
Abstract
Background:
Subtotal cholecystectomy is an important bailout procedure for difficult cholecystitis cases. Two novel closure techniques have been described: the fenestrating method (F-method) using Endoloop ligation and the reconstituting method (R-method) using barbed sutures. This study aimed to compare the short- and long-term outcomes of these two techniques.
Methods:
This retrospective study included 52 patients who underwent laparoscopic subtotal cholecystectomy between January 2022 and December 2025, with 33 patients in the F-method group and 19 patients in the R-method group. The primary outcome was early postoperative complications. The secondary outcomes included late complications, operative time, and remnant gallbladder tissue on imaging.
Results:
Patients in the R-method group were significantly older (median: 72 versus 62 years, P = .021) and had more severe cholecystitis (Tokyo Guidelines grade ≥ II: 79.0% versus 45.5%, P = .023). Unclear anatomy was more common in the R-method group (84.2% versus 21.2%, P < .0001). Closure time was significantly shorter in the F-method group (4 versus 18 minutes, P < .0001). No bile duct injury, bile leakage, or mortality was observed in either group. Among patients who underwent postoperative imaging, remnant gallbladder tissue was identified in 35.7% of patients in the R-method group and 0% in those in the F-method group (P = .012). One patient in each group developed late complications that required readmission (F-method, common bile duct stone; R-method, remnant cholecystitis).
Conclusions:
Both methods are safe and have distinct complication profiles. The F-method eliminates remnant gallbladder tissue, whereas the R-method is suitable when complete dissection poses a risk of injury. Technique selection should be based on intraoperative findings.
Keywords
Introduction
Laparoscopic cholecystectomy (LC) for acute cholecystitis remains technically challenging, and avoiding vasculobiliary injury is of paramount importance.1–3 The Tokyo Guidelines 2018 (TG18) recommend several bailout procedures when safe completion of total cholecystectomy is not feasible, including conversion to open cholecystectomy, the fundus-first approach, and subtotal cholecystectomy (SC). 4 Among these bailout procedures, SC has emerged as a crucial technique for preventing major complications while maintaining a minimally invasive approach. Recently, laparoscopic SC (LSC) has been increasingly performed and is now widely recommended as an alternative in difficult cases.5–7
However, SC is associated with specific complications related to the gallbladder closure technique. The primary concerns include bile leakage from the closure site and late complications such as remnant cholecystitis and stone formation in the remnant gallbladder.8–16 The optimal closure method remains a subject of ongoing investigation, as the technique directly influences both early postoperative outcomes and long-term complications.
Gallbladder closure methods for SC are classified into fenestrating, which does not create a remnant gallbladder, and reconstituting, which does. 11 The guidelines describe needle-and-thread suture closure techniques; 4 however, these procedures are technically complex. As simpler alternatives, fenestrating using an Endoloop17–20 and reconstituting using barbed sutures21,22 have been reported. We implemented these two gallbladder closure methods at our institution; however, their short- and long-term outcomes remain unclear. Understanding the complication profiles and technical characteristics of these two closure methods is essential for appropriate surgical decision-making in difficult cholecystectomy cases.
Therefore, this study aimed to compare the short- and long-term outcomes of the fenestrating method using Endoloop ligation and the reconstituting method using barbed sutures in LSC and to characterize the features of each technique.
Methods
Study design and patient selection
This retrospective cohort study included patients who underwent LSC for cholecystitis or cholelithiasis at the Division of Digestive Surgery, Department of Surgery, Nihon University School of Medicine, between January 2022 and December 2025. Patients were divided into two groups based on the gallbladder closure technique: the fenestrating group (F-method, n = 33), in which the remnant gallbladder was closed with an Endoloop, and the reconstituting group (R-method, n = 19), in which the remnant was closed with barbed sutures. Inclusion criteria were (1) symptomatic cholelithiasis or cholecystitis and (2) American Society of Anesthesiologists Physical Status classification ≤3. The exclusion criteria were (1) conversion to open cholecystectomy, (2) closure of the gallbladder with a stapler, and (3) nonclosure of the gallbladder remnant (lay-open technique) (Fig. 1).
