
Abstract
Background:
Liver transplantation is a life-saving procedure for patients with end-stage liver disease. Risk of post-transplantation infection remains high despite improvement in graft and patient survival. Antibacterial and antifungal prophylaxis plays an important role in reducing infection-related morbidity and mortality, but optimal timing and regimens are not well defined.
Methods:
The Surgical Infection Society’s (SIS) Therapeutics and Guidelines Committee and individuals with content expertise convened to develop guidelines on antibacterial and antifungal prophylaxis in liver transplant to prevent surgical site infection and other infections, shorten intensive care unit length of stay, and decrease mortality. PubMed, Embase, Web of Science, and the Cochrane Database were searched using Medical Subject Heading terms including “liver transplantation,” “antibiotic prophylaxis,” and “antifungal prophylaxis” for studies limited to randomized controlled trials, systematic reviews, meta-analyses, cohort, and case–control studies in adult patients. Evaluation of the published evidence was performed using the Grading of Recommendations Assessment, Development and Evaluation system, and final recommendations were developed by an iterative process.
Results:
We cannot make a recommendation for or against using pre-operative (more than 1 h before incision) antibiotic agent prophylaxis in liver transplantation with available evidence. We suggest the use of broad-spectrum antibiotic agent prophylaxis in liver transplantation rather than gram-positive antibiotic agent prophylaxis alone (Grade 2B). We recommend limiting administration of antibiotic agent prophylaxis to 24 hours post-operatively after liver transplant (Grade 1B). We recommend against empiric antifungal prophylaxis for patients at low risk for invasive fungal infections (IFIs) after liver transplant; for patients at high risk for IFI, we recommend antifungal prophylaxis (Grade 1B).
Conclusions:
This guideline summarizes the current SIS recommendations on antibacterial and antifungal prophylaxis in liver transplantation.
Background
Liver transplantation is a life-saving procedure for patients with end-stage liver disease. In the United States, the annual number of liver transplants performed has increased to 10,659 in 2023. 1 Patient outcomes following liver transplant have also improved. In 2022, the one-year graft failure rate was 7.9% and the mortality rate was 6.5%, down from 11.6% and 10% in 2012, respectively. 1 Despite these advances, peri-operative infections remain a substantial threat to successful liver transplant outcomes, leading to sepsis, organ dysfunction, prolonged hospital stays, and mortality. Recent studies estimate that 45%–55% of liver transplant recipients develop an infection within the first year after transplant.2,3 An analysis of United Network for Organ Sharing data from 2002 to 2016 found that infections accounted for 36.4%–55.6% of early mortality after liver transplant. 4
Several factors specific to liver transplant contribute to its elevated peri-operative infectious risks among solid organ transplants. 5 Pre-transplant hepatocellular dysfunction predisposes patients to infections, such as spontaneous bacterial peritonitis, cholangitis, and catheter-related blood stream infections. 6 Prolonged operative time can lead to intra-operative hypothermia and tissue ischemia that further compromise immune defense. 7 Contamination from biliary and gastrointestinal tracts can result in surgical site infections (SSIs). 8 Patients who experience post-operative organ failure often require prolonged intubation or placement of indwelling catheters that increase the risk of nosocomial infections. 9 A particularly concerning finding is that 41%–59% of infections are caused by multi-drug-resistant organisms (MDROs) with associated high morbidity and mortality, underscoring the importance of judicious antimicrobial agent stewardship in this patient population. 10
Antimicrobial agent prophylaxis is the standard of care for many surgical procedures to minimize the microbial load in the surgical wound and prevent peri-operative infections. 11 It is also routinely used in liver transplant; however, practices vary considerably across different institutions, which highlights the need for updated guidance to reduce infection-related complications and minimize the risk of MDRO propagation. 12 To address these concerns, the Surgical Infection Society (SIS) Therapeutics and Guidelines Committee convened to develop pragmatic recommendations to further guide the optimal timing and regimen of antibacterial and antifungal prophylaxis in adult patients undergoing liver transplant.
Level of evidence: Level IV, therapeutic/care management
Objectives
Clinical Question 1: In adult patients undergoing liver transplantation, does the administration of extended pre-operative (more than 1 h before incision) antibiotic agents decrease SSI, other infections, hospital length of stay (LOS), intensive care unit (ICU) LOS, in-hospital mortality, or 30-day mortality?
