
Abstract
Introduction:
Necrotizing pneumonia (NP) is a rare entity seen to occur in 0.9%–7% of cases of community-acquired pneumonia in the pediatric population. Medical management remains the cornerstone of treatment. However, the destruction of both parenchyma and blood vessels impairs blood flow, limiting antibiotic concentrations and allowing the infection to persist. Although surgical management remains debated, some authors advocate for it in cases of medical treatment failure or extensive disease. The objective of this study was to present the surgical outcomes of our experience in treating NP in the pediatric population.
Methods:
A retrospective and observational study was conducted on all cases of NP in children who required surgical management between January 2022 and June 2024.
Results:
During the study period, a total of 142 pediatric thoracic surgeries were performed, of which 25 involved patients with NP, who were included in our analysis. The median age was 3 years (2–4), with a nearly equal gender distribution (52% female, n = 13). The median duration of symptoms prior to the surgical procedure was 27 days (22–36), antibiotic therapy duration ranged from 5 to 18 days. On the basis of computed tomography findings regarding the extent of parenchymal involvement, 17 patients underwent sublobar resections, while 8 required lobar resections. While no statistically significant differences were observed in post-operative outcomes between groups, it is noteworthy that patients who underwent lobectomy experienced a higher frequency of complications.
Conclusion:
Surgical intervention, typically involving resection of necrotic lung tissue, may be considered in carefully selected pediatric patients who demonstrate persistent clinical deterioration despite optimized medical therapy and exhibit extensive parenchymal destruction on imaging. It is critical to tailor the treatment plan to the patient’s clinical status and disease progression.
Introduction
Necrotizing pneumonia (NP) is a rare entity seen to occur in 0.9%–7% of cases of community-acquired pneumonia in the pediatric population. 1 This is a severe manifestation of pneumonia that has a rapid progression from consolidation to necrosis, ultimately leading to cavitation and gangrene of the lung parenchyma. 2 This uncommon condition was first described in the 1940s and posed a significant challenge in terms of management, with mortality reaching 45% in both adult and pediatric patients. 3 Medical management remains the cornerstone of treatment. However, the destruction of both parenchyma and blood vessels impairs blood flow, limiting antibiotic concentrations and allowing the infection to persist. 4 Although surgical management remains debated, some authors advocate for it in cases of medical treatment failure or extensive disease.2,5 In our Institute, surgical management is proposed as an adjuvant to medical treatment when this has failed. The objective of this study was to present the surgical outcomes of our experience in treating NP in the pediatric population.
