
Abstract
Background:
Gastroesophageal reflux disease (GERD) is a common condition that affects millions of people worldwide. It can be stated that a defective esophageal reflux barrier (ERB) is the primary cause that can lead to these disease entities. The goal of this systematic review was to summarize and investigate the current literature regarding the functional and molecular aspects of the ERB in humans and the influence of anti-reflux surgery (ARS) on its improvement.
Materials and Methods:
Pubmed, Embase, MEDLINE, and the Cochrane Library were searched from the earliest available date of each database through April 12, 2026. Outcome measurements of interest were changes in the molecular and cellular components of the ERB, as well as improvement in GERD symptoms measured objectively or subjectively.
Results:
The primary literature search produced 110 results, including six duplicates. After screening on title and abstract, 15 studies were found possibly relevant and underwent full-text critical appraisal, resulting in 14 exclusions. Only the study by Ergun et al. fulfilled the inclusion criteria and was therefore included in this systematic review. This study showed significant improvements after ARS in mucosal integrity, mucosal permeability, and mRNA gene expression of the following molecules: E-cadherin, occludin, claudin 1, claudin 4, zonula occludens-1 and zonula occludens-2.
Conclusion:
ARS is responsible for many anatomical and physiological mechanisms, many of which are not yet fully understood. ARS may have positive effects on the mucosal and functional esophageal reflux barrier; however, further prospective studies need to further elucidate this.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is a common disease that affects millions of people worldwide.1–3 The spectrum of GERD includes multiple disease entities, such as reflux esophagitis, nonerosive reflux disease, extraesophageal GERD, (reflux) hypersensitivity, and Barrett’s esophagus. 2 In general, a defective esophageal reflux barrier (ERB) is the primary cause that can lead to these disease entities. However, the magnitude of disfunction may be greater in disease entities that induce mucosal damage with a quantitatively abnormal esophageal manometry. In other words, it can be stated that high-grade esophagitis (classified as Los Angeles grade C of grade D) may reflect greater ERB dysfunction than low-grade esophagitis (classified as Los Angeles grade A). 1
In an attempt to better understand the anatomical and physiological functions of the ERB, the American Foregut Society published a white paper with a 13-member working group of surgeons and gastroenterologists to summarize the function of ERB, its dysfunction, and the pathophysiological mechanisms that are responsible for it. 3 Based on this paper, the following aspects are crucial in the pathophysiology of ERB dysfunction: (1) separation of crural diaphragm from the lower esophageal sphincter (LES) with widening of the hiatus and diminished crural diaphragm sphincteric function; (2) loss of the intra-abdominal LES segment, resulting in complete disruption of the flap valve component; and (3) axial hiatal hernia leading to reflux during swallow-induced LES relaxation.
However, newer studies show that there is more to the ERB than previously understood. Ergun et al. 4 showed that, after laparoscopic anti-reflux surgery (LARS), epithelial remodeling of the esophageal mucosa plays an important role in restoring the molecular and functional ERB. In their study, they analyzed the expressions of E-cadherin (ECAD), occludin (OCLN), claudin 1 (CLDN1), claudin 4 (CLDN4), zonula occludens-1 (ZO-1), and zonula occludens-2 (ZO-2). They showed that there was a significant increase in ZO-1, OCLN, and ZO-2 after LARS. The goal of this systematic review is to summarize and investigate the current literature regarding the functional and molecular ERB in humans and the influence of LARS on its improvement.
Materials and Methods
A multi-database search was performed. The literature search strategy was converted using the PICO (Population-Intervention-Comparison-Outcomes) Framework. 5 The patient population of interest was patients with GERD. The studied intervention was surgical (LARS) or endoscopic therapies for GERD. Outcome measures of interest were changes in the molecular and cellular components of the ERB, as well as improvement in GERD symptoms measured using both objective and subjective measurements (like questionnaires).
Pubmed, Embase, MEDLINE, and the Cochrane Library were searched from the earliest available date of each database through April 12, 2026. We used a search string containing following keywords and the search string was modified for each database: ([Anti-Reflux Surgery OR LARS OR Toupet Fundoplication OR Nissen Fundoplication OR Dor Fundoplication OR Reflux Stop OR Linx] AND [Mucosal remodeling OR Esophageal Barrier Function OR Cytokine production]).