Clinical Question 2: In adult patients undergoing liver transplantation, does the administration of peri-operative (incision to 23 h post-operatively) broad-spectrum antibiotic agents versus antibiotic agents with gram-positive coverage alone decrease SSI, other infections, hospital LOS, ICU LOS, in-hospital mortality, or 30-day mortality?
Clinical Question 3: In adult patients undergoing liver transplantation, does the administration of peri-operative (incision to 23 h post-operatively) antibiotic agents versus prolonged post-operative (longer than 24 h) antibiotic agents decrease SSI, other infections, hospital LOS, ICU LOS, in-hospital mortality, or 30-day mortality?
Clinical Question 4: In adult patients undergoing liver transplantation, does the administration of antifungal agents in addition to antibiotic agents versus antibiotic agents alone decrease SSI, other infections, hospital LOS, ICU LOS, in-hospital mortality, or 30-day mortality?
Methods
Methodology for this practice management guideline was based on the framework described by Arksey and O’Malley and conforms to the multi-disciplinary international Reporting Items for practice Guidelines in HealThcare (RIGHT) Working Group standards (Supplementary Data S1).13,14 The SIS Therapeutics and Guidelines Committee and individuals with content expertise convened to develop guidelines on peri-operative antibacterial and antifungal prophylaxis in liver transplantation to prevent SSI and other infections, shorten ICU LOS, and decrease mortality. A guidelines team with experience in surgical infectious diseases, liver transplantation, epidemiology, and systematic reviews was established to determine the clinical questions and study protocol. Our review consisted of five phases: establishment of clinical questions and outcomes, identification of relevant studies, study selection, data abstraction, and collation and summary of results.
On August 2, 2023, a research librarian designed and performed searches of four bibliographic databases: PubMed, Embase, Web of Science, and Cochrane Database using Medical Subject Heading terms including “liver transplantation,” “antibiotic prophylaxis,” and “antifungal prophylaxis” (Supplementary Data S2). This search was repeated on September 4, 2024, to capture recent articles not captured in the original search. Only English-language articles or articles that could be translated into English were reviewed. Studies published in the year 2003 or later were included to maximize capture of modern, relevant studies. Inclusion criteria were limited to randomized controlled trials (RCTs), systematic reviews, meta-analyses, cohort, and case–control studies in adult patients undergoing liver transplantation. Systematic reviews without relevant outcomes, commentaries, operative technique descriptions, active clinical trials, and animal studies were excluded. Conflicts of interest (COIs) and funding sources were identified for each study.
Database results were uploaded into Covidence systematic review manager, a Cochrane-sanctioned, web-based application. Upon completion of the electronic literature search, a total of 2,699 studies were screened. Of these, 83 studies were identified for potential retrieval and assessed for eligibility. After applying the exclusion criteria, 30 studies remained (Fig. 1). These included both primary studies and systematic reviews/meta-analyses. Eight of the resulting articles were systematic reviews and meta-analyses.15–22 Nine primary articles identified through our search were also included in these systematic reviews.8,23–30 Any disagreement about study inclusion was resolved by consensus with an additional reviewer. Full-text review and data abstraction were performed by five authors. Quality and certainty of published evidence were evaluated using Grading of Recommendations Assessment, Development, and Evaluation definitions using high (A), moderate (B), or weak (C) nomenclature.31,32 Strength of the recommendation was graded as strong (1) or weak (2). 33 Missing data were sought from corresponding authors. Degree of bias and certainty were reported after group consensus. Using iterative consensus, all committee members voted to accept or reject each recommendation.
