
Abstract
Aim:
Incisional hernias (IHs) are a significant source of postoperative morbidity following liver transplants (LTs). Our aim is to perform a comprehensive systematic review and proportional meta-analysis to evaluate the pooled incidence of and risk factors associated with the development of IH following LT.
Methods:
A comprehensive search was conducted using PubMed, Cochrane, Embase, and Web of Science databases. All studies reporting the incidence of IHs following liver LT in adult patients were included. Data were extracted on IH incidence, age, gender, diabetes mellitus diagnosis, body mass index (BMI), Model for End-Stage Liver Disease (MELD) score, presence of ascites, and wound complications in both IH and non-IH cohorts. Statistical analysis was performed using RStudio.
Results:
From 2078 records, 28 studies were included, encompassing 12,354 patients, with 1709 IH reported. Proportional meta-analysis estimated an overall IH incidence of 14.5% (95% confidence interval [CI]: 10.88 to 19.08, I2 = 97%, P < .01) following LT. Risk factor analysis identified male sex (RR: 1.16; 95% CI: 1.08 to 1.24; P < .0001), wound complications (RR: 2.6; 95% CI: 1.35 to 5.07; P = .004), older age (RR: 2.00; 95% CI: 1.20 to 2.85; P < .0001), and high BMI (RR: 0.86; 95% CI: 0.39 to 1.33; P < .0001) as significant predictors of IH development. However, MELD scores, presence of ascites, and diabetes were not significantly associated with IH risk.
Conclusion:
LTs have a pooled IH incidence of 14%. Male sex, high BMI, older age, and post-transplant wound complications are associated with an increased risk of IH development.
Introduction
Liver transplantation has evolved into a standardized procedure with excellent long-term survival, but postoperative complications remain a significant challenge. Incisional hernia (IH) is one of the most frequent late morbidities, with reported incidence ranging from 4% to 46% depending on the cohort and methodology.1–4 Although not usually life-threatening, IH negatively affects quality of life, limits physical function, and in some cases leads to serious complications such as incarceration or strangulation.4,5 With improved survival after LT, the clinical relevance of this complication has increased substantially. 6
The development of IH after LT is multifactorial, involving both patient- and surgery-related determinants. Obesity, older age, smoking, diabetes, and malnutrition have been consistently described as patient-related risk factors.2,3,7 Technical aspects such as incision type, increased wound tension, postoperative wound complications, and repeated abdominal surgeries also play a significant role.1,6,7 Immunosuppressive therapy represents a unique factor in transplant recipients, with agents like sirolimus, everolimus, and mycophenolate mofetil associated with impaired wound healing and higher IH risk.3,4 Nonetheless, reported risk factors vary across studies: Hepatocellular carcinoma as an LT indication, small graft weight, prolonged ischemia time, bile leak, and surgical site infection have all been described as predictors, 5 whereas variables such as MELD score or ascites remain controversial. 3
Despite heterogeneity in incidence and risk factors, there is agreement that IH is a prevalent and clinically relevant complication after LT, contributing to morbidity and increased healthcare burden. Efforts to mitigate this problem have focused on optimizing modifiable risks, refining surgical closure techniques, and tailoring immunosuppressive regimens.2,4,6 Against this background, we conducted a systematic review and meta-analysis to provide a comprehensive assessment of the pooled incidence of IH following LT and to identify the main clinical and surgical risk factors associated with its development.
Methods
Material and methods
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 statement. 8 The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD420261324227). The review aimed to evaluate the incidence of IH and to identify perioperative risk factors associated with its development in adult liver transplant recipients.
Eligibility criteria
The Population, Intervention, Comparison, Outcome, Study design, Type of Study model (PICOST) 9 was followed in this systematic review, which considered studies that fulfilled all the following eligibility criteria: (1) adult patients (≥18 years) undergoing liver transplantation, (2) development of IH following liver transplantation, (3) liver transplant recipients without IH, and (4) incidence of IH and/or perioperative risk factors associated with IH development.
Studies were excluded if they addressed (1) studies without comparative data between patients who developed IH and those who did not following liver transplantation; (2) studies including patients who underwent abdominal surgeries other than liver transplantation; (3) systematic reviews, narrative reviews, case reports, and editorials; (4) conference abstracts without full-text availability; and (5) studies with overlapping patient populations, including studies recruiting from the same institution during overlapping study periods.
Search strategy and data extraction
A comprehensive and systematic literature search was performed in the following electronic databases: PubMed (MEDLINE), Embase, Cochrane Library, and Web of Science, from database inception to September 6, 2024. The search strategy was developed to identify studies reporting IH following liver transplantation and combined controlled vocabulary and free-text terms related to hernia and liver transplantation. The search strategy used was “hernia” AND (“liver transplant” OR “liver transplantation”). The number of records retrieved from each database was as follows: PubMed (n = 408), Embase (n = 1269), Cochrane Library (n = 33), and Web of Science (n = 368). All retrieved records were exported to a reference management software, and duplicate studies were removed prior to screening.
All records identified through the database search were independently screened based on titles and abstracts to assess potential eligibility. Full-text articles of potentially relevant studies were retrieved and assessed for inclusion according to the predefined eligibility criteria. Only studies meeting all inclusion criteria were included in the qualitative synthesis and, when appropriate, in the quantitative meta-analysis.
Data extraction was performed using a standardized data collection form. Extracted data included study characteristics and patient-level variables. The following data items were collected from each included study:
(1) incidence of IH following liver transplantation, (2) patient age and sex, (3) presence of diabetes mellitus, (4) body mass index (BMI), (5) Model for End-Stage Liver Disease (MELD) score, (6) presence of ascites, and (7) postoperative wound complications.
