
Abstract
Background:
Clostridium sordellii infections are rare and highly lethal. They are most associated with medical abortions and other genitourinary procedures. We report a fatal case of C. sordellii bacteremia from a perforated low rectal cancer with rectovaginal fistula.
Case Presentation:
A 60-year-old female presented with 10 days of abdominal pain, loose stools, and hematochezia. She developed rapidly progressive septic shock. Imaging identified a perforated rectal mass, pneumovagina, and a large pelvic abscess. She underwent fecal diversion and drainage of the pelvic abscess. Despite this intervention, she had refractory septic shock with multisystem organ failure resulting in death. Blood cultures grew C. sordellii post-mortem.
Conclusion:
C. sordellii infections are often fatal if not treated immediately. Clinicians must have a high index of suspicion in rectal cancer with associated gynecological involvement.
Introduction and Background
Clostridium sordellii is an anaerobic gram-positive bacillus known for its role in peri-partum infections and septic abortions. 1 Infections are highly lethal because of the development of toxic shock syndrome, with mortality rates approaching 70%.2–3 Infections have occurred after gynecological, prostatic, skin/soft tissue, and ophthalmical surgeries, as well as following intra-venous drug use and trauma.2,4–7 There are no reports to our knowledge of a case of C. sordellii bacteremia resulting from a perforated rectal cancer.
Presentation of Case
Informed consent was obtained from the legal next of kin for publication of this case report. A 60-year-old female presented to the emergency department with 10 days of left lower quadrant abdominal pain. She reported experiencing loose stools with hematochezia and orthostatic symptoms. She denied fevers, chills, nausea, and vomiting. She denied significant medical history and abdominal surgical history and had never had a colonoscopy. Her social history was positive for daily tobacco and alcohol use. Her presenting vital signs were temperature 36.7 C, heart rate 97 beats per minute, blood pressure 88/66 mmHg, respiratory rate 29 breaths per minute, oxygen saturation >92% on room air. The patient rapidly progressed into severe septic shock despite crystalloid resuscitation and required norepinephrine infusion to maintain adequate blood pressure. On physical exam, she appeared cachectic; the abdomen was soft, distended, and diffusely tender to palpation with rebound tenderness. Gross blood was noted in the rectal vault. A firm mass was palpable at 4 cm proximal to the anal verge. Significant laboratory values were a white blood cell count of 757,000 cells/µL and lactic acid 3.1 mmol/L. Computed tomography of the abdomen and pelvis revealed a large, perforated rectal mass with pneumovagina, concerning for rectovaginal fistula, pneumoperitoneum, and a multiloculated pelvic abscess (Fig. 1). There were enlarged retroperitoneal and iliac chain lymph nodes as well as numerous small liver lesions concerning for a metastatic process. Blood and urine cultures were obtained, and she was given a dose of piperacillin/tazobactam. An emergent surgical consultation was obtained. She underwent an exploratory laparotomy with sigmoid loop colostomy and transrectal biopsy of the rectal mass. A mesenteric lymph node was sent for biopsy. A vaginal culture was not obtained. A surgical drain was placed in the pelvis. The mass did not involve the posterior rectal wall; therefore, the presacral space was not explored. Postoperatively, she was admitted to the surgical intensive care unit and continued to require ventilator support for acute hypoxic and hypercapnic respiratory failure. She continued to have refractory severe septic shock despite three additional vasopressor (vasopressin, epinephrine, and angiotensin II) infusions. Antimicrobial coverage was broadened to vancomycin and micafungin. Additionally, the patient was started on steroids and continuous renal replacement therapy for refractory metabolic acidosis. She developed significant interstitial fluid accumulation of pulmonary edema, hypoxia, and anasarca. Cardiology consultation was obtained because of echocardiogram findings of severe concentric left ventricular hypertrophy with echo-dense myocardium concerning for an infiltrative cardiomyopathy and a small pericardial effusion (Fig. 2). Hematology consultation was obtained because of an aggressive leukemoid reaction with an increase in white blood cell count to 118,000 cells/µL. She developed abdominal compartment syndrome requiring chemical paralysis and ultimately a bedside decompressive laparotomy. The patient then suffered a terminal cardiac arrest.