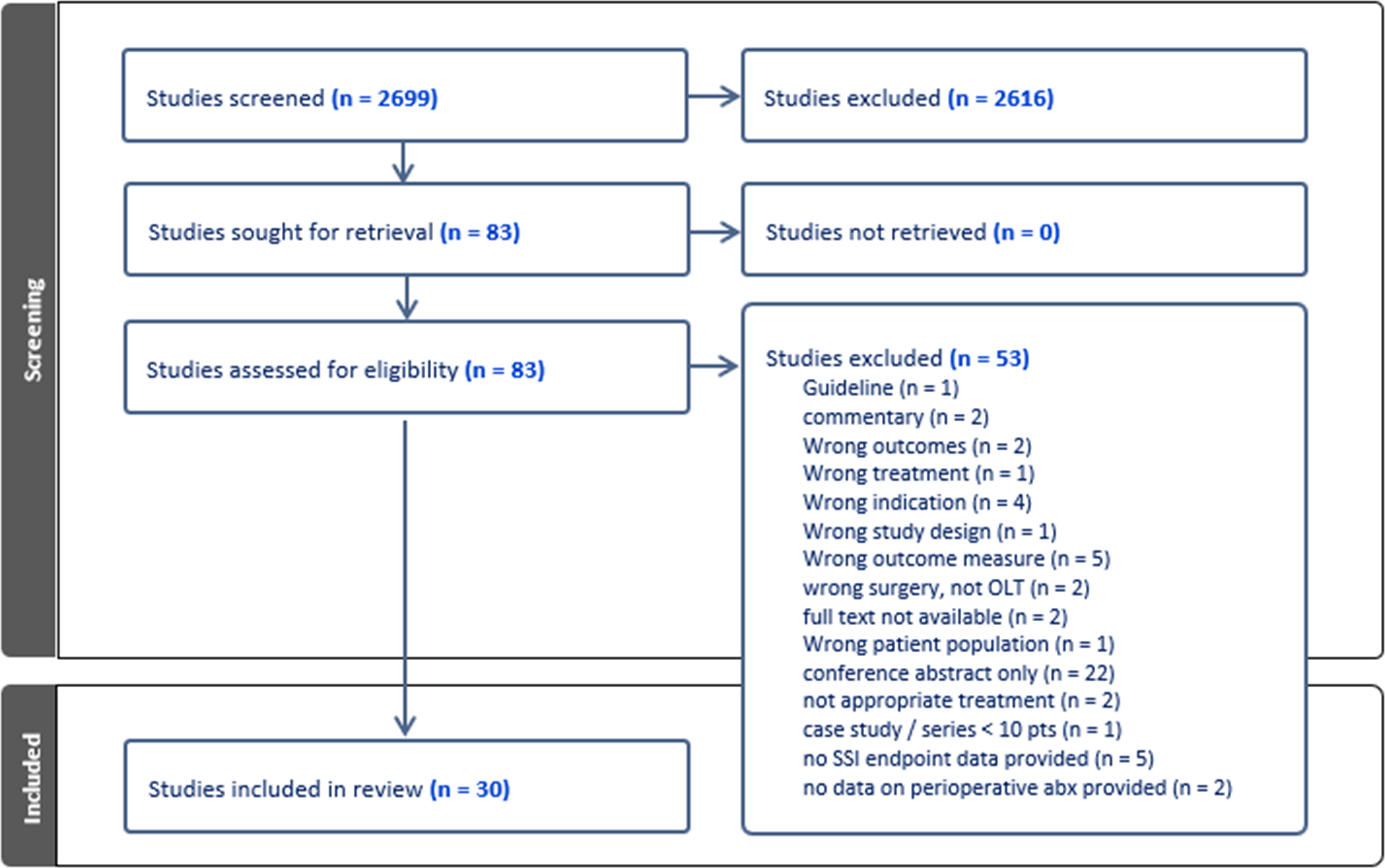
Flow diagram showing the selection process for included
The intended primary guideline users include surgeons, transplant specialists, operating room leadership, infection preventionists, hepatologists, infectious diseases physicians, and hospital administrators. The guideline is intended for inpatient settings. This study was IRB exempt as all articles were publicly available.
Results
Clinical question 1
In adult patients undergoing liver transplantation, does the administration of extended pre-operative (more than 1 h before incision) antibiotic agents decrease SSI, other infections, hospital LOS, ICU LOS, in-hospital mortality, or 30-day mortality?
Clinical question 1—qualitative synthesis
Of the 30 included studies, none addressed this clinical question. Therefore, there are not enough data to address this clinical question.
Clinical question 1—recommendation
We cannot make a recommendation for or against the use of extended pre-operative (more than 1 h before incision) antibiotic agent prophylaxis in liver transplantation with currently available evidence (Table 1).