The literature search was performed by two authors individually. Firstly, they screened and selected studies based on title and abstract. After the primary selection process, both authors reviewed the full texts of the selected studies and independently determined whether the article could be included in the systematic review based on predefined inclusion criteria. Both authors screened cross-references for further eligible studies. Any disagreements were resolved through discussion with each other and the senior author until consensus was reached. The protocol of this systematic review was not registered in advance.
Inclusion criteria
Study designs: randomized controlled trial, prospective cohort study, retrospective cohort study, case–control studies, and cross-sectional study. Studies including patients with GERD. Studies including patients who underwent anti-reflux surgery (either open, laparoscopic, or robotically) or endoscopic treatment for GERD. Outcome measurements: changes in molecular and cellular components of the ERB and symptom improvement of GERD, measured objectively or subjectively. Studies reporting changes in ECAD, OCLN, CLDN1, CLDN4, ZO-1, and ZO-2 were of interest.
Methodological quality assessment
The Newcastle–Ottawa Scale (NOS) was used to assess the methodological quality of the included studies. 6 The NOS is a visual system in which stars are awarded for each quality item. In total, nine stars can be allocated, in which the highest quality studies will have a total score of 9 stars. Risk of bias is assessed in three domains: selection of study groups, comparability of groups, and ascertainment of exposure and outcomes (in each of these domain’s studies can be awarded four points, two points, and three points, respectively). 