Data were extracted separately for patients who developed IH and for those who did not. Quantitative synthesis was performed when sufficient data were available.
Quality assessment
We assessed the risk of bias in nonrandomized studies using the Cochrane Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) 10 tool, rating each study as having low, moderate, serious, or critical risk of bias in seven domains: confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, outcome measurement, and selection of the reported result. Each trial was classified as having low risk, some concerns, or high risk of bias. Two independent reviewers (J.A.R.C.D.S. and D.P.A.D.A.) conducted the evaluations following the recommendations from the Cochrane Handbook for Systematic Reviews of Interventions, 11 and disagreements were resolved by consensus with a third reviewer (V.N.).
Statistical analysis
Statistical analyses were conducted using RStudio. Pooled analyses were used to assess the association between perioperative risk factors and the development of IH following liver transplantation. Effect estimates for binary outcomes were expressed as risk ratios (RR) with corresponding 95% confidence intervals (CIs), while continuous variables were analyzed using mean differences (MDs) with 95% CIs. A two-sided P value of <.05 was considered statistically significant.
Results
Incidence of IH after liver transplantation
A total of 56 studies were selected for final assessment after an initial screening of 817 records. Following the eligibility criteria, a total of 28 studies were included in the quantitative synthesis (Fig. 1). Across these studies, the reported incidence of IH following liver transplantation varied substantially, ranging from 4% to 46%.1–4 This wide variation reflects differences in study design, duration of follow-up, diagnostic criteria, and patient- and procedure-related characteristics across cohorts (Table 1).
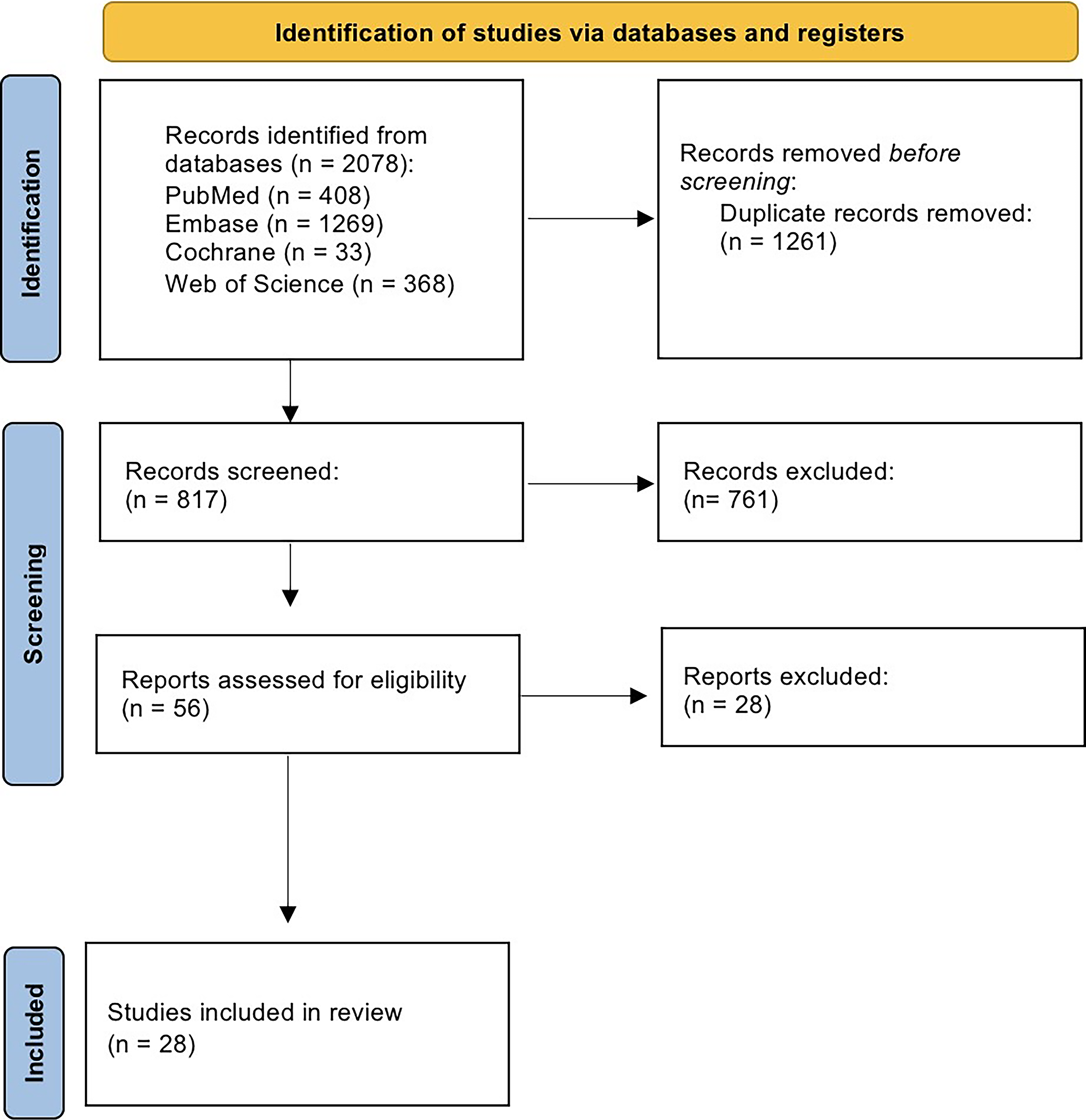
PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The pooled analysis of proportions demonstrated an overall IH incidence of 14.5% (95% CI: 10.8 to 19.1; Fig. 2), indicating that approximately one in seven patients develops this complication after liver transplantation.