Antimicrobial Agent Prophylaxis Recommendations in Adult Patients Undergoing Liver Transplantation
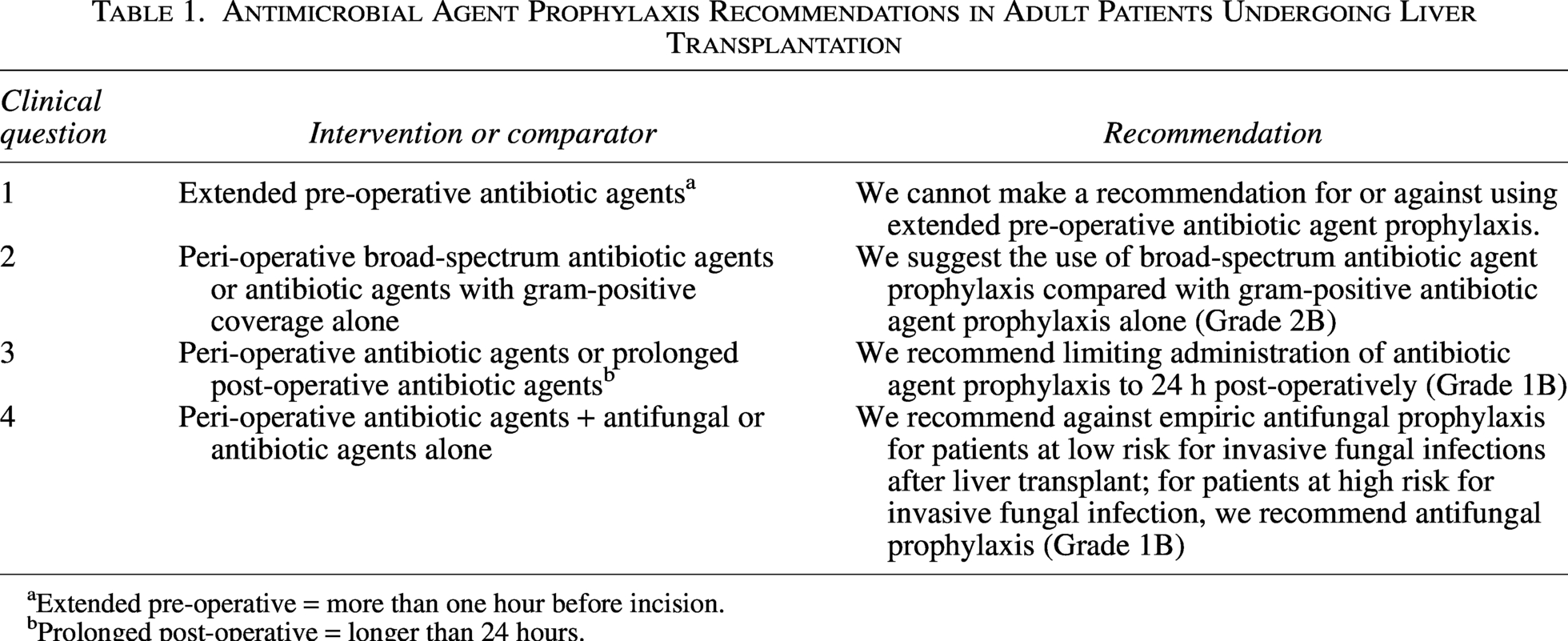
Extended pre-operative = more than one hour before incision.
Prolonged post-operative = longer than 24 hours.
Clinical question 2
In adult patients undergoing liver transplantation, does the administration of peri-operative (incision to 23 h post-operatively) broad-spectrum antibiotic agents versus antibiotic agents with gram-positive coverage alone decrease SSI, other infections, hospital LOS, ICU LOS, in-hospital mortality, or 30-day mortality?