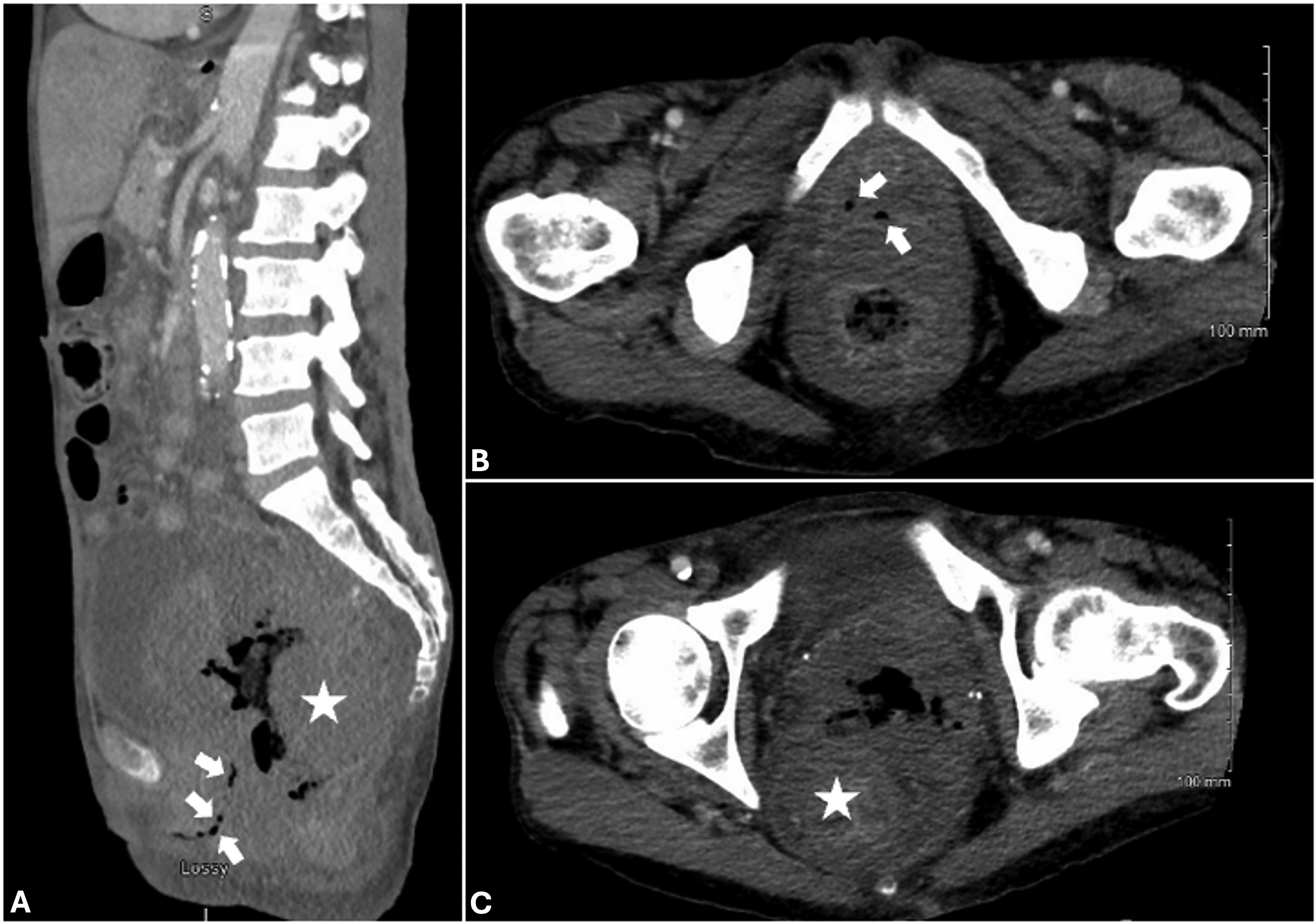
CT of the abdomen and pelvis in the
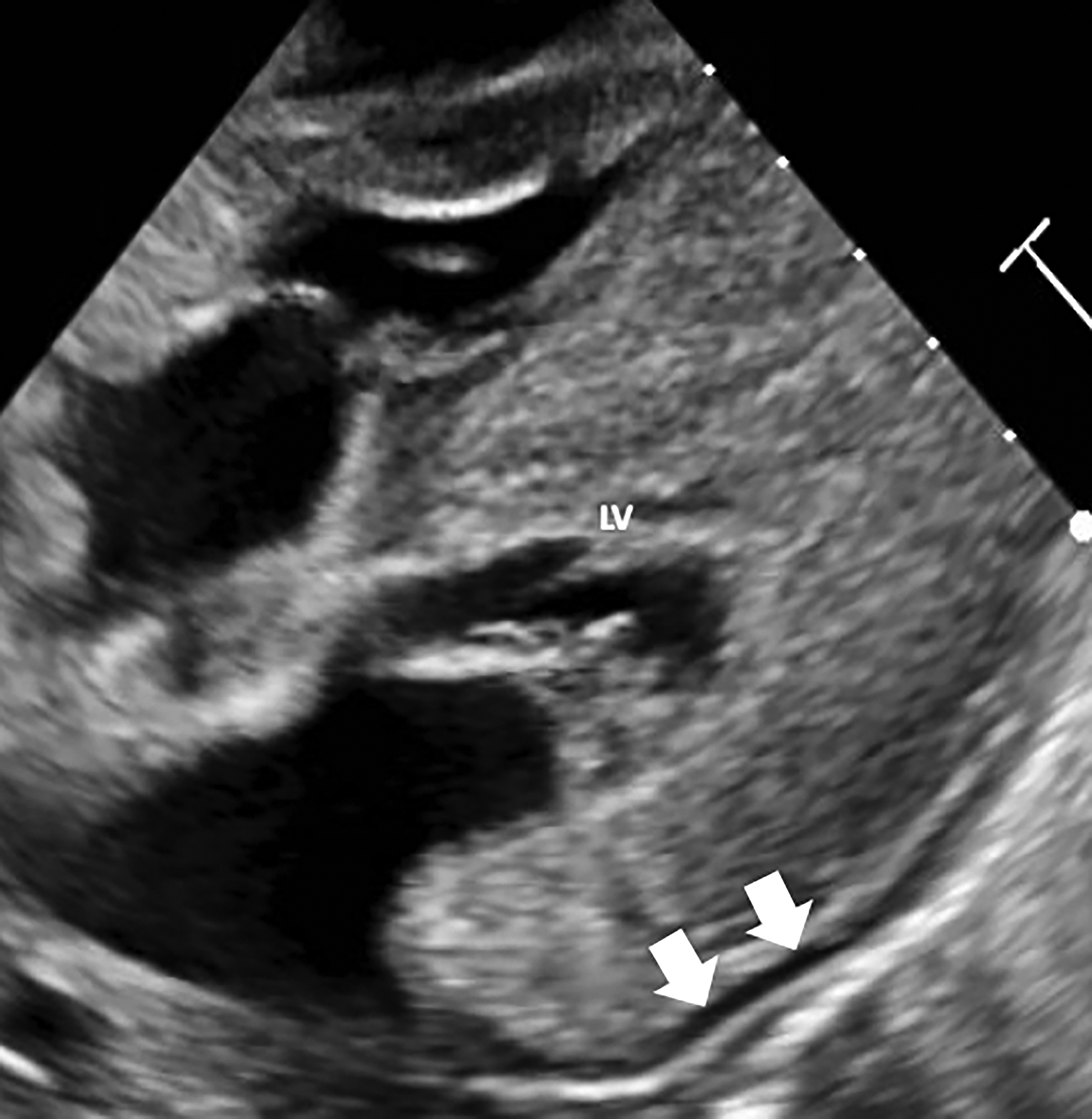
Echocardiogram of the left ventricle (LV) in the long axis. White arrows indicate a small pericardial effusion.