Methods
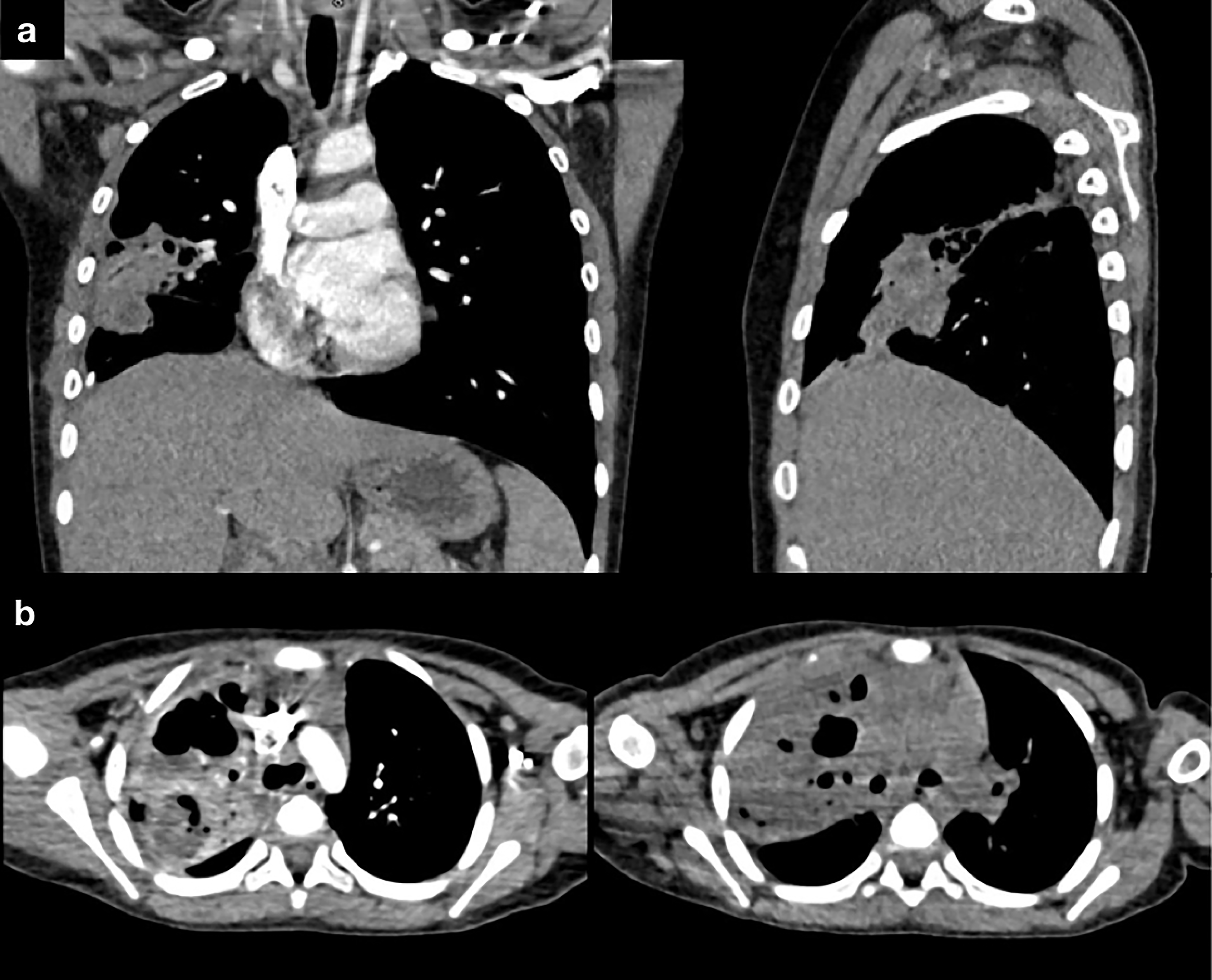
A retrospective observational study was carried out from January 2022 to June 2024 at the National Institute of Respiratory Diseases “Ismael Cosío Villegas.” This study was conducted following the recommendations of the World Medical Association (Declaration of Helsinki). The Institutional Review Board and Ethics Committee of the Instituto Nacional de Enfermedades Respiratorias approved our study with the following registration number: C81-24. We included patients aged <18 who were diagnosed with NP and, as part of their clinical evaluation, had a contrast-enhanced chest computed tomography (CT), which also allowed for surgical planning (Fig. 1). Patients with missing data on their files were excluded from the study. Consent was obtained from parents or guardians, and minors were provided with information to assess their understanding of the purpose of the research. For this work, the STROBE guidelines for conducting observational studies were followed. 6
The following clinical data were extracted from the patients’ files: age, gender, comorbidities, symptom duration, duration of antibiotic treatment, time from diagnosis to surgical procudure, type of resection, complications, length of hospitalization, and mortality.
Post-operative mortality was defined as any death occurring within 30 days after the surgical procedure. Prolonged air leak (PAL) was defined as air leak beyond the 5th post-operative day. Surgical intervention was considered only after failure of optimized medical therapy. Failure of medical treatment was defined as persistent or rising inflammatory markers (including leukocytosis and/or elevated acute phase reactants) and continued oxygen requirements despite appropriate intra-venous antibiotic therapy. Radiologic progression on contrast-enhanced CT, with extensive cavitation or parenchymal destruction, further supported the decision for operative management.
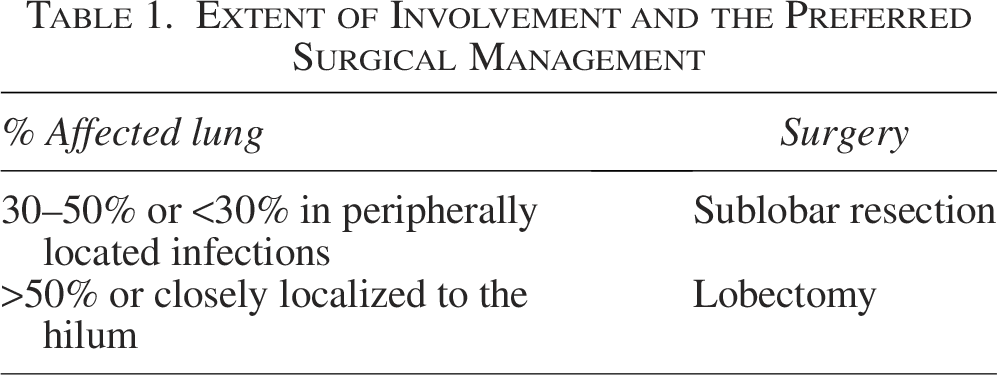
The extent and location of parenchymal involvement were used to guide the type of resection. Patients with predominantly peripheral disease or limited lobar involvement were considered for sublobar resection, whereas those with extensive parenchymal destruction or disease involving central/hilar structures were considered for lobectomy (Table 1).
