
Abstract
Background:
Neurologically impaired children frequently experience recurrent gastroesophageal reflux symptoms after laparoscopic Nissen fundoplication, even when the fundoplication remains anatomically intact. Esophagogastric dysfunction may contribute to these recurrences but is often underrecognized.
Aim:
To analyze the causes of recurrent gastroesophageal reflux symptoms in neurologically impaired children with an intact Nissen fundoplication attributable to esophagogastric dysfunction and to describe their management and outcomes.
Methods:
We conducted a retrospective descriptive study of neurologically impaired children who underwent laparoscopic Nissen fundoplication between 2010 and 2025 and subsequently developed recurrent gastroesophageal reflux-related symptoms. All patients were evaluated with contrast upper gastrointestinal studies and upper gastrointestinal endoscopy; gastric emptying scintigraphy was performed when gastric atony was suspected. Demographic data, neurological diagnosis, Gross Motor Function Classification System level, nutritional status, symptoms, time to recurrence, imaging findings, treatment, and follow-up were recorded.
Results:
A total of 124 children were included (96 with cerebral palsy, 18 with traumatic brain injury, and 10 with brain tumors). At 36-month follow-up, 82 patients achieved complete symptom remission. Forty-two children, all with cerebral palsy, developed recurrent symptoms between 10 and 48 months after surgery. Recurrence was due to paraesophageal hernia in 15 patients, all of whom underwent successful laparoscopic redo fundoplication. The remaining 27 children had an anatomically intact fundoplication: 10 presented bile reflux with duodenitis and improved with medical management, and 17 had gastric, pyloric, or duodenal dysfunction requiring laparoscopic pyloroplasty, esophagogastric disconnection, or gastrojejunostomy, with subsequent resolution of symptoms.
Conclusions:
In neurologically impaired children, esophagogastric dysfunction unrelated to wrap failure is a frequent and surgically treatable cause of recurrent symptoms after Nissen fundoplication.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is common in children with neurological impairment and may affect up to 91% of these patients. 1 Nissen fundoplication is the procedure of choice and is indicated when symptoms such as irritability, drooling, heartburn, vomiting, malnutrition, aspiration pneumonia, or esophageal peptic complications persist. 2
However, recurrence of symptoms after surgery has been reported in up to 75% of patients. 3 Disruption of the fundoplication, either due to wrap rupture or herniation, 4 accounts for only about one third of cases, while many children develop recurrent symptoms because of esophageal or gastric motility disorders and delayed gastric emptying.5–7 Neurological impairment leads to delayed gastric emptying and motor dysfunction, further aggravated by spasticity, seizures, scoliosis, and constipation.8,9 Additional mechanisms, including impaired gastric accommodation and dumping syndrome, may cause relapse of reflux in up to 11.4% of cases despite an intact fundoplication. 10
These conditions fall under the broader concept of esophagogastric dysfunction, which encompasses disorders of esophageal and/or gastric function that lead to reflux despite a competent esophagogastric junction, whether native or surgically reconstructed by fundoplication. When reflux persists or recurs, it is essential to identify the underlying cause and determine the most appropriate treatment, which may include redo fundoplication or additional procedures such as pyloroplasty, esophagogastric disconnection, or bypass procedures.6–8
The aim of this study was to analyze the causes of recurrent gastroesophageal reflux symptoms in neurologically impaired children with an anatomically intact Nissen fundoplication attributable to esophagogastric dysfunction and to describe their management and outcomes.
Methods
This was a retrospective descriptive study. We included pediatric patients with neurological impairment who had undergone laparoscopic Nissen fundoplication and subsequently developed recurrent GERD-related symptoms. All patients underwent contrast upper gastrointestinal studies and upper gastrointestinal endoscopy; gastric emptying scintigraphy was performed when gastric atony was suspected.
The following variables were analyzed: age, sex, weight, nutritional status, comorbidities, Gross Motor Function Classification System (GMFCS) level, symptoms, time to symptom recurrence, radiological findings, endoscopic findings, scintigraphic findings, diagnosis, treatment, complications, and follow-up. Descriptive statistics were used, and data are reported as means, ranges, and relative frequencies.
