
Abstract
Background:
Postoperative abdominopelvic abscesses are primarily managed with antimicrobial therapy and percutaneous drainage. A subset of abscesses is unamenable to drainage due to small size or technical inaccessibility and is therefore managed conservatively with antimicrobial therapy alone. Clinical outcomes and factors of treatment failure with antimicrobial therapy alone for postoperative non-drainable abscesses remain poorly defined.
Methods:
A retrospective cohort study included adult surgical patients at a tertiary hospital with abdominopelvic abscesses diagnosed within 30 days postoperatively and deemed non-drainable. All patients received systemic antimicrobials and were followed for 60 days. The primary outcome was therapy success. Other outcomes included clinical response, rehospitalization, and exploration of risk factors for antimicrobial therapy failure.
Results:
The study included 69 patients. Abscesses were considered non-drainable because of inaccessible location (n = 47, 68.1%) or small size (n = 22, 31.9%). The median duration of antimicrobial therapy was 18 days, including 12 days of inpatient treatment. At 60 days from antimicrobials initiation, 53 patients (76.8%) achieved therapy success. The median time to clinical response was 8 days. Among patients with follow-up imaging, most demonstrated abscess resolution or reduction in size. Independent predictors of treatment failure were pelvic abscess location (odds ratio [OR], 6.8; 95% confidence interval [CI], 1.5–30.3) and postoperative corticosteroid exposure (OR, 11.9; 95% CI: 1.1–129.7). A longer interval between procedure and abscess diagnosis was inversely associated with failure (OR, 0.8 per day; 95% CI, 0.7–0.9).
Conclusion:
When postoperative abdominopelvic abscesses are deemed not amenable to drainage, antimicrobial therapy with close clinical follow-up was associated with favorable outcomes.
Keywords
Introduction
Postoperative deep and subcutaneous collections are common radiologic findings following an abdominopelvic surgery.1,2 Loculated fluid accumulations, such as seromas, lymphoceles, hematomas, or biliomas, are reported in up to 64% of patients undergoing an abdominopelvic surgery. 2 While many of these collections resolve spontaneously, a considerable proportion become infected and progress to abscess formation, typically presenting with fever, localized pain, or ileus.1,3 Once an abscess develops, serious complications may ensue, including progression to diffuse peritonitis with an associated increased risk of mortality.3,4 Abscess formation may also adversely affect the treatment course in certain surgical populations, such as delaying the initiation of adjuvant chemotherapy in cancer patients or interrupting immunosuppressive therapy in solid organ transplant recipients.5,6
The standard management of postoperative abscesses involves both antimicrobial agent therapy and source control, preferably via percutaneous radiologically guided drainage.7–9 Current guidelines for the management of intra-abdominal infections (IAIs) largely assume that effective source control is achievable. However, a subset of postoperative abscesses is not amenable to drainage because of their small size, deep location, or proximity to critical structures, making percutaneous drainage technically challenging or risky.10,11 At the same time, these abscesses are not causing severe physiological derangement necessitating immediate reoperation. Despite their clinical relevance, evidence-based guidance to manage postoperative non-drainable abscesses is lacking.
Given the postoperative onset and the difficulty obtaining abscess samples for culture and sensitivity testing, empirical antimicrobial therapy with close follow-up is commonly used to manage postoperative non-drainable abscesses. Antibacterial regimens with activity against gram-negative aerobic and facultative bacilli, enterococci, and anaerobic bacteria are commonly used to manage these abscesses.3,7,10 However, this treatment approach is largely based on clinical pragmatism rather than robust data, as patients without achievable source control were excluded from clinical trials. 12 The expected clinical course, treatment success, and risk of failure of antimicrobial therapy for postoperative non-drainable abscesses remain poorly characterized.
Therefore, we aim to assess the clinical outcomes of antimicrobial therapy for postoperative non-drainable abdominopelvic abscesses and explore the factors associated with treatment failure.
Methods
Study design and setting
A retrospective cohort study was conducted at King Faisal Specialist Hospital and Research Center-Riyadh, an over 1,500-bed tertiary care academic medical center and the principal national referral hospital in Saudi Arabia. The study was approved by the Office of Research Affairs (RAC#2251133) and received a waiver of informed consent owing to its retrospective design.
All patients with computed tomography (CT)-confirmed post-operative abdominopelvic collections within 30 days of an abdominopelvic surgery between March 2021 and October 2025 were screened for eligibility. 13 Collections were required to be classified as non-drainable, either because of small size (maximum diameter <4 cm) 14 or because they were located in a technically inaccessible site or adjacent to organs where drainage poses a high risk of injury, as documented by a consultant radiologist.
