
Abstract
Objective:
To evaluate the impact of the Safe Surgery Program on surgical site infection (SSI) rates in spinal procedures and total hip and knee arthroplasties. The analysis compared the pre-implementation (2006–2010) and post-implementation (2010–2022) periods to determine the effect of the program on SSI rate reduction.
Methods:
We conducted a nested case–control study including adults (>18 y). Cases were patients with SSI matched 1:1 to controls by procedure type, gender, age, and operation date. Risk factors, antimicrobial agent use, hospital costs, and checklist adherence were analyzed.
Results:
A total of 142 patients were included in the analysis (71 cases and 71 matched controls). Most surgical procedures (84.5%) occurred after the implementation of the Safe Surgery Program, with 78.3% adherence to the World Health Organization checklist. In the analysis, blood transfusion was significantly associated with SSI (odds ratio = 2.67; 95% confidence interval: 1.04–6.82; p = 0.040), whereas a longer operative time showed a borderline trend (p = 0.050). SSI rates decreased from 2.0% to 0.7% after program implementation (p = 0.017). Hospital-wide antimicrobial agent consumption increased for cefazolin (+75 defined daily doses per 1,000 patient-days), cefuroxime (+10.6), and vancomycin (+10.2) during the same period, reflecting broader compliance with surgical prophylaxis protocols. Hospital costs were significantly lower among patients without SSI (p = 0.024).
Conclusions:
Implementation of the Safe Surgery Program was associated with reduced SSI incidence and hospital costs in complex orthopedic procedures. Blood transfusion remained an important risk factor, highlighting the value of optimization of peri-operative management and adherence to surgical safety practices.
Keywords
Background
Surgical site infections (SSIs) significantly impact patient morbidity, mortality, and healthcare costs, contributing to thousands of deaths and billions in expenditures annually in the United States alone.1,2 In Brazil and Latin America, SSIs are a leading cause of healthcare-associated infections, contributing to prolonged hospital stays and substantial resource utilization in both public and private health systems.3–5 Elderly patients are especially vulnerable, and as the global population ages, the demand for orthopedic procedures such as hip and knee arthroplasty is rising. 6 Although these procedures improve quality of life, they carry an SSI risk, which is exacerbated by biofilm-forming bacteria such as Staphylococcus aureus on prosthetic materials.7,8
Preventing SSI requires a multifaceted tactic. Key measures include appropriate antibiotic agent prophylaxis, which can reduce SSI rates by up to 50%.9,10 Recognizing that process failures also contribute to risk, the World Health Organization (WHO) introduced the Surgical Safety Checklist (SSC) in 200811,12 The WHO SSC was designed as a structured cognitive aid to ensure that critical steps in patient care are not overlooked. It encourages multidisciplinary communication, establishes a culture of accountability, and provides opportunities to detect potential errors before they cause harm. 11 Evidence from multi-center trials has demonstrated that checklist implementation reduces peri-operative mortality by nearly 50% and complication rates by more than one-third. 12
Despite global dissemination, adherence and effectiveness vary widely. Contextual factors such as institutional culture, team dynamics, resource availability, and leadership commitment strongly influence outcomes. Studies from low- and middle-income countries show even greater relative benefits from SSC use, reflecting the higher baseline rates of adverse surgical outcomes in resource-limited settings. 13 Brazil, with a heterogeneous healthcare system, presents a valuable case for assessing checklist effectiveness in complex surgical populations. An orthopedic surgical procedure is therefore an important setting for evaluating such safety interventions.
This study aimed to evaluate the impact of the “Safe Surgery Program,” centered on the WHO SSC, on SSI rates in a tertiary hospital. The analysis compared a 16-year period, spanning the pre-implementation (2006–2010) and post-implementation (2010–2022) eras, to determine the program’s effect on infection reduction in complex orthopedic procedures.
Methods
Study setting and population
A nested case–control study was conducted at Hospital Israelita Albert Einstein, a private not-for-profit philanthropic hospital with 670 beds in the city of São Paulo, Brazil. Adult patients (>18 y) who underwent elective orthopedic procedures—including spinal arthrodesis (instrumented) or decompression (non-instrumented), as well as total hip or knee arthroplasties, regardless of whether prosthesis implantation was performed between January 2006 and December 2022 were eligible. To ensure adequate post-operative surveillance, only patients with a hospital stay longer than 48 h were included.
