
Abstract
Background
Epstein-Barr virus (EBV) has recently been implicated in the development of various astrocytic proliferations.
Objective
to assess the prevalence of neurotropic EBV infection in brain tissue samples from astrocytoma patients classified into grades I, II, III, and IV, using a prospective case-control approach.
Methods
In this study, 100 brain tissue specimens were obtained from 75 patients who had astrocytoma grades1, 2, 3 and 4. In contrast, the rest of the brain tissues were enrolled as a control group. The technique of polymerase chain reaction was utilized to amplify and detect the neurotropic DNA sequence of EBV in the examined brain tissues.
Results
The most infected brain tumor tissues with DNA-EBV are related to the age (41–60 years), which accounted for 10.6%. The overall percentage of positive-PCR detection results for neurotropic EBV genomic DNA sequence in the examined brain tissues from astrocytomas grade 1–4 tissues was 28% (21 out of 75). The difference between the percentage of positivity of PCR detection results of neurotropic EBV genomic DNA sequence in the astrocytoma group and control group was statistically significant (P = 0.04).
Conclusion and cancer policy
the present results are shedding light on the importance of the studied neurotropic EBV infection in the tumorigenesis and carcinogenesis processes of the astrocytoma cases, possibly either as initiators in the induction of these brain tumors.
Keywords
Introduction
The two most frequent types of brain tumors are glioma and meningioma, which constitute 2% of all tumors in the body and need further research to elucidate the still unknown reasons behind them.1–3 Malignant brain tumors commonly occur as gliomas and make up roughly 60% of all primary CNS malignancies. They originated from the glial cells and since derived from the astrocytes, have been classified as astrocytomas.4–6 These gliomas have been classified by WHO into 4 grades (I-IV). Grade IV is recognized as IV (GBM), accounting for 50–60% of them and comprising the most frequent aggressive glial malignancies affecting adults and having the worst prognosis. 7 Although the cause of these cancers is still unclear, researchers have been involved in the GBM etiology of the affected patients both their genetic predisposition as well as their exposure to some agents, such as chemicals or ionizing radiation. 8 More recently, the associations between some infectious agents and gliomas have been considered. Among them, the associations of gliomas have been detected with several viral infections, such as HPV 16 and 18, EBV, human CMV, Kaposi sarcoma-associated herpes virus, HBV, HCV, HTLV1, JCV, BK virus, and SV40, which might involve an oncomodulation in these gliomas, were reported.9,10 However, the correlation of such viral infections with the tumorigenesis of these primary brains have raised an extensive controversies. 10 Epstein–Barr virus, a herpetic virus named as human herpes virus 4, belongs to Herpes Viridae, where globally its infection affects more than 90% of the population. The viral infection occurs in early childhood, establishing a lifelong asymptomatic latent infection in the principal targets that express CR2 as EBV major cellular receptor, switching into EBV - latent phase where most viral genes are turned off.11,12 EBV may remain invisible to the immune mechanisms by persisting in the epithelial and some T as well as Natural Killer cells, wherein these cells express one of three potential latency programs, Latency I, II, or III. 13 The CR2 receptor of EBV appears to be expressed on the astrocytes, too. In addition, the researchers revealed that this virus has differentially expressed its latency genes in the EBV-associated cancers.10,14 The present research was designed to unravel the rates of detection EBV - neuropersistance in a sample of brain tissues from Iraqi patients varying in grades of astrocytomas, starting from grade I to grade IV.
Material and methods
This study was designed as a case control-study.