Inclusion and exclusion criteria
Eligible patients were required to meet a composite definition of abdominopelvic abscess to reduce the risk of misclassifying non-infected collections as abscesses. This required the presence of (1) at least one clinical marker of infection (ileus, localized abdominal pain attributable to infection, or fever >38.0°C); and (2) at least one laboratory marker of infection, including leukocytosis (white blood cell [WBC] count >11 × 109/L), elevated serum procalcitonin level (>0.5 ng/mL), or a C-reactive protein (CRP) level >100 mg/L demonstrating a secondary increase after an initial post-operative decline; or (3) radiologic evidence of an abscess on CT imaging (presence of rim enhancement, surrounding fat stranding, thick internal content, or gas).1,15,16 In addition, all included patients received systemic antimicrobial therapy specifically initiated for the abscess, based on the documented clinical assessment of the treating physician. Patients with intra-operative drains were permitted if the drains were distant from the abscess.
Exclusion criteria included receipt of antibiotics for <48 hours, an abdominopelvic procedure involving placement of a foreign body, a diagnosis of abscess during antimicrobial treatment for another type of infection, and pregnancy.
Data
Data were gathered from the institutional electronic medical records. Baseline characteristics included demographics and comorbidities, with calculation of the Charlson Comorbidity Index. Relevant preoperative variables and index surgery details were recorded, along with the postoperative course data, including admission to the intensive care unit (ICU), sequential organ failure assessment scores, and systemic corticosteroid therapy.
Results of surveillance screening for multidrug-resistant organism (MDRO) genes performed at hospital or ICU admission using rectal or nasal swabs were recorded. Other microbiologic data included cultures obtained intraoperatively, from surgical drains, or from blood on the day of operation until the diagnosis of the abscess.
For antibiotic therapy, the timing of initiation and completion, as well as the need for outpatient administration, was recorded. Initial antibiotic regimens were categorized as carbapenem-based, non-carbapenem β-lactam-based, tigecycline-based, and fluoroquinolone-based. Regimens were evaluated for guideline-supported expected coverage for organisms implicated in postoperative abdominal infections. 7 An antimicrobial regimen was considered inappropriate if it was known to lack activity against microbes isolated from intra-operative surgically placed drain cultures or identified from surveillance screening of MDRO genes. The use of systemic antifungal agents was also recorded.
Abscess-related parameters included date of diagnostic imaging, number of abscesses, anatomic location, composition (based on CT imaging characteristics and description by a radiologist), maximum diameter (cm), and calculated volume (mL) derived from the product of three dimensions. Abscesses were categorized into five anatomic groups: upper abdomen, pelvic, retroperitoneal, intermesenteric, and subcutaneous.
Patients were followed for 60 days from antimicrobial initiation, with documentation of emergency visits and hospital readmissions, while assessing fever, abdominal pain, and laboratory markers of infection. Follow-up radiologic imaging findings were recorded when available within three months of antimicrobial therapy initiation.
Outcomes
The primary outcome was antimicrobial agent success at 60 days after treatment initiation for abdominopelvic abscess. Antimicrobial success was defined as a sustained clinical response at 60 days after antimicrobial initiation, with radiologic improvement (decreased abscess size or resolution) if present and the absence of predefined treatment failure events. Treatment failure was determined by the occurrence of any of the following events within 60 days of antimicrobial therapy initiation: (1) Death attributed to disseminated intra-abdominal abscess, (2) undergoing source-control intervention for the abscess (percutaneous drainage or reoperation) for no response to antimicrobial therapy, (3) reinitiation of abscess-directed antibiotics after discontinuation for more than 72 hours for relapse, (4) or radiologic persistence or progression (CT scan or ultrasound) of the abscess necessitating continuation of therapy.
Secondary endpoints included time to clinical response, defined as the day on which fever resolved, WBC count was <11 × 109/L, and CRP was reduced by 50% from its peak level. Additional outcomes included a return to the emergency department or hospital readmission within 60 days of initiation of antimicrobial therapy and the need to change the initial antimicrobial regimen because of non-response. Identification of risk factors associated with failure of antimicrobial treatment was also assessed as a secondary endpoint.
Statistical analysis
Descriptive statistics were used to summarize baseline characteristics and outcomes. Continuous variables were reported as means with standard deviations (SD) or medians with interquartile ranges (IQRs), depending on their distribution. Categorical variables were summarized as frequencies and percentages.
Uni-variable logistic regression was performed to identify potential risk factors for antimicrobial agent treatment failure, and results were presented as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Baseline predictors of failure with a p-value <0.1 in the univariable analysis and considered clinically relevant were entered into a multivariable logistic regression analysis. Given the limited sample size, these analyses were considered exploratory and hypothesis-generating.
Time to achieve clinical response was analyzed using Kaplan–Meier survival analysis, and the median time to clinical response, along with 95% CI, was reported. Patients who did not achieve success during the follow-up period were censored at their last observation.
All analyses were conducted using IBM SPSS Statistics (IBM Corp., 2017; IBM SPSS Statistics for Windows, Version 25.0, Armonk, NY), and a two-sided p-value <0.05 was considered statistically significant.
