
Abstract
Background:
Infectious complications following emergency colectomy are a significant cause of morbidity and mortality. We aimed to identify predictors of infection after emergency colectomy.
Patients and Methods:
We analyzed the 2013–2017 American College of Surgeons National Surgical Quality Improvement Program database to identify patients ≥ 18 years undergoing emergency colectomy. The primary outcome was post-operative infectious complication rate, defined as the presence of sepsis, septic shock, surgical site infection, pneumonia, or urinary tract infection. Multivariable logistic regression was used to investigate the effect of pre-operative/operative factors on infection risk.
Results:
Of 40,913 included patients, 17,481 (42.7%) developed infectious complications. On multivariable analyses, pre-operative factors associated with increased odds of infectious complications were body mass index ≥30, chronic obstructive pulmonary disease, bleeding disorder, ascites, smoking, dependent functional status, American Society of Anesthesiologists ≥3, blood urea nitrogen ≥ 20 mg/dL, and albumin ≤ 3 g/dL. Additionally, dirty wound class and open, delayed, or prolonged surgical procedure were associated with increased infection risk.
Conclusions:
Identifying predictors of infection following emergency colectomy may inform perioperative decision-making and guide strategies to reduce infection-related morbidity.
Introduction
Colectomy is a frequently performed surgical procedure indicated for a range of elective and emergent conditions, with emergency cases accounting for approximately 40% of all colon resections. 1 Urgent indications include acute colonic pathologies, such as ischemic colitis, toxic megacolon, and perforation.2–4 Compared with elective cases, patients undergoing emergency colectomy face significantly worse outcomes, with more than fourfold increased odds of mortality and over double the risk of post-operative complications. 5
Infectious complications are a leading cause of morbidity and mortality following emergency colectomy, with sepsis, pneumonia, and surgical site infections among the most frequently reported adverse events. 6 Prior studies have identified a range of risk factors for infection in colorectal surgical procedure, including prolonged hospitalization, unplanned reoperation, and immunosuppressive therapy. 7 Other investigations focusing on specific patient populations, such as fulminant ulcerative colitis, have identified factors such as diabetes, low white blood cell counts, and intraoperative blood transfusion to increase infection risk. 8 Identifying these predictors not only facilitates earlier recognition and intervention but also informs the development of targeted perioperative strategies to reduce complications and improve patient outcomes.9–11
Although several studies have examined predictors of infectious complications following colorectal surgical procedure, evidence specifically focused on emergency cases using nationally representative data remains limited. Patient-specific and operative factors independently predicting post-operative infectious complications among patients undergoing emergency colectomy have not been well characterized, and identifying such predictors, particularly potentially modifiable factors, may inform targeted strategies to reduce infection-related morbidity and guide preventive measures in high-risk patients. In this study, we aimed to identify patient-specific and operative risk factors associated with post-operative infections after emergency colectomy. We hypothesized that patients with a higher burden of comorbidities, abnormal pre-operative laboratory values, and operative factors such as open approach, delayed surgical procedure, or prolonged operative duration would have an increased risk of developing post-operative infectious complications.
Patients and Methods
Data source and patient selection
The 2013–2017 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was used to identify patients aged 18 years or older who underwent emergency colectomy. ACS-NSQIP is a nationally validated surgical outcomes database. Emergency colectomy was identified using Current Procedural Terminology codes. All elective cases were excluded. This study was deemed exempt by our Institutional Review Board, given the use of de-identified data in ACS-NSQIP.
Patient characteristics
Variables encompassing patient demographics, comorbidities, and operative factors were analyzed. Patient demographic data included age, gender, and race. We also assessed body mass index (BMI) and comorbidities, including smoking, chronic obstructive pulmonary disease (COPD), diabetes, hypertension, functional status, congestive heart failure (CHF), ascites, dialysis dependence, disseminated cancer, chronic steroid use, significant weight loss, and the modified Frailty Index-5 factors (mFI-5). Additionally, data on pre-operative transfusion, acute kidney injury (AKI), pre-operative ventilator dependence, and American Society of Anesthesiologists (ASA) physical status classification were analyzed. Pre-operative laboratory values, including white blood cell count, hematocrit, platelet count, albumin, blood urea nitrogen (BUN), creatinine, aspartate aminotransferase, alkaline phosphatase, bilirubin, and international normalized ratio, were also incorporated. Operative factors analyzed were wound classification, surgical approach, time to surgical procedure, and operative duration. All variables were defined and reported in accordance with the specifications outlined in the ACS-NSQIP Participant Use Data File.
