
Abstract
Purpose:
Multiple techniques have been described for laparoscopic inguinal hernia repair in children. The purpose of this study was to describe our experience using cautery and Endoloops in pediatric female patients.
Methods:
We conducted a retrospective review of pediatric female patients who underwent laparoscopic inguinal hernia repair using cautery and Endoloops at our center. This technique involves establishing laparoscopic access through the umbilicus, everting and cauterizing the hernia sac with a Maryland dissector, and placing two PDS Endoloops at the level of the internal ring. Outcomes included operative time and complications.
Results:
We identified 50 female patients (mean age 5.6 years, range 2 months to 17 years) who underwent laparoscopic inguinal hernia repair using cautery and Endoloops from January 2015 to March 2024. The indication for surgery in most patients was a clinical hernia (n = 43/50). One of these was incarcerated and another was a recurrent hernia. Seven other patients underwent ligation of an incidental patent processus vaginalis during laparoscopic appendectomy (n = 4), laparoscopic ovarian detorsion (n = 2), or diagnostic laparoscopy for possible Meckel’s diverticulum (n = 1). Median operative time was 30 minutes for unilateral inguinal hernias (n = 26/43) and 33 minutes for bilateral (n = 17/43). None experienced conversion to open procedure, surgical site infection, or recurrence.
Conclusion:
We conclude that laparoscopic inguinal hernia repair using cautery and Endoloops is safe and effective in pediatric female patients. This technique does not require specialized skills, training, or equipment. We have used this approach for primary repair of clinical hernia, incarcerated hernia, recurrent hernia, and incidental patent processus vaginalis.
Introduction
Inguinal hernias in children are repaired with high ligation of the hernia sac via open or laparoscopic surgery.1–4 With the open approach, a transverse incision is made in the inguinal area, the hernia sac is dissected off the surrounding structures, and the sac is ligated with sutures. 5 While this approach is effective in most cases, open surgery can still result in surgical site infection, recurrence, and other postoperative complications. 6
Many techniques have been described for laparoscopic inguinal hernia repair in children. Some involve intracorporeal suturing, and others involve extracorporeal suturing and/or tying. 7 The benefits of the laparoscopic approach include good visual exposure, excellent cosmetic results, shorter recovery times, and similar rates of recurrence.8,9 Laparoscopy may be especially helpful in cases of recurrent inguinal hernia following open surgery, since it avoids the need to dissect through scarred tissue planes. Laparoscopic repair may also be associated with a shorter operative time in cases of bilateral inguinal hernias. Multiple studies have suggested that laparoscopic inguinal hernia repair can be safe and effective in the pediatric population. 10
Many of the techniques described for laparoscopic inguinal hernia repair in children have an associated learning curve or require advanced laparoscopic skills. For example, a study by Safa et al. assessed the long-term outcomes of 1952 children who underwent inguinal hernia repair from 2011 to 2015 via open or laparoscopic surgery. 11 Patients in this study had a minimum follow-up of 4 years and a median follow-up of 6.6 years. Children in the laparoscopic group were treated with Subcutaneous Endoscopic-Assisted Ligation (SEAL), as described by Ozgediz et al. 12 This technique involves passing suture material around the hernia sac using a percutaneous spinal needle. Laparoscopic guidance is used to ensure that the sac is encircled and that the critical sutures (including the vas deferens and testicular vessels in boys) are not injured. High ligation is performed by tying the sutures extracorporeally. In this study, children who underwent laparoscopic repair had a lower rate of developing a metachronous inguinal hernia (1.4% vs. 3.8%, P = .047) but a higher rate of recurrence (9% vs. 0.9%, P < .001). The authors concluded that the higher than usual recurrence rate reflects “real-world” experience amongst a large group of surgeons with adequate long-term follow-up.