Clinical question 2—qualitative synthesis
Of the 30 included studies, four addressed different prophylactic antibacterial regimens in liver transplant. In a single-center RCT, Shafiekhani et al. 34 compared using ampicillin-sulbactam (3 g every 6 h) plus either ceftizoxime (2 g every 8 h) or gentamicin (5 mg/kg every 24 h for two single doses) for antibiotic agent prophylaxis. Both regimens were considered broad-spectrum coverage, and neither had gram-positive-only coverage. Therefore, the objectives of the study did not fully align with the clinical question. Campos-Varela et al. 22 conducted a systematic review to identify optimal antibacterial prophylaxis to prevent post-liver transplant infections and improve outcomes. Two studies included in this systematic review compared cefazolin with broad-spectrum antibacterial prophylaxis. Garcia Prado et al. 30 prospectively compared liver transplant recipients from the same institution who received pre-operative cefazolin (1 g intravenous dose) versus amoxicillin/clavulanate (2 g intravenous dose) after the prophylactic protocol was changed in November 2005, and there was no statistically significant difference in the rate of SSI, hospital LOS, or ICU LOS. In a multi-center prospective cohort study, Asensio et al. 8 demonstrated increased risk of SSI associated with cefazolin prophylaxis alone compared with glycopeptide/aztreonam in univariate analysis (17% vs. 2%, p < 0.001), although the difference did not remain after the Child–Pugh classification and transplant center were controlled for. As a result, Campos-Varela et al. concluded in the systematic review that there was no evidence to support the effectiveness of broad-spectrum over gram-positive-only prophylactic antibiotic agents.
Clinical question 2—recommendation
We suggest the use of broad-spectrum antibiotic agent prophylaxis compared with gram-positive antibiotic agent prophylaxis alone in patients undergoing liver transplantation (Grade 2B).
Clinical question 3
In adult patients undergoing liver transplantation, does the administration of peri-operative (incision to 23 h post-operatively) antibiotic agents versus prolonged post-operative (longer than 24 h) antibiotic agents decrease SSI, other infections, hospital LOS, ICU LOS, in-hospital mortality, or 30-day mortality?
Clinical question 3—qualitative synthesis
Two unique studies directly addressed the use of peri-operative (incision to 23 h post-operatively) versus prolonged (longer than 24 h) post-operative antibiotic agent prophylaxis, with a combined population of 146 adult liver transplant recipients.27,35 They were published between 2019 and 2020. Berry et al. conducted an RCT with 102 patients, whereas Bandali et al. performed a retrospective cohort study with 44 patients. Both were single-center studies in the United States, and neither disclosed industry sponsorship.
Neither study demonstrated benefits from extending antibiotic agent prophylaxis beyond 24 h for preventing SSIs or other post-operative complications. Berry et al. randomized participants to either intra-operative-only versus extended prophylaxis (piperacillin-tazobactam 3.375 g or vancomycin 1,000 mg plus ciprofloxacin 400 mg for those with penicillin allergies). The study was designed to detect a 15% reduction in SSI with a type I error rate (
Clinical question 3—recommendation
We recommend limiting the administration of antibiotic agent prophylaxis to 24 hours post-operatively in patients undergoing liver transplant (Grade 1B).
Clinical question 4
In adult patients undergoing liver transplantation, does the administration of antifungal agents in addition to antibiotic agents versus antibiotic agents alone decrease SSI, other infections, hospital LOS, ICU LOS, in-hospital mortality, or 30-day mortality?
Clinical question 4—qualitative synthesis
Invasive fungal infections (IFIs) remain an important cause of morbidity and mortality following liver transplantation. We identified multiple studies, including RCTs that involved antifungal prophylaxis. Given the heterogeneity of the studies addressing this clinical question, the qualitative analysis is broken down by outcomes.
Surgical site infections
No studies provided data on the addition of antifungal prophylaxis on SSIs as the specific outcome.
Other infections: Superficial and IFI
For the purposes of this analysis, superficial fungal infection (SFI) and IFI are categorized as “other infections,” with explicit mention of studies reporting on these distinctions. Five of 14 studies on antifungal prophylaxis looked at the reduction in SFI or IFI as the study outcomes.
Sharpe et al. published an RCT in 2003 demonstrating a statistically significant reduction in SFI and IFI as the composite outcome using itraconazole (oral itraconazole pre-operative single dose at 5.0 mg/kg followed by post-operative twice-daily doses at 2.5 mg/kg up to 56 d or discharge) versus placebo (4% vs. 24%; p = 0.04). 26 In the subgroup analyses, there were no statistically significant reductions in SFI (0% in the itraconazole group vs. 8% in the placebo group, p = 0.141) or suspected IFI (4% in the itraconazole group vs. 16% in the placebo group, p = 0.225).
