
Abstract
Background:
Sleeve gastrectomy (SG) has become the most common bariatric procedure worldwide. Unfortunately, a significant number of patients require conversion to Roux-en-Y gastric bypass (RYGB) or single-anastomosis duodeno-ileal bypass (SADI) because of recurrent weight gain. This study aimed to determine the rates of complications and mortality associated with conversion from SG to RYGB (SG-RYGB) compared with conversion from SG to SADI (SG-SADI).
Methods:
This retrospective analysis used data from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database from 2020 to 2022. Patients undergoing SG-RYGB or SG-SADI were included. Thirty-day operative outcomes, intraoperative and postoperative events, and mortality were analyzed.
Results:
A total of 28,758 patients were included. Of these, 27,412 (95.3%) underwent SG-RYGB and 1346 (4.6%) underwent SG-SADI. The mean preoperative body mass index was 39.7 kg/m2 for SG-RYGB and 45.3 kg/m2 for SG-SADI (P < .001). SG-RYGB was associated with a higher frequency of intraoperative/postoperative complications within the first 30 days (5.9% versus 3.4%, P < .001), including transfusion (1.3% versus 0.4%, P = .004), readmission (7.3% versus 4.6%, P < .001), and emergency department visits (12.5% versus 8.5%, P < .001). Although SG-SADI was associated with a higher rate of anastomotic leak (0.4% versus 1.1%, P < .001), there was no difference in reoperation rates (2.8% versus 2.5%) or deaths (0.02% versus 0%). Overall, SG-SADI-S was associated with a lower risk of intraoperative/postoperative complications, with an adjusted odds ratio of 0.741 (95% confidence interval: 0.543–0.901, P = .041).
Conclusions:
Both revisional procedures are safe. Although SG-RYGB was associated with a higher frequency of intraoperative/postoperative complications within the first 30 days, SG-SADI had a higher rate of anastomotic leaks, with no difference in reoperation rates or deaths.
Keywords
Introduction
Metabolic and bariatric surgery (MBS) remains one of the most effective treatments for obesity, with sleeve gastrectomy (SG) being the most commonly performed procedure. 1 Nevertheless, over time, many patients experience recurrent weight gain (RWG) or inadequate weight loss (IWL), ultimately leading them to seek revisional surgery. 2 According to Lazzati et al., up to 12.2% of patients undergo revisional surgery within 10 years after SG, with Roux-en-Y gastric bypass (RYGB) being the most frequently performed revisional procedure, representing 75.2% of cases. 3 Since the American Society for Metabolic and Bariatric Surgery (ASMBS) endorsed single-anastomosis duodeno-ileal bypass with SG (SADI-SG) in 2021, this procedure has gained popularity as both a primary and revisional surgery following SG. Its increasing adoption is supported by evidence demonstrating greater total weight loss and superior resolution of comorbidities compared with RYGB,4–6 and even with the traditional duodenal switch, particularly in patients with a body mass index (BMI) over 50. 7
Multiple studies with long-term follow-up have demonstrated that conversion from SG to RYGB (SG-RYGB) is a safe procedure with a low complication rate. In contrast, the limited analysis of short- and long-term outcomes following SG conversion to SADI (SG-SADI) may be a key factor limiting its adoption into routine surgical practice. Moreover, comparative data between the two revisional techniques remain scarce. Therefore, this study aims to analyze and compare 30-day morbidity and mortality rates in patients with prior SG undergoing either RYGB or SADI, using data from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP) database.
Materials and Methods
A cross-sectional study was conducted using the MBSAQIP database. This registry compiles yearly information on metabolic and bariatric surgeries performed at institutions accredited by both the American College of Surgeons and the ASMBS. As the largest clinical database in the United States focused exclusively on bariatric surgery, MBSAQIP supports the delivery of high-quality patient care through strict evaluation protocols and adherence to established clinical standards. Trained reviewers extract data directly from patient charts, and all participating accredited centers submit de-identified 30-day outcomes to the centralized registry. The American College of Surgeons Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (ACS MBSAQIP) and the centers participating in the ACS MBSAQIP are the sources of the data used herein; however, they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Patients were included if they underwent MBS between January 2020 and December 2022, specifically conversion to RYGB or SADI following SG as the primary procedure. These cases were identified using the appropriate CPT codes from the corresponding MBSAQIP Participant Use Files for the study period. Patients were excluded if they had a primary procedure other than SG, underwent a subsequent procedure other than RYGB or SADI, were younger than 18 years of age, or had incomplete data for the covariates of interest. The final sample size was determined based on these inclusion and exclusion criteria, thereby constituting a convenience sampling.