Results
Between 2010 and 2025, 124 children with GERD and neurological impairment were treated with laparoscopic Nissen fundoplication. Neurological impairment was due to cerebral palsy in 96 patients (77.41%), traumatic brain injury in 18 (14.5%), and brain tumors in 10 (8.06%). Age at surgery ranged from 1 to 15 years (mean 8.52 years); 61% of patients were older than 7.8 years. Regarding nutritional status, only 7 children (5.6%) had adequate weight for age, 20 (16.1%) had grade I malnutrition, 25 (20.16%) had grade II malnutrition, and 72 (58.06%) had grade III malnutrition.
Among the 96 patients with neurological impairment secondary to cerebral palsy, the distribution according to the GMFCS was as follows: 12 children were not classified because they were younger than 2 years, 11 were level III, 48 were level IV, and 25 were level V. The antireflux procedure was combined with gastrostomy in 106 patients (85.48%); 8 children (6.45%) already had a gastrostomy, which was taken down to perform the fundoplication, and only 10 (8.06%) did not undergo gastrostomy.
Eighty-two children (66.12%) achieved GERD control with complete symptom remission at 36-month follow-up. Forty-two patients (33.87%) developed recurrent GERD-related symptoms; all had neurological impairment due to cerebral palsy. Symptom recurrence occurred between 10 and 48 months after surgery (mean 36.2 months). Presenting features included irritability, cough, heartburn, arching, recurrent pneumonia, and late gastrostomy-related complications such as peristomal gastric leakage and gastrostomy prolapse. All of these patients underwent esophagogastroduodenal contrast studies and upper gastrointestinal endoscopy.
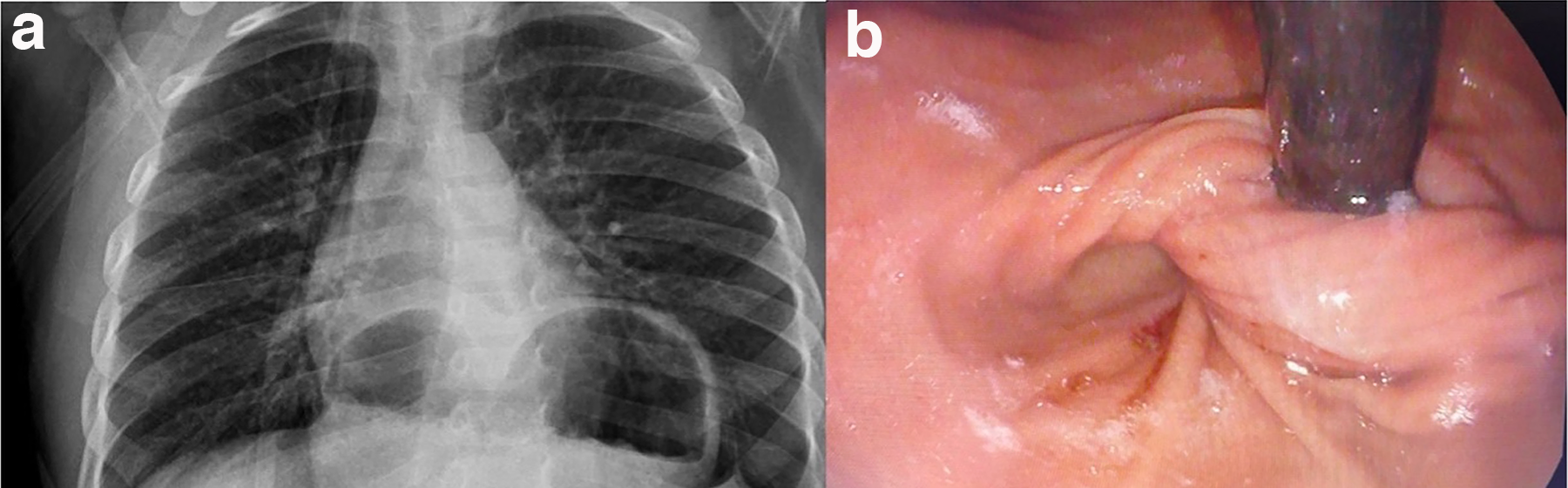
In 15 children (12.09% of the entire cohort), recurrence of symptoms was secondary to fundoplication dysfunction, with a paraesophageal hernia demonstrated on imaging and endoscopy. All underwent redo fundoplication with repair of the phrenoesophageal membrane, with good postoperative outcomes (Fig. 1a,b).