Some of the techniques reported for laparoscopic inguinal hernia repair in children do not require advanced laparoscopic skills and are not associated with such a high recurrence rate. In 1997, El-Gohary described his experience with laparoscopic inguinal hernia repair in pediatric female patients using Endoloops. 13 This technique involves eversion of the hernia sac and applying one or two Endoloops to perform high ligation. His original series included 28 females with unilateral (n = 24) or bilateral (n = 4) inguinal hernias. These patients ranged in age from 5 months to 10 years. Operative time was reported to be as short as 12–15 minutes for unilateral hernias and 15–20 minutes for bilateral cases. There was one recurrence early on in El-Gohary’s experience but none after that. Subsequent studies modified this technique by twisting or cutting the hernia sac.14–16 Like El-Gohary’s original series, pediatric female patients who underwent inguinal hernia repair with Endoloops had low recurrence rates. These included 0% among 30 patients, 0.8% among 173 patients, and 3.1% among 63 patients.14–16
One surgeon at our center (J.M.W.) first started performing laparoscopic inguinal hernia repair with cautery and Endoloops in pediatric female patients in 2015. Since then, multiple surgeons in our group have adopted this technique for elective inguinal repair and occasionally for closure of an incidental patent processus vaginalis discovered during another laparoscopic procedure.
The purpose of this study was to describe our experience with laparoscopic inguinal hernia repair in pediatric female patients using cautery and Endoloops. We described the operative steps, patient characteristics, procedure time, and incidence of postoperative complications, including surgical site infection and recurrence. We hope that this will provide surgeons with a laparoscopic technique that has acceptable clinical outcomes and does not require advanced skills or training.
Methods
Study design and participants
This study was a retrospective chart review of pediatric female patients who underwent laparoscopic inguinal hernia repair using cautery and Endoloops at McMaster Children’s Hospital between January 2015 and March 2024. Electronic medical records were used to abstract demographic data, operative indications, and postoperative outcomes. Ethics approval for this study was obtained by the Hamilton Integrated Research Ethics Board (Project ID #17794).
Statistical analysis
Descriptive statistics were used to summarize patient demographics and baseline characteristics using Microsoft Excel. These included mean and range for age. Indications for surgery, conversion to open procedure, surgical site infection, and recurrence were reported as counts and frequencies. Operative time was defined as the number of minutes required for the surgeon to complete the procedure (i.e., “skin-to-skin” time rather than the total time spent in the operating room). Median operative time was reported separately for unilateral and bilateral repairs.
Operative technique
Laparoscopic inguinal hernia repair using cautery and Endoloops is performed under general anesthesia in the operating room. We use a standard laparoscopic setup with a 5 mm 30-degree laparoscope, reusable 5 mm trocars, and 5 mm laparoscopic instruments. We do not use 3 mm instruments because a standard PDS Endoloop is too large for a 3 mm port.
Access to the abdomen is achieved via Hasson technique through a transumbilical or infraumbilical incision. A 5 mm trocar is inserted with a blunt introducer. Diagnostic laparoscopy is performed to confirm the presence of unilateral or bilateral indirect inguinal hernias (Fig. 1). In the unlikely event of a direct inguinal hernia, we would recommend conversion to an open procedure to perform a tissue repair without mesh (e.g., Bassini).