Study design
Cases were defined as patients who developed SSI, identified according to U.S. Centers for Disease Control and Prevention’s National Healthcare Safety Network criteria. 14 Each case was matched 1:1 with a control undergoing the same procedure, based on gender, age (±20 y), and date of operation (±120 d). Analyses were stratified into two time periods: pre-implementation (January 2006 to July 2010) and post-implementation (August 2010 to December 2022) of the WHO SSC.
Data collection
Data were extracted from institutional electronic systems (Cerner Millennium, SAP, REDCap) and included demographic information, comorbidities (with diabetes mellitus analyzed separately), American Society of Anesthesiologists (ASA) physical status, pre-operative laboratory values, corticosteroid use, blood transfusion, anesthesia type, procedure duration, antimicrobial agent prophylaxis (≤24 h), and adherence to the checklist. Microbiological data were obtained from the infection control unit and the clinical microbiology laboratory. Antimicrobial agent consumption was measured as defined daily doses per 1,000 patient-days (DDD/1,000 PD). Cost data, retrieved from the hospital costing system, included room charges, medications, supplies, and re-admissions.
Outcomes
The primary outcome was the occurrence of SSI. Secondary outcomes included risk factors associated with SSI, antimicrobial agent consumption, and total hospital costs for the admission during which the operation was performed.
Statistical analysis
No formal sample size calculation was performed, as this was a convenience sample including all eligible cases of SSI and their matched controls identified during the study period (2006–2022). Continuous variables were summarized as medians and interquartile ranges (IQRs), whereas categorical variables were presented as frequencies. Associations with SSI were assessed using conditional logistic regression, providing odds ratios (OR) with 95% confidence intervals (CIs). Variables with p <0.10 in uni-variable analysis were entered into multi-variable models using backward stepwise selection. Hospital costs were analyzed with generalized estimating equations (gamma distribution, log-link). Antimicrobial agent consumption trends were assessed with autoregressive integrated moving average time-series models. All analyses were performed in SPSS (IBM Corp.) and R (forecast package). A two-sided p < 0.05 was considered statistically significant.
Ethics
The study was approved by the Institutional Ethics Committee of Hospital Israelita Albert Einstein (Certificado de Apresentação de Apreciação Ética: 63739822.4.0000.0071, approval number: 5.702.040, date: October 14, 2022), which waived the requirement for informed consent because of its retrospective design and use of anonymized data.
Results
Between January 2006 and December 2022, a total of 9,163 patients underwent elective orthopedic procedures at our institution, including spinal operations and total hip and knee arthroplasties. This cohort formed the basis for the descriptive epidemiology and time-series comparison of SSI rates before and after the implementation of the Safe Surgery Program. From this overall cohort, a nested case–control subset was selected for in-depth analysis of risk factors. After applying strict eligibility criteria excluding revision surgical procedures, fractures, bone tumors, and deformities, the final analytical sample comprised 142 individuals. Exactly half of them developed an SSI (n = 71), whereas the other half served as matched controls (n = 71). When stratified by time period, only 22 patients (15.5%) had undergone an operation before the implementation of the Safe Surgery Program, whereas the majority (120 patients, 84.5%) were operated afterward. This imbalance reflects both the natural increase in surgical activity and the broader institutional adoption of the WHO SSC over time. The distribution of procedures was consistent with patterns typically observed in high-volume orthopedic centers: spinal arthrodesis represented the largest proportion (30.3%), followed by decompression (28.2%), hip arthroplasty (26.8%), and knee arthroplasty (14.8%). The similar proportions between cases and controls further support the comparability of the groups (Fig. 1).