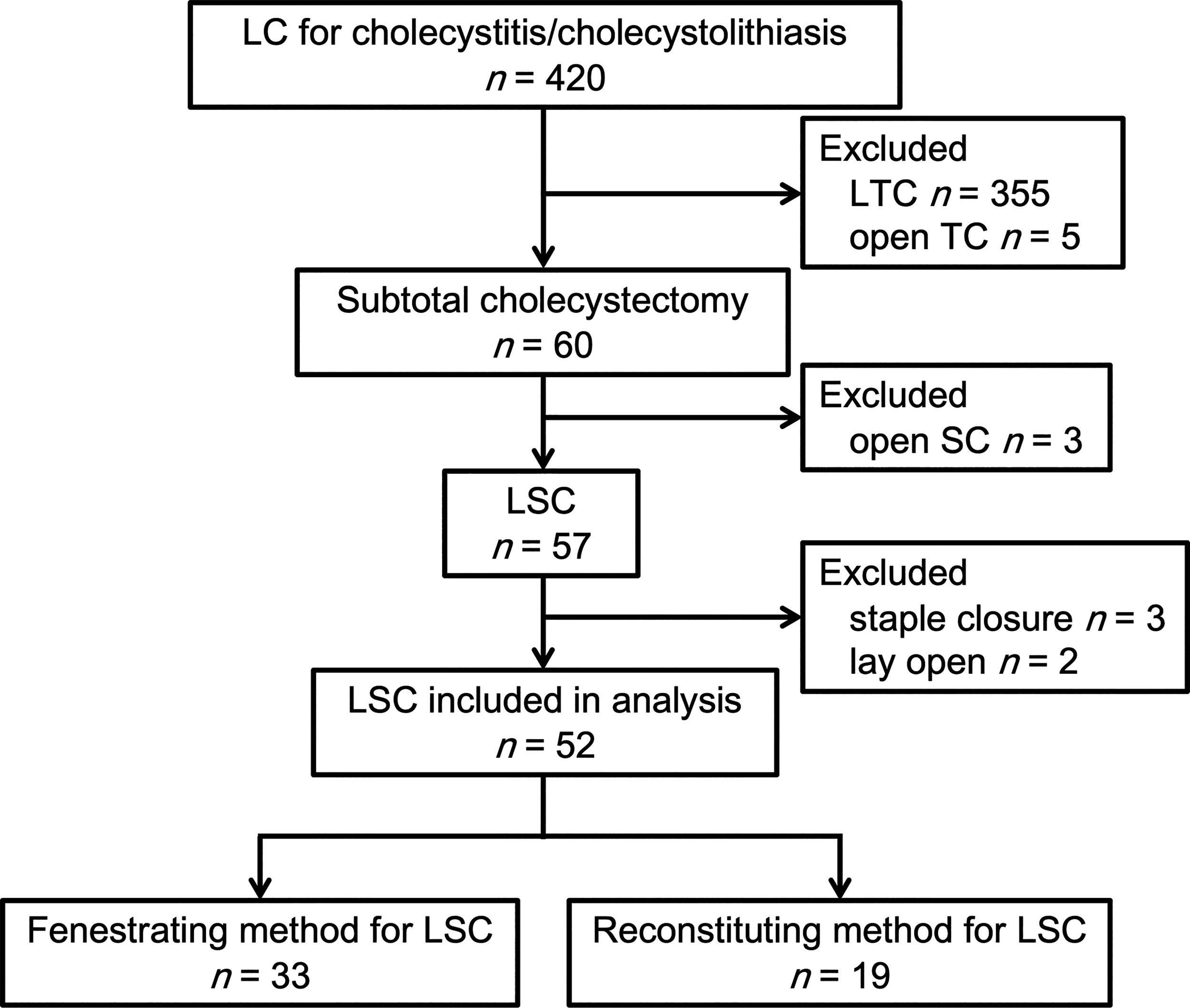
Flow diagram of patient recruitment (from 2022 to 2025). LC, laparoscopic cholecystectomy; LSC, laparoscopic subtotal cholecystectomy.
Surgical procedure
All procedures were performed using the conventional four-port LC technique. All cases followed the “safe steps” outlined in the TG18. 4 Initially, the posterior aspect of the gallbladder was dissected using the body-first approach. 23 When this proved difficult, the strategy was switched to the fundus-first approach. Indications for SC were classified into three categories: (1) inability to circumferentially encircle the gallbladder; (2) unclear anatomy in Calot’s triangle preventing safe identification and management of vascular structures; and (3) bleeding tendency during dissection. SC was defined as cases in which the gallbladder transection edge could not be closed using a Hem-o-lok ML clip (maximum closure diameter, 11 mm). All surgeries were performed by 15 surgeons in total (12 surgeons in the F-group and 10 surgeons in the R-group).
Fenestrating method
In cases where the gallbladder could be encircled at the posterior aspect of the infundibulum to the neck region, dissection was tracked as far distally as possible, and closure of the infundibulum to the neck was attempted using a Hem-o-lok ML clip (Teleflex, Wayne, PA, USA). When closure was not achievable with the clip, the gallbladder was completely mobilized from the gallbladder bed, and fenestration was performed by ligating the gallbladder from the external surface using an Endoloop (Ethicon, Somerville, NJ, USA). Before ligation with the Endoloop, the anterior wall of the gallbladder was incised, and the intraluminal space was inspected to confirm the absence of stones distal to the planned ligation site. In cases with endoscopic transpapillary gallbladder stenting, the stent was removed through this incision. The distal side of the incision was double-ligated with the Endoloop, and the gallbladder neck was transected (Fig. 2).