Results
Of 196 patients with postoperative non-drainable abdominopelvic collections identified during the study period, 69 were included in the final analysis. Eighty-four did not meet the infection criteria for inclusion. The remaining patients were excluded because of a diagnosis of abscess, while receiving treatment for another postoperative infection (n = 20), receipt of antimicrobial therapy <48 hours (n = 16), presence of surgical mesh (n = 6), or pregnancy (n = 1).
More than two-thirds of patients had malignant disease, and five (7.2%) patients were older than 70 years. The demographics and clinical characteristics are summarized in Table 1. The most frequent operation was a colorectal surgery (n = 19, 27.5%), including two pelvic exenterations (Table 2). Among solid organ transplant recipients, seven (10.1%) underwent liver transplantation, one (1.4%) had a kidney transplantation, and 1 (1.4%) and intestinal transplantation. Thirteen patients (18.8%) underwent a cytoreductive procedure, including nine who received concomitant hyperthermic intra-peritoneal chemotherapy (HIPEC).
Baseline Demographic and Clinical Characteristics of Patients with Postoperative Non-Drainable Abdominopelvic Abscesses
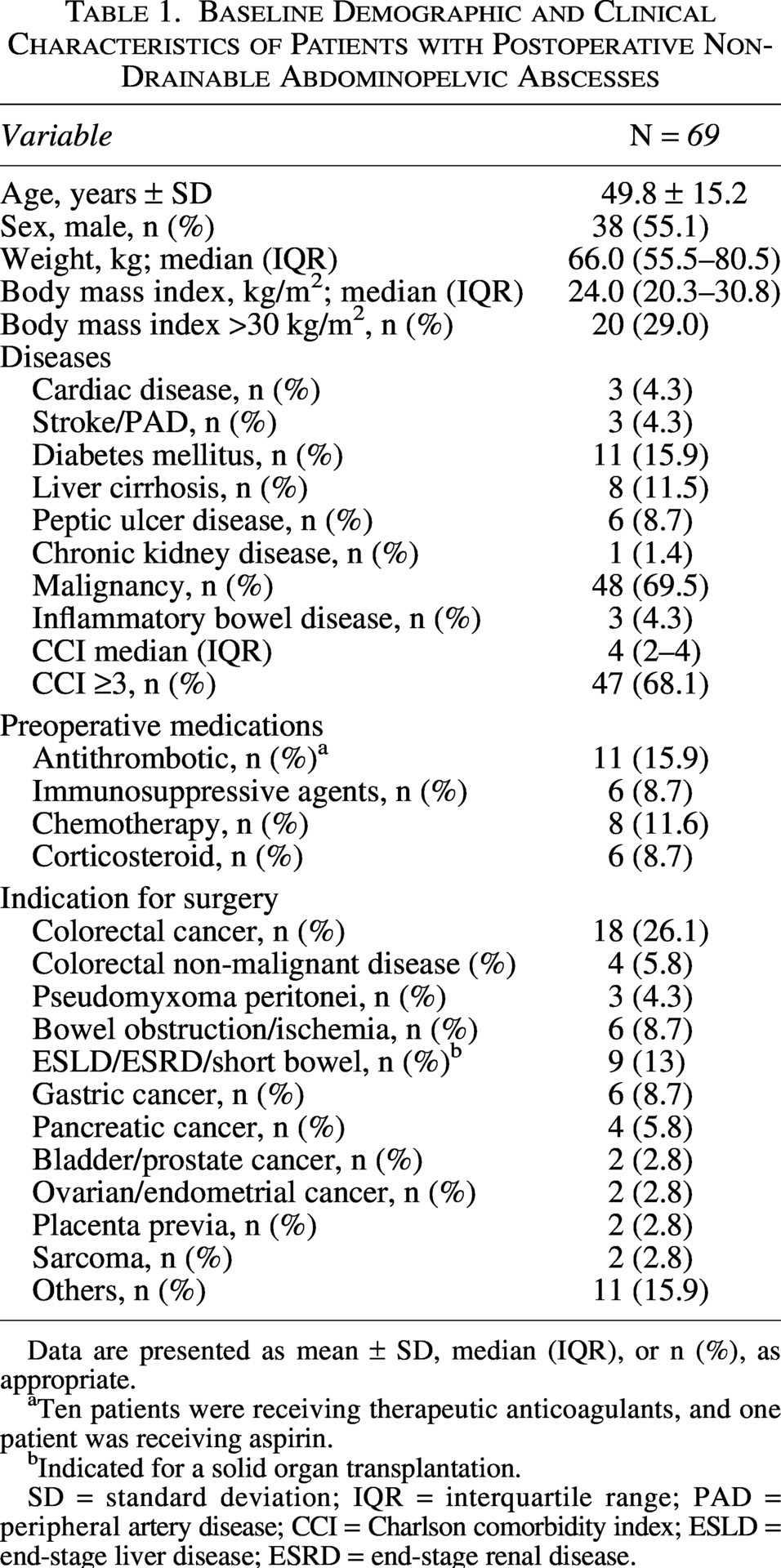
Data are presented as mean ± SD, median (IQR), or n (%), as appropriate.