The following variables were included in the study: age at the time of the initial surgery, gender, BMI before surgery, diabetes mellitus (DM), hypertension (HTN), hyperlipidemia (HLD), current smoker within 1 year surgery, chronic obstructive pulmonary disease (COPD), history of pulmonary embolism (PE), history of deep venous thromboembolism (DVT), obstructive sleep apnea (OSA), gastroesophageal reflux disease (GERD), hemodialysis, renal insufficiency, American Society of Anesthesiologists (ASA) classification, length of the procedure, hospital stay, robotic approach or not, and drain placement.
The primary outcomes of the study were intraoperative and postoperative complications occurring within the first 30 days, including surgical site infection, anastomotic leak, pneumonia, myocardial infarction, intraoperative or postoperative transfusion, unplanned admission, gastrointestinal bleeding (GIB), reoperation, readmission, emergency department (ED) visit, and death.
Quantitative variables were expressed as median and standard deviation, and qualitative variables were expressed as proportions. The chi-square and Mid-P exact test were used for categorical variables, and Student’s t-test was used for quantitative variables. To address potential sources of bias, univariate and multivariate logistic regression analyses were performed to model the relationship between the type of bariatric surgical procedure and 30-day intraoperative and postoperative complications, adjusting for relevant variables as covariates. A stratified analysis was conducted to assess variations in the effect of surgical technique on intraoperative and postoperative complications based on patients’ baseline characteristics, such as age, gender, and comorbidities.
The statistical software IBM SPSS Statistics for Windows, Version 29.0.2.0 (IBM Corp., Armonk, NY) was used to conduct statistical tests to assess for statistical significance (P < .05). Based on the study sample and the proportion of the primary outcome observed in each group, the estimated statistical power of the study was 0.9697 (95% confidence interval [CI]), as calculated using the OpenEpi web tool.
This study was deemed exempt from institutional review board approval because it utilized de-identified data from the MBSAQIP national database. No human or animal subjects were directly involved. It was conducted following the 1964 Helsinki Declaration and its later amendments or comparable ethical standards and following the guidelines and recommendations of the STROBE guidelines.
Results
An initial query of the 2020 and 2022 MBSAQIP databases identified 610,559 unique participants. After applying the inclusion criteria for primary operation and operation type, 35,336 participants remained. Following the application of exclusion criteria, 28,758 participants were retained in the dataset and included in the final analyses. No missing data were observed for the variables considered.
Of the patients included in the analysis, 95.3% (n = 27,412) underwent SG-RYGB, whereas 4.7% (n = 1346) underwent SG-SADI. The majority of patients in the cohort were female (90.6%, n = 26,072), with a mean age of 45.9 ± 10.4 years. The average BMI prior to the primary procedure was 39.9 ± 7.8 kg/m2, with a significantly higher preoperative BMI in the SG-SADI group than in the SG-RYGB group (45.3 versus 39.7 kg/m2, P < .001). Similarly, patients who underwent SG-SADI had higher rates of several comorbidities, including DM (18.0% versus 11.3%, P < .001), HTN (38.8% versus 34.7%, P = .002), HLD (20.1% versus 17.6%, P = .017), history of DVT (3.3% versus 2.3%, P = .017), OSA (32.2% versus 23.2%, P < .001), and need for hemodialysis (0.5% versus 0.1%, P = .002). In contrast, patients who underwent SG-RYGB had a significantly higher prevalence of GERD (73.7% versus 38.5%, P < .001). Regarding the ASA classification, ASA II was more frequent in the SG-RYGB group (27% versus 17.2% in SG-SADI, P < .001), whereas ASA III and IV were more common in the SG-SADI group (78.2% versus 70.7% for ASA III, and 4.2% versus 1.9% for ASA IV, P < .001). Demographic characteristics and comorbidity profiles are summarized in Table 1.