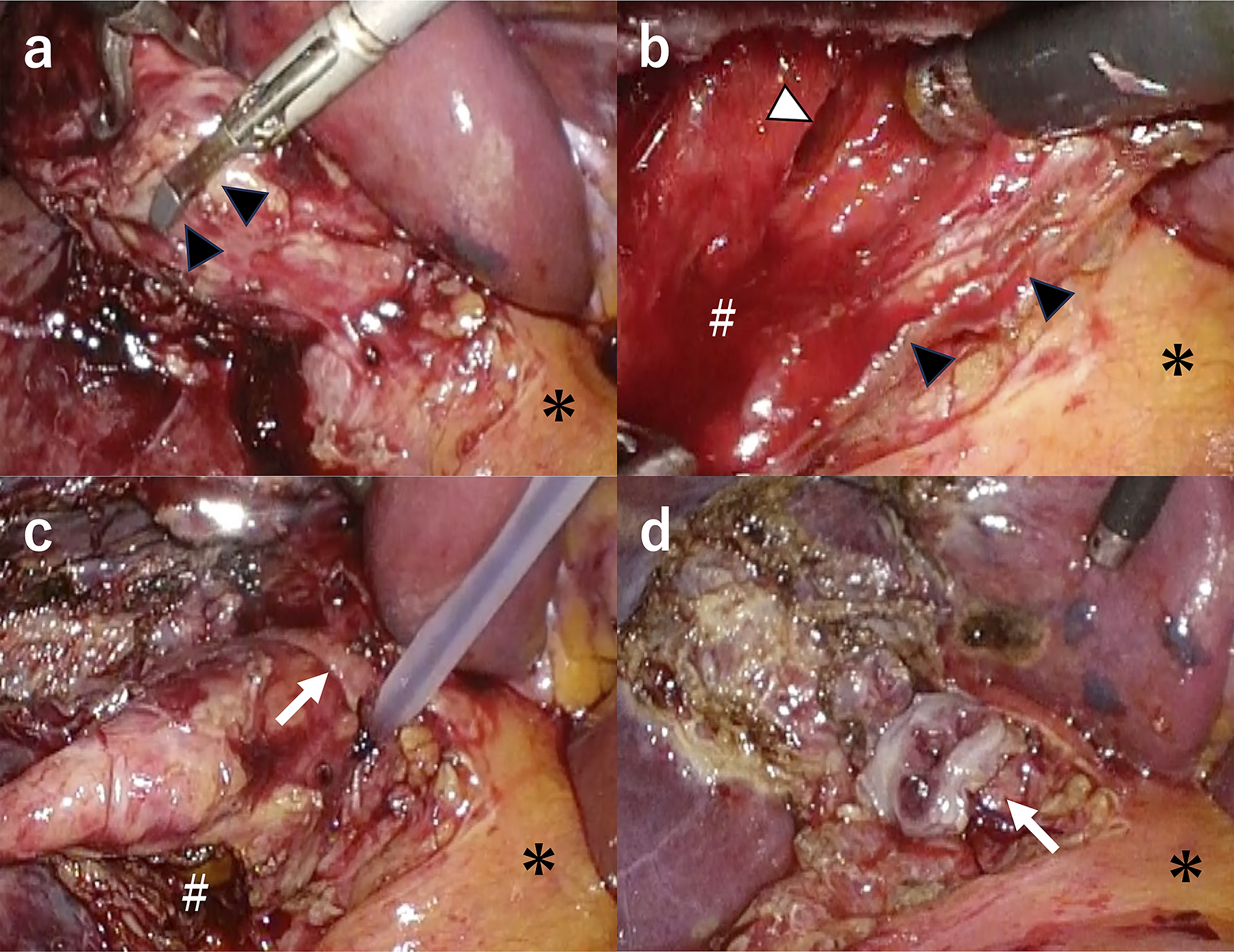
Fenestrating method for subtotal cholecystectomy.
Reconstituting method
In cases where the gallbladder could not be encircled at the posterior aspect of the infundibulum to the neck region or when the posterior aspect of the gallbladder neck could not be dissected even after switching to the fundus-first approach, the gallbladder wall adjacent to the gallbladder bed was left in situ, and reconstitution was performed using running sutures with a 3-0 V-Loc 180 absorbable barbed suture (V20, 15 cm; Medtronic, Minneapolis, MN, USA). When the posterior aspect of the neck could not be dissected, the tissue was insufficient for Endoloop ligation, necessitating suture closure. After transection of the gallbladder, stones were extracted through the gallbladder remnant, and the absence of stones distal to the planned suture site and the location of the cystic duct orifice were confirmed. When one 15-cm V-Loc suture was insufficient, an additional suture was used (Fig. 3).