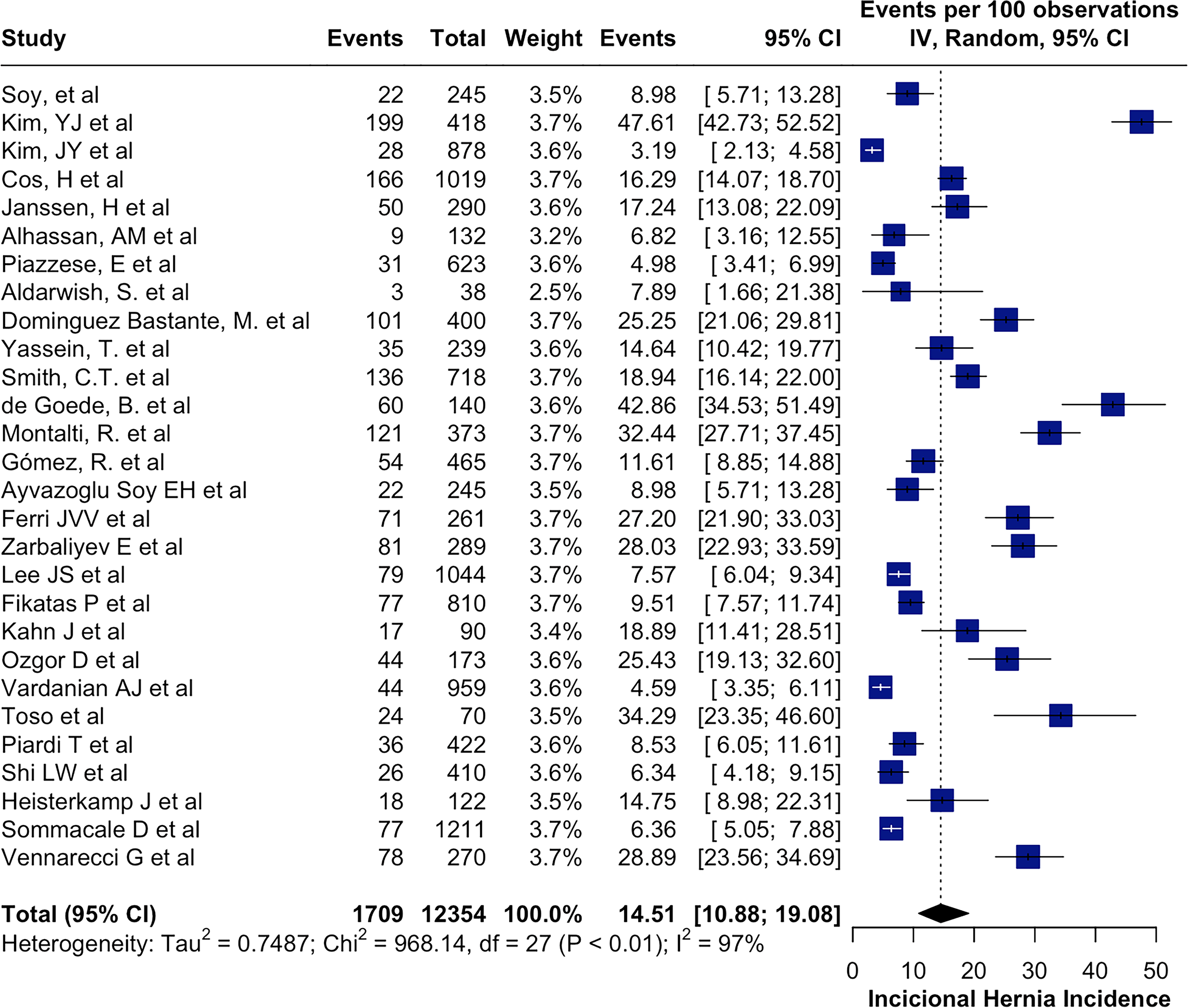
Pooled incisional hernia incidence.
A high degree of statistical heterogeneity was observed (I2 = 97%), suggesting considerable variability among the included studies. Such heterogeneity likely reflects differences in surgical techniques (including incision type and closure methods), perioperative management, and postoperative surveillance strategies, as well as variability in follow-up duration and definitions of IH across transplant centers.
Quality assessment
Figure 3 summarizes the individual assessment of each study included in the review using the ROBINS-I risk of bias tool. Overall, the analysis revealed a moderate risk of bias in most included studies, with a serious overall risk of bias identified in only two of the 23 studies. In these two studies, risk of bias due to confounding was the domain of concern in both. Among studies with a moderate overall risk of bias, the main issues were related to confounding, missing data, and selection of participants, while domains involving classification of interventions and deviations from intended interventions were generally considered low risk. These findings highlight the methodological limitations commonly encountered in observational studies.