Sample collection: Between 2023 and 2025, fresh frozen (FF) tissue specimens were systematically obtained from the Histopathology Department at the Specialized Surgeries Hospital in Baghdad, alongside two prominent teaching hospitals located in the Babylon and Al-Najaf governorates. Samples were collected from patients with Astrocytoma grades I, II, III, and IV. All patients included had not received prior treatment that could influence disease progression and had no history of immunological disorders, a total of (100) brain tissue specimens for preserving tissue samples which were obtained from (75) patients with brain tumors, ranging in age from 5 to 75, are provided these tissues under study. From each patient, three tissue fragments were randomly obtained from different regions of the tumor core. The study's control group consisted of 25 autopsies, with ages ranging from 14 to 67, and were found to have normal brain histology and no evident neurological reasons. Ethical Approval: his research complies with the ethical guidelines set forth by the Declaration of Helsinki. Before sample collection, verbal and analytical consent was obtained from patients. The study protocol, including subject information and the informed consent form, was reviewed and approved by the local ethics committee (Document No. 7/17/1442; Reference No. M220944; approved on 21 April 2023). Extraction of Viral Genome and EBV Detection: Viral genomic DNA was extracted from brain tissues of both patient and control groups using the PATHOGENE viral DNA extraction kit (INTRON, Korea). Epstein–Barr virus (EBV) detection was subsequently carried out using PCR. PCR of EBV: PCR procedures and gel electrophoresis, including imaging of results, were conducted with extreme caution and precision to prevent contamination or experimental error. 500 Nanogram of DNA from tissues were used for PCR in order to detect EBV by using specific primers:
EBV forward primer: 5’-CCAGTGCTGTGATCGAGCATCT-3’. EBV reverse primer: 5’-CTGCTGACAAACTGCTGCATTC-3’.
Product size : 526 bp
Dilution of Primers Pairs: The primers were acquired from the IDT / USA source, where units are typically provided as a mass (in Picomoles), and Bioneer primers are typically shipped in a lyophilized primer condition. It was necessary to rehydrate the primers in sterile, nuclease-free water to create primer stocks. The oligonucleotide manufacturer provided sterile, nuclease-free H2O, which was used to prepare a master stock solution at 100 mol/µL concentration. To create the working stock, tubes were spun down before opening, followed by the addition of water as per the manufacturer's guidelines to achieve a final concentration of 100 pmol/µL. The primers were vortexed thoroughly for uniform resuspension. Then, 10 µL of the master stock was transferred to a 0.2 mL Eppendorf tube containing 90 µL of sterile, nuclease-free water. Both master and working stocks were stored at −20°C. Before use in PCR, the working stock was thawed on ice, vortexed, and stored at −20°C for later application.
Analysis by PCR: DNA (500 nanograms) was isolated from freshly frozen tumor tissues and utilized in a PCR assay to determine the EBV DNA encoding sequence. To prevent any contaminations before, during, or after accomplishing the EBV PCR reactions, great care and safeguards were used. In each PCR reaction, negative controls were also conducted.
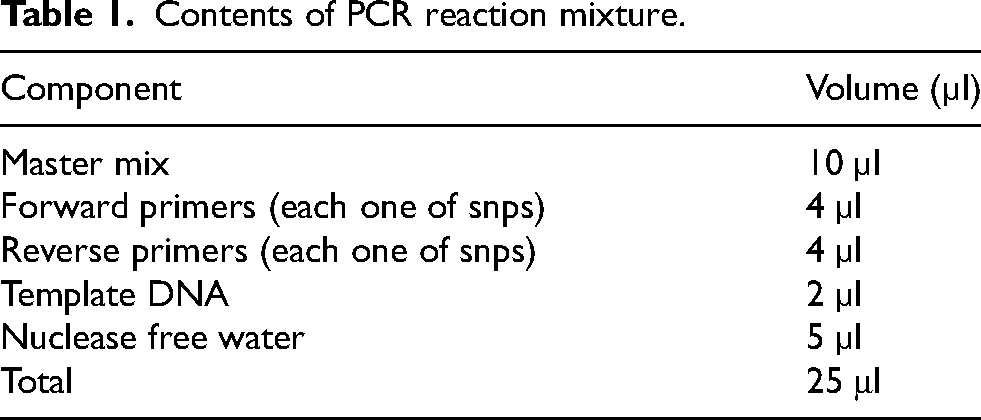
PCR Experiments: Template DNA (2 µL) was added to the prepared PCR master mix tubes, followed by one microliter each of forward and reverse primers. Amplification was performed using a traditional Biometra heat cycler (Germany). Distilled water was added to the PCR premix tubes to adjust the final reaction volume to 25 µL, as outlined in Table 1.
Thermal cycling: initiated by preheating the samples to 94°C, after which the master mix solutions were loaded into a thermal cycler (Biometra, Germany). The specific cycling conditions were manually configured, and targeted EBV polymorphic regions were amplified using specific primers, as detailed in Table 2.