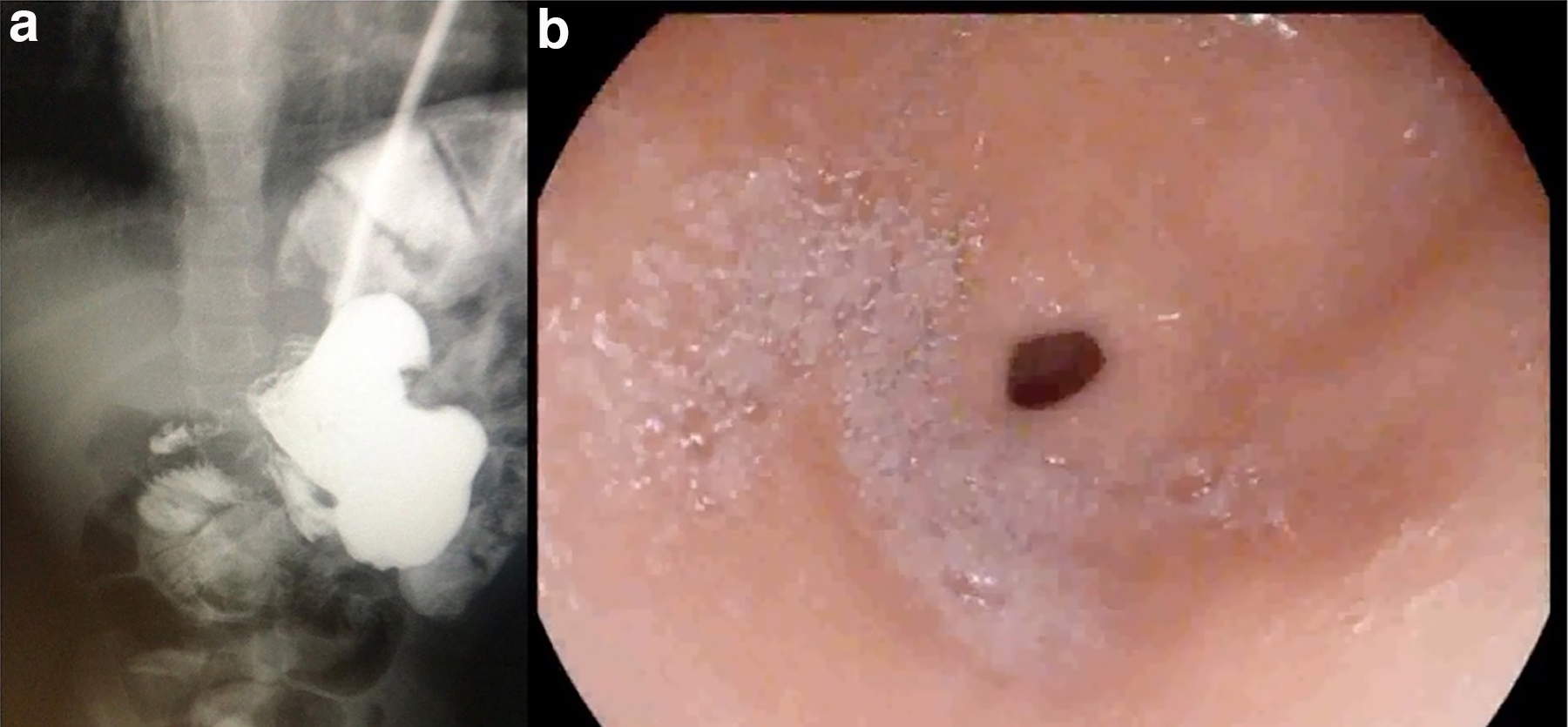
In the remaining 27 patients, the fundoplication was anatomically intact (Fig. 2). Ten of them had no additional structural abnormalities but showed bile reflux associated with duodenitis, characterized by a nodular mucosal pattern on endoscopy and normal pyloric motility during air insufflation; biopsies revealed chronic inflammation with eosinophilia. These patients were treated with sucralfate and dietary modifications, achieving complete symptom remission (Fig. 3).