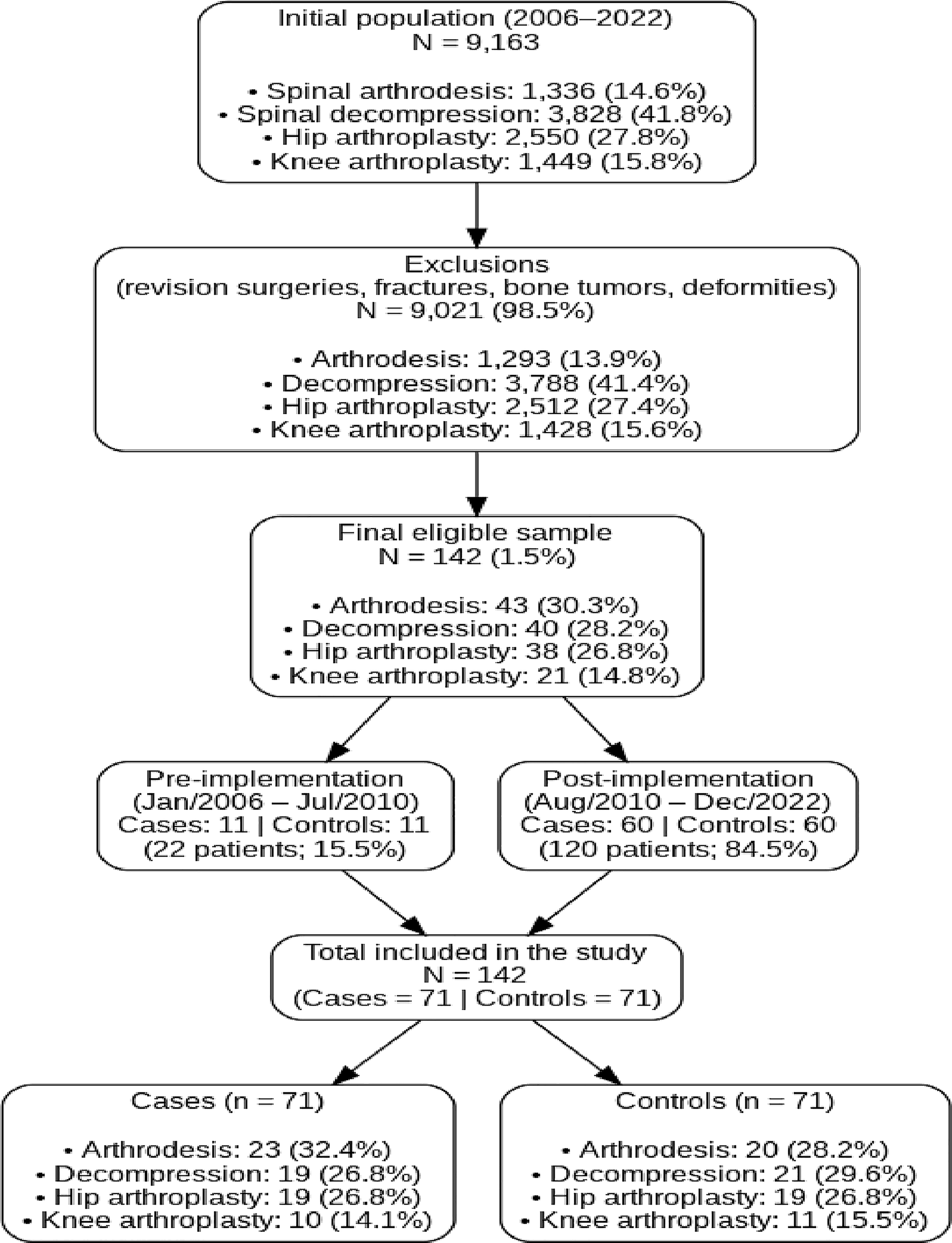
Flowchart of patient selection and distribution according to procedure type and study period.
Nearly six out of 10 participants were male (59.9%), and the median age was 64 years, with an IQR spanning from 50 to 77 years. This age distribution highlights a predominance of older adults, consistent with populations undergoing a major orthopedic surgical procedure. Body composition data added further nuance: the median body mass index was 27.7 kg/m2, placing the average patient in the overweight range. Importantly, more than one-third of the sample (35.9%) met the criteria for obesity, and obesity was somewhat more frequent among those who developed an infection compared with those who did not (40.8% vs. 31.0%). Although not statistically significant, this pattern aligns with prior literature describing obesity as a risk amplifier for post-operative complications. A comprehensive overview of baseline characteristics can be found in Supplementary Table S1.