Statistical Analysis: A t-test was employed to evaluate statistical significance among the study variables. All analyses were conducted using SPSS version 24, with a p-value < 0.05 deemed significant.
Results
Clinical and pathological characteristics of the studied groups
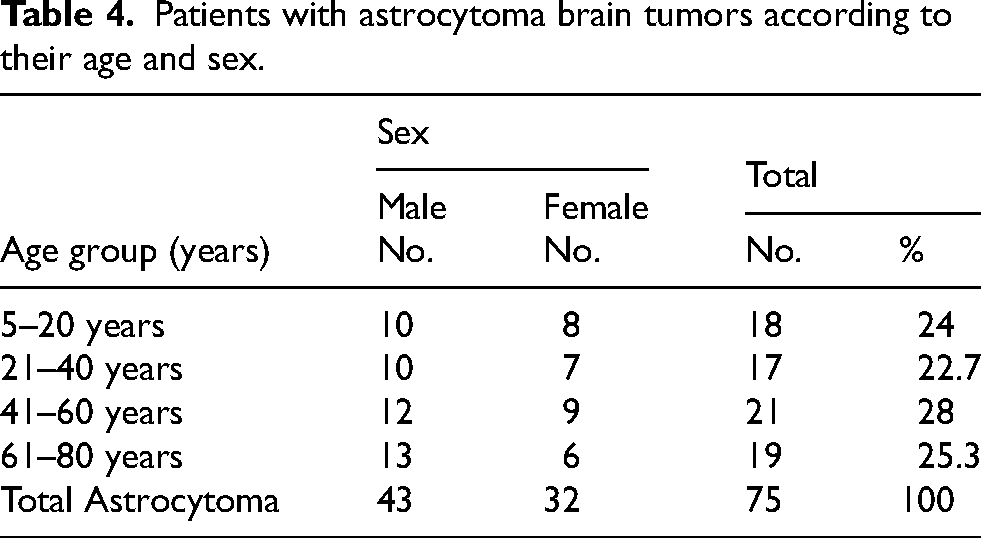
Age distribution of studied groups: The analyzed tissue samples were from astrocytoma patients aged 7 to 78 years, with a mean age of 54.3 ± 12.57 years. In contrast, control group individuals had a mean age of 51.32 ± 13.41 years. No significant age-related differences were observed (p > 0.05, Table 3). Distribution of astrocytoma patients by sex: In this study, 58% (43/75) of patients with astrocytoma and AHC were male, while 42% (32/75) were female, as illustrated in Figure 1. However, when comparing the astrocytoma group to the control group, statistical analysis revealed a significant difference (P > 0.05). Distribution of patients with astrocytoma brain tumors group according to their age stratum and sex: Regarding the age of astrocytoma brain tumors cases, Ages 5–20 years: 18/75 (24%) [10 men, 8 women], Ages 21–40 years: 17/75 (22.7%) [10 men, 7 women ], ages 41–60 years: 21/75 (28%) [12 men, 9 women ], Ages 61–80 years: 19/75 (25.3%) [13 men, 9 women]. Table 4 provides detailed demographic distribution. Distribution of studied group according to their grading:
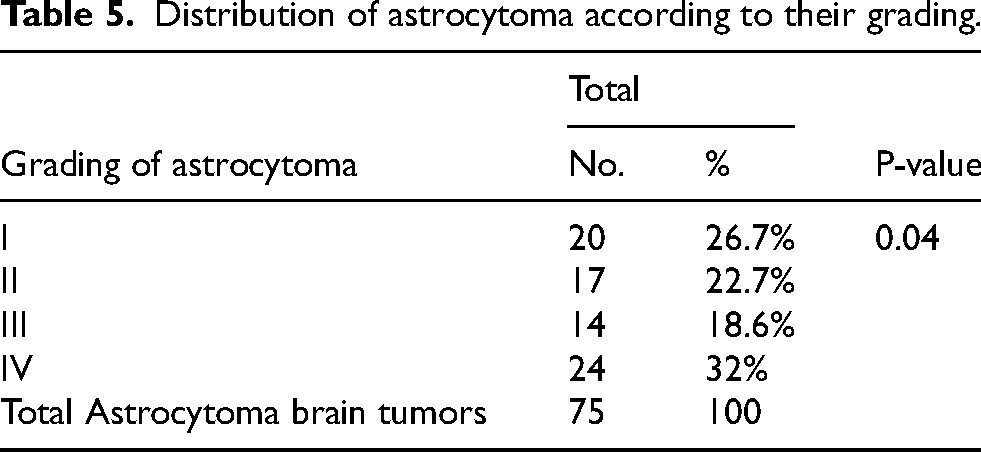
Sex Distribution of the patients with astrocytoma.. Contents of PCR reaction mixture. The study conditions for amplification the EBV gene. Distribution of patients by age. Patients with astrocytoma brain tumors according to their age and sex. In this study (grade I) was found in 20 (26.7%) patients with astrocytoma, while (grade II) was found in 17 patients with astrocytoma (22.7%), grade III was seen in 14 patients with astrocytoma which constituted (18.6%), finally, grade IV was seen in 24 patients with astrocytoma (32%) (Table 5). There existed statistically significant distinctions (P < 0.05) among the astrocytoma grading categories. Distribution of astrocytoma according to their grading.