Ten patients were receiving therapeutic anticoagulants, and one patient was receiving aspirin.
Indicated for a solid organ transplantation.
SD = standard deviation; IQR = interquartile range; PAD = peripheral artery disease; CCI = Charlson comorbidity index; ESLD = end-stage liver disease; ESRD = end-stage renal disease.
Operative and Postoperative Characteristics of Patients Developing Abdominopelvic Abscess
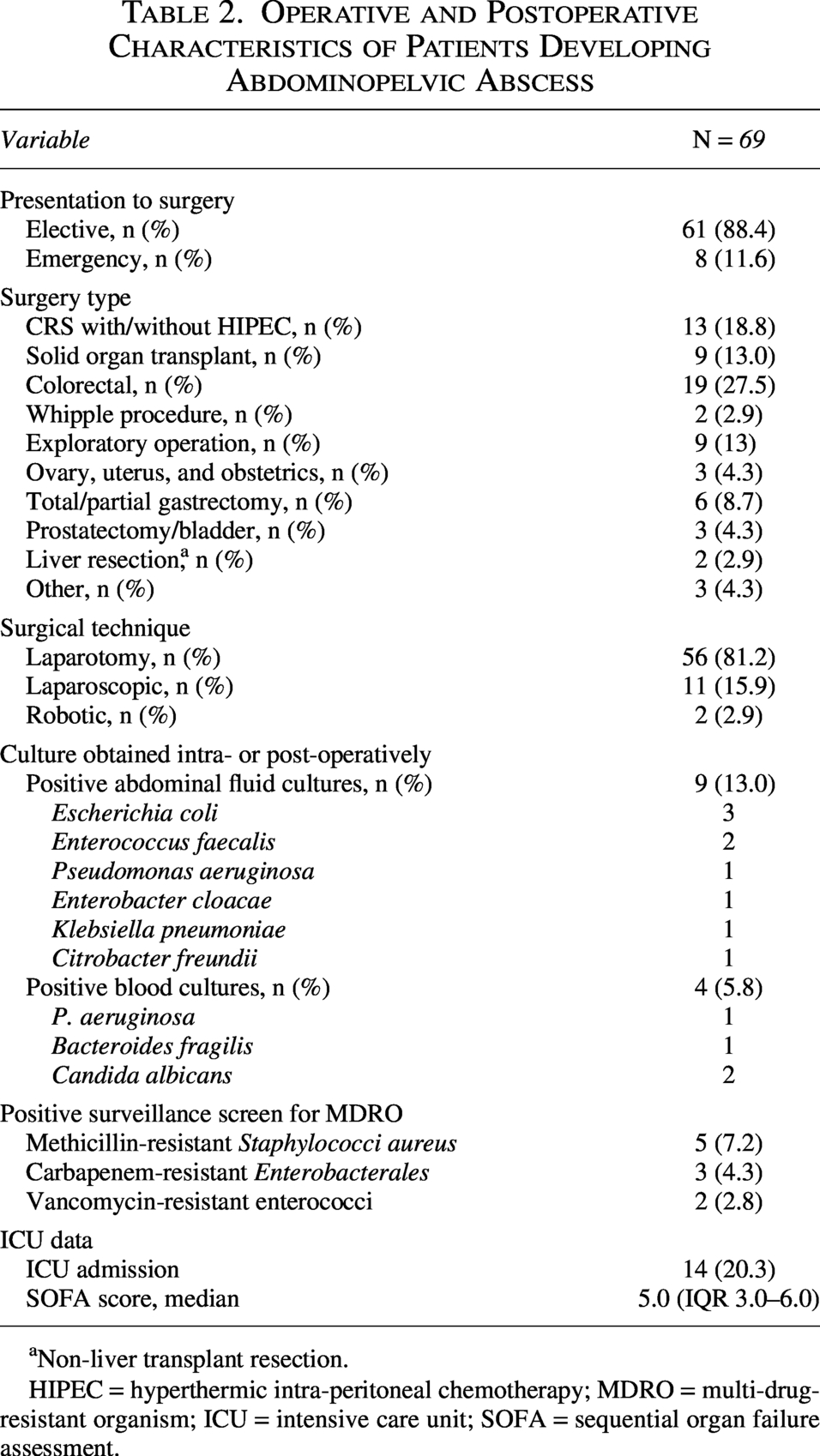
Non-liver transplant resection.
HIPEC = hyperthermic intra-peritoneal chemotherapy; MDRO = multi-drug-resistant organism; ICU = intensive care unit; SOFA = sequential organ failure assessment.