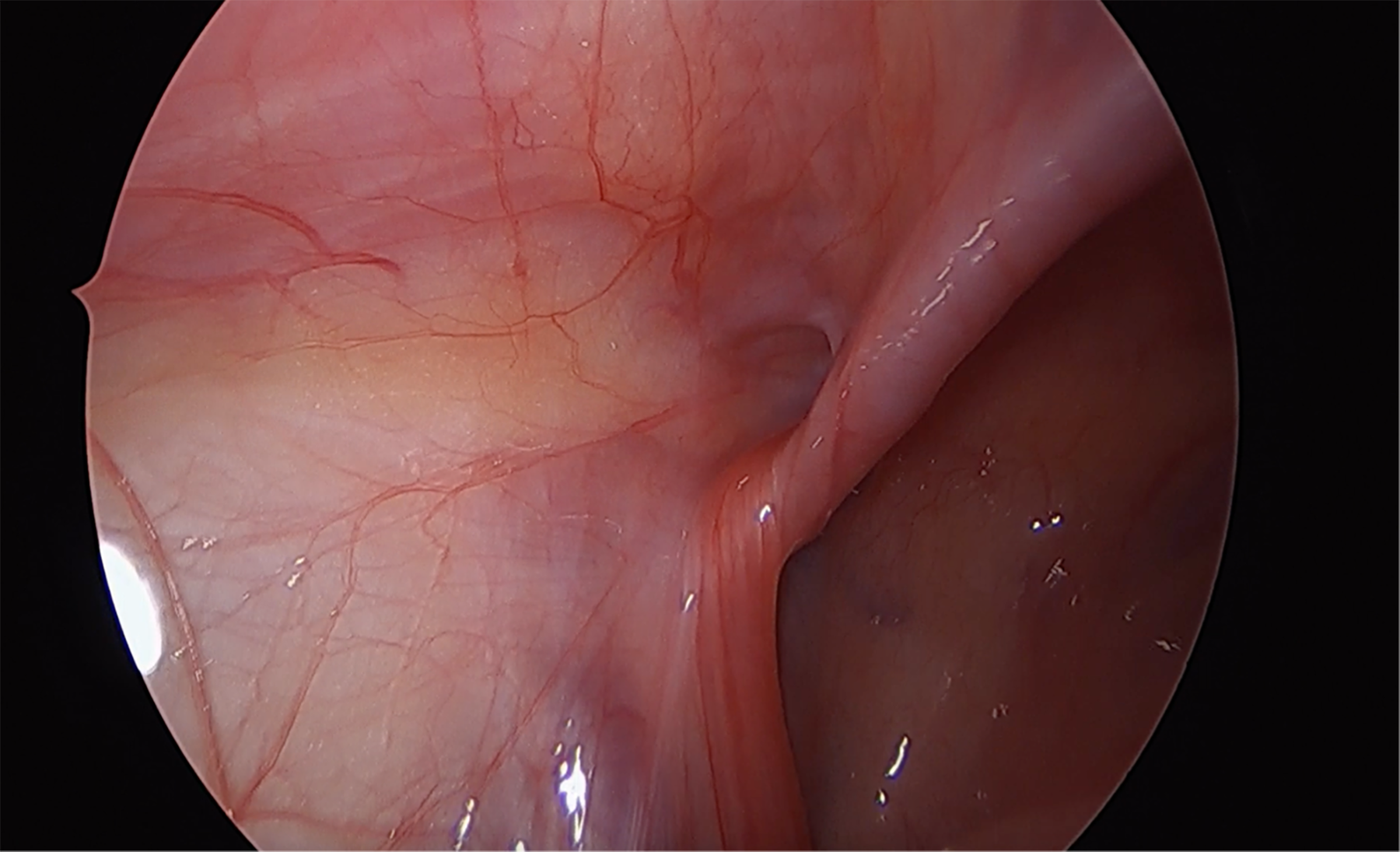
Laparoscopic view of inguinal hernia in a female patient.
Under direct visualization, we insert two 5 mm trocars to the right and left of the umbilicus. We confirm that the fallopian tube and ovary are not adherent to the hernia sac (i.e., that there is no element of a sliding hernia). If present, these structures can be carefully mobilized off the hernia sac using sharp dissection with laparoscopic Metzenbaum scissors or limited amounts of hook electrocautery. Care should be taken to avoid making a hole in the hernia sac.
To complete the repair, the most distal portion of the hernia sac is grasped and everted with a Maryland grasper (Fig. 2). This sometimes requires passing the sac “hand over hand” with a Maryland dissector in one hand and another laparoscopic grasper (e.g., a laparoscopic bowel grasper) in the other. Traction is maintained while the surgeon works to grasp the most distal portion of the everted hernia sac. Once the sac is fully everted with the Maryland dissector, we apply a limited amount of cautery via the Maryland (Fig. 3). This often causes the everted sac to remain in place. We do not use an excessive amount of cautery. This could cause a thermal injury to the surrounding structures or create a defect in the peritoneum and lead to a recurrence.