Outcomes
The primary outcome of the study was the rate of post-operative infectious complications, defined as the occurrence of one or more of the following within 30 days following surgical procedure: surgical site infection (SSI; superficial, deep, or organ-space), sepsis, septic shock, pneumonia, or urinary tract infection (UTI). We used a composite outcome consisting of these infectious complications on the basis of prior studies utilizing the ACS-NSQIP database. 12 Patients with missing data on these variables were excluded. We investigated pre-operative and operative factors associated with infectious complications.
Statistical analysis
Continuous variables were described as median with interquartile range (IQR), whereas categorical variables were presented using counts and percentages. Univariate analyses for continuous and categorical variables were performed with Mann–Whitney U test, and Pearson’s χ2 test, respectively. Bidirectional stepwise multivariable logistic regression was used to evaluate the association of patient demographics and comorbidities (age, BMI, smoking, COPD, diabetes, hypertension, functional status, CHF, ascites, dialysis, steroid use, bleeding disorder, pre-operative transfusion, pre-operative sepsis, ventilator dependence, laboratory abnormalities, ASA classification) and operative factors (wound classification, surgical approach, time to surgical procedure, and operative duration) with post-operative infectious complications. As a sensitivity analysis, we evaluated risk factors associated with individual infection types, including sepsis, SSI, pneumonia, and UTI. Results were reported as adjusted odds ratios (aORs) with 95% confidence intervals (CIs). Variables used to adjust the multivariable analyses were selected on the basis of clinical relevance or a p < 0.2 on the univariate analysis. The threshold for statistical significance was set at p < 0.05. All statistical analyses were performed using STATA version 18.0 (StataCorp, College Station, TX).
Results
Patient characteristics
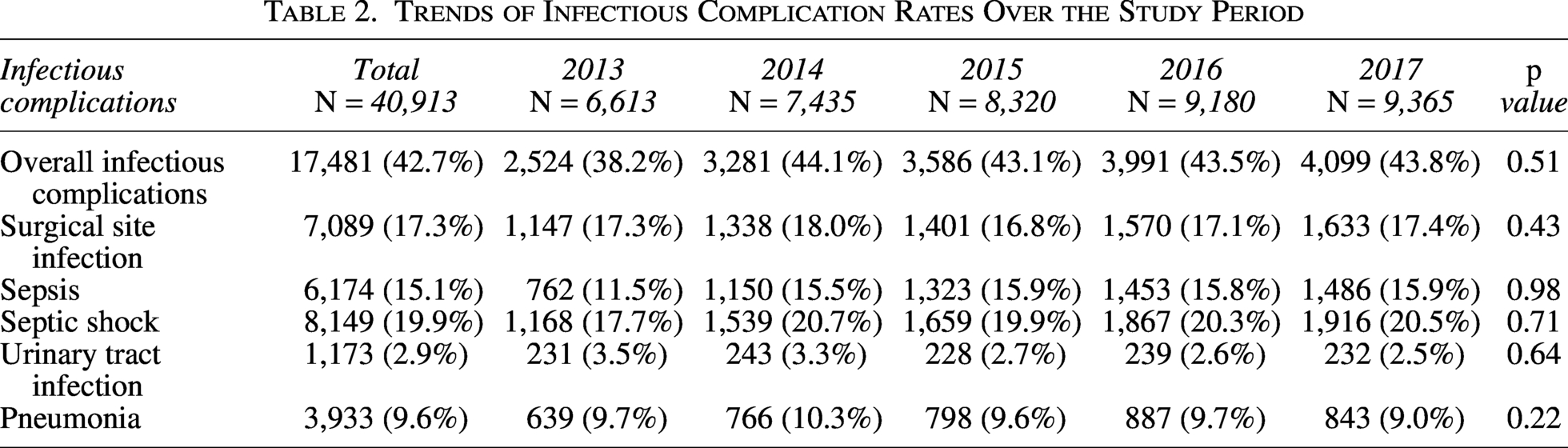
Out of 40,913 patients undergoing emergency colectomy, 17,481 (42.7%) developed post-operative infectious complications. The most common diagnoses in our cohort were bowel obstruction or perforation (43.3%), peritonitis (35.7%), and intestinal ischemia (7.7%) (Table 1). Compared with patients without infections, obesity (BMI ≥ 30) was present in 34.5% of patients with infections, compared with 26.3% of those without (p < 0.001). Several comorbidities were also more prevalent in the infection group, including smoking (23.4% vs. 19.2%), COPD (14.2% vs. 8.1%), diabetes mellitus (18.2% vs. 13.6%), and hypertension (56.1% vs. 48.9%) (p < 0.001 for all), among others (Table 1). When evaluating the rates of infectious complications, including specific infection types, over the study period, there were no significant differences in infection rates from 2013 to 2017 (Table 2).