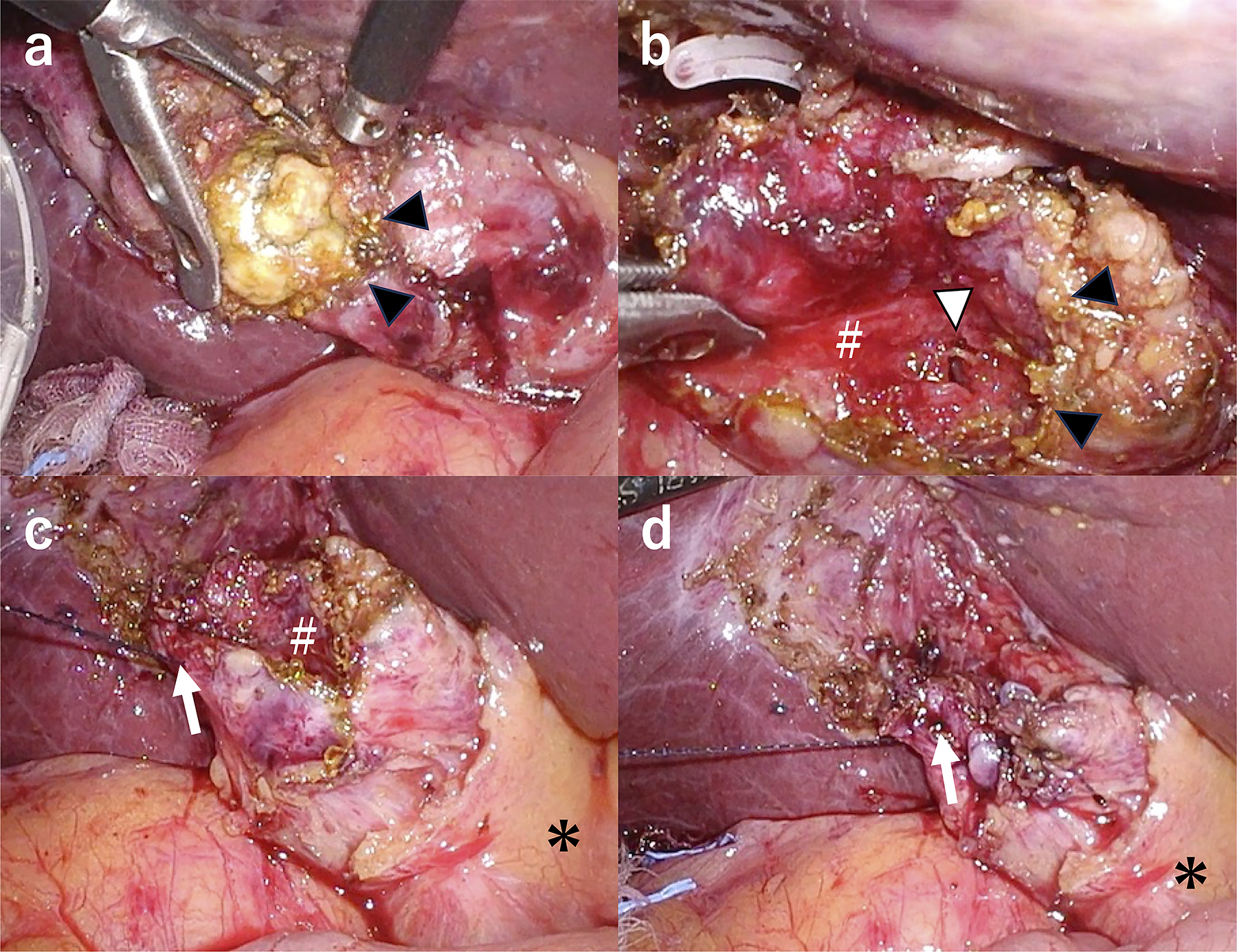
Reconstituting method for subtotal cholecystectomy.
Intraoperative procedures and drainage
Intraoperative cholangiography was not performed routinely. Although it may be performed to confirm the distance from the common bile duct, none of the patients in this study underwent intraoperative cholangiography. For both techniques, a drain was placed at the surgeon’s discretion.
Data collection and outcome measures
The primary outcome was early postoperative complications. Secondary outcomes included late complications (such as remnant cholecystitis and gallstones), operative time, and the presence of remnant gallbladder tissue on postoperative imaging. The gallbladder dissection time was defined as the period from the initiation of dissection of the gallbladder attachment using energy devices to immediately before ligation or suturing. Dissection time included stone removal and hemostatic procedures. The closure time was defined as the period from the initiation of ligation or suturing (when the suture became visible in the operative field) to the cutting of the suture. Dissection and closure times were measured by reviewing recorded videos. Videos were available for 29 of 33 patients (87.9%) in the F-group and 17 of 19 patients (89.5%) in the R-group. Postoperative complications were classified according to the Clavien–Dindo classification. Bile leakage was defined according to the International Study Group of Liver Surgery criteria. 24 The presence or absence of a remnant gallbladder on postoperative follow-up imaging was determined by two radiologists through image interpretation.
Statistical analysis
Continuous variables were compared using the Mann–Whitney U test because of the small sample size and the non-normal distribution. Categorical variables were compared using Fisher’s exact test. Missing data were handled by available case analysis; prothrombin time–international normalized ratio was available for 51 of 52 patients due to one missing value in the fenestrating method group. All statistical analyses were performed using JMP Pro version 17 (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at P < .05.
Ethical considerations
This study was approved by the Ethics Committee of Nihon University School of Medicine (protocol number: RK-211012-5) and was performed according to the principles of the Declaration of Helsinki. Written informed consent was obtained from all patients.
