
Abstract
Background:
Inguinal canal fat encountered during inguinal hernia repair is frequently described as a lipoma, although many lesions are continuous with preperitoneal fat (PPF) rather than true neoplasms. The lack of clear intraoperative criteria has led to controversy regarding routine excision versus conservative management. This study aimed to determine whether intraoperative differentiation between true lipomas and PPF can guide selective surgical management.
Methods:
We retrospectively reviewed 2465 adult patients (aged ≥20 years) who underwent transabdominal preperitoneal (TAPP) repair between January 2019 and December 2023. Among them, 271 patients with fatty tissue in the inguinal canal were analyzed. Intraoperative fatty tissue was classified as either true lipoma or PPF based on encapsulation and continuity with the preperitoneal space. True lipomas were excised, and PPF was managed with reduction alone.
Results:
The presence of inguinal canal fat was not associated with differences in the demographic or hernia-related clinical characteristics. Recurrence was rare in both groups (0.3% versus 0.4%), with no significant difference between the patients with and without fatty tissue. Operative time was longer in patients with fatty tissue (35.6 ± 8.2 versus 28.9 ± 5.8 minutes, P < .001). Within the fat group, lipoma excision required longer operative time (41.8 ± 9.5 versus 34.9 ± 7.8 minutes, P = .001) and was associated with a higher complication rate (10.0% versus 1.2%, P = .005) than was PPF reduction, while recurrence and metachronous contralateral inguinal hernia were rare in both subgroups. Other postoperative outcomes were comparable between the strategies.
Conclusions:
Most fatty protrusions encountered in the inguinal canal during TAPP repair were continuous with the PPF layer rather than discrete encapsulated lipomas. In appropriately selected cases, reduction of PPF without excision appeared feasible and safe, with favorable short- and long-term outcomes.
Introduction
Fatty tissue encountered within the inguinal canal during inguinal hernia (IH) repair is a common intraoperative finding and is frequently described as a spermatic cord or round ligament lipoma. Its clinical relevance has been emphasized because unrecognized inguinal canal fat has been associated with postoperative groin bulging, pseudo-recurrence, and unnecessary reoperation, even in the absence of a true hernia recurrence.1–3
Traditionally, these fatty tissues have been uniformly referred to as a “lipoma.” According to the World Health Organization classification, a true lipoma is a benign mesenchymal neoplasm composed of mature adipocytes characterized by a well-circumscribed encapsulated structure. 4 Conversely, several anatomical and surgical studies have shown that fatty tissue encountered during IH repair is often unencapsulated and shows direct continuity with the preperitoneal fat (PPF) layer. This observation indicates that many lesions described as cord or round ligament lipomas are not true neoplastic lesions but rather protrusions of the PPF.5–7
Reportedly, failure to appropriately manage inguinal canal fat results in persistent postoperative symptoms, including groin pain, palpable masses, and imaging findings that mimic hernia recurrence.2,8,9 Consequently, some authors have advocated routine excision of all inguinal canal fat during hernia repair, treating it as an indirect hernia equivalent.10,11 However, routine or indiscriminate excision may result in unnecessary dissection, increasing the risk of bleeding, nerve injury, or damage to the vas deferens and spermatic vessels, particularly when the fatty tissue is an unencapsulated PPF rather than a true lipoma.6,12
Despite growing awareness of this distinction, clear intraoperative criteria for differentiating true lipomas from PPF and standardized management strategies are lacking. The transabdominal preperitoneal (TAPP) approach offers a unique anatomical advantage, enabling direct visualization of the preperitoneal space and assessment of whether inguinal canal fat is continuous with preperitoneal tissue or exists as an isolated encapsulated mass.13,14 The importance of differentiating fat-containing lesions within the inguinal canal has also been emphasized in imaging studies. 15
This study evaluated whether laparoscopic assessment of encapsulation and anatomical continuity during TAPP repair could guide selective management of inguinal canal fat.
Material and Methods
Study design and population
In this retrospective observational study, we included patients who underwent TAPP repair for IH between January 2019 and December 2023 at a single institution (Fig. 1). During the study period, 2591 patients underwent the procedure. Among them, 105 patients with recurrent IH (Nyhus type IV) were excluded from the primary analysis because prior surgical intervention could alter the normal anatomy and confound the assessment of the inguinal canal fat, and 21 patients were lost to follow-up. Consequently, 2465 patients were included in the final analysis. Patients with fatty tissues within the inguinal canal during surgery were included in the subgroup analysis.