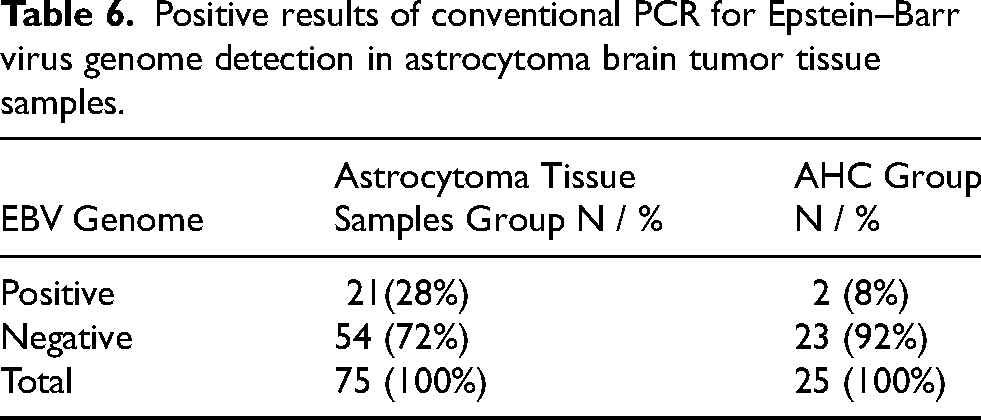
PCR analysis revealed that 28% (21 out of 75) of astrocytoma cases tested positive for the EBV genome, whereas 72% (54 out of 75) were negative, as illustrated in Table 6 and Figure 2. In contrast, in the control group, only 8% (2 out of 25) of the samples were EBV-positive. The statistical comparison between these groups demonstrated a significant difference (p = 0.03).
The EBV-PCR Results in Astrocytoma Patients Stratified by Age