Results
Patient characteristics
During the study period, 420 LCs were performed at our institution. Of these, 360 patients underwent total cholecystectomy (355 laparoscopic and 5 open), and 60 patients (14.3%) underwent SC. Eight patients were excluded from the analysis: Three due to conversion to open SC, three due to staple closure, and two due to the lay-open technique. The remaining 52 patients were divided into two groups: 33 in the F-method group and 19 in the R-method group (Fig. 1).
Patient characteristics are summarized in Table 1. The R-method group was significantly older than the F-method group (median age: 72 versus 62 years, P = .021) and had a significantly higher proportion of patients with Tokyo Guidelines grade II or higher disease severity (79.0% versus 45.5%, P = .023). Other baseline characteristics, including sex, body mass index, comorbidities, and laboratory values, were comparable between the groups. The indications for SC differed between the groups. “Unclear anatomy” was significantly more common in the R-method group (84.2%) than in the F-method group (21.2%, P < .0001). Nearly all patients in both groups had the indication of “inability to encircle the gallbladder” (F-method, 93.9%; R-method, 100%). The proportion of surgeons with ≥10 years of experience was similar between the groups (F-method, 72.7%; R-method, 63.2%).
Patient Characteristics and Operative Outcomes
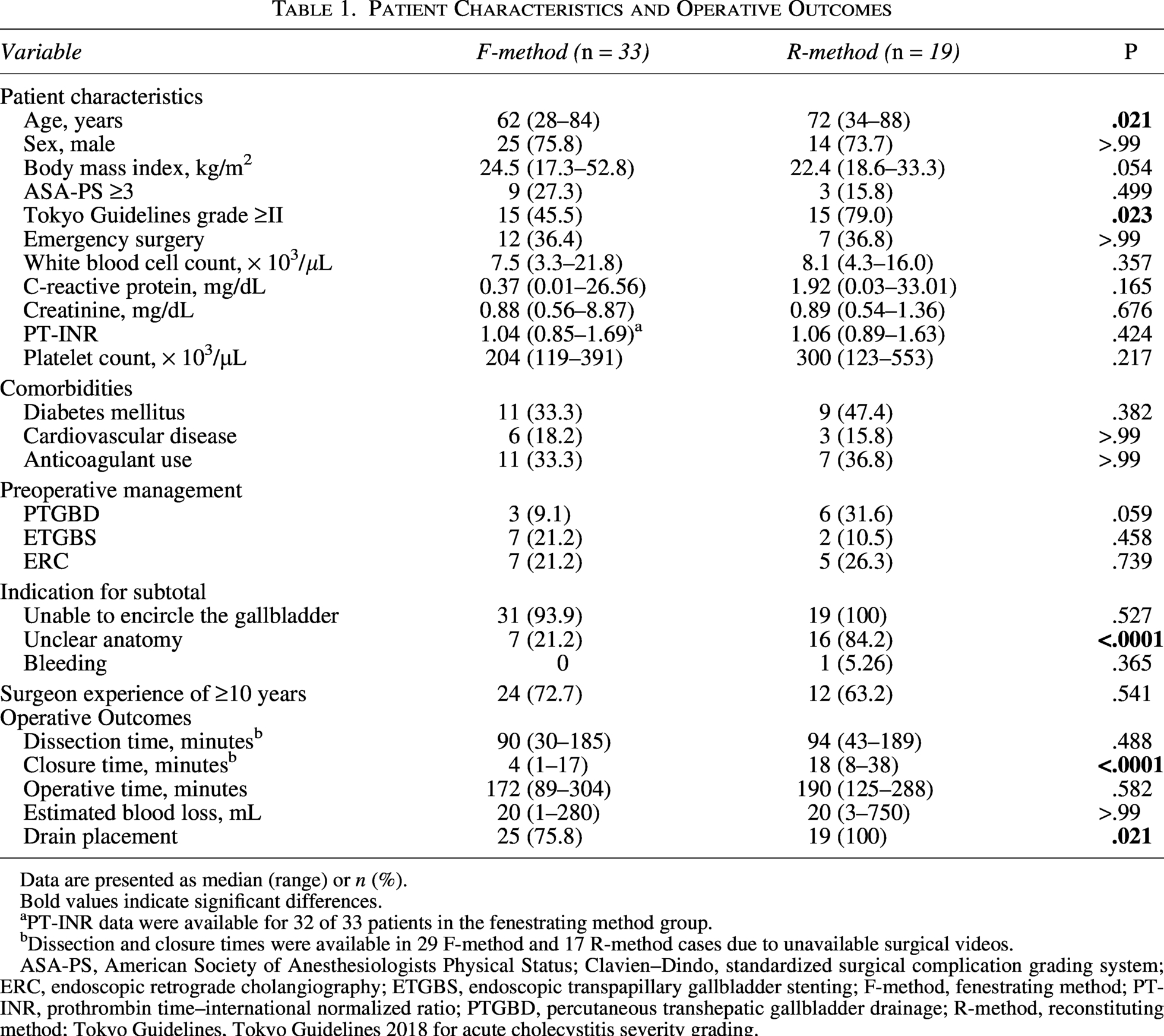
Data are presented as median (range) or n (%).
Bold values indicate significant differences.
PT-INR data were available for 32 of 33 patients in the fenestrating method group.