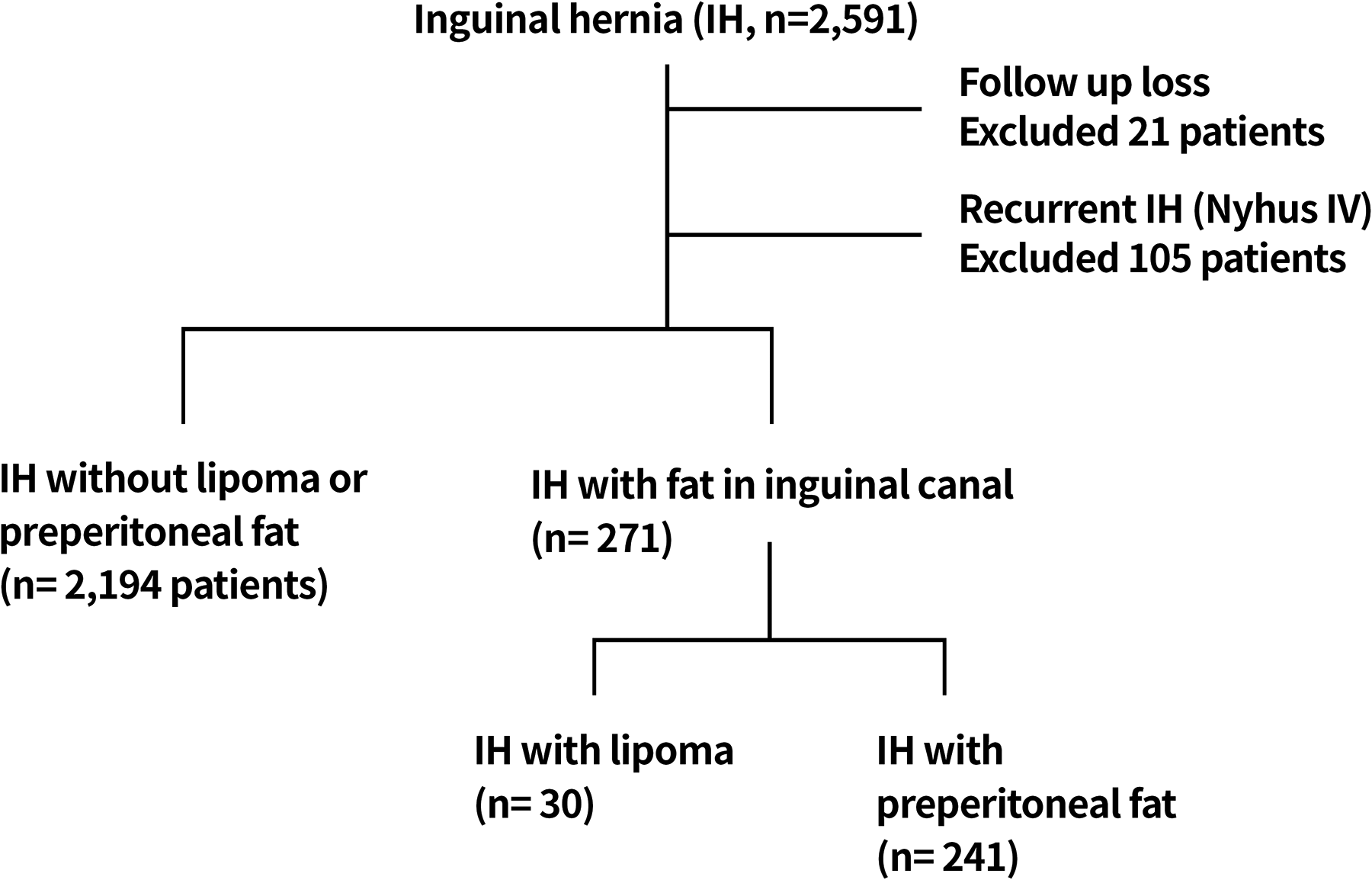
Flow diagram of patient enrollment. A total of 2591 patients underwent transabdominal preperitoneal (TAPP) repair for inguinal hernia during the study period. Among them, 105 patients with recurrent inguinal hernia (Nyhus type IV) were excluded because previous surgery could alter the normal anatomy of the inguinal canal. An additional 21 patients were excluded because they were lost to follow-up. Consequently, 2465 patients were included in the final analysis. Among these patients, 271 had fatty tissue within the inguinal canal, including 30 true lipomas and 241 protrusions of preperitoneal fat.
If abnormal findings other than benign-appearing inguinal canal fat were suspected preoperatively, further evaluation was performed using magnetic resonance imaging or biopsy. Surgery was performed only when no additional pathological findings were observed. Data on demographics, operative findings, surgical management of inguinal canal fat, operative time, and postoperative outcomes were collected from medical records. The study was approved by the Institutional Review Board of Damsoyu Hospital (DSY-2026-001).
Intraoperative classification of inguinal canal fat
Fatty tissue encountered within the inguinal canal was intraoperatively differentiated as either a true lipoma or PPF, based on encapsulation and continuity with the preperitoneal space. True lipoma was defined as a discrete encapsulated fatty mass without continuity with the surrounding preperitoneal tissue, whereas PPF exhibits direct continuity with the PPF layer and lacks a distinct capsule. Intraoperatively, the PPF extended into the inguinal canal, either lateral or medial to the spermatic cord, depending on anatomical continuity. Classification was made by the operating surgeon and confirmed by review of operative videos/images. All TAPP procedures were performed by experienced surgeons using standardized techniques.
Surgical technique
All surgeries were performed with the patient under general anesthesia and in the supine position. A 5-mm transumbilical trocar was inserted to establish a pneumoperitoneum at 8–10 mmHg, followed by placing two additional 5-mm working ports in the lateral abdomen. External compression was applied to assess the internal ring and identify PPF tissue (Fig. 2).