Endoscopic image of the duodenum with a nodular mucosal pattern consistent with duodenitis. Prolapsed gastric mucosa with vascular compromise protruding through the gastrostomy tract.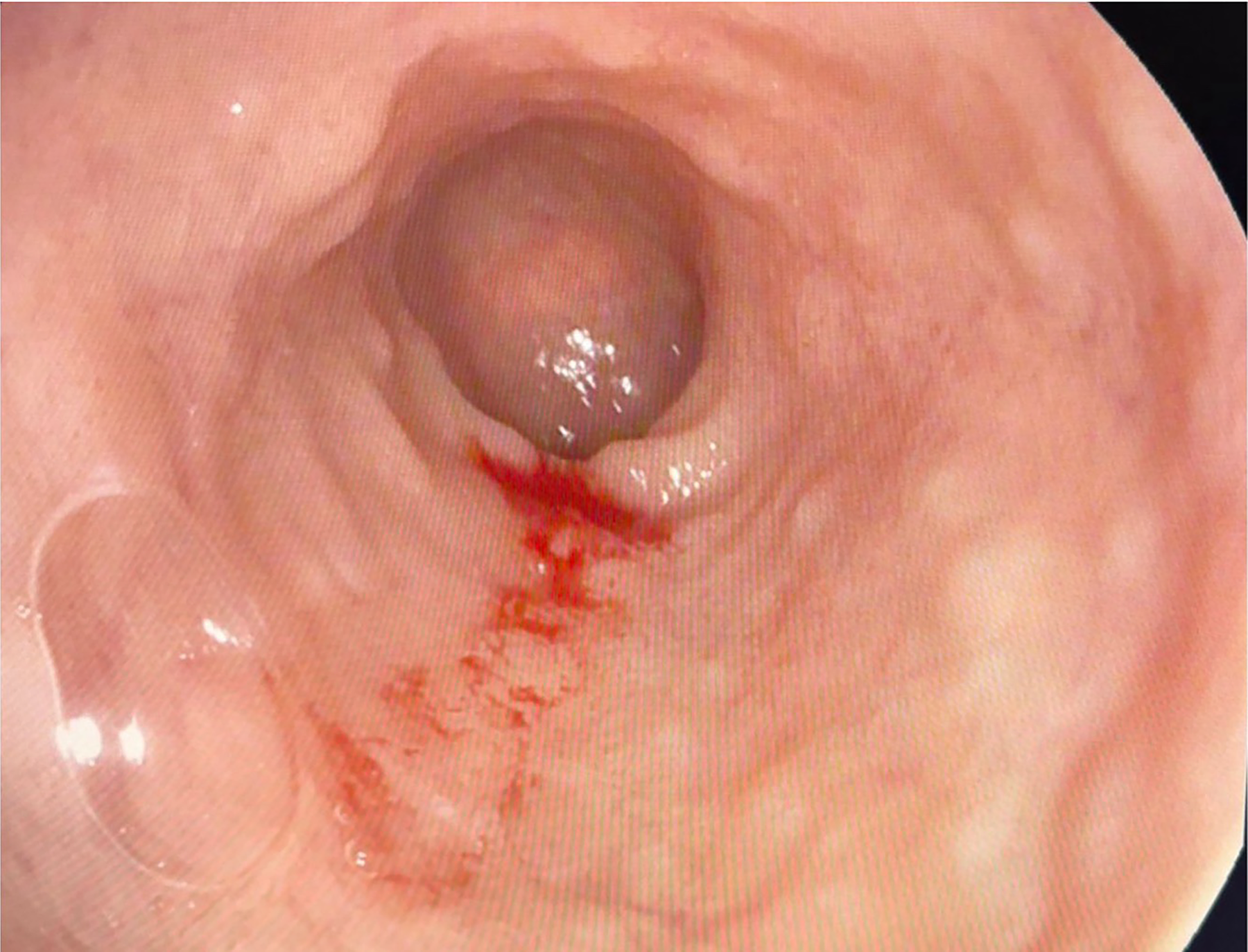

In the remaining 17 patients, different gastric and pyloric abnormalities responsible for symptom recurrence were identified and grouped according to radiological and endoscopic findings:
Nine patients with an intact fundoplication and inability to pass the endoscope through the pylorus. Their ages ranged from 2 to 6 years, and symptoms appeared 10–31 months after the initial surgery. All had GMFCS level IV and late gastrostomy-related complications, including peristomal leakage and gastric prolapse through the gastrostomy site. All underwent laparoscopic Mikulicz-type pyloroplasty without complications, with resolution of symptoms (Fig. 4). Four patients with an intact fundoplication and absent antral and pyloric movement during air insufflation on endoscopy. They were 5–8 years old, and symptoms developed 12–24 months after the initial surgery. The main manifestation was severe, recurrent pneumonia associated with feeding; two children had GMFCS level IV and two had level V. Two of these patients initially underwent redo fundoplication, despite a functionally adequate wrap, and continued to experience pneumonia. Contrast studies via the gastrostomy showed absent gastric emptying, and gastric emptying scintigraphy with a liquid test meal demonstrated marked delay in gastric emptying and GERD, with 80–90% gastric retention at 3 hours and a flat emptying curve compatible with gastric atony. All four children were eventually treated with laparoscopic esophagogastric disconnection, with complete symptom resolution at a minimum follow-up of 12 months (Fig. 5). Four patients with an intact fundoplication, abundant bile reflux, pyloric dilatation, and dilatation of the first portion of the duodenum on endoscopy. They were 12–15 years old, and symptoms started 8–10 years after the initial surgery. All had severe kyphoscoliotic deformity on physical and radiological examination, along with marked gastric dilatation. Diagnostic laparoscopy with simultaneous endoscopy showed duodenal dilatation secondary to compression by the superior mesenteric artery. All underwent laparoscopic gastrojejunostomy, with good clinical evolution and symptom control at 18-month follow-up (Fig. 5a,b and Table 1).