Dissection and closure times were available in 29 F-method and 17 R-method cases due to unavailable surgical videos.
ASA-PS, American Society of Anesthesiologists Physical Status; Clavien–Dindo, standardized surgical complication grading system; ERC, endoscopic retrograde cholangiography; ETGBS, endoscopic transpapillary gallbladder stenting; F-method, fenestrating method; PT-INR, prothrombin time–international normalized ratio; PTGBD, percutaneous transhepatic gallbladder drainage; R-method, reconstituting method; Tokyo Guidelines, Tokyo Guidelines 2018 for acute cholecystitis severity grading.
Operative outcomes
The operative outcomes are shown in Table 1. The median gallbladder dissection time was comparable between the groups (F-method, 90 minutes [range: 30–185] versus R-method, 94 minutes [range: 43–189], P = .488). However, the median closure time was significantly shorter in the F-method group (4 minutes [range: 1–17] versus 18 minutes [range: 8–38], P < .0001). The median total operative time and estimated blood loss were similar between the groups (Table 1). Drain placement was performed significantly more frequently in the R-method group (100%) than in the F-method group (75.8%, P = .021).
Postoperative outcomes and early complications
The postoperative outcomes are summarized in Table 2. The median postoperative hospital stay was 6 days in both groups. No bile leakage, bile duct injury, postoperative bleeding, or intra-abdominal abscess occurred in either group. Surgical site infection occurred in one patient in the F-method group (3.0%) and one patient in the R-method group (5.3%). No patients in either group experienced complications of Clavien–Dindo grade IIIa or higher within 30 days, and no 30-day mortality occurred in either group.
Postoperative Outcomes and Complications
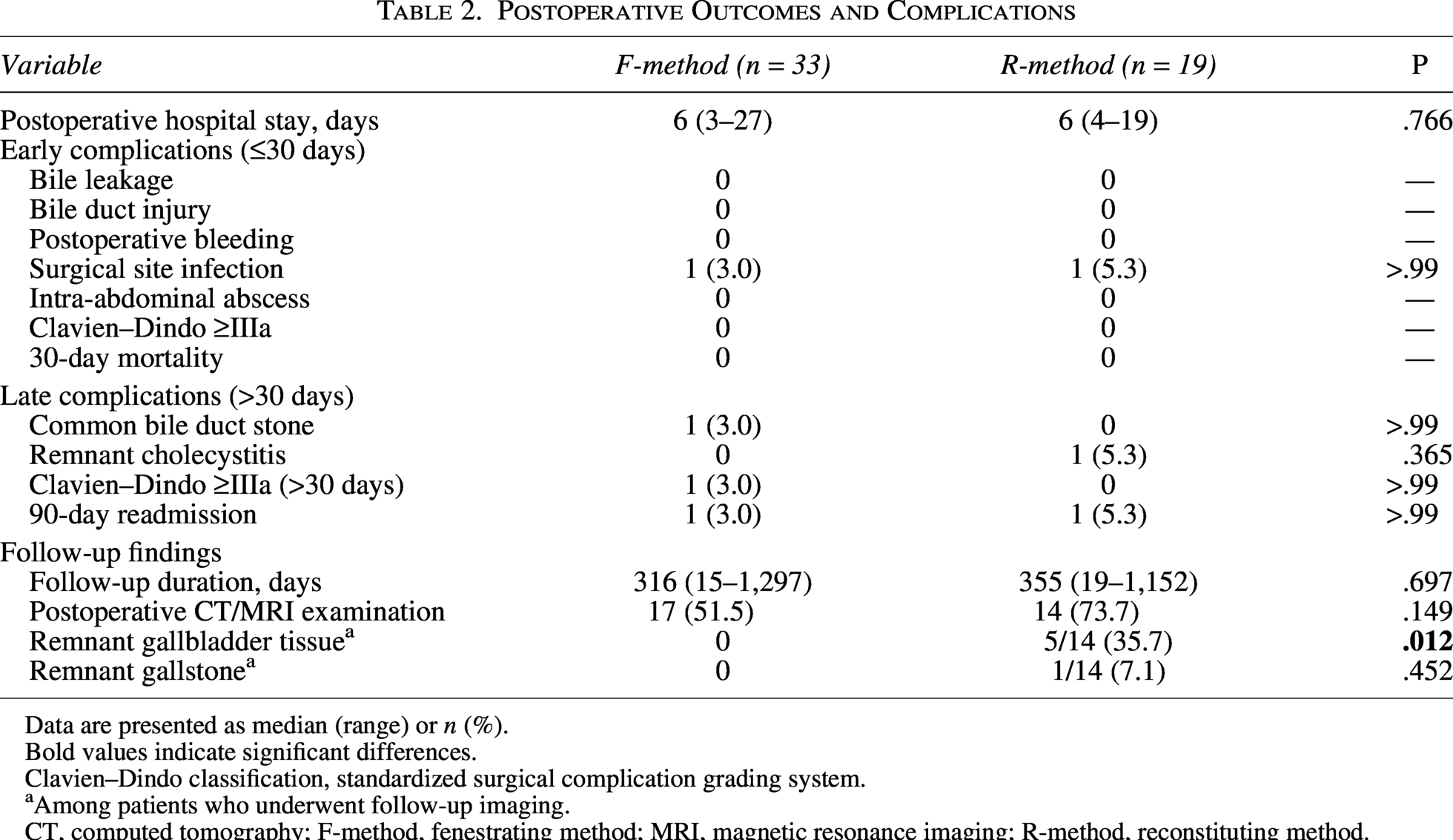
Data are presented as median (range) or n (%).