Eversion of the hernia sac using a Maryland dissector.

Application of cautery to the everted hernia sac.
After applying cautery to the hernia sac, we place two 0 PDS Endoloops at the level of the external ring. This requires an assistant to maintain traction with the Maryland dissector while each Endoloop is tightened (Figs. 4 and 5). The Endoloops should be snug enough that they do not slip off, but not so tight they tear the peritoneum. We do not recommend applying cautery after the placement of Endoloops, as this can cause the suture material to split and become dislodged.

Applying an Endoloop to the hernia sac at the level of the internal ring.

The completed repair with two Endoloops securely in place.
The repair is repeated on the contralateral side in cases of bilateral inguinal hernia. Once complete, the abdomen is desufflated. The fascia at the umbilicus is closed using a simple interrupted or figure-of-eight stitch with a heavy dissolvable suture (e.g., 0 Vicryl). The skin incisions are closed with subcuticular stitches and covered with dressing. The patient is discharged home the same day.
Results
Our study cohort included 50 pediatric female patients who underwent laparoscopic inguinal hernia repair with cautery and Endoloops between January 2015 and March 2024. Mean age was 5.6 years (ranging from 2 months to 17 years). Median weight was 21.4 kg (ranging from 2.8 to 68.3 kg). Eight of 50 participants (16%) had comorbidities, including prematurity (n = 3/50) or other conditions, such as juvenile polyposis, ovarian teratoma, sleep disorders, anxiety, and previous eye surgery (n = 5/50).
The most common indication for surgery was a clinical inguinal hernia (n = 43/50). Among these patients, one had an incarcerated inguinal hernia containing an ovary, and another had a recurrent inguinal hernia after a previous attempted repair using the SEAL technique. The remaining seven patients underwent ligation of an incidental patent processus vaginalis that was identified during another laparoscopic procedure. These included appendectomy (n = 4), ovarian detorsion (n = 2), and diagnostic laparoscopy for possible Meckel’s diverticulum (n = 1).
The median operative time for patients who underwent inguinal hernia repair as the sole procedure was 30 minutes for unilateral repairs (n = 26/43) and 33 minutes for bilateral repairs (n = 17/43). All cases were completed without conversion to open surgery. None of the patients in our cohort experienced a surgical site infection or recurrence. Nineteen patients (38%) completed a follow-up appointment in our outpatient clinic. These occurred at a mean of 4.8 months post-operatively (ranging from 1 week to 29 months after surgery). One patient presented to the emergency department due to pain at one of the laparoscopic port sites. This individual did not develop a surgical site infection or other complications.
Discussion
This study suggests that laparoscopic inguinal hernia repair using cautery and Endoloops is safe and effective in pediatric female patients. Over the study period, we did not identify any patients who experienced conversion to open surgery, surgical site infection, or recurrence. We have used this technique in a variety of settings, including the primary repair of a clinical hernia (both unilateral and bilateral), incarcerated hernia, recurrent hernia, and closure of an incidental patent processus vaginalis identified during another laparoscopic procedure.
Laparoscopic inguinal hernia repair using cautery and Endoloops is technically simple, does not involve specialized equipment, and does not require advanced training. A variety of other techniques have been described for laparoscopic inguinal hernia repair in children.9,10,12,17–20 Some of these involve intracorporeal suturing and other advanced techniques. We believe that all pediatric surgeons should be able to perform intracorporeal suturing and should maintain these skills with regular practice. However, some clinicians may be hesitant to use intracorporeal suturing during inguinal hernia repair, especially if their current approach is open surgery.