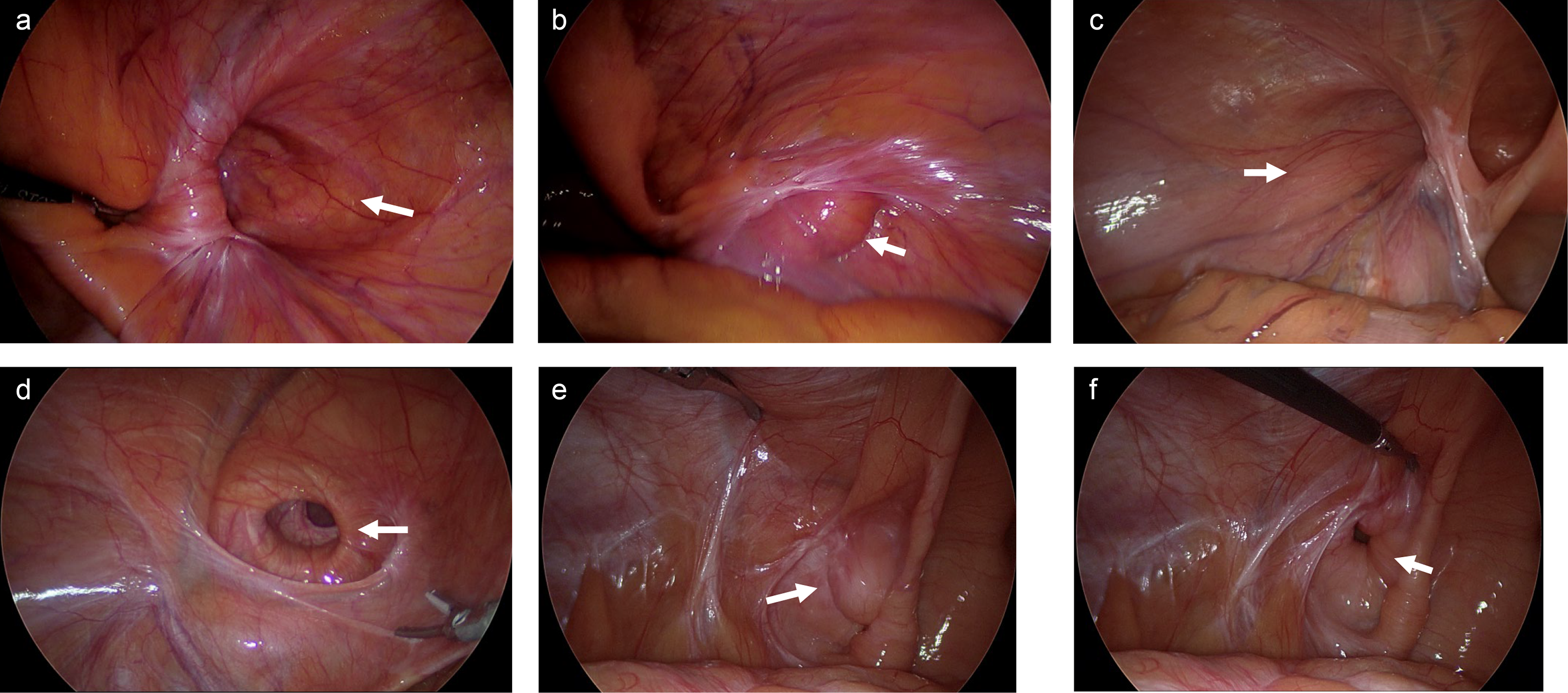
Laparoscopic view of the internal ring and detection of inguinal canal fat using external compression.
After identifying the internal ring, the hernial sac in male patients was carefully dissected from the vas deferens and spermatic vessels and divided at its base. Meanwhile, in female patients, the hernial sac was completely dissected while