Rectal or nasal surveillance swabs for MDRO gene screening were performed in 52 (75.3%) patients, of whom 42 tested negative. Results for 10 positive cases are shown in Table 2. Among the abdominal fluid microbial cultures, one carbapenem-resistant Citrobacter freundii and one carbapenem-resistant Klebsiella pneumoniae were isolated. Escherichia coli was the most frequently isolated organism from these abdominal fluids.
Most patients had a single abscess (52.2%), with a median of 1 abscess per patient (IQR: 1–2). All abscesses demonstrated rim enhancement. Characteristics of abscesses and antimicrobial regimens are presented in Table 3. Abscesses were classified as non-drainable because of inaccessible anatomic locations in 47 patients (68.1%) or small size in 22 patients (31.9%). The initial antimicrobial regimens used were known to have activity against Pseudomonas aeruginosa in 81.2% of patients, Enterococci in 91.3% of patients, and anaerobes in 92.8% of patients. On the basis of our definition, inappropriate antimicrobial agent therapy was identified in three patients (4.3%), and all three achieved treatment success by 60 days. The first patient had a positive methicillin-resistant Staphylococcus aureus (MRSA) identified on surveillance screen of MDRO genes and received an initial antimicrobial regimen known to lack MRSA activity. The second and third patients received meropenem as initial therapy despite the detection of the New Delhi metallo-Β-lactamase (NDM) gene on surveillance screening in one patient and the isolation of carbapenem-resistant C. freundii from the abdominal drain in the other. Six patients (10.1%) required escalation to broader-spectrum regimens due to inadequate clinical response; all six ultimately experienced treatment failure.
Characteristics of Postoperative Abdominopelvic Abscesses and Antimicrobial Regimens
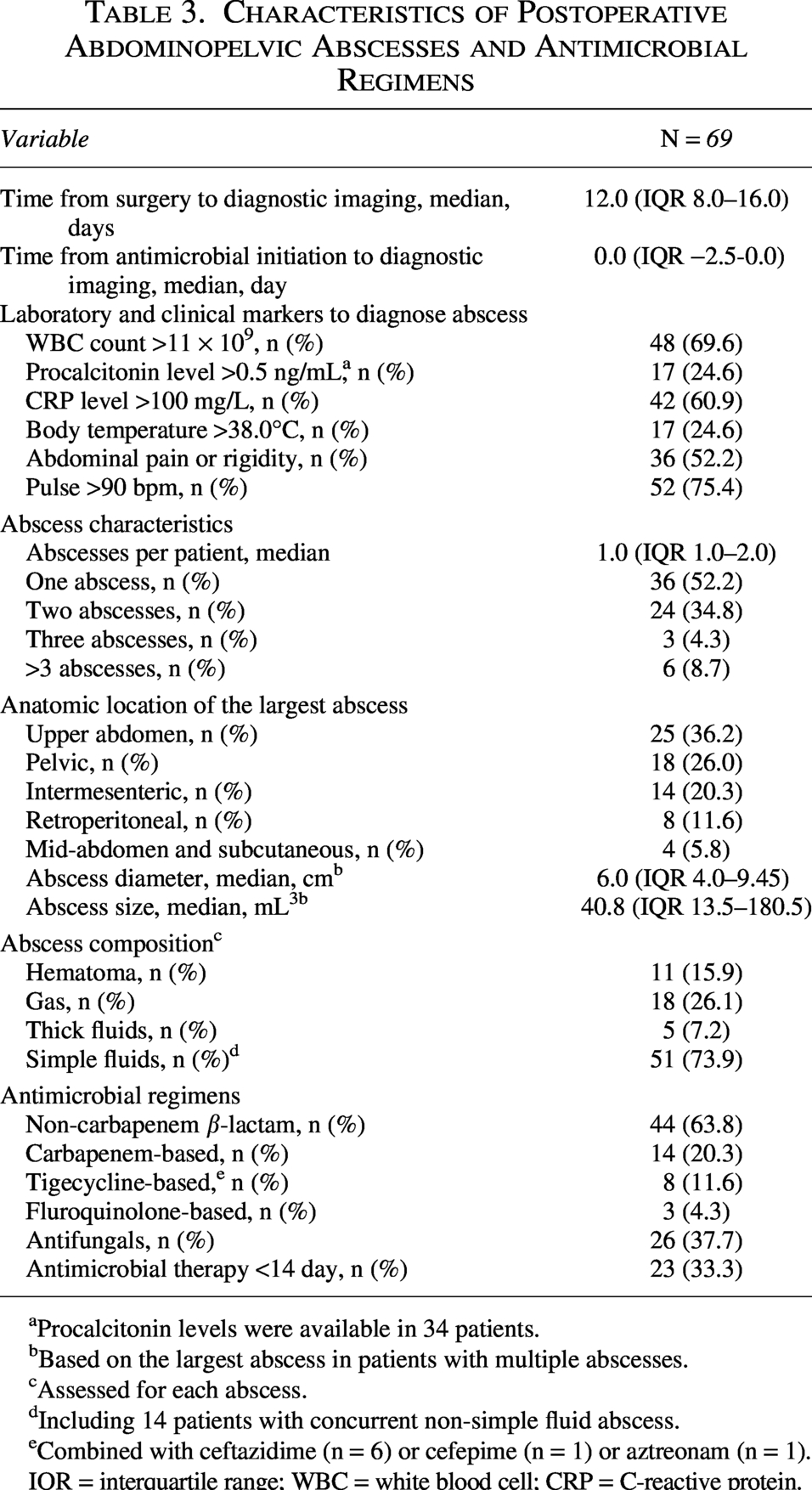
Procalcitonin levels were available in 34 patients.