Extent of Involvement and the Preferred Surgical Management
Surgical technique
General anesthesia and single-lung ventilation with an endotracheal tube and bronchial blocker were used. The patient was positioned in the right or left lateral decubitus position based on the laterality of the lung involvement. For the surgical procedure, all patients were planned for a video-assisted thoracic surgical procedure approach. Once inside the chest cavity, adhesions were dissected, followed by close evaluation of the affected pulmonary tissue, and intra-operative review of the CT to determine the resection to be carried out. This followed cavity washout and placement of 1–2 chest drains.
Post-operative care
Patients were discharged after the pleural drain was removed, confirming the absence of leaks and adequate lung expansion by means of a control chest X-ray, and after completing antibiotic treatment directed at isolated microorganisms. All tissue was sent for histopathological analysis (Fig. 2).
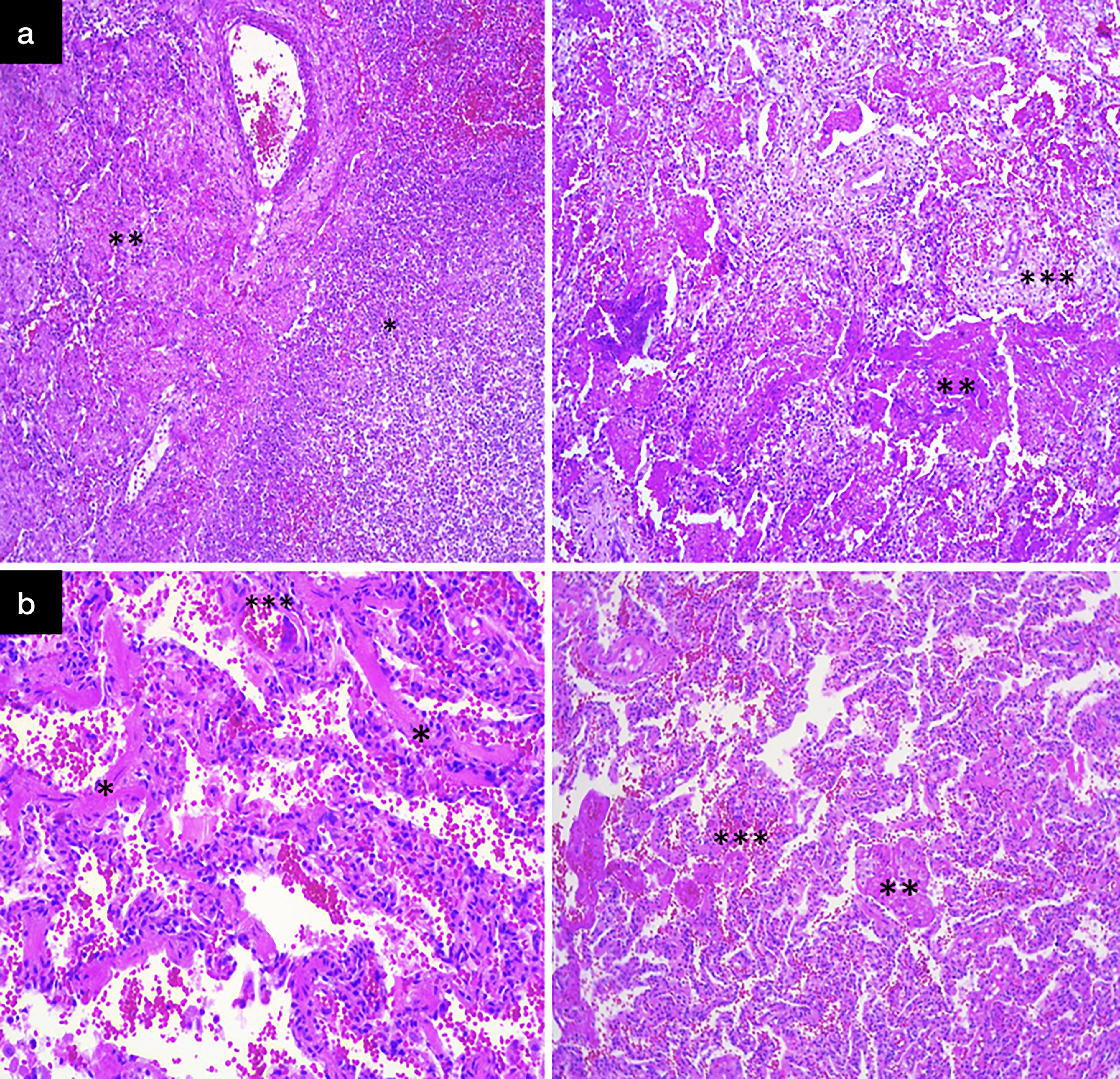
Histopathological findings following resection of the infected tissue.