preserving the round ligament. The internal ring was then reevaluated to assess the residual fatty tissue.
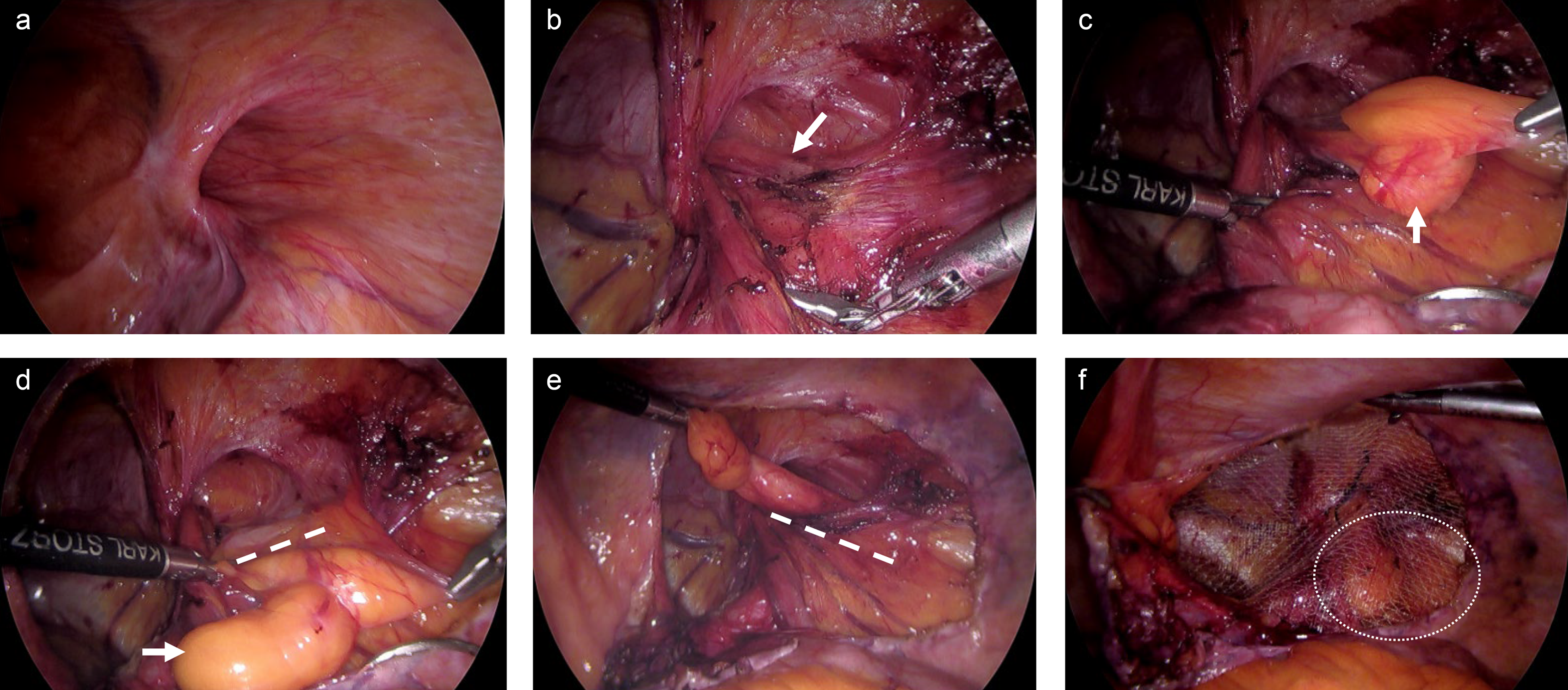
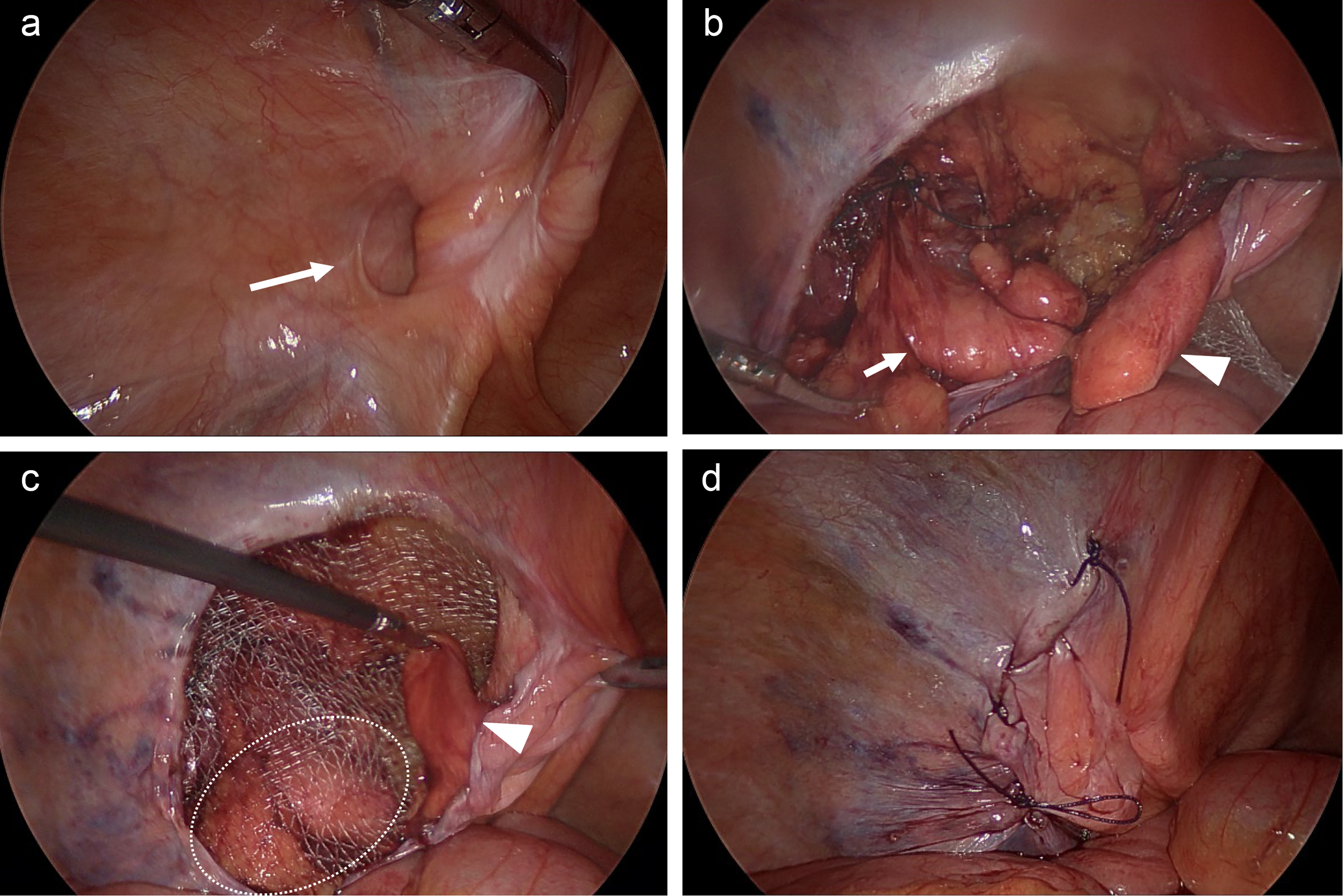
Excision was performed when a true lipoma was identified (Fig. 3). In cases of PPF, excision was avoided, and gentle traction was applied to reduce the fat in the preperitoneal space before mesh placement.