bBased on the largest abscess in patients with multiple abscesses.
cAssessed for each abscess.
Including 14 patients with concurrent non-simple fluid abscess.
Combined with ceftazidime (n = 6) or cefepime (n = 1) or aztreonam (n = 1).
IQR = interquartile range; WBC = white blood cell; CRP = C-reactive protein.
All patients initiated antimicrobial treatment during hospitalization, with 42 patients (60.9%) receiving therapy based on clinical suspicion before radiologic confirmation of abscess formation. The median time from initiation of antimicrobials for abscess treatment and diagnostic imaging was day 0 (IQR, –2.5 to 0.0). The most frequently used antimicrobial regimen was a non-carbapenem β-lactam (n = 44, 63.8%), including 34 patients who received piperacillin-tazobactam. Among the 14 patients (20.2%) who received carbapenems, 12 had meropenem. Continuation of antimicrobial therapy after hospital discharge was required in 32 (46.3%) patients, including intravenous ertapenem (n = 4), oral ciprofloxacin combined with either metronidazole or clindamycin (n = 20), oral amoxicillin-clavulanate (n = 7), or oral co-trimoxazole (n = 1). The median total duration of antimicrobial therapy (inpatients plus outpatients) was 18 days (IQR, 11.5–32.5), including a median of inpatient duration of 12 days (IQR, 4.0–25.0) and a median outpatient treatment of 10 days (IQR, 7.0–14.0). Antifungals were used in 26 (37.6%) of patients, with the highest proportions in those who underwent solid organ transplant (n = 7), gastrectomy (n = 4), and cytoreductive procedure and HIPEC (n = 3).
Within three months of antimicrobial therapy initiation, 58 patients (84.0%) underwent repeat imaging (55 had a CT scan and 3 had an ultrasound) for various indications at a median of 27.0 days (IQR,18.0–52.7). In these patients with follow-up imaging, abscess resolution was observed in 25 patients at a median of 51 days (IQR, 19.5–83.5), and 17 patients had a decrease in abscess size. Eight patients had persistent, stable-sized abscesses, and eight demonstrated radiologic progression. The remaining 11 patients did not undergo follow-up imaging and were confirmed alive, clinically stable, and without evidence of treatment failure based on outpatient follow-up and medical record review.
By day 60 of antimicrobial treatment, success was achieved in 53 patients (76.8%) at a median of 16 days (IQR, 11.0–25.0), and failure occurred in 16 patients (23.2%) (Table 4). The Kaplan–Meier analysis demonstrated a median time to clinical response of 8.0 days (95% CI, 3.5–12.4) (Supplementary Fig. S1). All patients who failed were receiving antimicrobial therapy at the time of failure (31.5 day [IQR, 16.25–42.25]). The most frequent reasons for failure were the need for percutaneous drainage (n = 5) or re-operation (n = 5). All 16 patients who failed antimicrobial therapy had follow-up CT scan imaging demonstrating radiologic persistence of the abscess. None of the patients who failed antimicrobial therapy had a sole subcutaneous abscess.