Baseline Characteristics of Patients Undergoing Roux-en-Y Gastric Bypass Versus Single-Anastomosis Duodeno-Ileal Bypass After Sleeve Gastrectomy
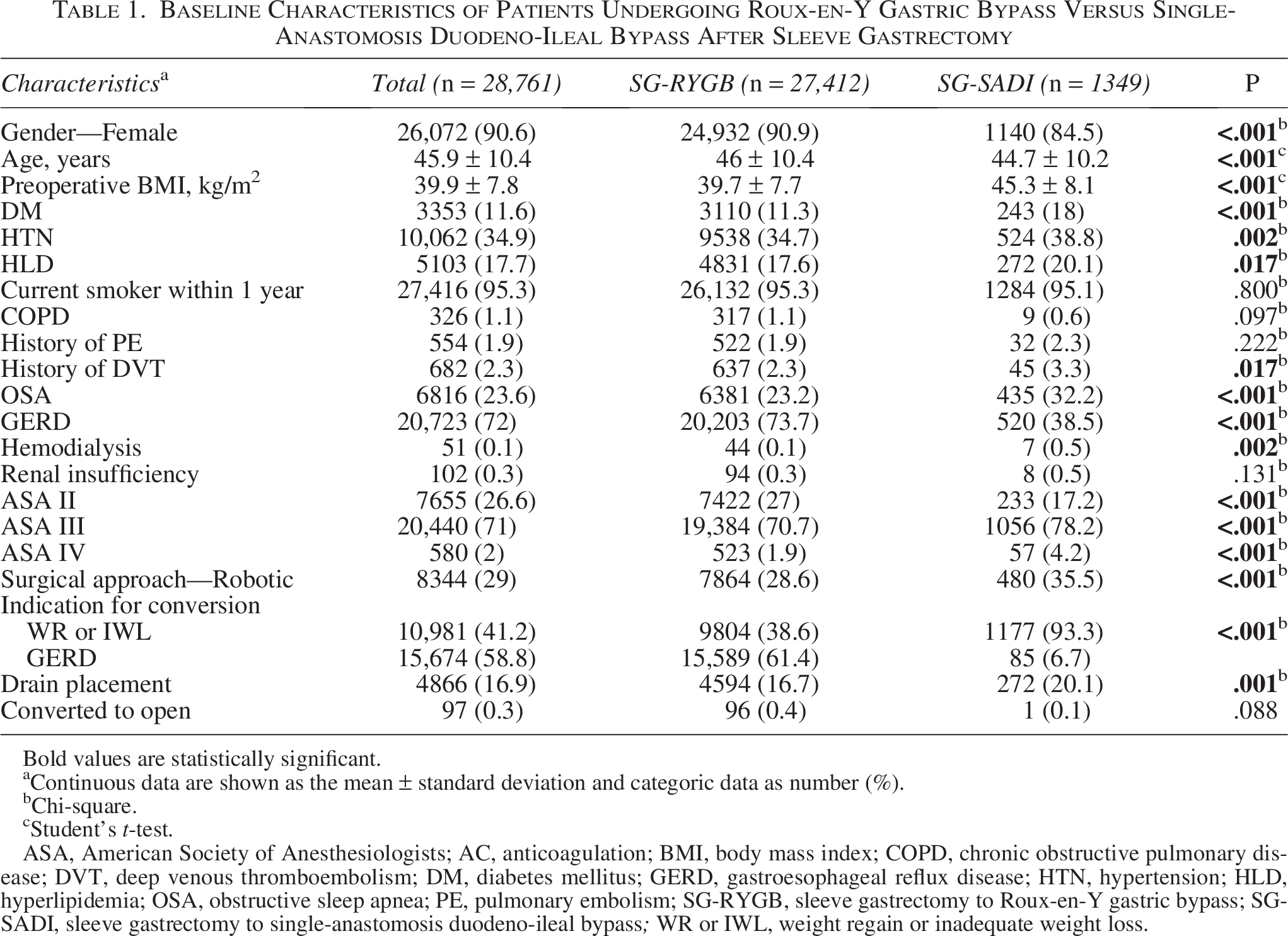
Bold values are statistically significant.
Continuous data are shown as the mean ± standard deviation and categoric data as number (%).
bChi-square.
cStudent’s t-test.
ASA, American Society of Anesthesiologists; AC, anticoagulation; BMI, body mass index; COPD, chronic obstructive pulmonary disease; DVT, deep venous thromboembolism; DM, diabetes mellitus; GERD, gastroesophageal reflux disease; HTN, hypertension; HLD, hyperlipidemia; OSA, obstructive sleep apnea; PE, pulmonary embolism; SG-RYGB, sleeve gastrectomy to Roux-en-Y gastric bypass; SG-SADI, sleeve gastrectomy to single-anastomosis duodeno-ileal bypass; WR or IWL, weight regain or inadequate weight loss.