TAPP repair with excision of a true lipoma.
When the PPF extended laterally to the spermatic cord, the mesh directly covered the reduced fat (peritoneum–mesh–PPF–inguinal canal configuration; Fig. 4). Meanwhile, the reduced fat overlaid the mesh (peritoneum–PPF–mesh–inguinal canal configuration; Fig. 5) when the PPF extended medially to the spermatic cord.
TAPP repair with reduction of lateral PPF in an indirect inguinal hernia.
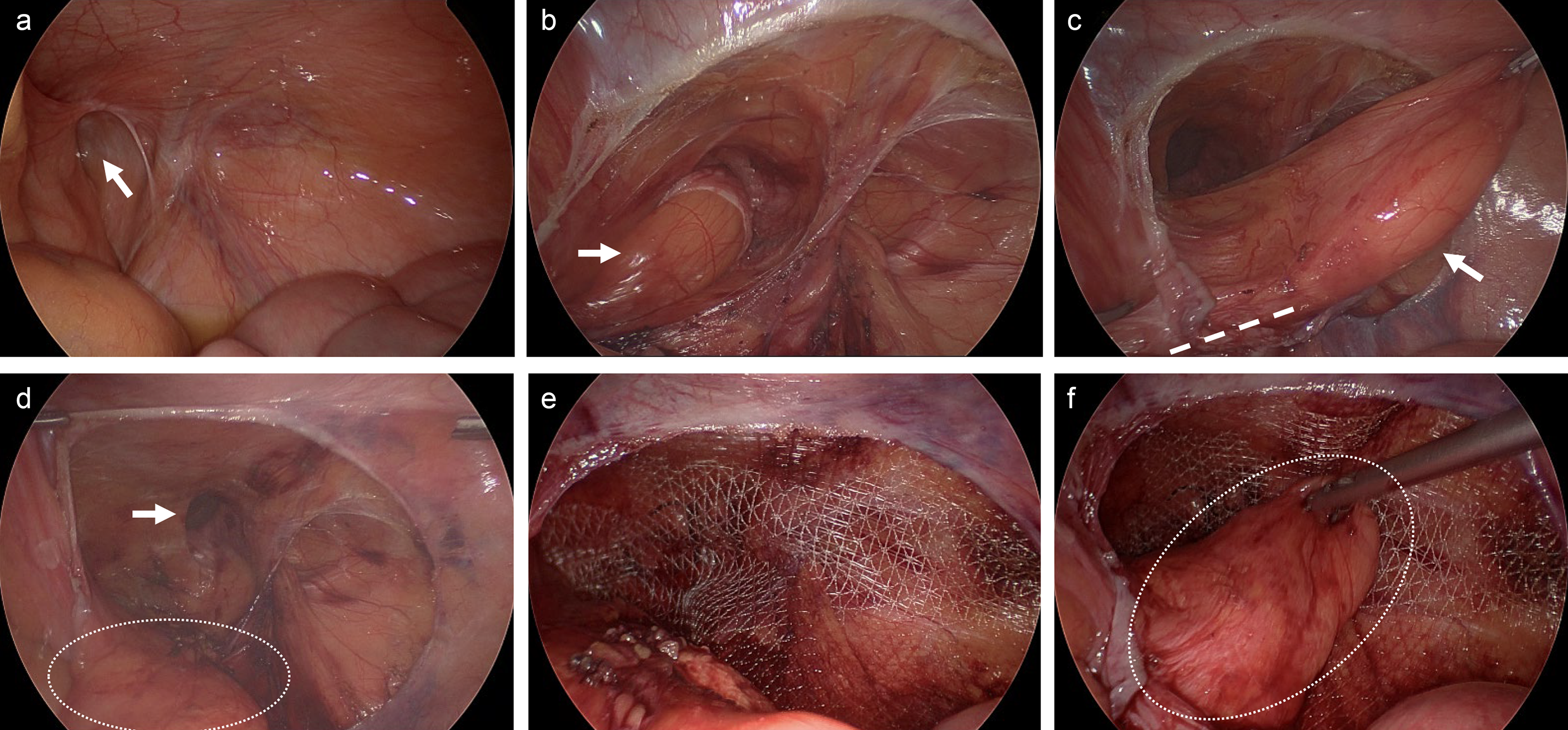
TAPP repair with reduction of medial PPF in a direct inguinal hernia.
Postoperative management and follow-up
Primary outcomes included intraoperative feasibility, operative time, and postoperative complications, whereas IH recurrence, postoperative bulging or pseudo-recurrence, and the development of a new IH during follow-up comprised the secondary outcomes.
Patients were followed up through outpatient visits, and clinical examinations were conducted to assess recurrence or postoperative symptoms. Long-term follow-ups consisted of annual outpatient visits or structured telephone interviews.