Post-mortem, C. sordellii and Fusobacterium species were isolated from blood cultures. Pathological review of intra-operative biopsies was consistent with ischemic colitis and poorly differentiated adenocarcinoma. A post-mortem examination was declined.
Discussion and Literature Review
C. sordellii bacteremia is exceedingly rare, with only 11 reported cases in the literature. Infections are typically associated with the genitourinary tract and often occur in immunocompromised patients.8,9 C. sordellii has been implicated in septic abortions, both with instrumentation of the reproductive tract and in mifepristone-induced abortions.1,10 A study by Chong et al. in 2016 sampled the vaginal and rectal flora of 4,152 women and found that C. sordellii was present in 3.4% of women. 11 Bacteremia has also been described in men after transrectal prostate biopsy. 12 While more commonly associated with vaginal flora, our patient had radiographical evidence of a rectovaginal fistula with an infiltrative rectal mass and pneumovagina, which may have facilitated the spread of the bacteria.
Most C. sordellii isolates are sensitive to beta-lactams, clindamycin, and tetracyclines. 2 Appropriate antibiotic coverage was selected with piperacillin-tazobactam. Clindamycin can be considered to reduce toxin production, though there are no studies to date demonstrating this in C. sordellii infections. This approach has shown benefit in other Clostridial infections. 13
There are two known clostridial cytotoxins that are responsible for the toxic shock syndrome associated with C. sordellii. 3 The lethal toxin (TscL) and hemorrhagic toxin (TscH) modify the intrinsic Rho GTPase activity to alter vascular endothelial cells, resulting in significant increases in vascular permeability. 14 The presence of the lethal toxin gene is rare and was present in 0.8% of 238 C. sordellii isolates in colonized, healthy women. 11 We were not able to perform the testing for these toxins in our patient but suspect the lethal toxin was present because of our patient developing the characteristic rapidly progressing pulmonary edema and anasarca associated with the lethal toxin.
In response to overwhelming infection, both mature and immature leukocytes may be released into the blood stream in a phenomenon known as a leukemoid reaction. Our patient’s leukocytosis peaked at 118,000 cells/µL by hospital day 2. Pathological review of the blood smear was consistent with a leukemoid reaction. In the largest review of C. sordellii cases to date, Aldape et al. found that a leukemoid reaction was a poor prognostic indicator and was present in 80% of fatal cases. No survivors in this review demonstrated a leukemoid reaction. 2
Proximal colonic diversion with wide pelvic drainage was utilized rather than resection of the perforated rectal mass. This is a reasonable option in a patient with profound hemodynamic instability, as it achieves stool diversion while minimizing time in the operating room. However, definitive source control may not be obtained.
Though rare, cardiac complications have been reported with C. sordellii infections. Caundhry et al., described an 8-month-old infant who developed constrictive pericarditis with pyopericardium and cardiac tamponade and a 28-year-old female who developed infective endocarditis.15–16 Our patient was found to have a pericardial effusion without tamponade physiology. The pericardial fluid was not sampled. The structural changes on echocardiogram, including severe left ventricular hypertrophy and evidence of an infiltrative cardiomyopathy were felt to represent chronic disease processes.
Conclusion
C. sordellii causes a rapidly progressive and often fatal infection with a characteristic toxic shock syndrome. Prior reports describe cases following instrumentation of the genitourinary tract; however, we report a case following a perforated, infiltrative, low rectal cancer. Clinicians should consider this in the differential diagnosis of rapidly progressing septic shock following a colon operation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding supported the publication of this case report.