There was no difference in procedure length between the groups (144.5 versus 144 minutes). Similarly, SG-RYGB was associated with a higher frequency of intraoperative and postoperative complications within the first 30 days (5.9% versus 3.4%, P < .001), including transfusion (1.3% versus 0.4%, P = .004), readmission (7.3% versus 4.6%, P < .001), and ED visits (12.5% versus 8.5%, P < .001). Despite SG-SADI being associated with a higher rate of anastomotic leak (0.4% versus 1.1%, P < .001), there was no difference in reoperation rates (2.8% versus 2.5%) or deaths (0.02% versus 0%). A comparison of intraoperative and postoperative outcomes is shown in Table 2.
Comparison of Intra- and Postoperative Outcomes Between Roux-en-Y Gastric Bypass and Single-Anastomosis Duodeno-Ileal Bypass After Sleeve Gastrectomy
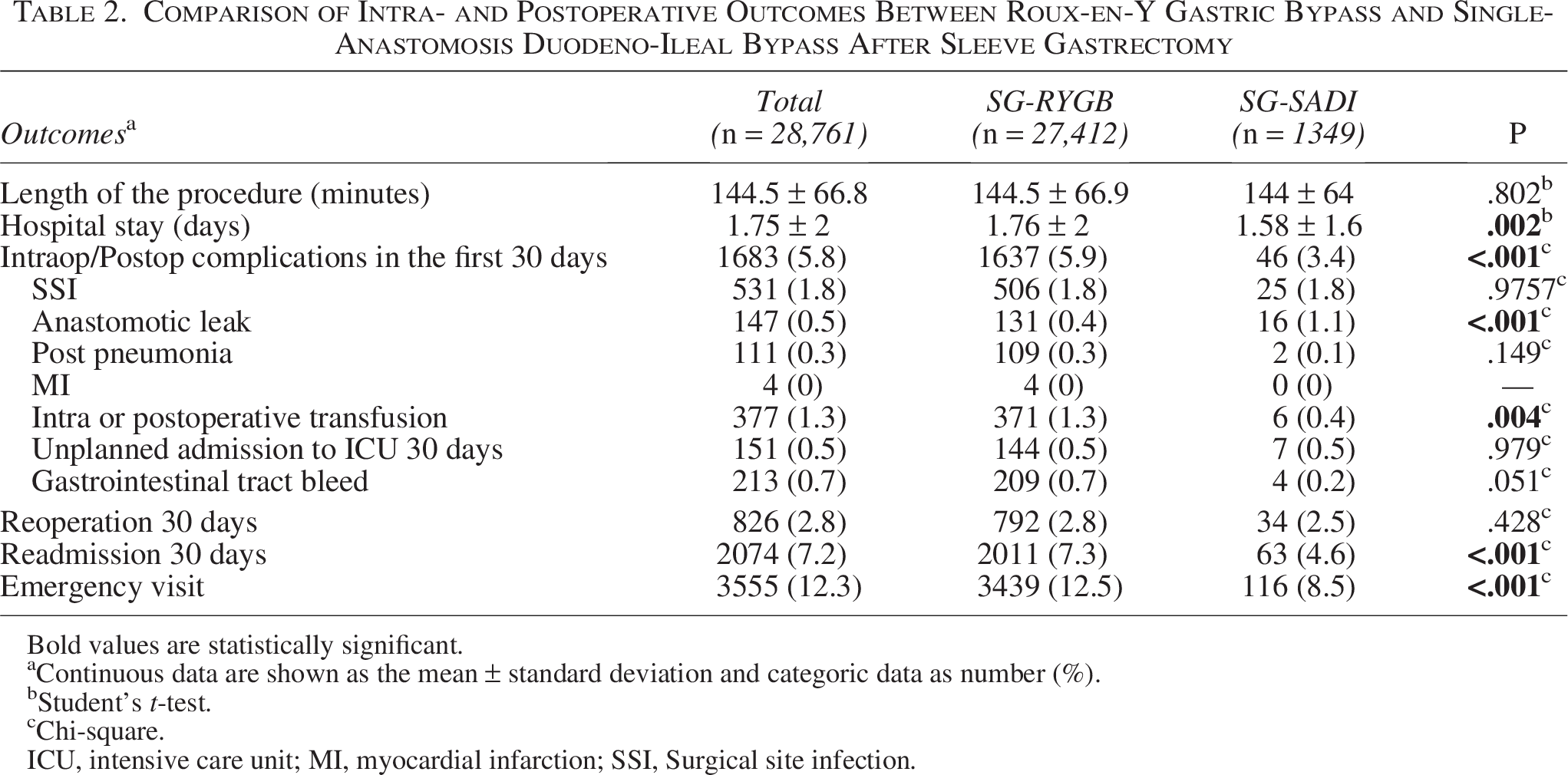
Bold values are statistically significant.