Gastric atony treated by esophagogastric disconnection.
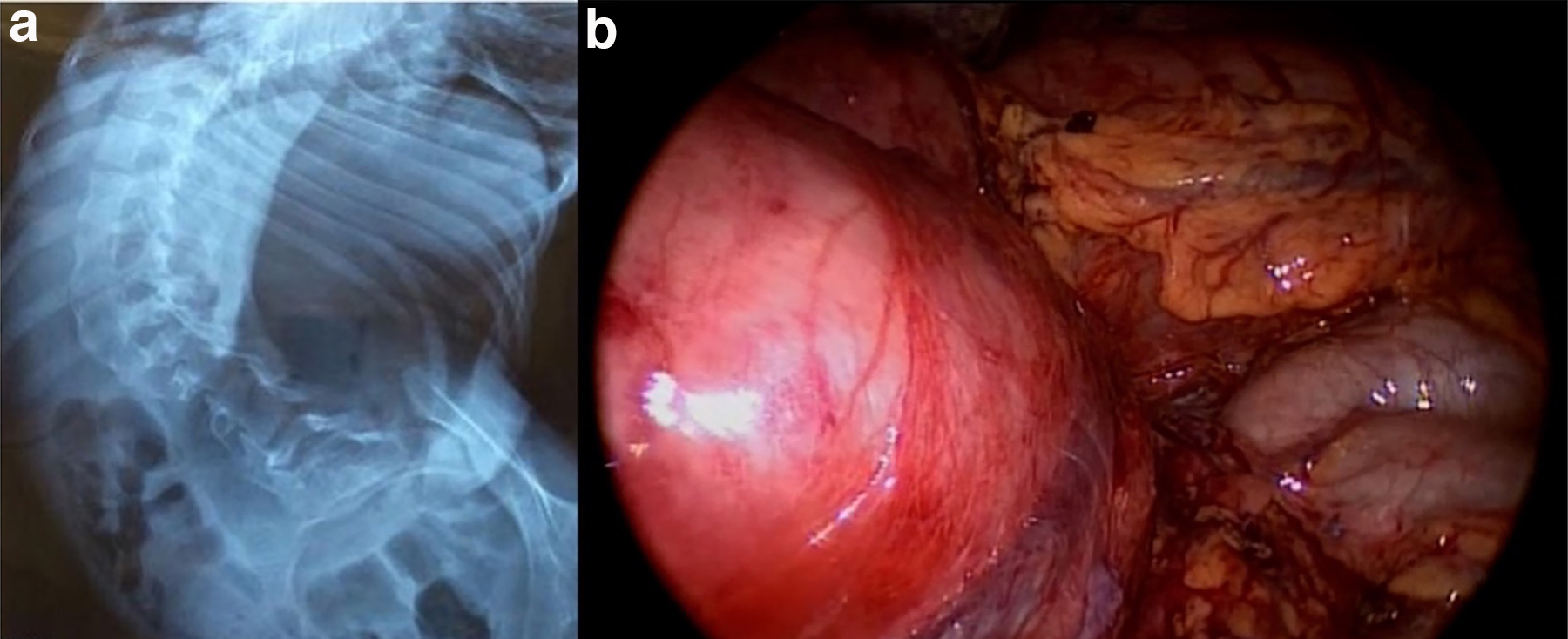
Duodenal obstruction due to superior mesenteric artery syndrome.