The risk factor analysis identified several associations. Blood transfusion stood out as a strong predictor of SSI, with patients requiring transfusion having more than double the risk of infection compared with those who did not (OR = 2.67; 95% CI: 1.04–6.82; p = 0.040). Surgical duration also revealed a borderline association, suggesting that each additional increment of operative time could contribute to heightened risk (OR = 1.27; p = 0.050). Other variables showed trends, such as general anesthesia (OR = 4.00; p = 0.080) and the presence of neoplasia (OR = 6.00; p = 0.097), but these did not reach conventional thresholds of statistical significance. Notably, neither obesity nor most comorbidities were independently linked to SSI in this dataset. In multi-variable analysis, only transfusion remained independently associated with infection, reinforcing its role as a modifiable and clinically relevant factor (OR = 2.67; 95% CI: 1.04–6.82; p = 0.040) (Tables 1 and 2).
Factors Associated with Surgical Site Infection in Spine (Arthrodesis and Decompression), Total Hip, and Knee Arthroplasty Procedures: A Case–Control Study (142 Patients), January 2006 to December 2022*
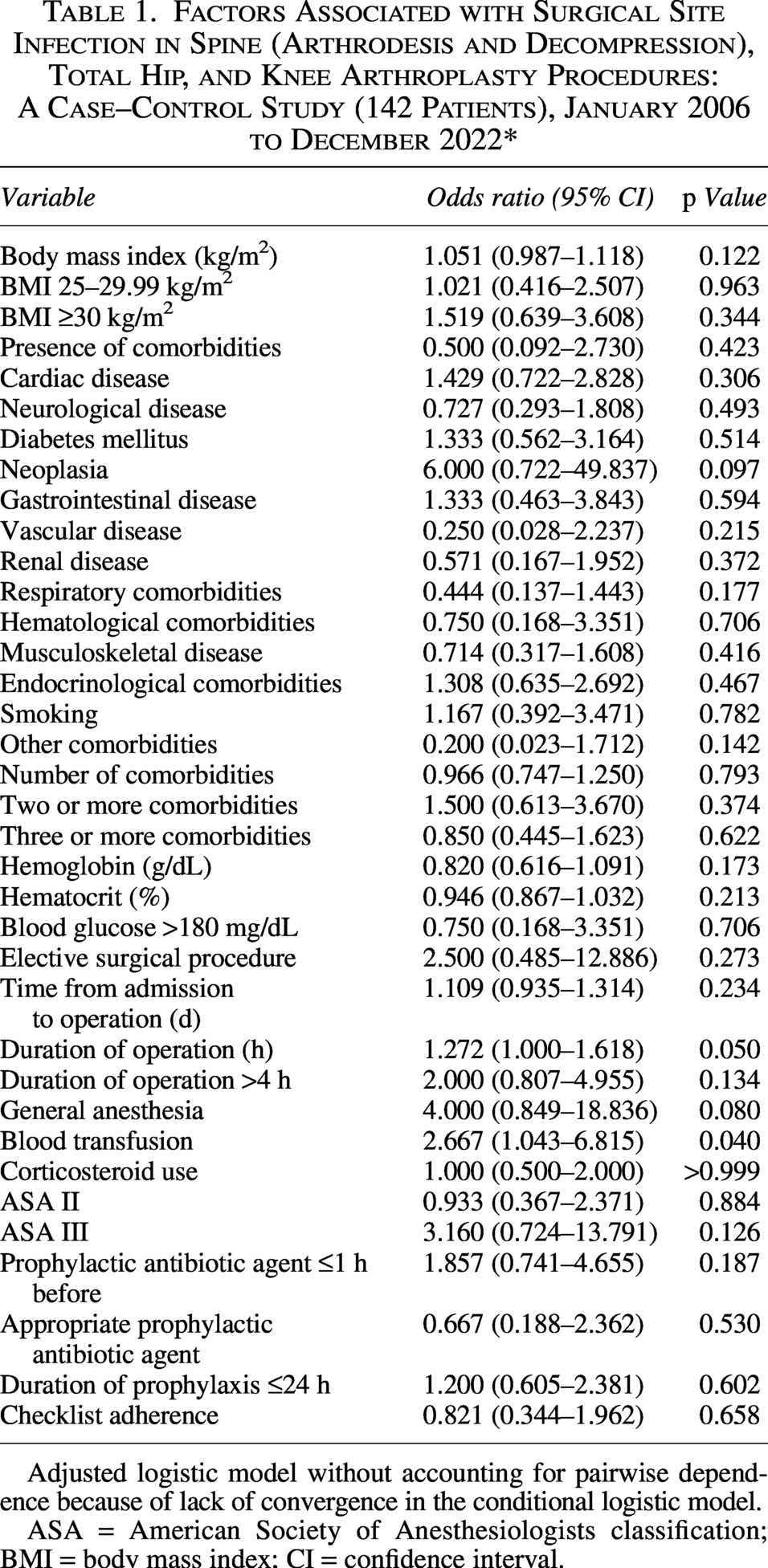
Adjusted logistic model without accounting for pairwise dependence because of lack of convergence in the conditional logistic model.