Continuous data are shown as the mean ± standard deviation and categoric data as number (%).
Student’s t-test.
Chi-square.
ICU, intensive care unit; MI, myocardial infarction; SSI, Surgical site infection.
The crude odds ratio (OR) for the effect of the type of revisional bariatric procedure—SADI versus RYGB following SG—on intraoperative and postoperative complications was 0.556 (95% CI: 0.413–0.749, P < .001). After adjustment for all baseline patient characteristics, the OR was 0.741 (95% CI: 0.543–0.901, P = .041).
Stratified analysis based on patient characteristics revealed that the reduction in intraoperative and postoperative complication risk associated with SADI-S compared with RYGB was more pronounced among female patients (OR = 0.528, 95% CI: 0.379–0.736), patients with a BMI < 50 kg/m2 (OR = 0.531, 95% CI: 0.375–0.750), patients without diabetes (OR = 0.535, 95% CI: 0.382–0.749), patients without a history of DVT (OR = 0.535, 95% CI: 0.392–0.731), GERD as the indication for conversion instead of weight regain or inadequate weight loss (OR = 0.341, 95%CI: 0.084–1.387), laparoscopic instead of robotic approach (OR = 0.532, 95% CI: 0.367–0.769), as well as in patients who did not undergo drain placement (OR = 0.429, 95% CI: 0.290–0.636). The subgroup analysis results are summarized in Table 3.
Stratified Analysis of Single Anastomosis Duodeno-Ileal Bypass with Sleeve Gastrectomy Versus Roux-en-Y Gastric Bypass and Surgical Complications in Revisional Bariatric Surgery
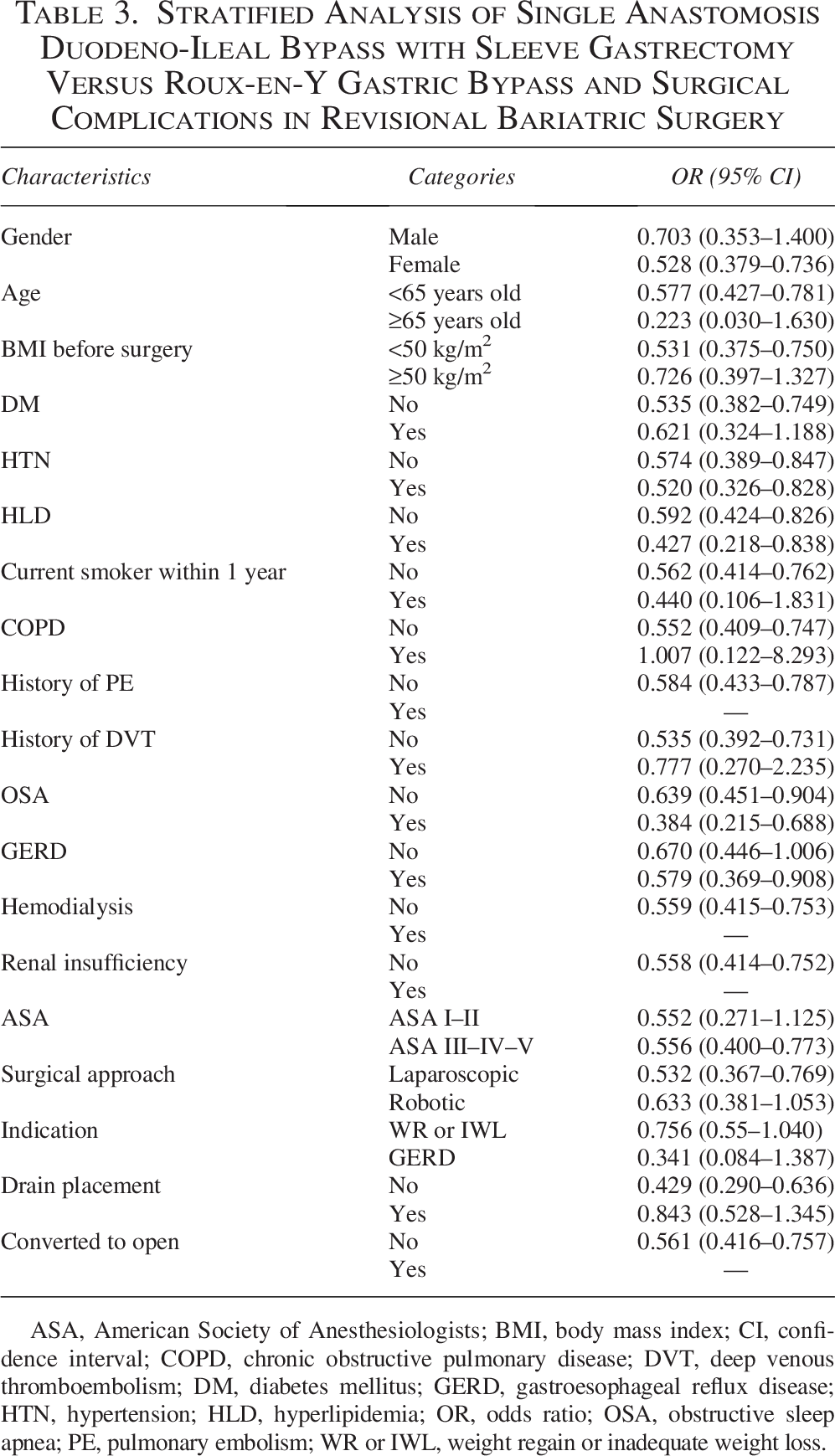
ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; DVT, deep venous thromboembolism; DM, diabetes mellitus; GERD, gastroesophageal reflux disease; HTN, hypertension; HLD, hyperlipidemia; OR, odds ratio; OSA, obstructive sleep apnea; PE, pulmonary embolism; WR or IWL, weight regain or inadequate weight loss.