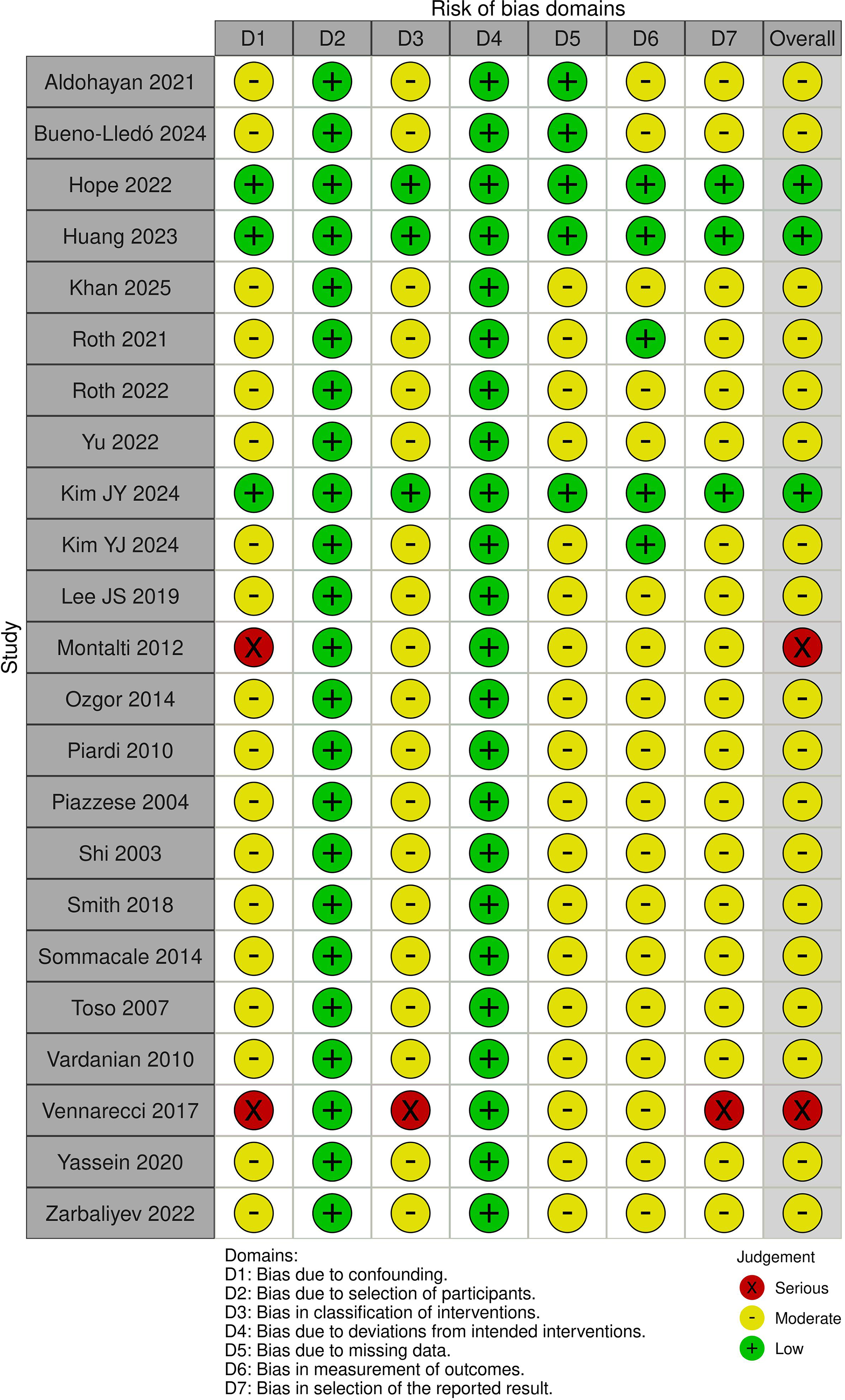
Risk of bias domains—ROBINS-I. ROBINS-I, Risk of Bias in Non-Randomized Studies of Interventions.
Demographic risk factors
Sex distribution
Fifteen studies contributed data to the meta-analysis evaluating sex as a risk factor for IH development. Across most cohorts, IH occurred more frequently in male recipients. The pooled random-effects analysis demonstrated that male sex was associated with a statistically significant increased risk of IH (RR: 1.16, 95% CI: 1.08 to 1.24), with substantial heterogeneity (I2 = 64%) (Fig. 4).
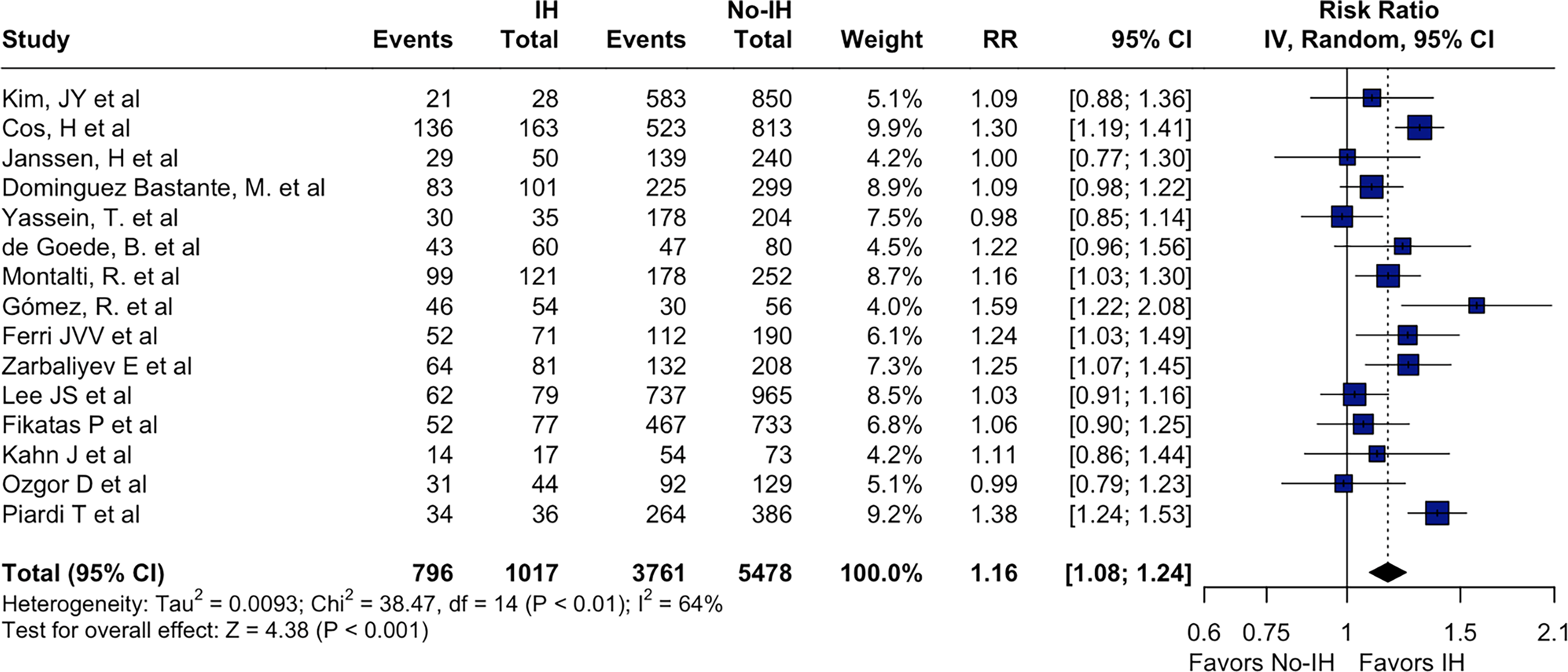
Incidence of incisional hernia in male patients.