Bold values indicate significant differences.
Clavien–Dindo classification, standardized surgical complication grading system.
Among patients who underwent follow-up imaging.
CT, computed tomography; F-method, fenestrating method; MRI, magnetic resonance imaging; R-method, reconstituting method.
Late complications and follow-up findings
The late complications are shown in Table 2. One patient in the F-method group developed a common bile duct stone requiring endoscopic retrograde cholangiopancreatography (Clavien–Dindo grade IIIa), resulting in a 90-day readmission. In the R-method group, one patient experienced acalculous remnant cholecystitis leading to a 90-day readmission, which was managed conservatively (Clavien–Dindo grade II). The median follow-up duration was comparable between the groups (F-method, 316 days [range: 15–1297] versus R-method, 355 days [range: 19–1152]). Postoperative imaging evaluation with computed tomography (CT) or magnetic resonance imaging was performed in 17 patients (51.5%) in the F-method group and 14 patients (73.7%) in the R-method group. Among the patients who underwent postoperative imaging, remnant gallbladder tissue was identified in 5 of 14 cases (35.7%) in the R-method group, whereas no remnant tissue was detected in any of the 17 cases in the F-method group (P = .012). Representative imaging findings are shown in Figure 4. Acalculous remnant cholecystitis was observed on CT (Fig. 4a), and subsequent magnetic resonance cholangiopancreatography revealed the remnant gallbladder tissue after conservative treatment (Fig. 4b). In the case of an asymptomatic remnant gallstone, a gallstone was identified within the remnant gallbladder (Fig. 4c). In contrast, the F-method group showed no remnant gallbladder tissue, with only the remnant cystic duct visible (Fig. 4d). Among the R-method patients with identified remnant gallbladder tissue, the longest follow-up duration was 19 months in the case of an asymptomatic remnant gallstone, in which the remnant gallbladder persisted because of the retained stone. The follow-up periods for the other four patients with remnant gallbladder tissue identified on imaging were 460, 150, 132, and 19 days, respectively, although these follow-up periods were short.

Late complications and postoperative imaging findings after subtotal cholecystectomy.
Discussion
This study demonstrated three key findings regarding closure techniques in LSC. First, the two techniques showed distinct late complication profiles. Second, both techniques demonstrated comparable perioperative safety, despite the application of the R-method to more difficult cases. Third, both techniques were feasible and could be performed by surgeons regardless of their experience level.
In this study, the incidence of symptomatic late complications did not differ significantly between the F-method and R-method groups. However, postoperative imaging findings revealed different profiles. No remnant gallbladder tissue was detected in any of the F-method patients (0%) who underwent imaging evaluation. In the R-method group, among those who underwent postoperative imaging, remnant gallbladder tissue was identified in five patients (35.7%) and a remnant gallstone in one patient (7.1%). One patient (5.3%) developed acalculous remnant cholecystitis that resolved with conservative management (Fig. 4a). The F-method allows circumferential mobilization of the gallbladder neck, enabling traction from various directions toward the cystic duct side. Consequently, the gallbladder can be ligated more distally, thereby minimizing remnant gallbladder formation. In contrast, the R-method leaves the posterior gallbladder wall attached to the gallbladder bed, preventing adequate distal dissection with traction. In the R-method, the transected edge is closed with sutures without sufficient mobilization of the gallbladder neck, which tends to create a remnant gallbladder. Additionally, when the distance to the cystic duct is long, there is also a risk of remnant gallstone formation. Therefore, it is necessary to extend the area of SC while avoiding bile duct injury to minimize the remnant gallbladder cavity and prevent overlooking retained stones. However, the actual size of the remnant gallbladder varies among cases, and the gallbladder lumen may be obliterated by barbed suture reconstruction in the R-method. Whether remnant gallbladder function remains after reconstitution is unclear, and its presence in the R-method does not necessarily translate into clinical problems. In this study, remnant cholecystitis occurred in only one case, developing at 4 weeks postoperatively and requiring readmission. However, no recurrence of cholecystitis was observed during the follow-up period. Remnant cholecystitis did not develop in the other cases with longer follow-up periods, suggesting that careful monitoring for early postoperative onset may be warranted. Although no remnant gallbladder cancer was observed in this study, the long-term oncological risk associated with remnant gallbladder tissue cannot be entirely dismissed. 25 Based on these findings, the F-method following circumferential dissection of the gallbladder neck with Endoloop ligation is recommended for LSC because it prevents remnant gallbladder formation, whereas the R-method with barbed sutures represents a rational alternative when dissection from the liver parenchyma poses a significant risk of injury.