Patient Demographics and Characteristics
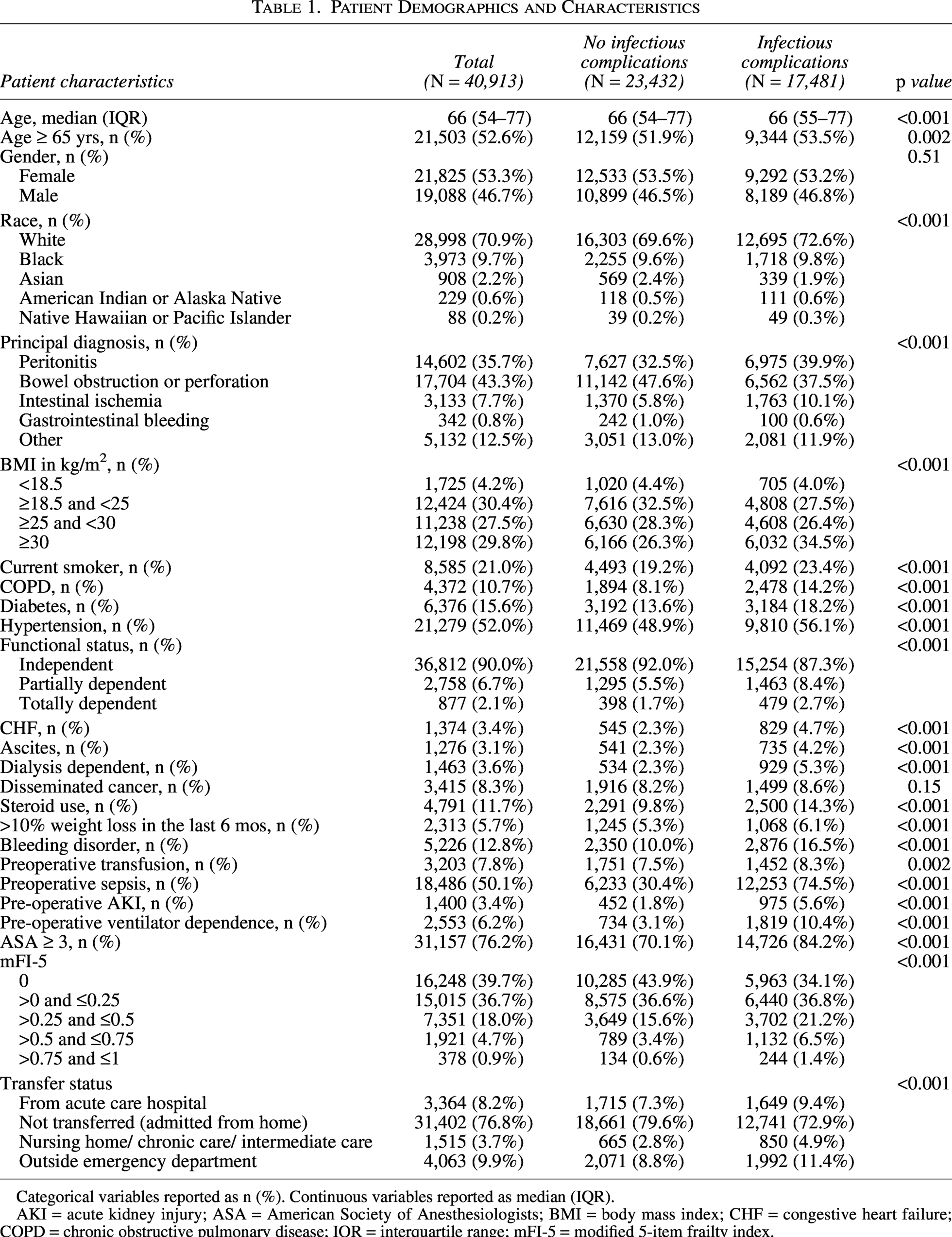
Categorical variables reported as n (%). Continuous variables reported as median (IQR).