The EBV DNA electrophoresis pattern (526 bp) detection in tissues from patients with astrocytoma by PCR. Lanes 1 - - refer to EBV DNA; Conditions for electrophoresis: 5 µl in each well (1% agarose and 75 V, 20 mA) for 1 h, and red safe solution staining. Positive results of conventional PCR for Epstein–Barr virus genome detection in astrocytoma brain tumor tissue samples.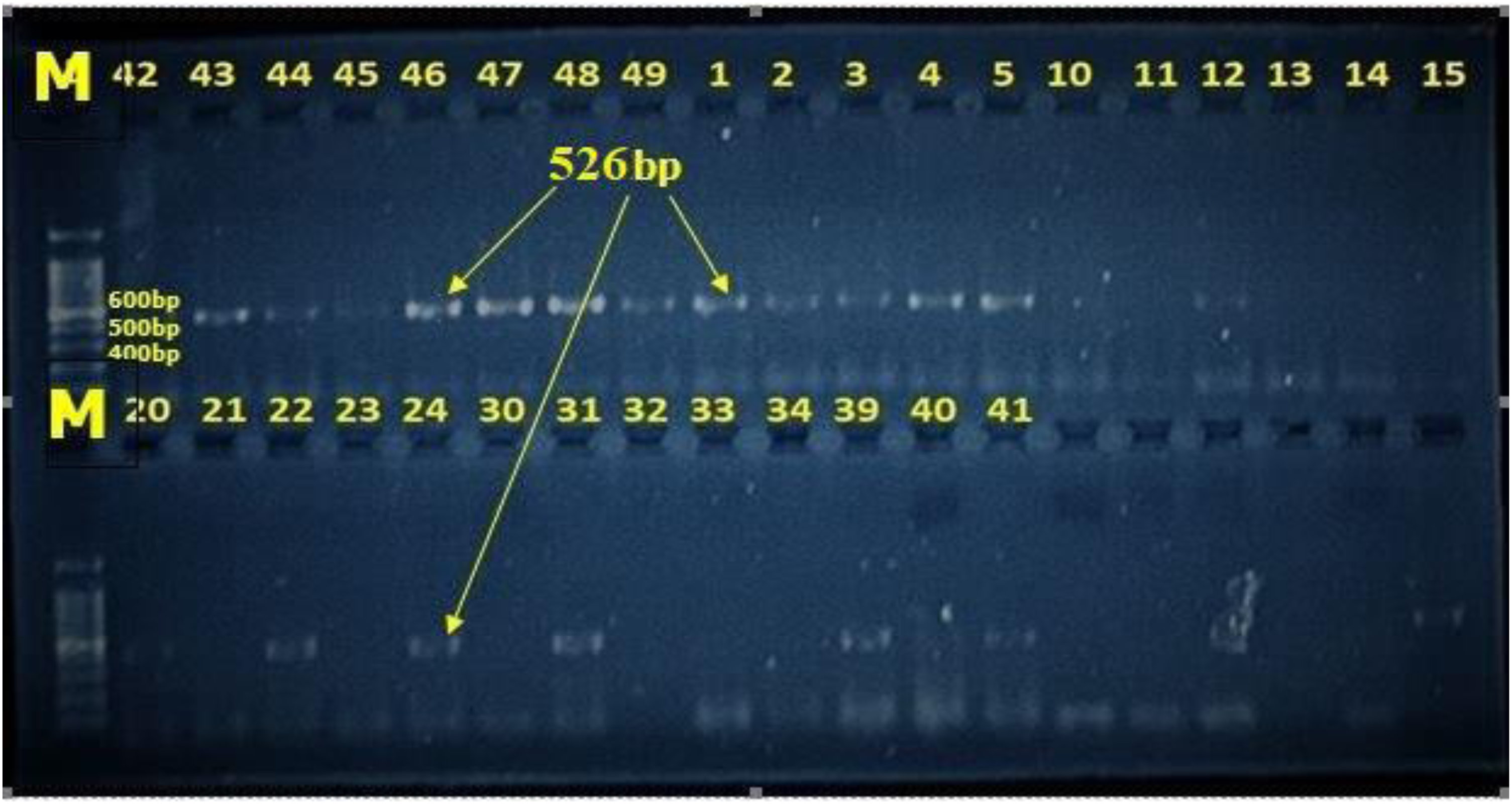
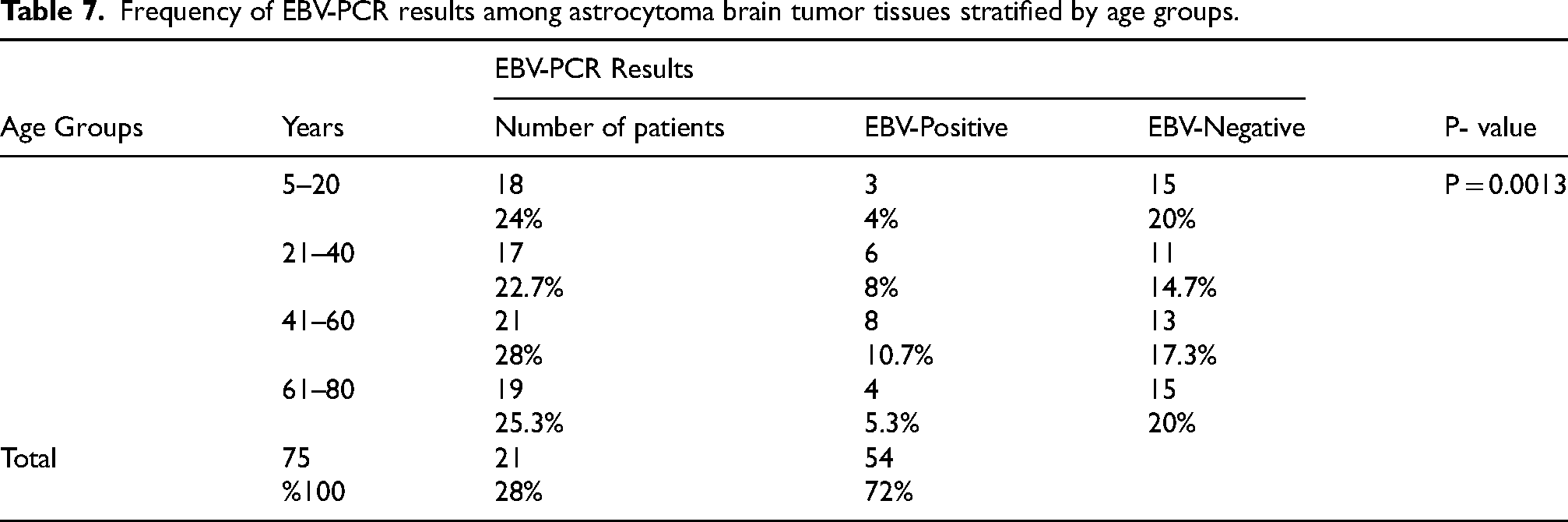