Statistical analysis
Categorical variables are presented as frequencies with percentages (%), while continuous variables are shown as medians and interquartile ranges. The Shapiro-Wilk test was used to assess the distribution of the data. For bivariate analysis, comparisons were made using the Mann-Whitney U test, Pearson’s chi-squared test, and Fisher exact test, exact test for non-parametric data. Statistical analysis was performed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA), with a significance level set at a p value <0.05.
Results
During the study period, a total of 142 pediatric thoracic surgeries were performed, of which 25 involved patients with NP that were included in our analysis. Table 2 provides a summary of the included patients. The median age was 3 years (2–4), with a nearly equal gender distribution (52% female, n = 13). Among these patients, five had a prior history of pneumonia, three presented with mild-to-moderate malnutrition, three with prolonged neonatal jaundice, and one with a history of gastroesophageal reflux disease. The median duration of symptoms prior to the surgical procedure was 27 days (22–36). During this period, patients had received intra-venous antibiotic therapy over a period ranging from 5 to 18 days. Leukocytosis was observed in 64% of cases (n = 16) and persisted despite intra-venous antibiotic therapy. Elevated C-reactive protein levels were present in all patients. Microbiological cultures were positive in only five patients (20%), with Streptococcus pneumoniae being the most frequently isolated pathogen.