AKI = acute kidney injury; ASA = American Society of Anesthesiologists; BMI = body mass index; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; IQR = interquartile range; mFI-5 = modified 5-item frailty index.
Trends of Infectious Complication Rates Over the Study Period
Pre-operative laboratory abnormalities were more frequently observed in the infection group. Albumin ≤3 g/dL was present in 12.1% of patients with infections compared with 17.4% of those without (p < 0.001). Elevated BUN and creatinine were also more common in the infection cohort (40.6% vs. 22.3% and 28.8% versus 13.7%, respectively; p < 0.001) (Table 3).
Preoperative Laboratory Values
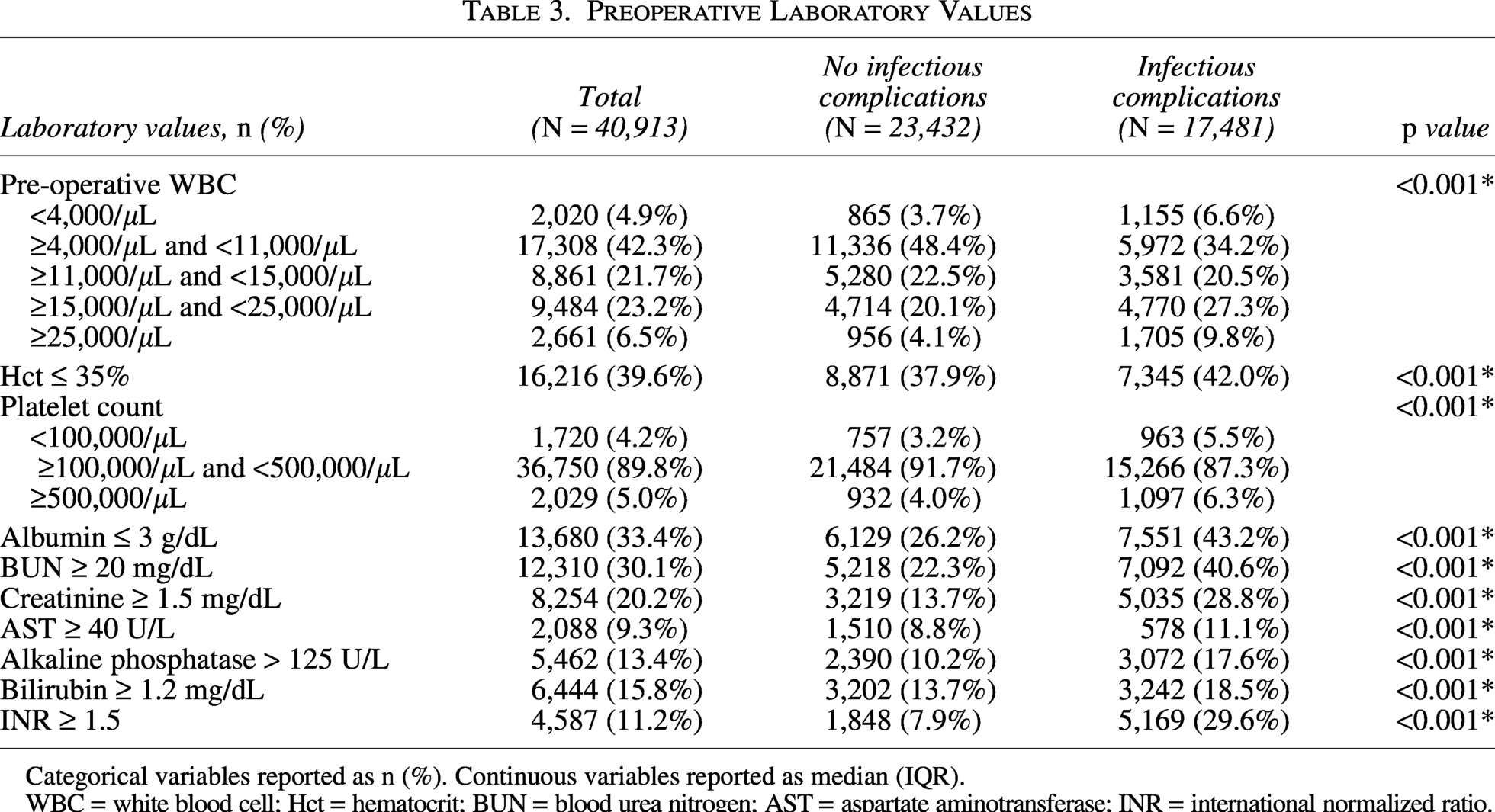
Categorical variables reported as n (%). Continuous variables reported as median (IQR).