The highest prevalence of EBV DNA detection in astrocytoma brain tumor tissues was observed in the 41–60 year age group, accounting for 10.6%. In contrast, the 5–20 year age group showed a lower infection rate, at 4%. A statistical comparison between these age groups revealed a highly significant difference (P < 0.01) (Table 7).
Frequency of EBV-PCR results among astrocytoma brain tumor tissues stratified by age groups.
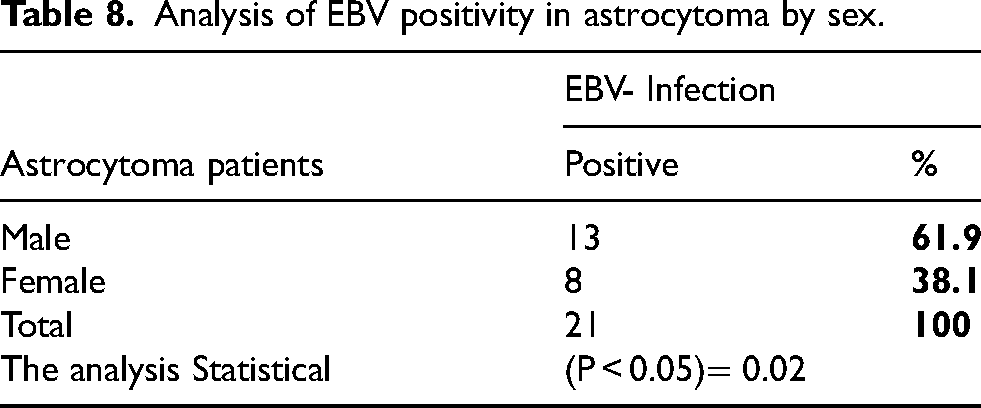
Analysis of EBV positivity in astrocytoma by sex.