Outcomes of Antimicrobial Therapy of Postoperative Non-Drainable Abdominopelvic Abscesses
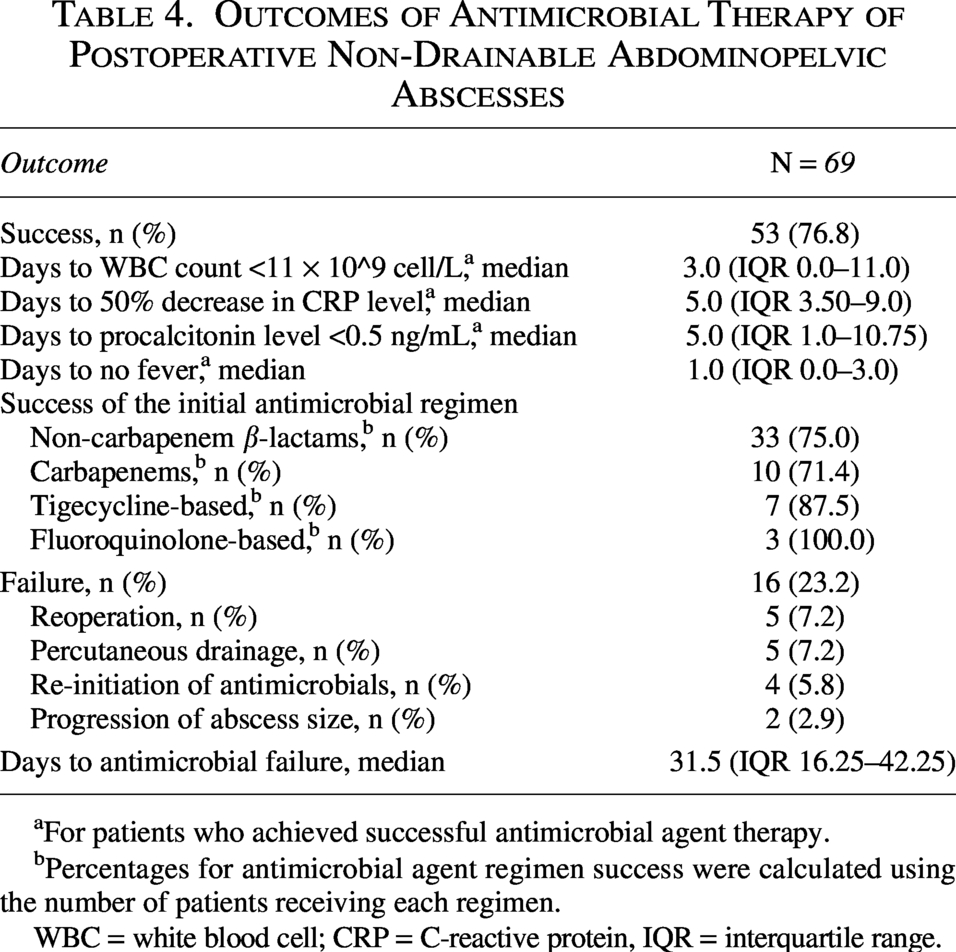
For patients who achieved successful antimicrobial agent therapy.
Percentages for antimicrobial agent regimen success were calculated using the number of patients receiving each regimen.
WBC = white blood cell; CRP = C-reactive protein, IQR = interquartile range.
Within 60 days of antimicrobial therapy initiation, 13 patients (18.8%) were readmitted to the hospital, and 20 patients (28.9%) visited the emergency department and underwent abdominal CT scans.
In univariable logistic regression analysis, preoperative immunosuppressive agents and postoperative corticosteroids were associated with an increased risk of antimicrobial therapy failure (OR, 8.50; 95% CI, 1.39–51.94; p = 0.02, and OR, 7.35; 95% CI, 1.74–30.91; p = 0.006, respectively). In multivariable logistic regression analysis, pelvic abscess location (OR, 6.87, 95% CI, 1.55–30.33; p = 0.011), postoperative corticosteroids (OR, 11.90; 95% CI, 1.01–129.68; p = 0.041), and longer time from procedure date to diagnostic imaging (OR, 0.85 per day; 95% CI, 0.73–0.98; p = 0.029) were independently associated with treatment failure (Supplementary Table S2).
Discussion
This retrospective cohort study demonstrates a 76.8% success rate of antimicrobial therapy alone for postoperative non-drainable abdominopelvic abscesses at 60 days. Clinical improvement occurred at a median of 8 days after treatment initiation. Among successfully treated patients who underwent follow-up imaging, radiologic resolution or reduction in abscess size was observed in more than 75%, with complete resolution observed at a median of 51 days. These findings suggest that in selected patients with postoperative abdominopelvic abscesses not amenable to drainage, antimicrobial therapy alone with close clinical monitoring may be a reasonable management approach.
The success rate observed in our study aligns with that reported with antimicrobial management of abdominopelvic abscesses in non-surgical patients. A randomized controlled trial of patients with diverticulitis and extraluminal abscess managed nonoperatively reported a slightly higher success rate (81%). 17 However, important differences exist between the two populations. Postoperative abscesses represent hospital-acquired infections and are more likely to involve MDROs, which are associated with increased risk of therapy failure.10,18
In our cohort, most patients received regimens with activity against Enterobacter spp., lactose-negative gram-negative bacilli (e.g., P. aeruginosa), and Enterococci consistent with the Surgical Infections Society guidelines that consider postoperative IAI as high-risk and recommend broad-spectrum antimicrobial coverage. 7 Approximately one-third of patients received a concomitant antifungal therapy, which likely reflects clinicians concern for invasive fungal infection in a high-risk population, including patients with malignant disease, and those receiving immunosuppressive therapy.