WBC = white blood cell; Hct = hematocrit; BUN = blood urea nitrogen; AST = aspartate aminotransferase; INR = international normalized ratio.
Operative characteristics also differed between the two groups. Patients who developed infections were more likely to have a dirty wound class (67.9% vs. 39.3%, p < 0.001) and open surgical approach (91.8% vs. 81.6%, p < 0.001). Operative time exceeding 4 h was more common in the infection group (7.4% vs. 5.8%, p < 0.001), as was time to surgical procedure greater than 72 h from admission (18.1% vs. 16.1%, p < 0.001) (Table 4).
Operative Characteristics

Categorical variables reported as n (%). Continuous variables reported as median (IQR).
Predictors of infectious complications
Multivariable analyses identified several pre-operative and operative factors independently associated with increased odds of infectious complications. Among patient comorbidities, BMI ≥ 30 (aOR: 1.18, 95% CI: 1.12–1.26), COPD (aOR: 1.22, 95% CI: 1.12–1.34), bleeding disorder (aOR: 1.24, 95% CI: 1.14-1.06), ascites (aOR: 1.25, 95% CI: 1.08–1.45), current smoking (aOR: 1.11, 95% CI: 1.04–1.19), totally dependent functional status (aOR: 1.22, 95% CI: 1.01–1.47), and ASA physical status ≥ 3 (aOR: 1.33, 95% CI: 1.24–1.43) were significant contributors. Laboratory abnormalities, particularly BUN ≥ 20 mg/dL (aOR: 1.23, 95% CI: 1.15–1.33) and albumin ≤3 g/dL (aOR: 1.29, 95% CI: 1.22–1.37), were significantly associated with increased odds of post-operative infection. Among operative factors, dirty wound class (aOR: 1.40, 95% CI: 1.30–1.50), open surgical procedure compared with laparoscopic (aOR: 1.59, 95% CI: 1.46–1.73), time to surgical procedure > 24 h (aOR: 1.09, 95% CI: 1.03–1.16), and operative duration > 2 h (aOR: 1.11, 95% CI: 1.08–1.13) were significantly associated with increased risk of post-operative infectious complications (Fig. 1). On sensitivity analyses, open and delayed surgical procedure were associated with sepsis; obesity, dirty wound class, and open surgical procedure with SSI; COPD, dependent functional status, and ASA physical status ≥ 3 with pneumonia; and dependent functional status with UTI (Fig. 2).