Description of the Cases
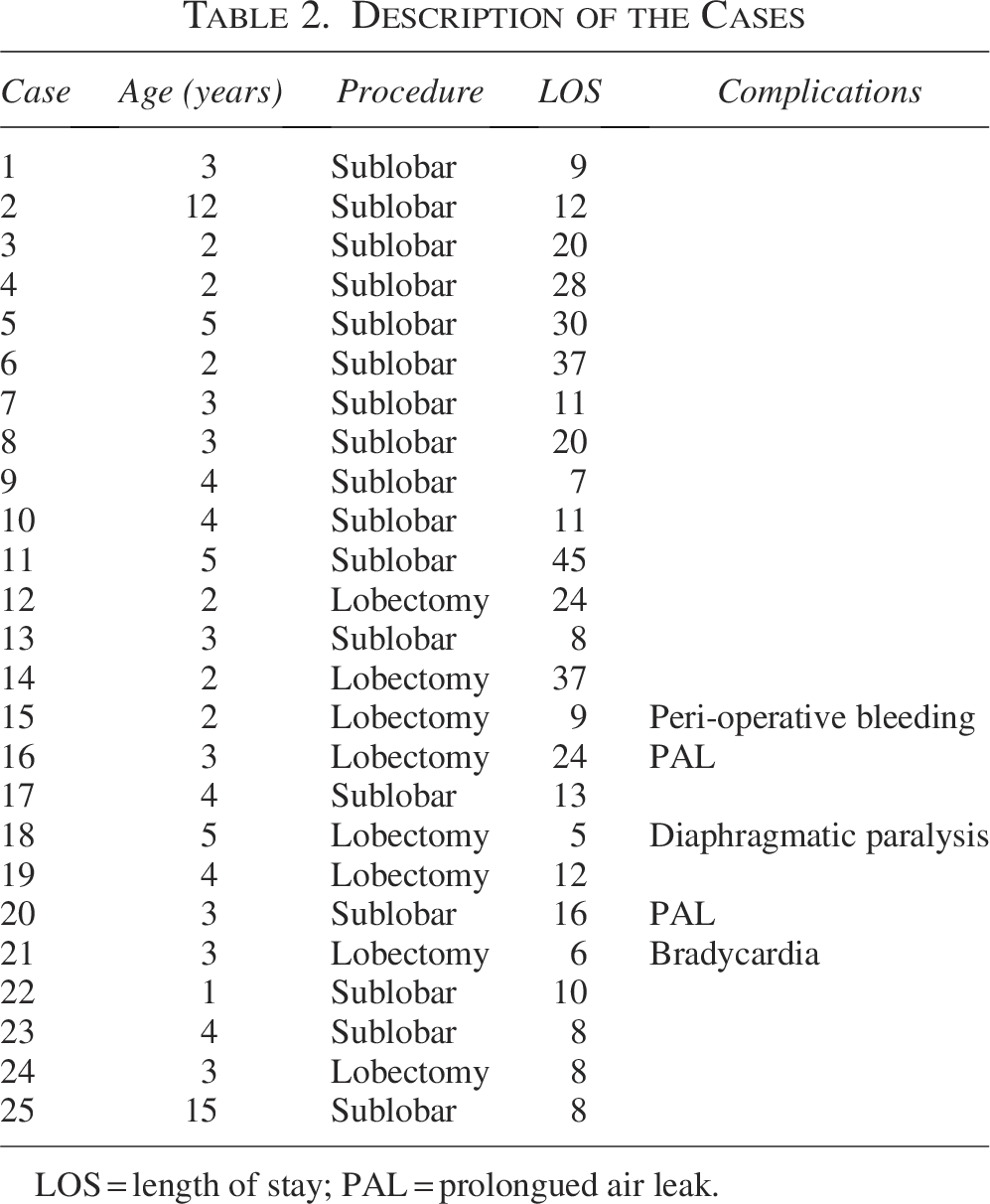
LOS = length of stay; PAL = prolongued air leak.
Operative characteristics
Right-sided involvement was observed in 64% of cases (n = 16), predominantly affecting the lower lobes (68%, n = 17). On the basis of CT findings regarding the extent of parenchymal involvement, 17 patients underwent sublobar resections, while 8 required lobar resections. Among the sublobar procedures, 14 were necrosectomies and 3 were wedge resections. Post-operative complications occurred in 20% of patients and included PAL (n = 2), diaphragmatic paralysis, hypoxic bradycardia, and intra-operative bleeding (one patient each). Three patients required re-operation. The median length of hospital stay was 12 days (8–22), without any post-operative mortality. While no statistically significant differences were observed in post-operative outcomes between groups, it is noteworthy that patients who underwent lobectomy experienced a higher frequency of complications. These data are summarized in Table 3.
Comparing the Post-Operative Outcomes Between Lobar and Sublobar Resections
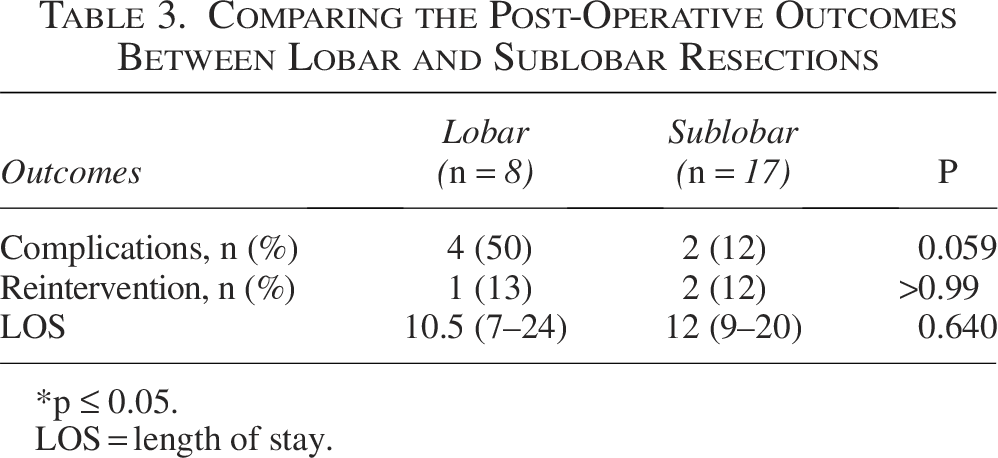
*p ≤ 0.05.
LOS = length of stay.