Sensitivity analysis confirmed the stability of this association, as sequential omission of individual studies did not materially alter the pooled estimate.
Age
Age was reported as a continuous variable in 12 studies, allowing direct comparison between patients with and without IH. Patients who developed IH were consistently older across cohorts. The pooled analysis showed a mean age difference of 2.03 years (95% CI: 1.20 to 2.85), favoring higher age in the IH group, with moderate heterogeneity (I2 = 42%; Fig. 5). Leave-one-out sensitivity analysis demonstrated that this association remained robust across all iterations.
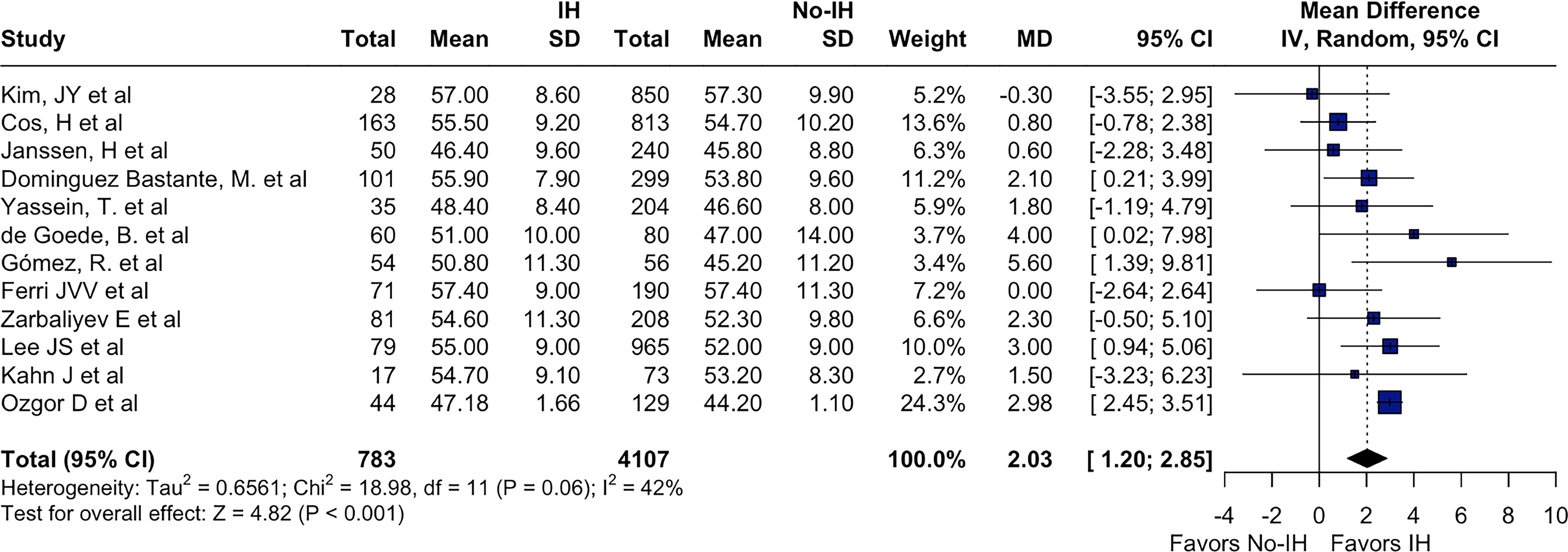
Incidence of incisional hernia in elderly patients.
Metabolic and comorbidity-related risk factors
Body mass index
Nine studies reported BMI as a continuous variable. Patients who developed IH exhibited higher BMI values compared with those without IH across most cohorts. The pooled random-effects analysis demonstrated an MD of 0.86 kg/m2 (95% CI: 0.39 to 1.33), with moderate heterogeneity (I2 = 47%). Sensitivity analysis showed consistent results after sequential exclusion of individual studies (Fig. 6).