ASA = American Society of Anesthesiologists classification; BMI = body mass index; CI = confidence interval.
Multi-Variable Logistic Regression Model for Risk of Surgical Site Infection
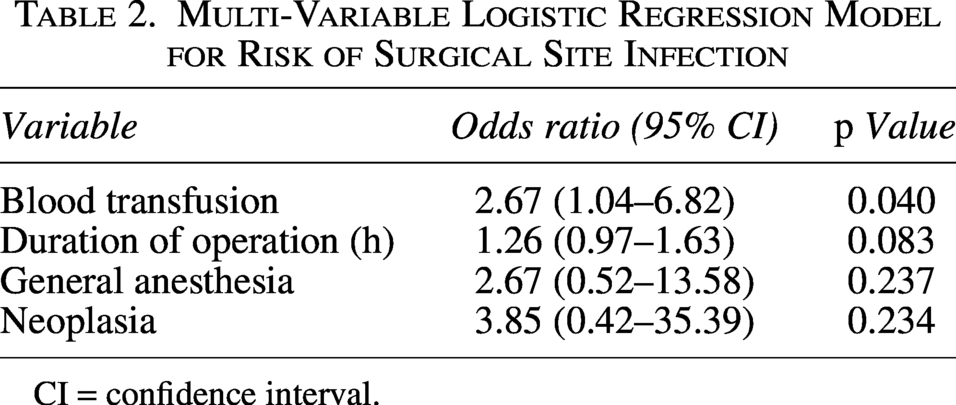
CI = confidence interval.
Regarding the SSC itself, adherence was formally documented in 78.3% of procedures performed after the program’s implementation. This represents encouraging uptake, yet statistical analysis did not reveal a significant protective effect against SSI in isolation (OR = 0.82; p = 0.658). Notably, the critical “Time Out” and “Sign Out” steps were completed in approximately 80% of both cases and controls, suggesting that although the checklist became embedded in daily practice, compliance was not absolute (Table 3).
Adherence to the Surgical Safety Checklist Among Patients Undergoing Orthopedic Operation

n, number of patients.
Surgical activity at the hospital grew exponentially during the study period. Procedures increased by more than 1,190%, climbing from only 99 operations in 2006 to an impressive 1,280 in 2022. Despite this massive growth in surgical volume, the institutional rate of SSI declined markedly. Before implementation of the program (2006–2009), SSI occurred in about 2.0% of patients. After implementation (2010–2022), the rate fell to 0.7%, a statistically significant improvement (p = 0.017). The trajectory reached its most remarkable milestone in 2018, when the infection rate dropped to just 0.1%, underscoring the sustained benefits of standardized surgical safety practices (Fig. 2).