In comparison, Winston et al. 24 demonstrated reductions in both SFI and IFI with fluconazole prophylaxis (400 mg daily intravenous or oral doses initiated pre-operatively on the day of operation until 10 wks after liver transplantation). SFI reduced from 28% in the placebo group to 4% in the fluconazole group (p < 0.001) and a reduction in IFIs from 23% to 6% (p < 0.001). Of note, there was a substantially reduced overall fungal colonization from 70% to 28% in the fluconazole group compared with an increase from 60% to 90% in the placebo group (p < 0.001).
Biancofiore et al. 23 conducted a randomized placebo-controlled study comparing intravenous amphotericin B (1 mg/kg daily for 7 d) plus oral itraconazole (200 mg daily for 3 wks), intravenous fluconazole (400 mg daily for 7 d) plus oral itraconazole (200 mg daily for 3 wks), or intravenous and oral placebo in prevention of IFIs. Although the incidence of mycotic colonization was substantially higher in the placebo group compared with treatment groups (p < 0.01), there was no statistically significant difference in the incidence of IFIs between the three groups (7% in the amphotericin group, 9% in the fluconazole group, and 9% in the placebo group; p > 0.05). The authors concluded that routine antifungal prophylaxis for all liver transplant recipients did not appear justified, despite the reduction in fungal colonization observed with prophylactic treatment.
Eschenauer et al. 28 published a retrospective review of two historical cohorts before and after the institution revised antifungal prophylaxis from a universal approach (oral voriconazole 200 mg twice daily for 30 d for all patients) to a targeted approach after patients were risk-stratified into three categories. The first category was patients who had undergone re-transplantation, renal failure requiring renal replacement therapy, fulminant liver failure as the indication for liver transplant, intra-abdominal or intra-thoracic re-exploration within the first month after liver transplant received oral voriconazole 200 mg twice daily for 30 days; the second category was patients with choledochojejunostomy, both prolonged operative time (>11 h) and requiring substantial amount of blood products (>40 units), Candida colonization or infection within three months before liver transplant, living donor transplantation or post-transplant bile leak, and received oral fluconazole 400 mg daily for the duration of ICU stay. The last category was low-risk patients, defined as those who had none of the above risk factors and therefore received no antifungal prophylaxis. The overall incidence of IFIs was 4% in the universal cohort and 7% in the targeted cohort, but the difference was not statistically significant (p = 0.34). The authors did not identify the high model for end-stage liver disease (MELD) score as a risk factor for IFIs. Patients with MELD ≥30 had an IFI rate of 3.4%, and there was no significant difference between the targeted and universal groups. The study also compared low-risk patients who only received antibiotic agents and high-risk patients who received antibiotic agents with antifungal prophylaxis in the targeted cohort. The incidence of IFIs in low-risk patients was 4%, comparable with 6% in high-risk patients who received antifungal prophylaxis with antibiotic agents, without statistical significance (p = 1.0). This study was limited in that it did not compare universal antifungal prophylaxis with universal antibiotic agents alone, and therefore did not directly address our clinical question. Its findings did suggest that antifungal prophylaxis might not be necessary for low-risk patients, as their IFI rates were similar to those of high-risk patients who received prophylaxis.
San-Juan et al. 29 published a retrospective cohort study that looked at low-risk liver transplant recipients, finding no statistically significant difference in IFI incidence between patients receiving fluconazole prophylaxis (100–200 mg daily until discharge or for a minimum of 7 d) and those who did not (1% vs. 2%; p = 0.36).
Length of stay
The impact of antifungal prophylaxis on hospital and ICU LOS appeared to be limited, with most studies reporting no significant differences between the prophylaxis and placebo groups. Sharpe et al. 26 found no significant difference in ICU LOS (28 ± 32 d for the itraconazole group vs. 24 ± 19 d for the placebo group) or hospital LOS (61 ± 24 d vs. 68 ± 30 d). Similarly, Biancofiore et al. 23 reported no significant differences in ICU LOS between the antifungal prophylaxis groups and placebo (approximately 4 d in both groups; p > 0.05).