Statistical analysis
The patient characteristics were summarized using descriptive statistics. Continuous variables are presented as mean ± standard deviation (SD) and range, and categorical variables are expressed as number (%). The R software (R Foundation for Statistical Computing, Vienna, Austria) was used for statistical analysis. Continuous variables were compared using independent t-tests and validated using the Wilcoxon rank-sum test for sensitivity analysis. Categorical variables were compared using the χ2 test or Fisher’s exact test, as appropriate. Mean differences with 95% confidence intervals (CIs) were reported for continuous variables. Odds ratios with 95% CIs were reported for binary categorical variables, and Cramer’s V with 95% CIs was reported for multi-category variables. All tests were two-sided, and a P < .05 was considered statistically significant.
Results
Overall, 2465 patients were included in the final analysis. Among them, 271 (11.0%) had PPF or lipoma within the inguinal canal, whereas 2194 had no fatty protrusions.
Patients with versus without inguinal canal fat (Table 1)
The baseline demographic and hernia-related characteristics were largely comparable between patients with and without inguinal canal fat. The distribution of Nyhus type differed between the groups, with a higher proportion of type IIIA hernias observed in patients with fatty protrusions.
Comparison of the Clinical Characteristics and Surgical Outcomes Between Patients with and without Preperitoneal Fat/Lipoma in the Inguinal Canal
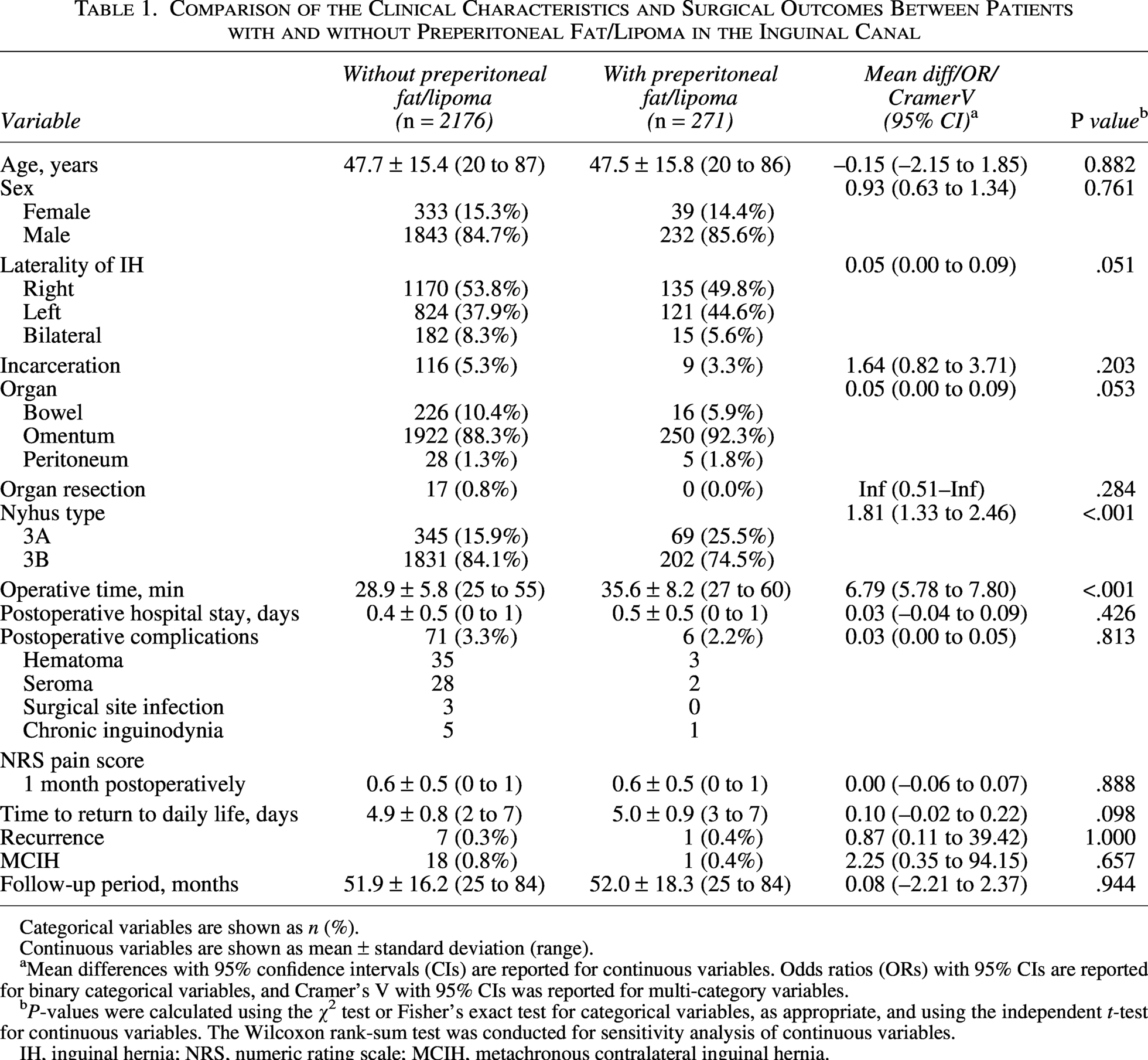
Categorical variables are shown as n (%).
Continuous variables are shown as mean ± standard deviation (range).
Mean differences with 95% confidence intervals (CIs) are reported for continuous variables. Odds ratios (ORs) with 95% CIs are reported for binary categorical variables, and Cramer’s V with 95% CIs was reported for multi-category variables.