Discussion
The application of various molecular technologies in clinical practices has revealed that a big list of viruses, among them EBV, have linkages, whether as a cause or an association, with brain tumorigenesis and/or their progression. 15 The objective of the present research was to unravel the rate of neurotropic EBV infection in a group of brain tissues with astrocytes taken from the group of Iraqi patients in Baghdad, and their correlation with astrocytoma grades I, II, III, and IV. For such purposes, and as shown in Table (4), the current study has enrolled 75 brain tumor cases that were diagnosed as astrocytomas, among them, 26.7% were astrocytoma grade 1, 22.7% were astrocytoma grade 2, 18.6% were astrocytoma grade 3, and 32% cases were diagnosed as glioblastoma multiform (astrocytoma grade 4). Also, Table (1) of this study shows that the age of the studied patients with different grades of astrocytoma ranged (7–78) years with a mean age of 54.3 + 12.57 years where the males accounted for 57.3% of these astrocytoma cases, while females accounted for 42.7% with a ratio of 1.3:1 of male to female (Figure 1). Epstein–Barr virus (EBV) was recognized in 1964 as the first human oncovirus. Further, this virus among other important risk factors for human cancers which were originated in the lymphocytes, epithelial cells, and mesenchymal cells. 16 EBV has clearly characterized functions in gastric carcinomas, nasopharyngeal, Hodgkin's, peripheral T-cell lymphomas, Burkitt's, thymomas, and other's diseases.17–22
In addition, the researchers had found that EBV has causal associations with many CNS disorders, like demyelinating disease, acute cerebellar ataxia, meningitis, acute encephalitis, and other CNS neuropathies, yet, the investigations intended to be directed for focusing on EBV involvement in gliomagenesis and only lately possesses the involvement of EBV in gliomas been investigated.12,23 According to the results of the Polymerase Chain Reaction Technique (PCR) for the detection of Epstein–Barr virus (EBV), 28% (21 out of 75) of the total samples of astrocytoma tissues group were positive for EBV genome detection. While, in the control tissues group, positive results for EBV were found in 8% (2 out of 25) of them, constituting statistically significant differences between these groups (Table 5). Recently, also several studies in Brazil, Slovenia, and Mexico as well as in Europe, USA, South America, and Japan, have documented positive associations of EBV with cases of gliomas. 24
Among the studied Mexican patients with gliomas by Limam et al., 25 they reported 21.4% EBV-positive results, In these cases, 24 patients had EBV DNA identified, 4 had EBER and LMP1 discovered, and all EBV-positive cases had glioblastoma multiforme (GBM) as their diagnosis. A retrospective study performed by Zavala-Vega et al. 9 On GBM-brain tissues from 21 adult Mexican patients (whose average age was 52 years, and a range of 23–83 years) and by using immunohistochemistry for LMP-1 detection as well as by using in situ hybridization for EBER expression, they reported the presence EBV infection in 6 out of 21 (28.6%) of these patients. Limam et al. 25 who studied Mexican GBM patients, also reported mixed infections of EBV both with HSV1/2 and CMV in brain tissues from these patients. A study done on GBM-brain tissues from adult Mexican patients reported the presence of mixed EBV with both HSV-1/2 infections in 4 out of 21 patients (19%) as well as mixed EBV with CMV infections in 5 out of 21 (23.8%) of these patient samples. 9 Another PCR study (2016) 26 showed that while HHV-6B and EBV were found in 13.3% and 8.9% of the examined astrocytoma samples, respectively, neither HCMV nor HHV-6A genomes were found in any of the reviewed astrocytoma samples. However, Cosset et al., study in (2014) 27 reported no detection of each the following viruses (CMV, VZV, EBV, HSV and HHV-6) in each of tissues from (low-grade gliomas, meningiomas, oligodendroglioma, oligoastrocytoma and ependymoma). Another study by Fonesca et al. 24 from Brazil in (2015) on 75 freshly frozen primary gliomatous tissues from primary glioma cases to identify EBV in these samples of tumors, by using PCR and that were confirmed by using direct sequencing, they detected 11 out of 75 gliomas (14.7%) were positive for EBV where (6 out of 11) being low-grade gliomas, followed by (2 out of 11) grade III, oligoastrocytoma (1 out of 11), ependymoma (1 out of 11), only (1 out of 11) being grade IV (GBM) and in one ependymoma, and one oligoastrocytoma, but not in any other CNS tumors including two non-HL, a tumor with EBV association has been reported previously. However, the results of Fonesca et al. 24 were contrasting the study from Slovenia in (2015), who stated that EBV-positive high-grade gliomas were the only ones. Zavala-Vega et al., 9 who carried out a study that was retrospective on brain tissues from 21 adults Mexican patients with GBM whose average age was 52 years (and had an age range of 23–83 years) had indicated the presence EBV infection in 6 out of 21 (28.6%) of patients by using immunohistochemistry for LMP-1 and by in situ hybridization for EBER expression.