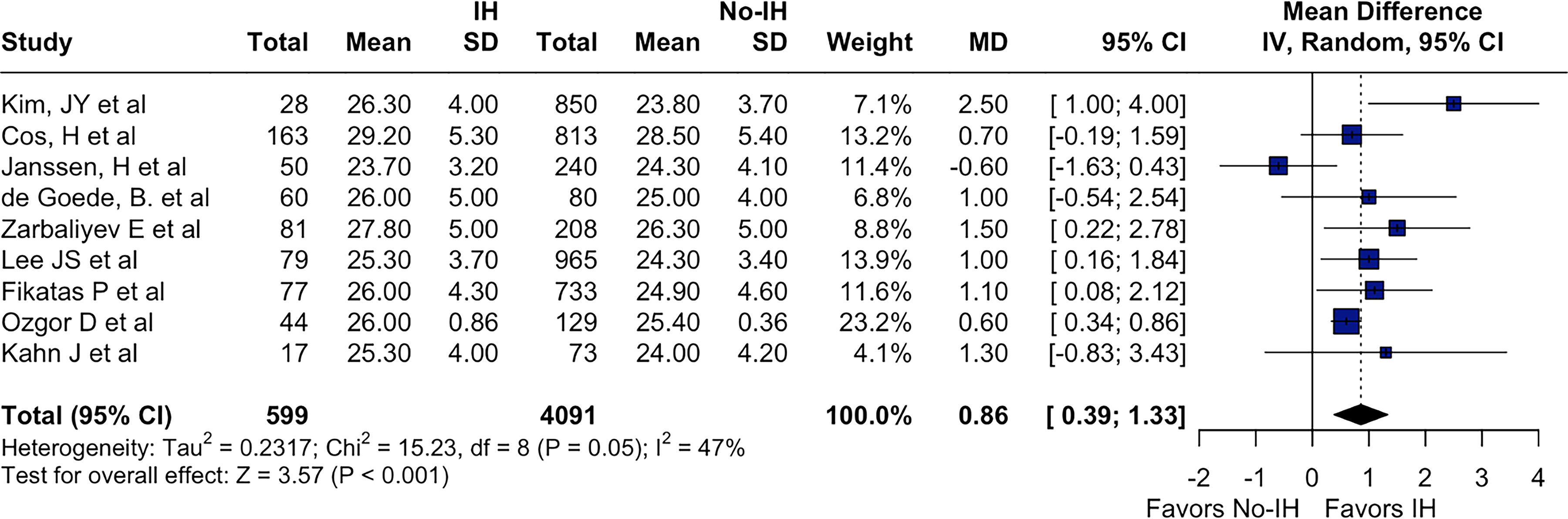
Incidence of incisional hernia related to high BMI. BMI, body mass index.
Diabetes mellitus
Eleven studies evaluated diabetes mellitus as a binary risk factor for IH development. Diabetes was more prevalent among patients who developed IH. The pooled random-effects analysis demonstrated a statistically significant association between diabetes mellitus and IH (RR: 1.22, 95% CI: 1.01 to 1.49), with moderate heterogeneity (I2 = 57%). This association remained stable in leave-one-out sensitivity analyses (Fig. 7).
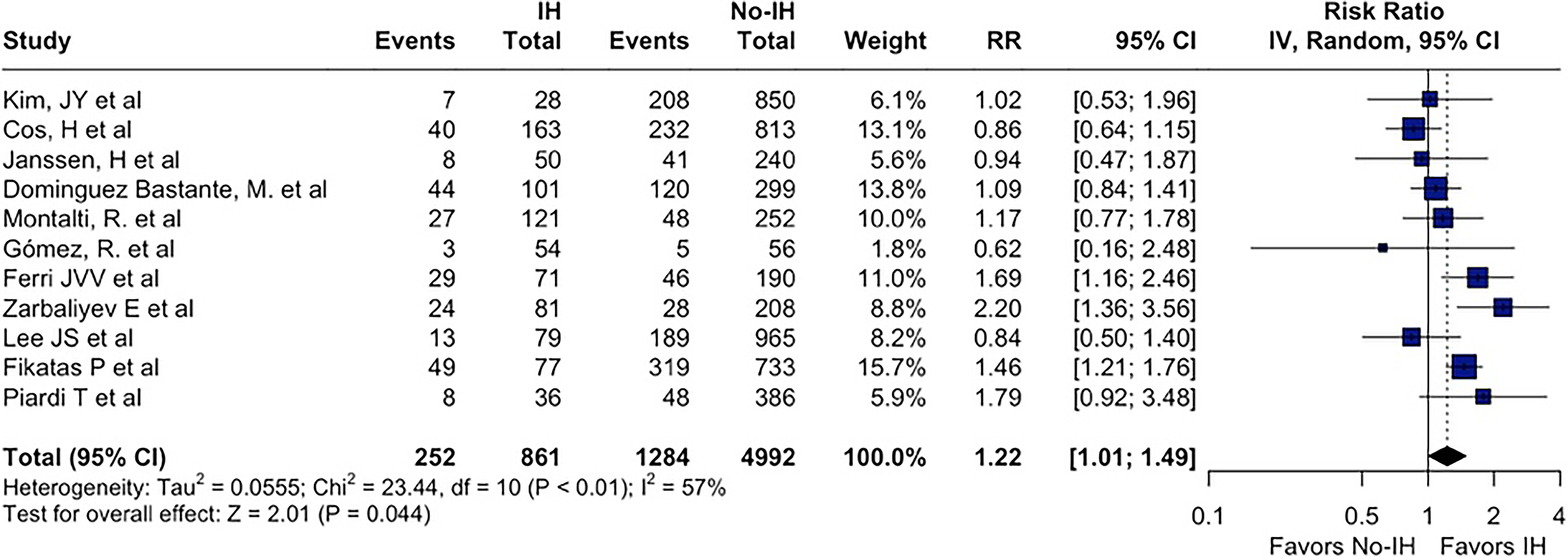
Incidence of incisional hernia in patients with diabetes mellitus.
Liver disease severity and ascites
MELD score
Ten studies reported MELD score as a continuous variable at the time of transplantation. No significant difference in MELD score was observed between patients who developed IH and those who did not. The pooled random-effects analysis demonstrated an MD of −0.15 (95% CI: −0.75 to 0.45), with low heterogeneity (I2 = 22%). Sensitivity analyses confirmed the consistency of this finding.