Mortality
None of the studies reported a statistically significant difference in in-hospital or 30-day mortality.
Clinical question 4—recommendation
We recommend against empiric antifungal prophylaxis for patients at low risk for IFIs after liver transplant; for patients at high risk for IFI, we recommend antifungal prophylaxis (Grade 1B).
Discussion
Using the guidelines in clinical practice
The global increase of infectious complications from MDROs makes it imperative to implement guideline-directed practice in antibacterial and antifungal prophylaxis. Liver transplant recipients are especially vulnerable to MDROs because of frequent healthcare exposures, prolonged hospitalizations, immunosuppression, and operative complexity. 38 MDRO infections correlate with high graft loss and increased short- and long-term mortality.38,39 Updated, stewardship-focused guidelines are essential to optimize peri-operative management, mitigate MDRO impact, and improve post-transplant outcomes. 40
This guideline development aimed to address clinical questions centering on timing and spectrum of prophylactic antibacterial and antifungal coverage in liver transplant to minimize infectious complications and optimize post-transplant outcomes. In line with the guidelines published jointly by ASHP/IDSA/SIS/SHEA in 2013 and those published by the American Society of Transplantation (AST) ID Community of Practice in 2019, we continue to recommend limiting the duration of post-operative antibacterial prophylaxis to up to 24 hours. The updated literature did not demonstrate the benefits of extending antibacterial prophylaxis beyond 24 hours in reducing post-operative infections, mortality, and in-hospital and ICU LOS. Our recommendation also accounts for the potential harms of extended antibiotic agent exposure. A recent study published after our literature search found that prolonged post-transplant antibiotic agent therapy may increase antibiotic agent resistance. 41 Although the studies included in our search were underpowered to detect a difference in CDI rates between the 24-hour and extended antibiotic agent prophylaxis groups, extended antibiotic agent exposure is a known risk factor for post-transplant CDI that can worsen liver transplant outcomes. 37 Regarding the use of pre-operative (more than 1 h before incision) antibacterial prophylaxis in liver transplant without pre-transplant infections, there is no current evidence for or against this clinical practice. Regarding the spectrum of antibiotic agent coverage, although the available evidence comparing broad-spectrum antibiotic agents versus antibiotic agents with gram-positive coverage alone shows largely equivocal outcomes, the Committee reached consensus in favor of broad-spectrum coverage. The decision was based on risk–benefit considerations specific to liver transplantation, given that gram-negative organisms (including Enterobacteriaceae, Acinetobacter, and Pseudomonas) account for a substantial proportion of post-liver transplant infections. However, the selection of prophylactic antibiotic agents should ultimately take into consideration individual liver transplant recipients’ risks and locoregional epidemiology of antibiotic agent resistance.
Regarding antifungal prophylaxis in liver transplant, we reviewed the currently available literature and agree with the ASHP/IDSA/SIS/SHEA and AST ID Community of Practice in the recommendation of adding antifungal coverage for patients at high risk for fungal infection, whereas avoiding antifungal prophylaxis in low-risk patients. Although the specific high-risk factors are not uniformly defined, renal failure requiring renal replacement therapy, re-operation, prolonged operative time, and excessive blood loss is cited in multiple studies as increasing this risk.28,42 Future investigations are needed to further risk stratify liver transplant recipients and delineate pre-transplant criteria for antifungal prophylaxis.
A high MELD score is recognized as an independent risk factor for post-transplant infections.43,44 Cirrhosis-associated immune dysfunction, characterized by systemic inflammation and immune dysfunction that compromise host defense against infections, is more prevalent in advanced cirrhosis with decompensation or organ failure. 45 To further compound infectious risks, patients with high MELD scores often receive broad-spectrum antibiotic agent therapy for bacterial infection, which is associated with bacterial and fungal dysbiosis that increases risks of IFI and MDRO infection.43,44 These considerations suggest that antimicrobial agent prophylaxis could be tailored to MELD-based risk stratification; however, there is still a knowledge gap on how this can be achieved. In the 2015 study by Eschenauer et al., 28 patients with MELD ≥30 did not have higher post-transplant IFI rate, although they were not uniformly assigned to the targeted prophylaxis group. A single-center study evaluation of carbapenem-based prophylaxis instead of cephalosporins or piperacillin-tazobactam among patients with MELD ≥30 did not demonstrate superiority in reducing infectious complications or improving survival. 46 These studies were not designed to evaluate antimicrobial agent prophylactic strategies based on cirrhosis severity, highlighting the need for future MELD-tiered trials.