Discussion
NP in children is a rare but serious complication of bacterial pneumonia, occurring in approximately 0.9%–7% of cases. It is characterized by intense inflammation and pulmonary consolidation, accompanied by vascular thrombosis that leads to parenchymal necrosis and cavitation, often with coalescing lesions. 1 The resulting disruption of blood flow to the affected lung tissue impairs antibiotic penetration, reducing therapeutic efficacy and promoting the progression of necrosis. 7 This study aimed to analyze the characteristics of pediatric patients with NP who underwent surgical treatment at our institution. It is important to emphasize that the patients included in this study represented a highly selected cohort with advanced disease who had failed conservative management, for whom surgical resection was considered after clinical deterioration despite optimized medical therapy. While the standard of care is medical management with antibiotic therapy, some authors have advocated for surgical intervention in cases with complications, an incomplete response to conservative treatment, or extensive involvement of the lung parenchyma.8,9 In such cases, the goals of surgical intervention are twofold: to address complications and to manage progressive necrosis of the lung parenchyma. 9
As reported in other studies, our most common isolated pathogen was Streptococcus pneumonia, 10 although it is important to note that the low rate of microorganisms isolated through culture may be because of the prolonged period of antibiotic therapy the patients had prior to being referred to our institution.
All patients in our study underwent pre-operative chest CT, which is now considered the standard imaging modality for diagnosing NP. In addition to confirming the diagnosis, CT played a critical role in pre-operative planning. This imaging approach is also valuable in differentiating NP from lung abscess, the latter typically presenting as a single thick-walled cavity, whereas NP often manifests as multiple thin-walled cavities that may coalesce into a larger lesion. 8
Even though the indications for surgical procedure in NP are still debated, some authors argue that prompt removal of the necrotic parenchyma is especially indicated for those with respiratory distress or complications associated with NP. 11 Regarding hospitalization, our patients exhibited a similar distribution to that reported in other studies.10,12–14 In terms of the volume of lung tissue resected, there were no significant differences between patients who underwent lobectomy and those who received sublobar resections. However, it is important to acknowledge the small sample size in our study, which may limit the statistical power of these findings. Notably, the lobectomy group experienced a higher proportion of complications, likely reflecting a more advanced disease stage rather than an association with the extent of resection itself. While post-operative hospitalization appears to benefit from surgical removal of the infectious focus, the potential long-term consequences of lung resection in pediatric patients warrant careful consideration. Even though evidence suggests it may have minimal effect on parameters such as FVC and FEV1, some authors have emphasized the impact of resection on pulmonary function.7,8
Although there is no established timeframe for surgical intervention, the study by Dalponte et al. found that delayed surgical procedure was associated with higher rates of complications and progressive parenchymal infection. 15 In our study, surgical intervention was performed after a median symptom duration of 27 days, by which time the disease had generally advanced to a critically debilitating stage, making the surgical procedure a potentially life-saving measure. Nevertheless, the management of NP should prioritize the least invasive strategies whenever possible, carefully balancing the risks of a conservative, watch-and-wait approach against those associated with surgical intervention. In the context of critically ill patients with NP, it is imperative to individualize treatment plans based on the patient’s clinical status and disease progression.
Although NP remains a relatively rare condition, several authors have reported an increase in its incidence in recent years. This trend is likely attributable to factors such as rising antibiotic resistance and the emergence of more virulent infectious agents.16,17 With the increasing number of patients presenting with NP, there is an urgent need for standardized treatment guidelines to ensure accurate categorization and optimal management of affected patients.
Our study has several limitations. First, the small sample size restricts the generalizability of our findings. Additionally, the retrospective design may introduce potential sources of bias. Furthermore, the absence of long-term follow-up limits our ability to assess the extended outcomes of patients who underwent surgical resection.
Conclusion
NP is a rare but severe complication of pulmonary infection. Failure to respond to medical management significantly increases the risk of serious outcomes, including respiratory failure and sepsis. Surgical intervention, typically involving resection of necrotic lung tissue, may be considered in carefully selected pediatric patients who demonstrate persistent clinical deterioration despite optimized medical therapy and exhibit extensive parenchymal destruction on imaging. While minimally invasive approaches appear feasible, operative management should remain reserved for refractory cases, and treatment must be individualized according to the patient’s clinical status and disease progression.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Institutional Review Board and Ethics Committee of the National Institute of Respiratory Diseases (Instituto Nacional de Enfermedades Respiratorias) with the following registration number: C81-24.
Authors’ Contributions
Conception and design: All authors. Administrative support: All authors. Provision of study materials or patients: All authors. Collection and assembly of data: All authors. Data analysis and interpretation: P.G.-d.S.d.R., and M.M.F.; Manuscript writing: All authors. Final approval of article: All authors.
Footnotes
Acknowledgments
The authors have completed the STROBE reporting checklist.
Data Sharing Statement
The data from this project are available upon reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.