Ascites
Eight studies assessed the relationship between ascites and IH development. While individual studies reported variable associations, the pooled random-effects analysis did not demonstrate a statistically significant association (RR: 1.11, 95% CI: 0.86 to 1.43), with very high heterogeneity (I2 = 89%). Leave-one-out sensitivity analysis showed that no single study disproportionately influenced the pooled estimate.
Wound complication
Five studies evaluated postoperative wound complications as predictors of subsequent IH formation. Across all contributing cohorts, wound complications, including surgical site infection, wound dehiscence, or delayed healing, were more frequent among patients who developed IH. The pooled random-effects analysis demonstrated a markedly increased risk of IH associated with wound complications (RR: 2.62, 95% CI: 1.35 to 5.07), with moderate-to-high heterogeneity (I2 = 70%) (Fig. 8). Sensitivity analysis confirmed the robustness of this association.
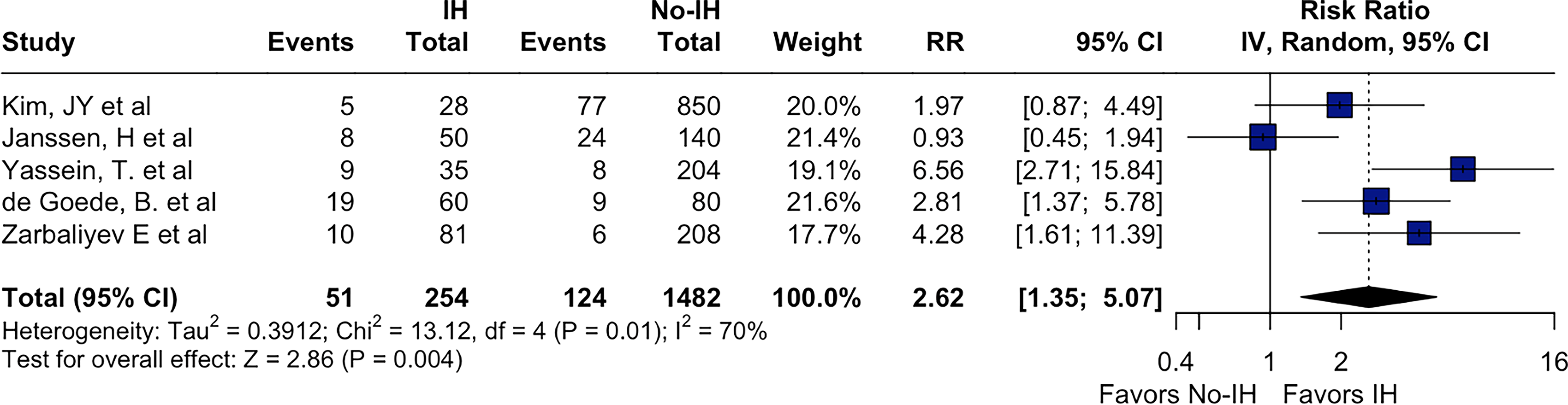
Incidence of incisional hernia in patients with wound complications.
Sensitivity analyses
Leave-one-out sensitivity analyses were conducted for all primary outcomes and risk factor analyses. Across all models, sequential exclusion of individual studies did not materially change pooled effect estimates or their direction, supporting the robustness of the findings despite heterogeneity observed in several analyses.
Discussion
In this systematic review and meta-analysis, a higher risk of IH development was observed in male patients, individuals with elevated BMI, elderly patients, and those who experienced postoperative wound complications. The first noteworthy finding in our results is that these factors are not specific to the post–liver transplantation population. Rather, they represent well-established risk factors for IH development in the general surgical population.
With regard to BMI, we observed that very high levels are not required to increase the risk of developing an IH. Patients outside the ideal weight range already present a higher risk of IH after liver transplantation. Kim et al., 23 Fikatas et al., 18 Lee et al., 24 Smith et al., 7 Piazzese et al., 1 and Piardi et al. 25 have demonstrated that BMI values greater than 25 kg/m2 are sufficient to increase this risk. In contrast, other authors such as Soy et al., 2 Kim et al., 3 Dominguez et al., 4 and Ayvazoglu et al. 27 have reported that a BMI threshold of 30 kg/m2 is required to significantly increase the risk. Although the development of IH is known to be multifactorial, our results reinforce the importance of normal weight maintenance after transplantation.
Regarding age, De Goede et al. 20 showed that patients older than 49 years already have a higher propensity for developing IH. Gomez et al. 22 identified age ≥50 years as a risk factor. In contrast, Fikatas et al. 18 and Lee et al. 24 suggest that the risk becomes more significant in patients older than 54 years.
When discussing complications related to the surgical wound, there is a higher propensity for the development of IH in these patients.1,2,5,7,15,20,23,27 Surgical site infection was the complication most frequently cited in these studies as a risk factor for increased incidence of IH following liver transplantation. These findings are consistent with those observed in other populations and are not specific to transplant patients.
Although we were unable to identify studies suitable for a meta-analysis, it is worthwhile to include in the discussion an appraisal of the type of incision performed that may contribute to the development of IHs. Some studies have attempted to establish a direct association between the type of incision and the occurrence of IH. In liver transplantation, several incision options are available, each with inherent advantages and disadvantages. Zarbaliyev et al. compared three types of incisions and reported a lower incidence of IH with the use of the J-shaped incision. 12 Heisterkamp et al. compared the J-shaped and Mercedes incisions and similarly demonstrated a reduction in IH incidence with the J-shaped approach. 13 However, this association was not confirmed in the studies by Alhassan et al. 14 and Shi et al., who did not observe a statistically significant relationship between incision type and hernia development. 15
Another important consideration in this population is the impact of immunosuppressive therapy. Toso et al. described a one-third increase in the incidence of IH among patients receiving Sirolimus. 16 Similar findings were reported by Kahn et al., who, in addition to sirolimus, observed a higher incidence of IH in patients treated with mycophenolate, 17 as also described by Fikatas et al. 18 Montalti R et al. reported the occurrence of IH in approximately half of the patients treated with mammalian target of rapamycin inhibitors, 19 a finding also described by Kim et al. 3 However, we were not able to evaluate the impact of immunosuppressive medications as risk factors for the development of IH in our meta-analysis.
