias. 21 Second, although longitudinal modeling was applied, the sample size remains modest, particularly for subgroup analyses. Third, QoR-15 scores approached the upper limit at later follow-up points, raising the possibility of a ceiling effect that may attenuate detectable differences between groups. Fourth, long-term outcomes such as chronic pain were not evaluated. Finally, subgroup and interaction analyses should be interpreted as exploratory, requiring confirmation in prospective studies.
Another important consideration is hernia recurrence, which was not evaluated in the present study due to the short-term follow-up design. Previous studies have demonstrated that mesh fixation strategy does not significantly influence recurrence rates in laparoscopic inguinal hernia repair when adequate mesh overlap is achieved. Therefore, the recovery differences observed in our study should be interpreted independently from long-term recurrence outcomes. Additionally, although procedures were performed by multiple surgeons, all operations were conducted within a single high-volume center using a standardized surgical technique, which likely reduced inter-operator variability.
Despite these limitations, this study provides a detailed trajectory-based evaluation of recovery following unilateral TEP repair and suggests that the fixation strategy may exert differential effects depending on defect size. Rather than demonstrating a universal superiority of one fixation technique, our findings indicate that clinical impact may be context-specific. Prospective studies incorporating stratified design and longer follow-up are warranted to clarify whether larger defects represent a subgroup that may derive greater benefit from nonpenetrating fixation strategies. 22
Conclusion
In patients undergoing unilateral TEP inguinal hernia repair, the mesh fixation strategy does not substantially influence overall early and short-term recovery in the general cohort. Longitudinal trajectory analysis demonstrated significant recovery improvement over time irrespective of fixation method.
However, in patients with larger hernia defects (≥20 mm), self-fixating mesh was associated with improved quality-of-recovery scores in adjusted analyses, suggesting that fixation-related effects may be context-dependent and influenced by defect size rather than uniform across all cases.
These findings indicate that fixation strategy selection in routine unilateral TEP repair may reasonably be guided by surgeon preference and institutional considerations in most patients, while larger defects may represent a subgroup in which nonpenetrating fixation could confer recovery advantages. Prospective stratified studies with longer follow-up are warranted to validate these observations.
Authors’ Contributions
K.I.: Conceptualization, methodology, formal analysis, data curation, investigation, writing—original draft, writing—review and editing, visualization, project administration. K.T.: Supervision, methodology, writing—review and editing, and validation. B.T.: Investigation, data curation, writing—review & editing.
Footnotes
Acknowledgments
The authors thank the surgical and nursing staff involved in the perioperative care and follow-up of the patients.
Consent to Participate
Due to the retrospective nature of the study, the requirement for written informed consent to participate was waived by the ethics committee.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.