Patients requiring early re-operation or staged abdominal closure following liver transplant warrant specific consideration in peri-operative antimicrobial agent prophylaxis, given their heightened risks of post-transplant infections and distinct antimicrobial agent redosing schedule between each intervention. 47 However, none of the studies reviewed for this guideline conducted subgroup analyses for this patient population, precluding evidence-based recommendations. Future studies should specifically address the antimicrobial agent prophylactic strategies for patients undergoing early re-interventions following liver transplant.
There are several limitations to the development of these guidelines. First, the number of studies identified pertinent to the clinical questions remained small. Despite the increase in liver transplant volume in the past decade, there has not been a proportionate increase in clinical trials examining antibacterial and antifungal prophylaxis. This is particularly relevant to antifungal prophylaxis, where there is a paucity of data evaluating the efficacy of newer antifungal agents. Second, certain clinical outcomes reported in the identified studies did not fully align with the specific clinical questions. For example, the time frame of post-liver transplant mortality was sometimes omitted, and specifically, in-hospital or 30-day mortality was not reported in several studies. Third, due to the heterogeneity of interventions and outcome measures in the studies, it was not possible to generate aggregate data for meta-analysis. Using systematic reviews and their foundational studies with concordant conclusions could potentially result in additive bias. Specifically on the outcome of antifungal prophylaxis, there was variability in how studies distinguished between SFIs and IFIs. Most of the studies also did not identify whether the fungal infections were SSIs. Fourth, there was no available literature to conduct cost-effectiveness analysis of different antibacterial and antifungal prophylactic strategies. Fifth, as liver transplant and the peri-operative care are inherently complex, factors other than antibacterial and antifungal prophylaxis contributing to the clinical outcomes of interest could not be comprehensively accounted for. LOS is increasingly recognized as a process metric, rather than an outcome metric due to challenges in short- and long-term rehabilitation placement, particularly among solid organ transplant recipients. Last, the identified studies did not contain granularity for us to make recommendations based on the specific etiology for liver transplant or differentiate between deceased-donor versus living-donor liver transplant, MELD score, or extended-criteria allografts. Recommendations for antibacterial and antifungal prophylaxis for high-risk liver transplant recipients including those with fulminant liver failure, re-transplants for primary non-functioning grafts, and re-transplants in the event of an infected graft are outside the scope of these guidelines. With the continuing evolution of donor and recipient selection criteria, organ preservation and surgical techniques, as well as immunosuppression regimens, our guidelines can continue to be further updated to reflect recommendations based on the contemporary standard of care in liver transplant.
Conclusions
The updated SIS guidelines on antibacterial and antifungal prophylaxis in liver transplant continue to recommend limiting the duration of post-operative antibacterial prophylaxis to 24 hours or less, recommend adding antifungal coverage for patients at high risk of IFI but abstaining from antifungal prophylaxis for patients at low risk for fungal infection, and recommend using broad-spectrum coverage compared with gram-positive coverage alone. Future studies, ideally multi-center, should focus on the spectrum of prophylactic antibiotic agent and antifungal coverage and risk stratification of liver transplant recipients to allow optimal selection of antibacterial and antifungal agents and improve liver transplant outcomes.
Authors’ Contributions
S.W. and S.-M.B.: Data abstraction, data analysis, article preparation, and critical review. H.B., W.C.C., J.M.H., A.R.J., and D.K.O.: Data abstraction, data analysis, and critical review. J.D.F.: Project conception, data abstraction, data analysis, article preparation, and critical review.
Footnotes
Acknowledgment
The authors thank Chris Stave for his assistance in performing the literature search.
Author Disclosure Statement
No COIs were reported for any author for this work product. J.D.F.: Unrestricted research funding from Varian and Pacira for an investigator-initiated trial; funding from Eclipse Regenesis for industry-sponsored clinical trial; consultant, stock, patent—Costa Surgical, Inc and received author royalties from Merck and UpToDate.
Funding Information
No funding was received for this work product.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.