P-values were calculated using the χ2 test or Fisher’s exact test for categorical variables, as appropriate, and using the independent t-test for continuous variables. The Wilcoxon rank-sum test was conducted for sensitivity analysis of continuous variables.
IH, inguinal hernia; NRS, numeric rating scale; MCIH, metachronous contralateral inguinal hernia.
Operative time was significantly longer in patients with inguinal canal fat (35.6 ± 8.2 versus 28.9 ± 5.8 minutes, P < .001). However, the postoperative complication rates, pain scores, time to return to daily life, and hospital stay were comparable between the groups. Recurrence was rare in both groups (0.3% versus 0.4%), and the presence of metachronous contralateral inguinal hernia (MCIH) was infrequent (0.8% versus 0.4%), with no significant difference between the groups.
Lipoma excision versus PPF reduction (Table 2)
Among patients with inguinal canal fat, 30 underwent lipoma excision, while 241 underwent PPF reduction. Operation time was longer in the lipoma excision group. Postoperative complications were more frequent in the lipoma excision group (10.0% versus 1.2%, P = .005).
Comparison of the Clinical Characteristics and Surgical Outcomes Between Lipoma Excision and PPF Reduction
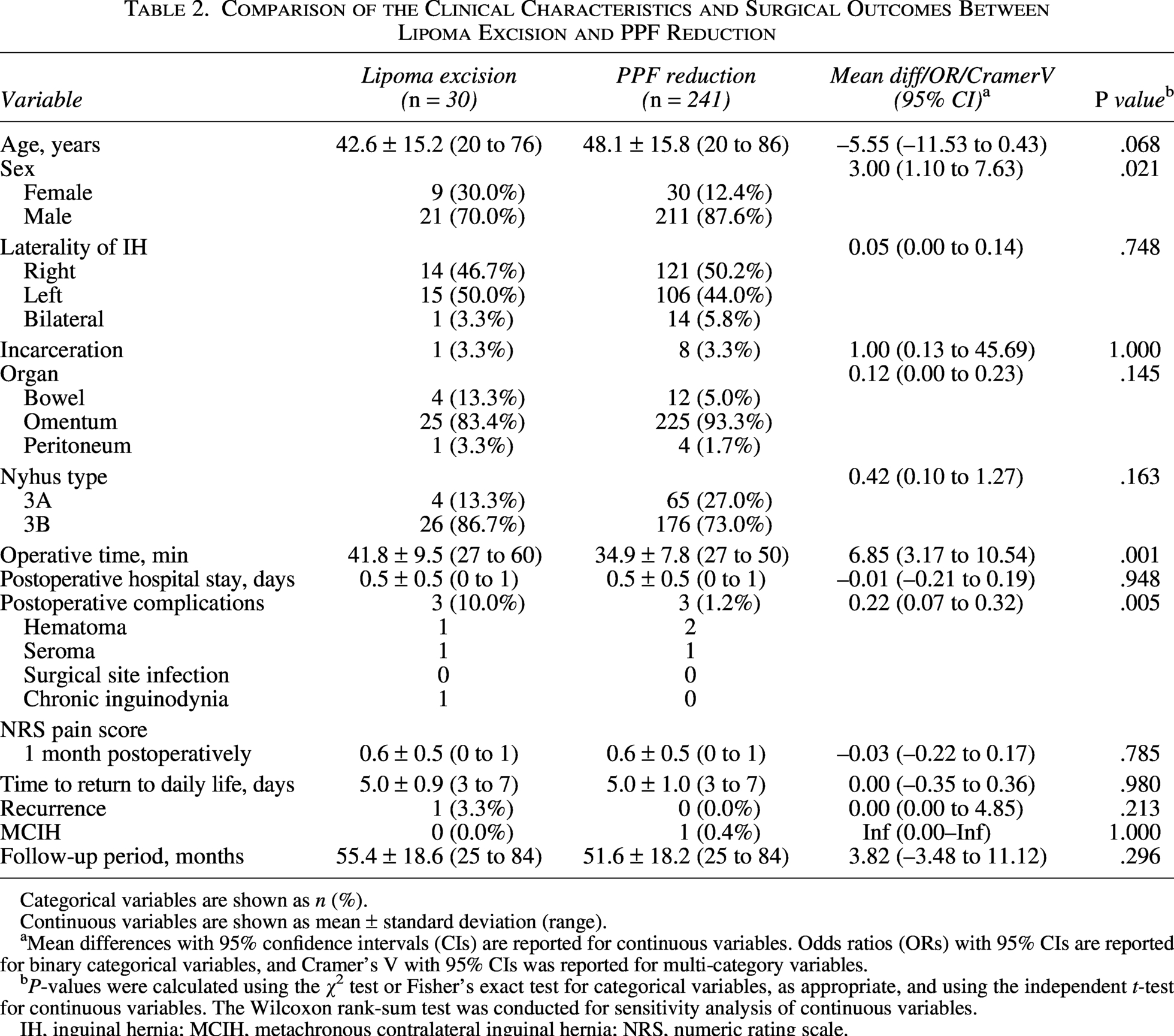
Categorical variables are shown as n (%).
Continuous variables are shown as mean ± standard deviation (range).
Mean differences with 95% confidence intervals (CIs) are reported for continuous variables. Odds ratios (ORs) with 95% CIs are reported for binary categorical variables, and Cramer’s V with 95% CIs was reported for multi-category variables.