A retrospective study by Zavala-Vega et al., 9 on brain tissues from adult Mexican patients with GBM discovered combination EBV and HSV-1/2 infections in 4 of the 21 patients (19%), EBV and CMV infections in 5 of the 21 GBM patients (23.8%) samples. Another study using PCR revealed non-detection of (HCMV and HHV-6) genomes in any of the astrocytoma samples, while (HHV-6B and EBV) were detected in 13.3% and 8.9%, respectively. 26 However, Cosset et al., 27 reported the non-presence of each of the following viruses: VZV, EBV, HHV-6, HSV, and CMV, in oligoastrocytoma, oligodendroglioma, meningiomas, low-grade gliomas, and ependymoma. A study by Lin et al. 26 (2016), who used multiplex droplet digital PCR for EBV detection, found 21.1% positivity of EBV (4 out of 19) in formalin-fixed paraffin-embedded GBM tissue samples but no tissue samples in the control group revealed EBV. Another study (2008) analyzed EBV both by PCR and IHC in brain tissue samples from patients with cerebellar astrocytoma, whose average age was 15.5 years, detected EBV by PCR in 9 out of 35 (30%) while by IHC revealed that none of these samples tested positive for EBV-LMP1. 28 Interestingly, a study from the USA indicated there may be more than one viral infection associated with GBMs when they reported that 8.3% (2 out of 24) of the GBM samples revealed positivity of both (HHV-6B and EBV). 9 In the study done by Karimzadeh et al., 29 they indicated statistically significant presence of EBV infection in 17.24% of tissue samples from CNS tumors and among those samples infected with EBV, astrocytoma exhibited the greatest incidence of EBV-DNA (44.4%), and IV (33.3%). Because PCR and viral-specific immunohistochemical analyses have shown bias where only specific or targeted genes or proteins of viruses are studied in tumors, 28 recently next-generation sequencing (NGS) research has been conducted to examine the existence of viral sequences in gliomas with unbiased results.29,30 In the current as well as in these previous studies, PCR and IHC viral-specific assays were biased since they only investigate targeted proteins or genes of EBV in tumors, and the next-generation sequencing (NGS) is one technology now used for rather a unbiased approach30–32 and in this respect, recently, EBV sequences in gliomas have been studied by next-generation sequencing (NGS). 33 Lastly, could it be that focusing on Epstein–Barr virus (EBV) and other herpesviruses like cytomegalovirus (CMV) in gliomas has led researchers to investigate the wrong viral candidates? Recent Next-Generation Sequencing (NGS) data suggest that most viruses—particularly CMV—are entirely absent from gliomas. Many reported positive associations may actually be artifacts, potentially explained by factors such as the high sequence homology between detected viral fragments and host DNA, as observed in chromosomal telomere repeats. 30
Conclusions
This study's notably high detection rate of Epstein-Barr virus (EBV) in glioma samples suggests a possible involvement of the virus in brain tumor development. To further validate these findings and clarify the potential role of EBV in tumor initiation, advanced molecular research is strongly recommended. Such investigations could provide deeper insight into the mechanisms underlying this viral association with gliomas and its implications for cancer progression.
Footnotes
Acknowledgments
We would like to the staff at the Al-Mustaqbal University and the University of Baghdad for their continuous support and encouragement. Special thanks to the laboratory technicians for their assistance with the PCR techniques and data analysis.
Authors’ Contributions
Saad Hasan Mohammed Ali: Conceptualization of the study, methodology, interpretation and analysis of data, validation, formal analysis, resources, data curation, preparation of the manuscript, and writing-review and editing. Heba Fadhil Hassan: Data collection, interpretation and analysis of data, validation, preparation of the manuscript, and writing-review and editing.Shakir H. Mohammed Al-Alwany: Review of methodology, interpretation and analysis of data, critical revisions of the manuscript, and supervision of the study. Athraa Y. Al-hijazi: Histopathological analysis, interpretation and analysis of data, validation, and writing-review and editing.Basim Mohammed Khashman: Implementation of PCR techniques, interpretation and analysis of data, validation, and writing-review and editing.All authors have read and approved the final manuscript.
Ethical approval and informed consent statements
This study was conducted in accordance with the ethical guidelines set forth by the Declaration of Helsinki. Ethical approval was obtained from the local ethics committee (Document No. 7/17/1442; Reference No. M220944) on April 21, 2023.Informed consent was obtained verbally and in writing from all participants prior to sample collection. Participants were fully informed about the study's purpose, procedures, and potential risks, ensuring their voluntary participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available upon request from the corresponding author.