Univariate and multivariate analyses were performed to identify factors significantly associated with intraoperative and postoperative complications within the first 30 days. In the multivariate analysis, HTN, HLD, COPD, history of PE and DVT, GERD, conversion to open surgery, and drain placement were identified as independent risk factors for 30-day intraoperative and postoperative complications. In contrast, conversion to SADI, use of a robotic approach, and a BMI ≥ 50 kg/m2 were associated with a reduced risk of complications. However, no reliable predictive model could be constructed based on the identified risk factors (κ = 0.001). Table 4 displays the detailed results.
Factors Associated with 30-Day Intraoperative and Postoperative Complications Following Revisional Surgery After Primary Sleeve Gastrectomy
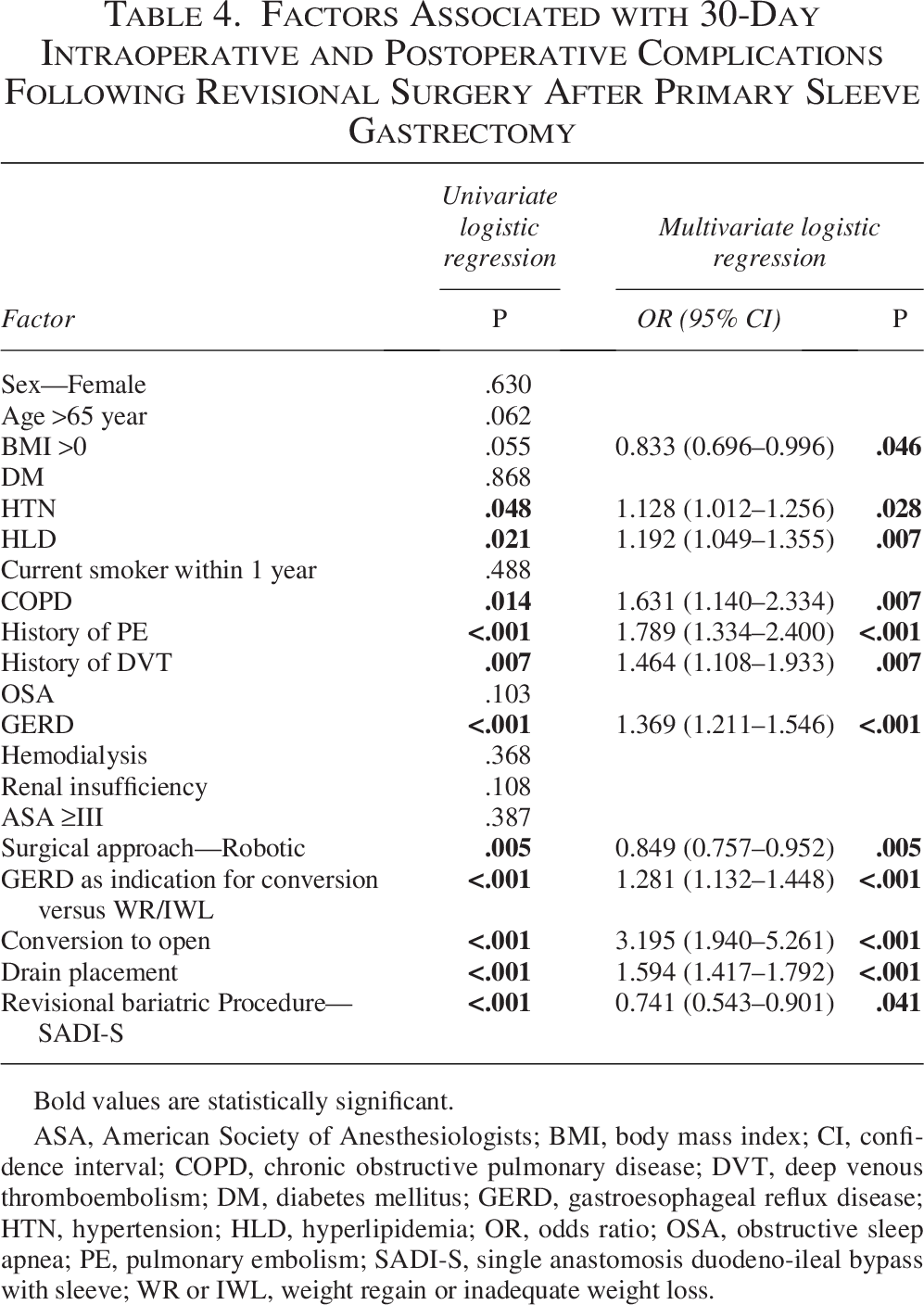
Bold values are statistically significant.
ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; DVT, deep venous thromboembolism; DM, diabetes mellitus; GERD, gastroesophageal reflux disease; HTN, hypertension; HLD, hyperlipidemia; OR, odds ratio; OSA, obstructive sleep apnea; PE, pulmonary embolism; SADI-S, single anastomosis duodeno-ileal bypass with sleeve; WR or IWL, weight regain or inadequate weight loss.
Discussion
This is the most comprehensive study to date assessing 30-day perioperative complications in patients undergoing conversion from SG to either RYGB or SADI. Patients converted to SADI had higher baseline BMI and a greater comorbidity burden. Despite these differences, SG-SADI was associated with a lower risk of 30-day intraoperative and postoperative complications compared with SG-RYGB in both crude and adjusted analyses. Subgroup analyses indicated that the reduction in complication risk with SG-SADI was more pronounced among female patients; those with a BMI < 50 kg/m2; those without diabetes or prior DVT; and those without drain placement. Other independent risk factors for complications were: HTN, HLD, COPD, a history of PE or DVT, GERD, conversion to open surgery, and drain placement.
The SG-SADI group demonstrated more frequent drain placement (20.1% versus 16.7%). Given that SADI patients tend to have higher baseline BMI and more metabolic comorbidities, these patient characteristics, rather than the procedure itself, might influence drain placement decisions. Additionally, the technical complexity of the procedure could theoretically prompt surgeons to place drains more frequently. 8