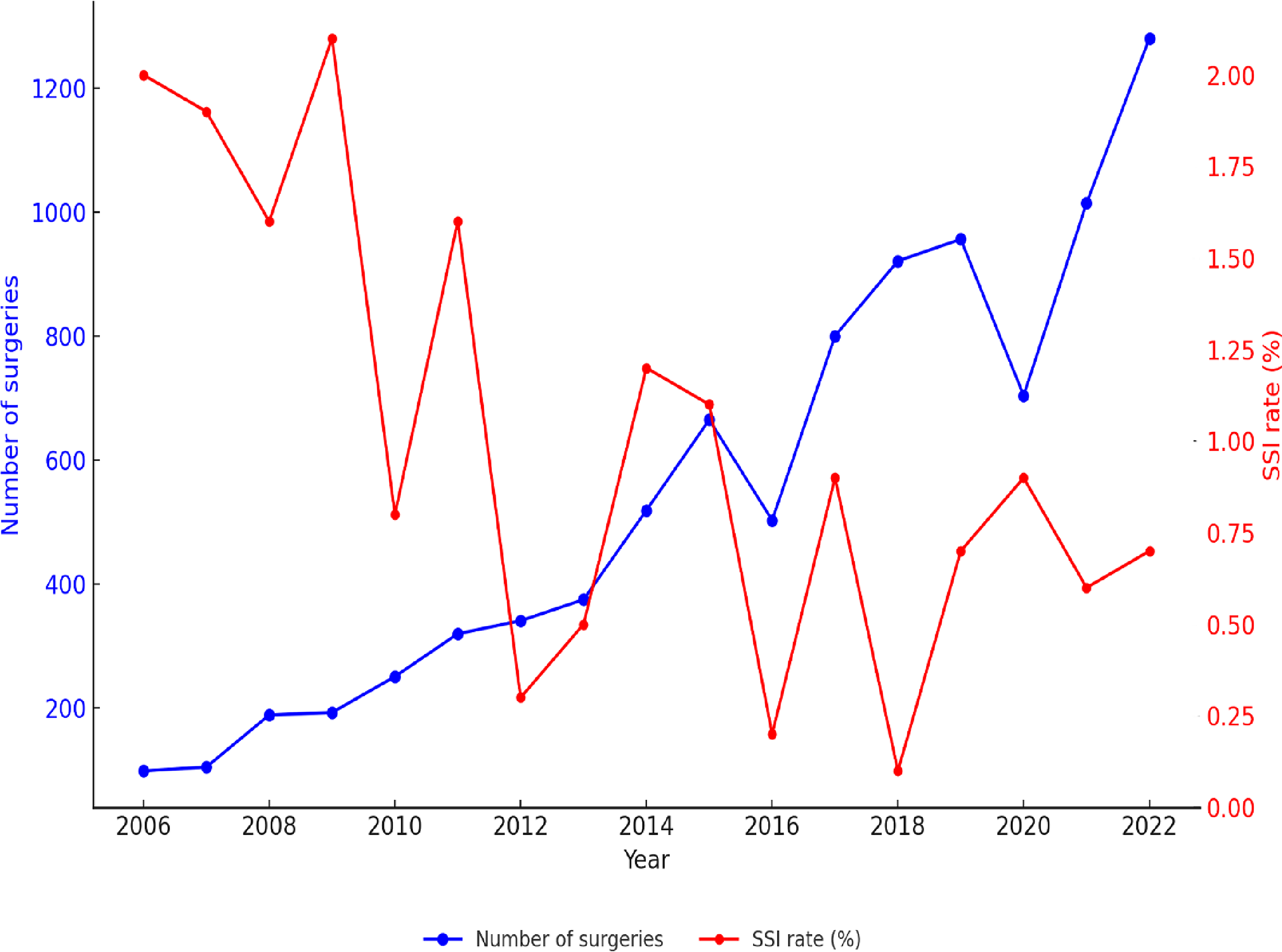
Annual number of orthopedic operations and surgical site infection (SSI) rates, January 2006 to December 2022.
Trends in antimicrobial agent use further contextualized these findings. After the program was introduced, hospital-wide consumption of certain antibiotic agents rose, particularly cefazolin (+75 DDD/1,000 PD), cefuroxime (+10.6), and vancomycin (+10.2). This reflects both increased surgical activity and the reinforcement of peri-operative prophylaxis protocols (Supplementary Table S2).