Despite a relatively high overall success rate, nearly one-quarter of patients experienced antimicrobial treatment failure. This failure rate is similar to that reported in a systematic review of 42 studies evaluating various approaches to managing colonic diverticulitis with abscess, and reported a 21% failure rate of antibiotic therapy without drainage. 19 In our cohort, the median abscess diameter was larger (6.0 vs. 4.0 cm) than that reported in the systematic review. This difference in abscess size underscores the complexity of postoperative abscess and supports the observed failure rate.
Pelvic abscess location emerged as an independent predictor of antimicrobial therapy failure, conferring more than a sixfold increase in odds of failure compared with abscesses at other anatomic locations. This finding is consistent with previous studies of pelvic-infected collections, including tubo-ovarian abscesses, which reported a similar OR (5.8) for treatment failure with antimicrobial therapy. 20 Pelvic abscesses are often associated with a higher bacterial inoculum burden and complex polymicrobial milieu than upper abdominal abscesses, which may contribute to reduced responsiveness to antimicrobial therapy alone.21,22
Postoperative corticosteroid exposure was independently associated with antimicrobial failure. Corticosteroids are known to impair innate immune response, including neutrophil and macrophage function, which may reduce the host’s ability to contain localized infections. 23 Although the CI is wide, reflecting the limited number of exposed patients, this finding is scientifically plausible.
Another notable finding in our study was an association between a longer time to diagnostic imaging and a lower likelihood of antimicrobial failure. Specifically, each incremental increase in time to imaging was associated with a 13% reduction in the odds of treatment failure. This counterintuitive association likely reflects confounding by indication, whereby patients with more severe or rapidly progressive disease undergo earlier imaging and are intrinsically at higher risk of antimicrobial failure. Similar associations have been reported in other IAI cohorts, where early imaging reflects greater clinical severity rather than improved outcomes. 24
The prolonged, broad-spectrum antimicrobial therapy observed in this study reflects the high-risk nature of the population. A substantial proportion of patients had malignant disease and were candidates for chemotherapy, in whom the relapse of infection could delay oncologic treatment.5,25 In addition, a subset of patients were solid organ transplant recipients, for whom postoperative infection may require stopping immunosuppressive therapy or dose reduction. 6 In these settings, clinicians often favored antimicrobial regimens with broad coverage and extended duration to mitigate the risk of relapse during periods of altered host immunity. However, this study was not designed to define the optimal spectrum or duration of antimicrobial therapy.
While our findings demonstrated that antimicrobial therapy has the ability to control abscesses, this approach should not be considered a substitute for source control when drainage or reoperation are feasible. All reasonable efforts to achieve source control should remain the standard of care.3,7 Furthermore, antimicrobials only management should be reserved for carefully selected patients, and early re-assessment is essential. Lack of clinical improvement or evidence of disease progression should prompt reconsideration of source-control strategies. This is particularly important to avoid prolonged exposure to antimicrobial agents, which may contribute to the emergence of MDROs.
Although 71% of patients had simple fluid on imaging, more than one-fourth had a concurrent abscess with a different fluid composition. Furthermore, postoperative simple fluid on imaging does not preclude abscess diagnosis, as classic abscess features may not be present in the early stages. 26
Several limitations should be acknowledged. First, the retrospective design introduces potential bias. Second, the single-center setting may limit the generalizability of the findings. Third, no formal sample size calculation was performed, and the relatively small sample size, together with the limited number of outcome events, resulted in a low event-per-variable ratio, which may contribute to model instability and imprecision of effect estimates, as reflected by the wide CIs. Although multivariable modeling was restricted to reduce the risk of overfitting, these findings should be interpreted with caution and considered exploratory and hypothesis-generating rather than confirmatory. Fourth, follow-up imaging was not available for all patients; however, all patients were followed for 60 days, allowing assessment of clinical outcomes irrespective of imaging availability. Finally, antimicrobial regimens were heterogeneous, reflecting real-world practice.
Conclusions
Using antimicrobial therapy with close follow-up in managing postoperative abdominopelvic abscesses unamenable to percutaneous drainage is associated with favorable clinical outcomes. Factors associated with antimicrobial agent therapy failure include pelvic abscess location, postoperative corticosteroid exposure, and a shorter interval between operation and diagnostic imaging. Although antimicrobial therapy should not be considered a substitute for source control when feasible, these findings support its role as a management option in selected patients. Prospective studies are warranted to validate these findings and optimize antimicrobial regimens.
Ethical Considerations
The study was approved by the Office of Research Affairs (RAC#2251133) on March 10, 2025, and received a waiver of informed consent because of the retrospective design.
Data Availability
Data available from the authors upon reasonable request.
Authors’ Contributions
H.A.H. conceived the idea and drafted the original article. H.A.H. and Ald.Z. developed the statistical analysis plan. Ald.Z. performed the analysis. H.A.H., Ald.Z., Aly.Z., and A.A. contributed to the design of methods. A.A., A.L., and A.T. were responsible for data curation; and A.S. assisted with data organization and study coordination. All authors reviewed the article critically and approved the final version.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received to conduct the study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.