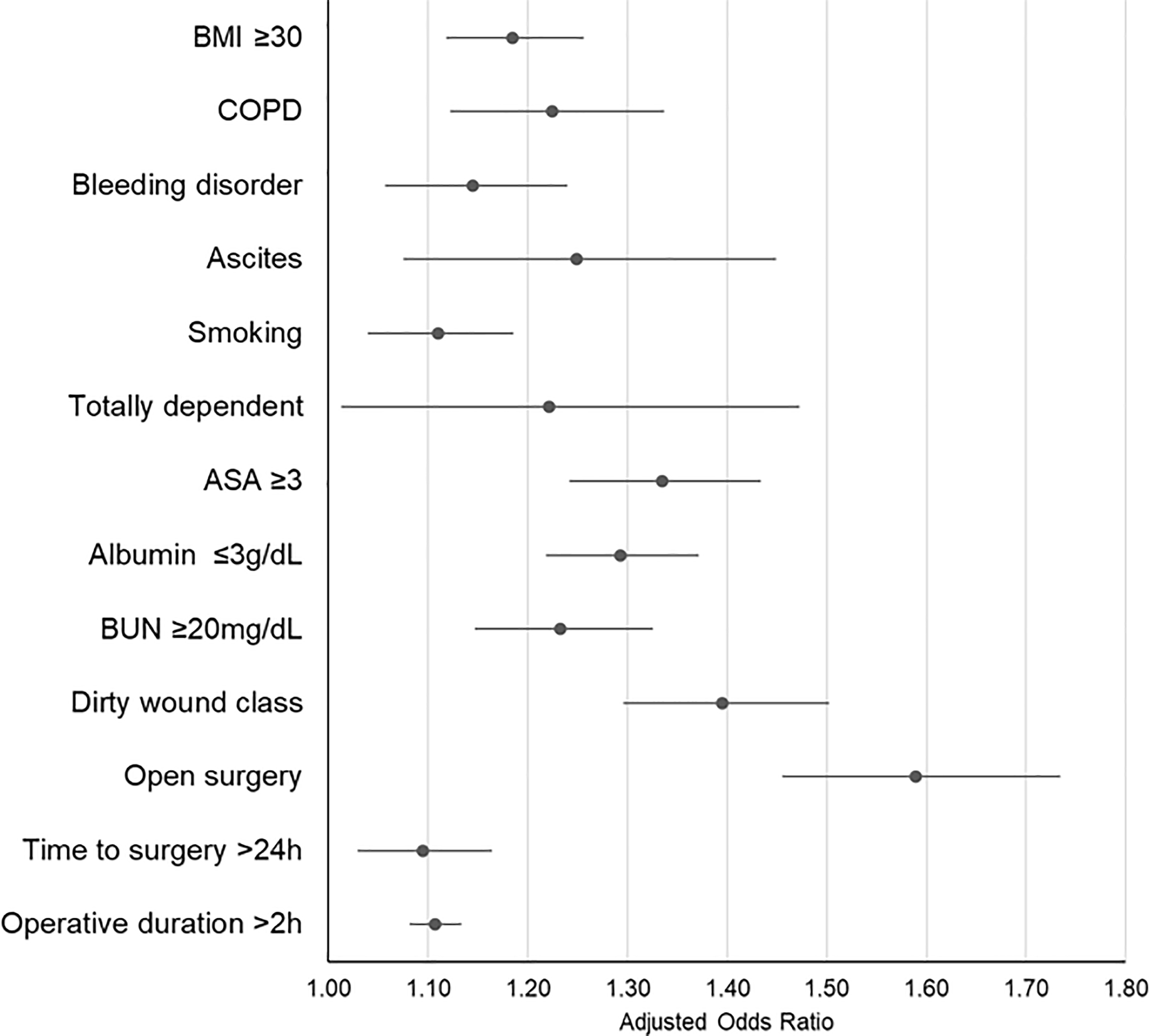
Multivariable logistic regression identifying risk factors for post-operative infectious complications.
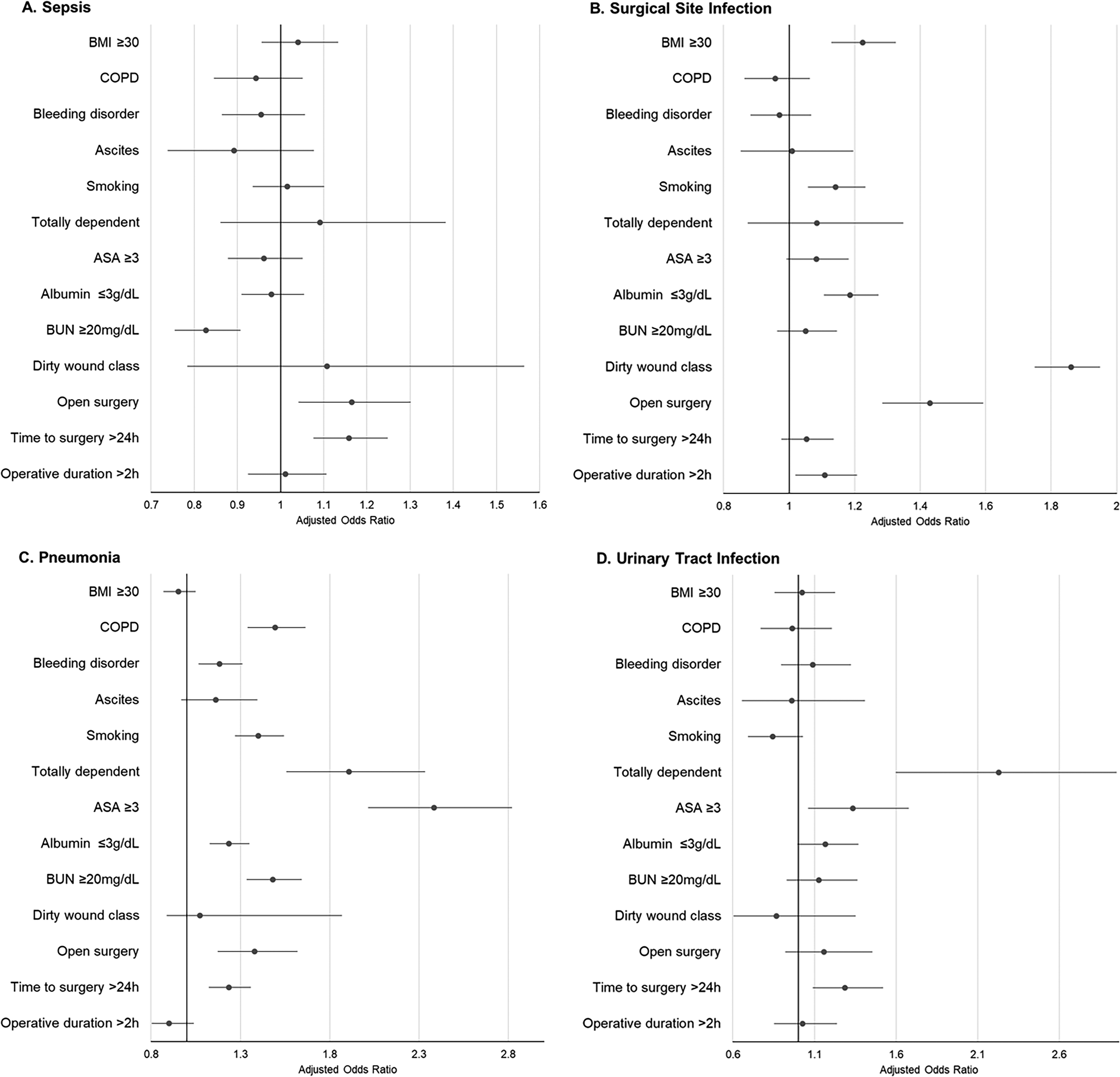
Multivariable logistic regression identifying risk factors for sepsis
Discussion
In this study, we found that over 40% of patients developed infectious complications following emergency colectomy, reinforcing the significant burden of infectious morbidity in this population. We identified a range of pre-operative factors, such as obesity, COPD, bleeding disorder, ascites, current smoking, and dependent functional status, and laboratory abnormalities, including low albumin and high BUN levels, as significant contributors to increased odds of post-operative infection. Operative factors, such as open surgical approach, delayed surgical procedure, and prolonged operative duration, were additional predictors of infectious complications.
Implementing targeted interventions in emergency surgical procedure requires the development of predictive models that reflect the acuity and complexity of such cases. Although the ACS-NSQIP surgical risk calculator has demonstrated utility in predicting post-operative mortality across various surgical populations, including emergency abdominal procedures, its performance in high-risk emergency settings remains inconsistent.12–14 The emergency surgeryscore (ESS) has been validated as an accurate post-operative mortality risk calculator specifically for Emergency General Surgery (EGS). 12 In an analysis of ACS-NSQIP data, Han et al. demonstrated that ESS can also be used to predict the risk of post-operative infectious complications and could inform pre-operative decision-making and serve as a benchmarking tool for infection rates in EGS. 12 However, there remains a paucity of procedure-specific tools to predict infection risk among patients undergoing emergency colectomy and other high-risk EGS procedures.