6 Two authors have separately assessed the methodological quality of the included studies using the NOS. To compare the level of agreement between these two authors a Cohen’s kappa was calculated. 5 A Cohen’s kappa score < 0.20 indicates poor agreement, 0.21–0.40 fair agreement, 0.41–0.60 moderate agreement, 0.61–0.80 good agreement, and 0.81–1.00 very good agreement. 5
Results
The primary literature search produced 110 results, including six duplicates. After screening on title and abstract, 15 studies were found possibly relevant and underwent a full-text critical appraisal, resulting in 14 exclusions. Reasons for exclusion were the following: studies on only peristalsis or pH monitoring without other assessments,7–15 anatomical studies, 16 experimental treatment options,17,18 and narrative reviews.19,20 Only the study by Ergun et al. 4 fulfilled the inclusion criteria and was therefore included in this systematic review. Figure 1 summarizes the search results according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 21 The methodological quality of the included study ranges was good, indicated by the NOS for nonrandomized trials (Table 1). 6 A Cohen’s kappa of 0.75 reflected a good agreement between the two authors that conducted the search strategy. Table 2 gives an overview of the results of the included studies.
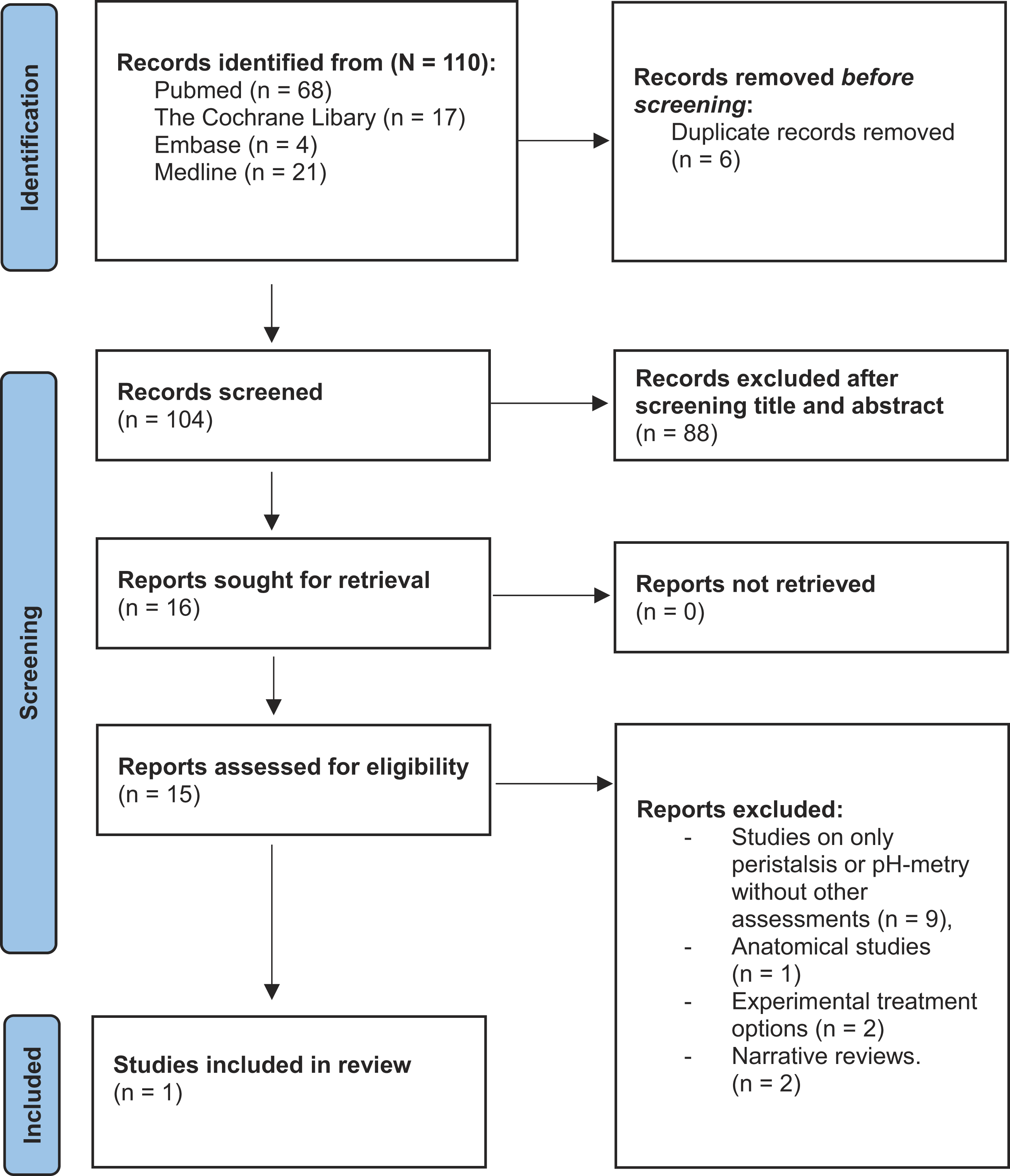
PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Assessment of Methodological Quality Using the Newcastle–Ottawa Scale for Nonrandomized Trials
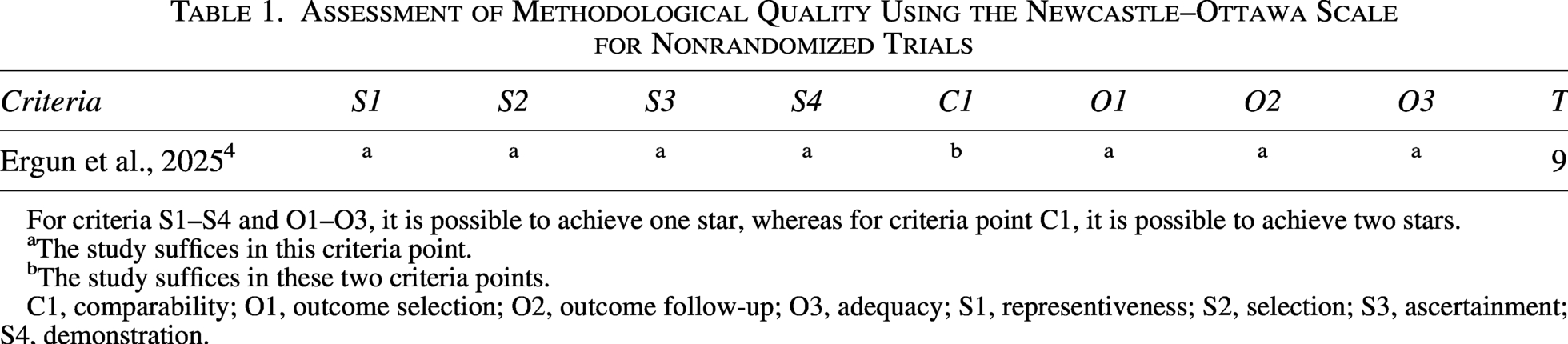
For criteria S1–S4 and O1–O3, it is possible to achieve one star, whereas for criteria point C1, it is possible to achieve two stars.
The study suffices in this criteria point.
The study suffices in these two criteria points.
C1, comparability; O1, outcome selection; O2, outcome follow-up; O3, adequacy; S1, representiveness; S2, selection; S3, ascertainment; S4, demonstration.