Baseline Characteristics of Included Studies
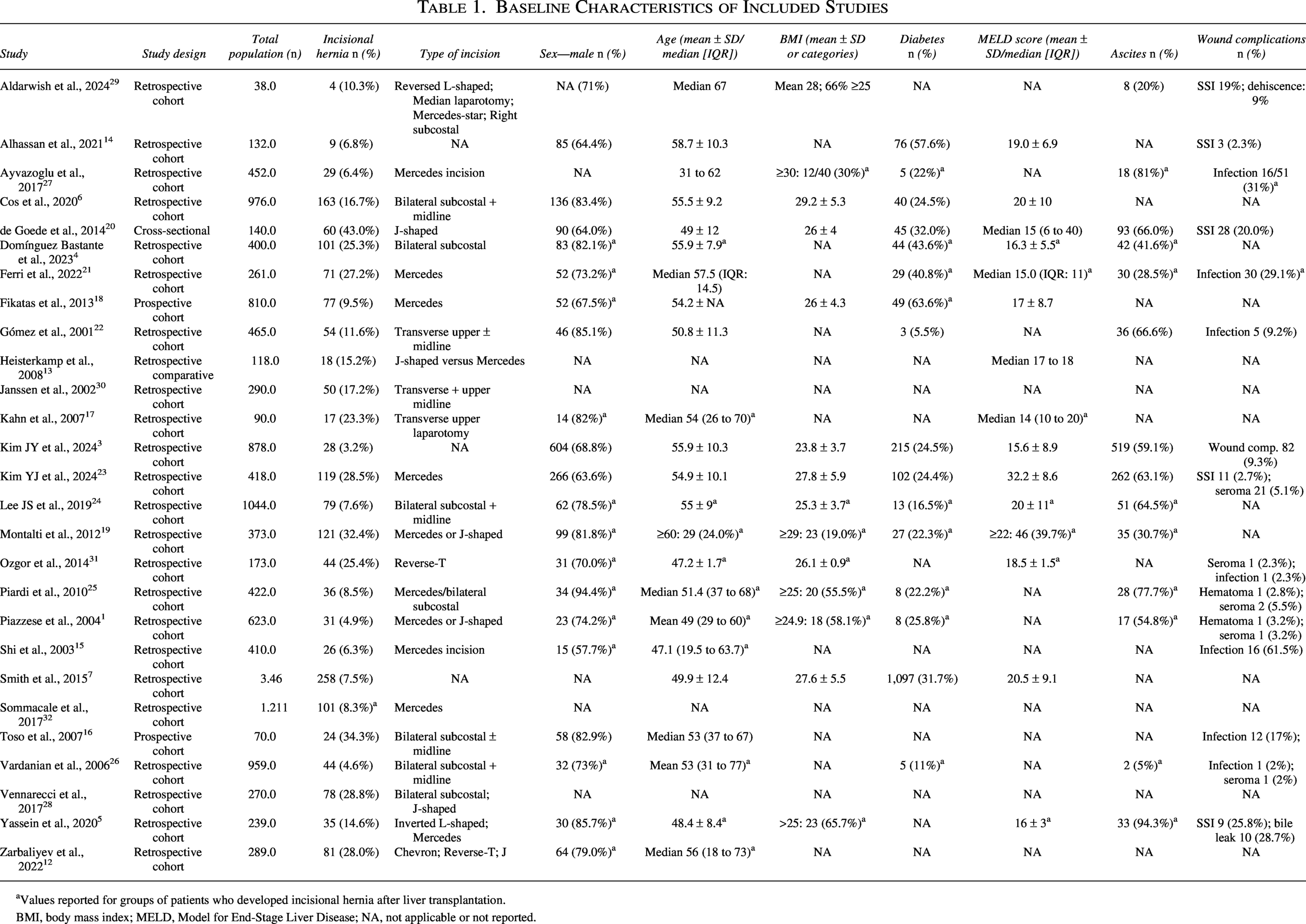
Values reported for groups of patients who developed incisional hernia after liver transplantation.
BMI, body mass index; MELD, Model for End-Stage Liver Disease; NA, not applicable or not reported.
This study has several limitations. First, the predominantly retrospective design of most available studies and the lack of more granular data regarding immunosuppressive regimens these patients were on. Second, studies reported different LT incision types and follow-up varied across studies. The increased risk may stem from patient-related characteristics, surgical technique, postoperative complications, and the specific immunosuppressive protocols employed. Greater access to patient data and follow-up could provide the opportunity for additional subanalyses that may influence outcomes.
Conclusion
Liver transplants have a pooled IH incidence of 14%. Male sex, high BMI, older age, and post-transplant wound complications are associated with an increased risk of IH development.
Authors’ Contributions
All authors have contributed equally for the project development and manuscript writing.
Ethical Approval
The prospective systematic review protocol was registered in the PROSPERO with an ID number CRD420261324227 on February 23, 2026.
Informed Consent
Not applicable.
Author Disclosure Statement
No competing financial interests exist.
Footnotes
Funding Information
This study did not receive any funding from any agencies in the public, commercial, or not-for-profit areas.