Both techniques demonstrated comparable perioperative safety within acceptable ranges. Importantly, no vasculobiliary injuries occurred in either group, underscoring the importance of selecting LSC in difficult cases to avoid major complications, consistent with the findings of previous studies.5–7 While previous studies have reported bile leakage rates of 10%–35% in SC,8–16 we observed no bile leakage in either group. The choice between the F-method and R-method is determined by two intraoperative factors: First, whether the gallbladder can be circumferentially mobilized at the dorsal aspect of the body-to-neck region; and second, if circumferential mobilization is achieved, at what level of the gallbladder neck-to-cystic duct the closure can be performed. When the diameter at the planned closure site exceeds 11 mm (the maximum closure diameter of the Hem-o-lok ML clip), complete gallbladder mobilization is performed, and the F-method with Endoloop ligation is selected. If circumferential mobilization is not feasible, the approach is switched to the fundus-first technique. If the fundus-first approach allows complete dissection of the gallbladder from the gallbladder bed, total cholecystectomy can be achieved. If dissection reaches the neck level, the F-method with an Endoloop becomes possible. When neck dissection cannot be performed, the R-method with barbed sutures is selected. Of these two methods, the F-method with an Endoloop should be attempted first, whereas the R-method is indicated for cases in which dissection is difficult. Our results confirmed that the R-method group included cases with higher surgical difficulty, as evidenced by the significantly higher proportion of patients with unclear anatomy (84.2% versus 21.2%, P < .0001). These techniques should be viewed as complementary rather than competing options, with selection based on intraoperative findings. This algorithm provides objective criteria for technique selection.
Similar to our study, only one report by Loh et al. classified Endoloop-based gallbladder closure in LSC as fenestrating. 18 Loh et al. classified Endoloop ligation as fenestrating because “it does not create a functional remnant gallbladder,” and we followed this classification. In addition, three other reports have described external gallbladder closure using an Endoloop in LSC, indicating that this technique has been widely adopted.17,19,20 Strasberg et al. recommended intraluminal closure of the cystic duct and considered external ligation of the cystic duct undesirable because it “could potentially cause common bile duct injury.” 11 However, in previous studies and in our study, when an Endoloop is used for gallbladder closure, the gallbladder is mobilized from the gallbladder bed to the ligation site. In previous reports and in our series using external Endoloop ligation, no bile duct strictures or injuries occurred.17–20 External ligation is safe when the gallbladder is adequately mobilized and a sufficient distance from the common bile duct is maintained. Furthermore, external ligation provides more reliable closure than intraluminal suture closure of the cystic duct. Regarding the R-method, gallbladder closure using barbed sutures represents a newer technique. To date, only case reports have been published without substantial case series.21,22 In this study, we performed barbed suture–based gallbladder closure in 19 cases and demonstrated its short- and long-term safety.
Both techniques represent standard laparoscopic surgical techniques and were performed by 15 surgeons with different levels of experience. However, our operative times were longer than those reported in previous studies (F-method, 172 minutes; R-method, 190 minutes).17,18,20 Closure time was significantly shorter in the F-method (4 versus 18 minutes, P < .0001), whereas dissection time was not significantly different (90 versus 94 minutes, P = .488), indicating that substantial time was spent dissecting the gallbladder body-to-neck region to determine which closure method to select. Notably, no postoperative bile leakage was observed, suggesting that this additional dissection time may contribute to reducing complications.
This study has several limitations. First, this was a single-center, retrospective study, though prospective randomization was not feasible given that technique selection depended on intraoperative anatomical findings. Second, the sample size was small, particularly in the R-method group (n = 19), which may have limited our ability to detect differences in rare complications. Third, the follow-up period was relatively short (median: 10–11 months), which may be insufficient to evaluate long-term complications. Additionally, postoperative imaging was not performed routinely, and the imaging evaluation rate differed between the groups (F-method, 51.5%; R-method, 73.7%), which may have introduced selection bias in detecting remnant gallbladder tissue.
In conclusion, both fenestrating and reconstituting methods are safe and feasible for LSC with distinct complication profiles. The reconstituting method using barbed sutures provides a reliable option when complete gallbladder wall dissection carries a risk of injury. Understanding these complication profiles enables appropriate surgical decision-making.
Ethics Statement
This study was approved by the Ethics Committee of Nihon University School of Medicine (protocol number: RK-211012-5) and was performed according to the principles of the Declaration of Helsinki.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The authors would like to thank Editage (![]() ) for English language editing. The authors used Claude Sonnet 4.6 (Anthropic, San Francisco, CA, USA) to improve the language and readability of this article. All content was originally drafted by the authors, and the artificial intelligence tool was used for grammatical and stylistic refinement. The authors reviewed and take full responsibility for the final content.
) for English language editing. The authors used Claude Sonnet 4.6 (Anthropic, San Francisco, CA, USA) to improve the language and readability of this article. All content was originally drafted by the authors, and the artificial intelligence tool was used for grammatical and stylistic refinement. The authors reviewed and take full responsibility for the final content.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received for this article.