Results of Studies Included in This Systematic Review
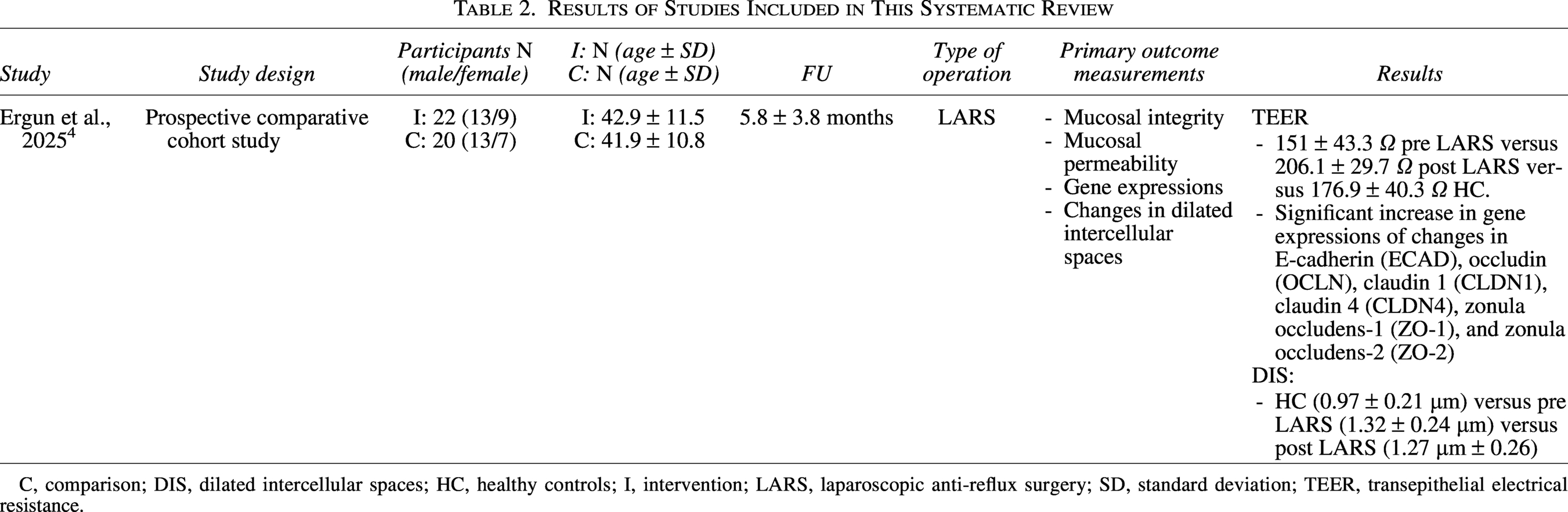
C, comparison; DIS, dilated intercellular spaces; HC, healthy controls; I, intervention; LARS, laparoscopic anti-reflux surgery; SD, standard deviation; TEER, transepithelial electrical resistance.
Included studies
Ergun et al. 4 investigated 23 patients before and after LARS and compared them with 20 healthy controls to evaluate the molecular and functional recovery of esophageal barrier integrity. Upper gastrointestinal endoscopies were performed after a mean follow-up period of 5.8 ± 3.8 months.
To assess mucosal integrity and permeability, transepithelial electrical resistance (TEER) measurements were performed. TEER values showed asignificant difference after LARS compared with preoperative values and with those of the healthy control group (206.1 ± 29.7 Ω, 151.0 ± 43.3 Ω, 176.9 ± 40.3 Ω, respectively). In terms of mucosal permeability, it was seen that there was a decrease after LARS (post LARS 29.7 ± 18.1 pmols versus 43.3 ± 19.2 pmols, P = .008). A negative correlation was found between TEER and permeability (r = − 0.4622, P = .0002). 4
When evaluatingdilated intracellular spaces (DIS), the control group was significantly lower (0.97 ± 0.21 µm) compared with both the preoperative (1.32 ± 0.24 µm) and postoperative (1.27 ± 0.26 µm) groups (P < .001).
After LARS there was a significant increase of mRNA gene expressions. ECAD rose 1.7-fold, ZO-1 increased 3.5-fold, and ZO-1 increased 1.8-fold. All of them showed a significant increase after LARS compared with the preoperative values. There was no correlation between these genes with either permeability or TEER. DIS and OCLN were shown to be negatively correlated (r = − 0.3359, P = .026).