Identifying risk factors of infectious complications is essential to guiding targeted prevention strategies, particularly in high-risk procedures such as emergency colectomy. 15 A comprehensive approach to reduce post-operative complications involves recognizing key contributing factors and implementing interventions across the timeline of care, including pre-operative risk assessment, intraoperative decision-making, and post-operative management. This framework allows for the distinction between non-modifiable patient characteristics, such as comorbidities or functional status, and modifiable factors, such as time to surgical procedure, that can be optimized to improve clinical outcomes.16–18
In the pre-operative setting, optimizing patient status and administering appropriate prophylaxis are key strategies to reduce infection risk. In a prospective clinical trial, Clarke et al. demonstrated that the administration of short-term, low-dose pre-operative oral antibiotics significantly reduced wound infections and septic complications in patients undergoing elective colorectal surgical procedure. 19 Although mechanical bowel preparation is routinely used in elective colectomy to reduce infectious complications, its use in emergency cases is often not feasible, which has raised concerns about a potentially increased infection risk in unprepared bowels. 20 However, prospective studies in trauma settings have shown no significant association between the omission of bowel preparation and post-operative infections, suggesting limited impact in emergent contexts. 21 Additionally, addressing modifiable factors, such as glycemic control, has been shown to reduce the risk of SSI in patients undergoing gastrointestinal surgical procedure. 22
Several predictors identified in our analysis were related to operative factors, including dirty wound class, open surgical approach, delayed surgical procedure, and operative duration >2 h. Although open surgical procedure is often unavoidable in emergency settings, strict adherence to infection prevention protocols, such as the use of wound protector devices, may reduce wound contamination and infectious complications.23–25 Similarly, although operative duration is generally non-modifiable, targeted intraoperative interventions can reduce infection risk. For instance, a meta-analysis of seven observational studies found that intraoperative redosing of prophylactic antibiotics in surgeries lasting over 3 to 4 hours was associated with a 35% reduction in the risk of SSI. 26 Additionally, well-established practices, such as appropriate hair removal and avoiding perioperative hypothermia, have been shown to significantly reduce SSI risk.27,28 Our finding that delayed surgical procedure was associated with increased infection risk aligns with previous literature evaluating the impact of delay in surgical intervention on outcomes in several surgical procedures, including emergency hernia repair and appendectomy.29,30
Post-operative infection risk remains a critical consideration following emergency colectomy. Enhanced surveillance and timely intervention protocols have been shown to reduce the risk of post-operative infectious complications, particularly in patients with obesity, COPD, wound contamination, or prolonged operation.31,32 Targeted strategies, such as prophylactic negative-pressure wound therapy, have demonstrated efficacy in lowering infection-related morbidity in high-risk surgical populations. 33 Additionally, early post-operative mobilization may further reduce infection risk. For example, mobilization within 36 h in spinal fusion surgical procedure was associated with a significantly lower risk of SSI compared with delayed ambulation. 34 These findings underscore the importance of proactive, individualized post-operative care in reducing infection risk and improving patient outcomes following emergency surgical procedure.
Our study has several limitations. First, the use of retrospective ACS-NSQIP data introduces the potential for unmeasured confounding and limits our ability to establish causality. Second, hospital-level variables, such as infection control practices, perioperative protocols, and institutional volume, and important clinical factors, such as severity of illness, are not captured in the database. Third, we could not evaluate the association between several important perioperative factors, including glycemic control, temperature management, oral antibiotic use, or bowel preparation, and post-operative infectious complications, as these variables are not captured in ACS-NSQIP. Finally, the database reports outcomes only within 30 days post-operatively, potentially underestimating the true incidence of infectious complications, as prior studies have shown that many complications occur beyond this period. 35
Conclusion
Infectious complications following emergency colectomy remain a significant source of post-operative morbidity, affecting almost half of patients. Our findings highlight key pre-operative and operative predictors of infection, offering targets for interventions aimed at mitigating infection risk. Further research should focus on developing and integrating procedure-specific risk stratification tools to inform perioperative decision-making and guide targeted strategies to reduce infection-related morbidity.
Authors’ Contributions
Y.A.: Conceptualization, methodology, data curation, data analysis, literature review, writing-original draft, writing—review & editing, visualization. J.P.: Writing—original draft. J.F.J.: Writing—original draft. J.H.A.M.: Data analysis. R.B.B.: Writing—original draft. C.N.P.: Writing—review & editing. J.O.H.: Writing—review & editing. H.M.A.K.: Writing—review & editing. G.C.V.: Writing—review & editing. M.P.D.: Conceptualization, supervision, project administration, writing-review & editing.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
There was no funding available for this study.