In our cohort, these patients also had higher utilization of the robotic approach (35.5% versus 28.6%). These findings are consistent with the growing trend toward robotic bariatric surgery. An increasing number of bariatric procedures are being performed robotically, offering potential advantages such as three-dimensional high-definition visualization, wristed instrumentation, and improved access to multiple abdominal quadrants. These features may be particularly beneficial in technically complex procedures such as SADI-SG. 9 Although, in the stratified analysis, the robotic approach group had an OR of 0.633 compared with 0.532 for the laparoscopic group (Table 3), the difference was small, and the overall trend of reduced complication risk with SG-SADI versus SG-RYGB was maintained. However, in the multivariable analysis, surgical approach was identified as an independent factor associated with a reduced risk of postoperative complications (OR = 0.849, 95% CI: 0.757–0.952) (Table 4).
The primary outcome of the study showed that conversion from SG to RYGB was associated with statistically significantly higher rates of overall intraoperative and postoperative complications (5.9% versus 3.4%), readmissions, and ED visits within the first 30 days. Notably, perioperative transfusions were significantly more frequent in this group. In a matched case–control analysis, Shin et al. reported similar findings, with significantly higher rates of hemorrhage in patients undergoing conversion from SG to RYGB compared with those converted to SADI or biliopancreatic diversion with duodenal switch (1.98% versus 0.87%, P = .01). 10 It is important to note that conversion from SG to RYGB involves gastric resection to create a new pouch within a reoperative surgical field, as well as the construction of two anastomoses—both requiring manipulation of highly vascularized tissue, thereby increasing the risk of bleeding. In contrast, conversion from SG to SADI does not require additional gastric resection, avoids mesenteric division, and involves only a single anastomosis.