Discussion
This systematic review illustrates a significant lack of understanding of the molecular and functional ERB and its potential differences after surgery or other endoscopic treatment modalities for GERD. In current literature, there is a focus on the anatomical and physiological function of ERB, as described in the position paper by the American Foregut Society 3 ; however, we have to keep into account that there is a complex interplay between the anatomy and physiological responses induced by LARS. 4 Given the fact that LARS has a very high success rate in alleviating reflux symptoms (especially in expert centers), it is likely that both inflammatory responses caused by the reflux and epithelium changes are responsible for this. 22
In general, due to a lack of protective mechanisms, the esophagus is vulnerable to (mucosal) injury from gastric acid, digestive enzymes, and other irritants.23–25 The primary response of the esophageal mucosa is to secrete, or increase the secretion of, bicarbonate to neutralize the injury done by the acid through the action of carbonic anhydrase-III. 26 Unfortunately, the presence of acid in the esophagus downregulates the production and expression of ECAD, resulting in increased cellular permeability and, thus, greater mucosal damage. 27 In addition, increased expression of proton pumps in esophageal tissue may induce local acid secretion, which can also cause inflammation, mitochondrial damage, and potentially carcinogenic effects. 28 Another potential damaging enzyme for esophageal mucosa is pepsin, which is a group of proteases that are secreted by chief cells in the stomach.28,29 Under acidic conditions, pepsinogen (its precursor) is converted in pepsin (active form) by cleavage of acid-labeled bonds, which initiate digestion of proteins. 30 Pepsin can, therefore, damage the proteins of mucous membranes and epithelial barrier by digesting the intercellular (tight) junctions. Furthermore, the presence of pepsin downregulates the carbonic anhydrase-III levels, which play an important role in protection of the damaging effects of gastric contents to the esophageal mucosa.31,32
Under normal conditions carbonic anhydrase-III induce bicarbonate secretion, leading to alkalinization of the esophageal (micro) environment and deactivate of pepsin. Logically, when the activity of carbonic anhydrase-III is reduced, an acidic environment maintains and therefore pepsin remains active.29,33 Pepsin operates at a pH of 2–3.2, it still remains active at much higher pH levels (around 6.5), which means when present in the oral cavity and/or respiratory tract it can still inflict damage. 31 As reported earlier, pepsin negatively regulates ECAD levels but also increases the production and release of β-catenin, a molecule that increases the risk of tumor cell infiltration and metastasis.29,34 β-catenin is known to accumulate in the cytoplasm and induces transcription of various oncogenes. These oncogenes are associated with carcinogenesis and tumor progression through the Wnt/β-catenin pathway.35,36 Furthermore, pepsin can be reactivated in environments with a low pH, due to endocytosis and therefore causing mitochondrial damage and promoting the expression of oncogenes.29,33–37
Another important contributor to GERD is the reflux of bile acids, which can also induce inflammatory damage to the esophageal mucosa. 36 The physiological function of bile acids is to facilitate the absorption and digestion of fats and fat-soluble nutrients in the small intestine. 38 In case of biliary acid reflux in the distal portions of the esophagus, epithelial-to-mesenchymal cell transformation may occur through vascular endothelial growth factor signaling 39 and NF-κB activation, leading to local inflammation and abnormal expression of tumor-related factors.40,41 Secondary, trypsin activates the protease-2 receptor, which induces IL-8 secretion, an interleukin involved in inflammatory response. Collectively, these mechanisms alleviate oxidative stress and pro-inflammatory cytokine production in the mucosa of the esophagus.42–44
Translating these pathophysiological findings is a very challenging task, since the literature on cytokine responses after LARS is scarce,45–48 and studies specifically assessing mucosal and/or tissue integrity are even more scarce.4,22
Therefore, based on the current literature, it is very difficult to make any conclusions, which is also the limitation of this systematic review. Future research studies need to further elucidate mechanisms responsible for the changes in ERB induced by anti-reflux surgery.
Conclusion
ARS is responsible for many anatomical and physiological mechanism, many of which are not fully understood. ARS may have positive effects on the mucosal and functional esophageal reflux barrier; however, further prospective studies need to further elucidate this.
Authors’ Contributions
M.E. and S.P.: Initial idea. M.E. and S.P.: Data collection. M.E., S.P., A.A., D.B., L.B., O.T., S.S., and J.L.: Data analysis. M.E., S.P., A.A., D.B., L.B., O.T., S.S., and J.L.: Writing and correcting the article. M.E., S.P., A.A., D.B., L.B., O.T., S.S., and J.L.: Final approval.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.