Another advantage of laparoscopic inguinal hernia repair is the ability to perform direct visualization of the internal rings. This facilitates the detection of a contralateral defect and decreases the risk of metachronous hernia. 11 The laparoscopic approach also minimizes tissue trauma, results in smaller incisions, and is associated with shorter operative time for bilateral inguinal hernia repair. Conversely, open surgery avoids the risks associated with laparoscopy and allows surgeons to reinforce the floor of the inguinal canal, which may be an important consideration in adolescents. 21
Some pediatric surgeons use cautery alone to perform laparoscopic inguinal hernia repair in female patients.22,23 This technique is sometimes referred to as a “burnia” repair. While this method is straightforward, there are concerns about the risk of thermal injury to adjacent structures, and the possibility of incomplete sac closure leading to recurrence.22,23 Other surgeons have opted to use Endoloops only, which provides secure ligation of the hernia sac, but may lead to knot slippage and recurrence. The technique described in the current study is unique because both cautery and Endoloops are used. This combines the efficacy of cautery with the reliability of a mechanical closure. This may explain why there were no recurrences in our series.
This study has several limitations. Our cohort included 50 patients treated at a single children’s hospital, which may limit the generalizability of the findings. Another important limitation is the duration and frequency of follow-up. At our center, children are only seen for follow-up after inguinal hernia repair if there is concern for complications or at the request of the patient’s family. The majority of families do not opt for routine follow-up in clinic. McMaster Children’s Hospital is the only children’s hospital in a regional catchment area of 2.4 million residents, but it is possible that some patients may have developed complications and presented to another center, especially if they moved. As a result, adverse events may have been underreported. This study also did not capture patient-reported outcomes, such as quality of life, pain, or satisfaction with the cosmetic appearance. Finally, we did not utilize a control group of pediatric female patients who underwent inguinal hernia repair via open surgery.
Future studies should explore the comparative effectiveness of different laparoscopic techniques for inguinal hernia repair in children. There is currently no gold standard among any of the laparoscopic approaches, suggesting that each technique may have advantages and disadvantages. The learning curve associated with different types of laparoscopic inguinal hernia repair in children is also not clear, especially among surgeons who have not undergone formalized training. While supervised practice should be provided to all surgeons who are planning to adopt laparoscopic inguinal hernia repair into their practice for the first time, the cautery and Endoloop technique is likely more accessible than other approaches (e.g., the SEAL technique). Many pediatric surgeons already use PDS Endoloops to ligate the appendix during laparoscopic appendectomy. Applying this technique to laparoscopic inguinal hernia repair is less novel for a surgeon than learning an approach that requires new skills or equipment.
Future research should assess long-term outcomes whenever possible to monitor for late recurrences, particularly in adolescents. While the primary cause of inguinal hernias in children is a patent processus vaginalis, weakness in the floor of the inguinal canal could be a contributing factor in adolescents. 21 The cautery and Endoloop technique requires minimal tissue handling and does not reinforce the floor of the inguinal canal. In contrast, open inguinal hernia repair also involves high ligation of the hernia sac and provides an opportunity to reinforce the floor of the inguinal canal with mesh or tissue if the surgeon feels that this might prevent a recurrence.
We conclude that laparoscopic inguinal hernia repair in pediatric female patients using cautery and Endoloops is safe and effective. This technique is one of many possible approaches for laparoscopic inguinal hernia repair in this sex and age group. Further studies are needed to determine which laparoscopic technique is best in children.
Authors’ Contributions
H.N.: Formal analysis, investigation, writing—original draft, and writing—review and editing. H.A.: Conceptualization, data curation, formal analysis, methodology, and writing—review and editing. D.B.: Conceptualization, data curation, formal analysis, methodology, and writing—review and editing. S.W.: Formal analysis and writing—review and editing. J.M.W.: Conceptualization, data curation, methodology, project administration, supervision, and writing—review and editing. M.H.L.: Conceptualization, data curation, methodology, project administration, supervision, and writing—review and editing.
Footnotes
Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.