The economic dimension of our results is equally compelling. Among patients without infection, hospital costs fell sharply after the intervention, with a cost ratio of 0.50 (95% CI: 0.27–0.91; p = 0.024), indicating that care became almost twice as efficient in financial terms. For patients with SSI, the reduction in costs was less pronounced and did not achieve statistical significance (0.67; p = 0.121). Nevertheless, when comparing cases and controls directly, the economic burden of infection was evident. Before the program, patients with SSI incurred costs 1.56 times higher than their matched counterparts, and this differential widened after the program to 2.09-fold greater (95% CI: 1.46–3.01; p < 0.001). The persistent financial toll of SSI, even in the context of global improvements in surgical safety, can be found in Supplementary Table S3.
Discussion
Surgical safety has increasingly been recognized not merely as an operational requirement but also as a cornerstone of patient-centered care. Our findings, derived from a 16-year evaluation of high-complexity orthopedic procedures, reinforce this perspective: the implementation of the WHO SSC was associated with a sustained decline in SSI rates and a measurable reduction in hospital costs. Although this echoes global evidence,11–13,15 the importance lies in understanding why these changes occurred and what lessons can be extrapolated for both clinical practice and healthcare policy.
One of the most compelling insights from our analysis is that its effectiveness cannot be attributed to the mechanical act of checking boxes. Rather, the SSC functions as a catalyst for cultivating a culture of verification, accountability, and team communication. This cultural shift is subtle yet powerful. Our data support this interpretation. The high adherence rate (78.3%) and the concurrent, significant increase in the consumption of key prophylactic antibiotic agents following program implementation suggest that the checklist was integrated into a broader institutional effort to standardize and reinforce safety protocols, rather than being a stand-alone intervention. In a high-stakes environment such as an orthopedic surgical procedure, where minor oversights can have cascading consequences, the SSC provides structured opportunities for interdisciplinary dialogue. By formalizing these checkpoints, the SSC reduces ambiguity, minimizes miscommunication, and reinforces collective responsibility.16,17
Our study population’s demographic profile was typical for orthopedic populations requiring arthroplasty or spinal operation: predominantly male, with a median age of 64 years, and overweight on average. These features are not trivial descriptors; they highlight a population inherently vulnerable to complications. Older adults accumulate comorbidities, present with diminished physiological reserve, and are more likely to require peri-operative support measures. Obesity, present in more than one-third of the cohort, deserves specific mention. This prevalence is comparable with that of the general Brazilian adult population, in which approximately 60% are overweight, and 25% meet the criteria for obesity according to the national surveillance data. 18 Although obesity did not achieve statistical significance in our dataset, prior studies have demonstrated up to a 2.5-fold increased risk of infection in patients with obesity undergoing implant-based operations.7,19–22
Among all the variables examined, blood transfusion emerged as the most robust and independent risk factor for SSI. This is not merely an incidental association but one supported by extensive literature as well. Transfusion-related immunomodulation is a well-documented phenomenon whereby allogeneic blood transfusion suppresses cellular immunity, alters cytokine profiles, and diminishes host defense mechanisms. Beyond immunological pathways, transfusion can contribute to volume overload, hemodilution, and iron availability, conditions that facilitate bacterial growth.23–25
The clinical implications are profound. Unlike age or comorbidities, transfusion is a modifiable risk factor. Restrictive transfusion tactics, now recommended in many guidelines, have been shown to be both safe and effective in reducing complications. Furthermore, blood conservation techniques such as pre-operative anemia correction, intra-operative cell salvage, and the use of pharmacological agents including tranexamic acid offer practical avenues to minimize transfusion exposure. Our findings provide institutional evidence that these tactics are not only beneficial for blood stewardship but also integral to infection prevention. This result should resonate strongly with policymakers and clinicians alike: reducing unnecessary transfusions is not merely about conserving a scarce resource but also about directly lowering the risk of life-threatening infections and the associated financial burden.23–25
Although surgical duration demonstrated only borderline statistical significance in our dataset, its clinical relevance cannot be understated. Multiple studies confirm that each additional hour of operative time incrementally increases the likelihood of SSI, with procedures exceeding six hours tripling the risk.26–29 The mechanisms are intuitive: longer exposure increases opportunities for contamination, tissue desiccation, hypothermia, and hemodynamic instability. Mitigation tactics include thorough pre-operative planning, streamlined surgical workflows, and intra-operative warming to maintain normothermia.28,29 Although some factors influencing duration are intrinsic to case complexity, others such as unnecessary delays, equipment malfunctions, or poor coordination are preventable through systems-level improvements.28,29
Our analysis did not demonstrate statistically significant associations between higher ASA class or general anesthesia and SSI. However, the literature consistently identifies these as risk indicators.10,30 Patients classified as ASA III or IV often carry multiple comorbidities that compromise the immune defense and healing capacity. General anesthesia, although sometimes unavoidable, can extend operative time and impose greater physiological stress. The absence of significance in our study may be attributable to sample size limitations or uniformity in anesthetic practice, but it does not diminish the relevance of these variables as markers of clinical complexity.10,30
The lack of a statistical association between antibiotic agent prophylaxis and SSI in our cohort likely reflects a high degree of protocol adherence. Prophylaxis was administered within 60 minutes before incision, tailored to institutional epidemiology, and discontinued within 24 hours. Such standardization is widely regarded as one of the most cost-effective interventions in SSI prevention. The uniformity of practice likely blunted variability, rendering a statistical association undetectable, yet its contribution to the overall reduction in SSI cannot be overstated.9,11,31,32 In many ways, antibiotic agent prophylaxis provided the silent backdrop against which the SSC and other interventions operated.