Discussion
When recurrent GERD-related symptoms appear, it is essential to assess both the integrity and the function of the fundoplication. Contrast studies and upper endoscopy are useful not only to evaluate the wrap but also to assess antral motility and the morphology of the pylorus and duodenum.11–14 In our cohort, 42 children (33.87%) had recurrent symptoms, but only 15 had recurrence due to paraesophageal hernia and wrap dysfunction, a rate similar to previously reported series in which 15%–25% of pediatric patients require reoperation for mechanical failure.12–14
The remaining 27 patients had a functionally intact fundoplication. Ten of them showed duodenal involvement with nodular mucosa and alkaline reflux gastritis and were successfully treated with prokinetics, sucralfate, and dietary changes. The other 17 children shared advanced motor impairment (GMFCS levels IV and V), reflecting more severe neurological damage and early onset of injury, all secondary to cerebral palsy. Neurologically impaired children have autonomic disturbances affecting vagal control of gastric motility, leading to impaired motor output to the antrum and pylorus and resulting in antral hypomotility, gastric paresis, and pylorospasm.15–18 This pathophysiology was evident in our cohort, either as pylorospasm resolved by a gastric emptying procedure or as gastric atony requiring esophagogastric disconnection.
In the remaining subgroup, severe kyphoscoliosis was a common finding and was associated with persistent vomiting and marked gastric dilatation. These skeletal deformities can cause the duodenum to become trapped between the spine and the superior mesenteric artery, leading to intestinal obstruction consistent with superior mesenteric artery syndrome, which we treated successfully with laparoscopic gastrojejunostomy. Together, these patterns illustrate esophagogastric dysfunction as a clinically relevant spectrum of gastric, pyloric, and duodenal abnormalities that can be targeted with tailored medical or surgical interventions.
Our study has some limitations, including its retrospective design, the absence of standardized high-resolution manometry or pH-impedance monitoring in all patients, and the potential for selection bias in a single-center cohort. Nevertheless, the relatively large sample size and homogeneous population of neurologically impaired children provide clinically relevant insight into mechanisms of symptom recurrence after Nissen fundoplication and highlight the need for systematic evaluation beyond wrap integrity alone.
Conclusions
Esophagogastric dysfunction is a major cause of recurrent gastroesophageal reflux-related symptoms in neurologically impaired children after Nissen fundoplication, even when the wrap remains anatomically intact. In our series, a substantial proportion of recurrences was related to gastric, pyloric, or duodenal abnormalities that were amenable to tailored medical or surgical treatment. Comprehensive radiological and endoscopic assessment should systematically include the antrum, pylorus, and duodenum, in addition to evaluation of the fundoplication itself, to identify specific patterns of dysfunction. Recognizing esophagogastric dysfunction as a distinct entity may prevent unnecessary redo fundoplications and support the selection of more effective, targeted interventions in this vulnerable population.
These findings support incorporating targeted assessment and management of esophagogastric dysfunction into standard algorithms for recurrent symptoms after fundoplication in neurologically impaired children.
Authors’ Contributions
C.G.-H.: Conceptualization, methodology, data curation, formal analysis, investigation, visualization, writing—original draft, writing—review and editing, supervision, project administration, and final approval of the submitted version. C.A.-G.: Investigation, visualization, writing—original draft, writing—review and editing, and final approval of the submitted version. D.L.H.-O.: Visualization, writing—review and editing, and final approval of the submitted version. L.C.-F.: Conceptualization, methodology, formal analysis, writing—review and editing, and final approval of the submitted version. All authors meet the ICMJE criteria for authorship and approved the final version of the article.
Ethics
This study was approved by the Institutional Research and Ethics Committee of Hospital Star Médica Infantil Privado and was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. The requirement for individual informed consent was waived due to the retrospective nature of the study, and all patient data were anonymized to ensure confidentiality.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to institutional and ethical restrictions related to patient confidentiality but are available from the corresponding author on reasonable request and with permission from the Institutional Research and Ethics Committee of Hospital Star Médica Infantil Privado.
Footnotes
Acknowledgments
The authors thank the surgical, anesthesiology, and nursing teams of Hospital Star Médica Infantil Privado for their support in the care of these patients. They used an AI-based language tool to assist with English language editing of this article. All scientific content, data interpretation, and conclusions are the sole responsibility of the authors.
Author Disclosure Statement
The authors declare that they have no conflicts of interest related to this study.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.