P-values were calculated using the χ2 test or Fisher’s exact test for categorical variables, as appropriate, and using the independent t-test for continuous variables. The Wilcoxon rank-sum test was conducted for sensitivity analysis of continuous variables.
IH, inguinal hernia; MCIH, metachronous contralateral inguinal hernia; NRS, numeric rating scale.
Recurrence and MCIH were rare in both subgroups. Other postoperative outcomes, including pain scores (P = .785), length of hospital stay (P = .948), and time to return to daily activities (P = .980), were comparable between the two strategies.
Discussion
The principal finding of this study is that most fatty tissue encountered in the inguinal canal during TAPP repair represents a continuous extension of PPF rather than a discrete encapsulated lipoma. Using a clear intraoperative anatomical criterion based on encapsulation and continuity with the preperitoneal space, we distinguished encapsulated lipomas from nonencapsulated PPF and tailored surgical management accordingly. These findings challenge the long-standing assumption that all inguinal canal fat should be regarded as neoplastic lesions requiring routine excision.
Previous studies have highlighted the clinical relevance of inguinal canal fat, reporting that missed cord or round ligament lipomas result in postoperative groin bulging, pseudo-recurrence, or reoperation.1–3,8 Consequently, some authors have advocated routine excision of all inguinal canal fat during hernia repair.10,11 Furthermore, a previous report described laparoscopic findings of groin bulging without an obvious peritoneal sac, underscoring the diagnostic challenge of distinguishing fatty protrusions from true hernia recurrence. 16 However, many earlier reports did not clearly differentiate true encapsulated lipomas from protruding PPF, nor did they assess their anatomical continuity with the preperitoneal space. Therefore, nonneoplastic fat may have been overtreated in many cases.6,7 Our data show that a selective approach based on anatomical characteristics is feasible and safe.
The TAPP approach has unique diagnostic advantages. Direct visualization of the preperitoneal space allows real-time assessment of whether the fatty tissue is a discrete encapsulated mass or a continuous extension of PPF. In our experience, this distinction was consistently reproducible when laparoscopic inspection and gentle traction were used. This anatomical perspective is particularly relevant because management decisions can be made intraoperatively without arbitrary or subjective criteria.
Reduction in PPF offers several practical advantages. Because PPF represents normal adipose tissue lacking encapsulation, aggressive dissection may be associated with an increased risk of bleeding, nerve injury, or damage to adjacent structures.6,12 In the present cohort, reduction alone did not increase recurrence or postoperative morbidity, and the overall outcomes remained excellent. This strategy was further supported by subgroup analysis: although lipoma excision required a longer operative time and was associated with a higher complication rate, recurrence was rare in both groups. These findings support a selective rather than routine excision strategy for inguinal canal fat during TAPP repair.
The anatomical orientation of the PPF relative to the spermatic cord influenced the spatial relationship between the reduced fat and the mesh. Notably, in some patients, the medial and lateral extensions of the PPF were observed simultaneously (Fig. 6), demonstrating that the protrusion pattern was determined by anatomical continuity rather than by fat volume. Depending on its orientation, the reduced PPF was positioned either over or beneath the mesh, which may have influenced the intraoperative mesh placement strategy. This observation was not analyzed quantitatively; however, it provides practical guidance and reinforces the importance of anatomical assessments over size-based judgments.
TAPP repair with simultaneous medial and lateral PPF reduction in an indirect inguinal hernia.
This study has some limitations. Its retrospective design and single-center setting may limit its generalizability. Histopathological confirmation was not routinely performed because the primary objective of this study was anatomical and surgical characterization rather than pathological diagnosis. In most cases, the fatty tissue demonstrated clear intraoperative features distinguishing protruding PPF from a true encapsulated lipoma. These features included the absence of a capsule and direct continuity with the PPF layer. Therefore, routine excision solely for histopathological confirmation was considered unnecessary and potentially associated with additional dissection risk. In addition, the orientation of the PPF was not recorded as a formal variable for statistical comparisons. Nevertheless, the large cohort size, consistent surgical technique, and favorable long-term outcomes support the robustness of our findings.
In conclusion, the fatty tissue encountered within the inguinal canal during TAPP repair appears to represent an extension of PPF rather than a true lipoma in most cases. Selective management based on anatomical continuity allows avoidance of unnecessary excision while maintaining excellent surgical outcomes.
Authors’ Contributions
S.R.L.: Conceptualization, methodology, investigation, data curation, formal analysis, writing—original draft, and writing—review and editing; G.Y.B.: Methodology, investigation, formal analysis, writing—original draft, and writing—review and editing; I.G.S.: Methodology, investigation, formal analysis, writing—original draft, and writing—review and editing.
Ethics Approval
This study was approved by the Institutional Review Board of Damsoyu Hospital (DSY-2026-001).
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Corresponding author has read and approved the final version of the article and consent to its publication in Journal of Laparoendoscopic & Advanced Surgical Techniques.
Footnotes
Acknowledgments
The authors thank Hyejin Park for her assistance with English language editing, and Beom Seok Oh from the Research Center of Damsoyu Hospital and Young Hyun Lee from the Graduate School of Engineering at Ewha Womans University for their assistance with statistical analysis and data organization.
Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose
Funding Information
The authors have no financial ties to disclose