The economic analysis of this study demonstrated a significant reduction in hospital costs for patients without SSI in the post-implementation period of the SSC (p = 0.024). This finding is consistent with robust evidence of cost-effectiveness associated with surgical safety protocols. Systematic reviews have shown that cost reductions are primarily driven by fewer surgical complications, shorter hospital stays, and decreased need for additional therapeutic interventions such as re-operations and prolonged antimicrobial agent treatments. 2 On average, the WHO checklist-based safety programs can lower direct hospital costs by 7%–20%, depending on the type of procedure and baseline adverse event rates. 2 Furthermore, recent studies emphasize that the economic benefits are magnified in an elective orthopedic operation, given the high expenses related to implants and the complexity of infectious complications. 33
Several limitations of this study should be considered. First, its retrospective, observational, and single-center design limits the ability to establish direct causality, and the findings may have been influenced by unmeasured confounding factors. Second, the focus on a high-complexity orthopedic population may affect the generalizability of the results to other surgical specialties or lower complexity settings. The specific cultural context and high level of protocol adherence at our institution factors that were likely instrumental in achieving the observed outcomes may not be fully replicable in other healthcare environments. Furthermore, the extended study period introduces the possibility of historical biases, such as the evolution of clinical practices and technologies, which were not explicitly measured but may have contributed to the observed improvements. Finally, post-operative infection surveillance at our institution does not routinely extend beyond hospital discharge, which limits the detection of SSIs that, according to the literature, account for approximately 60% of cases and are generally identified after discharge. This limitation prevents the capture of post-discharge events such as re-admissions or re-operations, which may significantly impact costs and patient outcomes. 34 Furthermore, the financial impact of an SSI is greatly amplified when prosthetic implants are involved, because of potential implant removal, multi-stage revisions, and long-term antimicrobial agent therapy. Our cost analysis, restricted to the index hospitalization, therefore cannot capture this substantial potential long-term economic burden. Consequently, our cost analysis likely underestimates the true economic burden of SSI, and the reported infection rates should be interpreted as in-hospital incidence rather than complete 30- or 90-day SSI rates.
Conclusions
Our study demonstrated a significant reduction in SSI following the implementation of the Safe Surgery Program. It highlights how patient safety initiatives should go beyond isolated interventions and instead be integrated into a broader institutional culture that prioritizes multidisciplinary communication, process standardization, and evidence-based practices. Orthopedic populations, given their complexity, serve as an ideal model to illustrate both the challenges and the benefits of surgical safety interventions. Future research should focus on tactics to increase adherence to the checklist, assess its impact in other surgical specialties, and explore the integration of digital technologies and real-time feedback mechanisms to further strengthen the safety culture. In addition, cost-effectiveness analyses across different healthcare systems will be essential to support widespread implementation.
Footnotes
Acknowledgments
The authors thank all the participants for their contributions to this study.
Author Disclosure Statement
All authors report no conflicts of interest relevant to this article.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.