Conversely, SG-SADI was associated with a significantly higher rate of anastomotic leak (1.1%, n = 16) compared with SG-RYGB (0.4%, n = 131; P < .001). In a retrospective analysis, Hage et al. reported similar findings, with anastomotic leak rates of 1.6% for SG-SADI compared with 0.5% for SG-RYGB. 11 Reported rates of anastomotic leakage following SG-to-SADI conversion vary across studies and appear to decrease with increasing surgical experience. In an early series, Torres et al. 12 reported a leak rate of 4%, reflecting the technical challenges associated with the initial adoption of the procedure. By contrast, Surve et al. 13 reported a substantially lower rate of 0.6% in a 2023 study, likely reflecting advancements in surgical technique and greater institutional expertise. These variations may reflect the learning curve associated with SADI, which remains a relatively new procedure in many bariatric centers across the United States.
When comparing SADI-S versus RYGB as primary procedures, the available data suggest similar findings, with higher leak rates reported for SADI-S. In the SADISLEEVE randomized trial, three (2%) duodeno-ileal anastomotic leaks occurred in the SADI-S group compared with one (1%) in the RYGB group. 14 A 2020 MBSAQIP analysis did report higher anastomotic leak rates with SADI-S (2.2% versus 0.5%, P < .001), although the authors considered that this likely reflected the early learning curve rather than an inherent procedural difference, noting that it remained unclear whether the findings represented true procedural differences or learning curve effects. 8 The technical complexity of the duodeno-ileal anastomosis in SADI-S presents unique challenges. The duodenal tissue is thicker and more vascular, and the anastomosis is performed in a more challenging anatomical location. When leaks do occur, they involve the duodeno-ileal anastomosis rather than the gastrojejunal anastomosis typically seen in RYGB. 14
Rates of surgical site infection, postoperative pneumonia, myocardial infarction, unplanned intensive care unit admission, GIB, reoperation, and 30-day mortality did not differ significantly between the two groups, aligning with previously published findings. 15
This study has several limitations inherent to the use of MBSAQIP data. First, the retrospective design limits control over the nature and quality of predictor variables. Second, long-term complications could not be assessed because the dataset is restricted to 30-day postoperative outcomes. Substantial variability in surgeon experience and surgical technique also could not be accounted for, limiting the ability to differentiate between operative approaches and patterns of patient selection. Additionally, the database lacks important details, such as the time interval between SG and revisional procedures. Furthermore, MBSAQIP does not provide information on the specific site of complications or the reasons for emergency department visits and readmissions, which may lead to an overestimation of complication rates.
Another limitation of this study is the marked difference in group sizes, which may reflect the fact that SADI procedures, being more technically complex and relatively novel, are likely performed at a smaller number of specialized centers, whereas RYGB procedures are more widely performed across centers with varying levels of experience. This difference in center volume and expertise could influence outcomes and should be considered when interpreting our results.
Propensity score matching (PSM) was not performed to adjust for baseline differences between groups. However, given the large number of outcome events relative to the number of covariates, multivariable logistic regression was selected as the primary analytic approach because it provides robust adjustment for measured confounders in large datasets. Therefore, although the absence of PSM may be considered a limitation, we believe that the analytical strategy used (univariable and multivariable logistic regression analysis and subgroup analysis) adequately mitigated potential bias inherent to the observational design. In light of these limitations, further studies with prospective designs, longer follow-up periods, and larger sample sizes are necessary to validate and generalize our findings.
Conclusion
Conversion of SG to either SADI or RYGB appears to be safe. Although SG-RYGB was associated with a higher frequency of intraoperative and postoperative complications, readmissions, and ED visits within the first 30 days, SG-SADI was associated with a higher rate of anastomotic leaks, with no difference in reoperation rates or deaths.
Authors’ Contributions
Study conception and design, as well as analysis and interpretation of data, were performed by Y.R.-M. Data acquisition was conducted by Y.R.-M., A.E., and V.V. Critical revision of the article was carried out by J.C., E.M.-A., and D.C.
Footnotes
Disclosure Statement
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this article.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.